

Abstract
We report a case of a 42-year-old man presenting with shortness of breath and palpitation on exertion, who was evaluated to have left sinus of Valsalva aneurysm rupturing into right atrium. This is a very rare congenital cardiac anomaly with variable clinical presentation ranging from asymptomatic detection on imaging to acute coronary syndrome and sudden cardiac death. Rupture is the most dreaded complication and usually manifests as an acute event. Aneurysmal dilation less commonly affects the left sinus and rupture into the right atrium is still rarer and a chronic insidious presentation as in this case is odd.
Background
Sinus of Valsalva aneurysm (SVA) is one of the rare congenital anomalies described in the literature, prevalence being 1% of all congenital anomalies of heart and circulation1 and 0.78% of all congenital open heart operations.2 Aneurysmal dilation affects the right sinus of Valsalva in 70% cases, non-coronary sinus in 25% cases and only 5% affects the left coronary sinus (LCS).3 Congenital deficiency of elastic and muscular tissue at the junction of aortic media and annulus fibrosus of aortic valve is the aetiology in majority of cases. Risks associated with SVA include rupture, compression of adjacent cardiac structures and development of aortic regurgitation. Rupture is the most dreaded complication of SVA. We hereby describe a case of ruptured SVA (RSOV, rupture of sinus of Valsalva) arising from left sinus of Valsalva into right atrium (RA) which is extremely rare.
Case presentation
A 42-year-old man with no other significant comorbidities presented with history of palpitations and shortness of breath on exertion for 6 years duration. On examination he was found to have continuous murmur in the right second intercostal space with peripheral signs of aortic run off.
Investigations
ECG showed left ventricular hypertrophy with right atrial enlargement and chest x-ray showed mild cardiomegaly with right atrial enlargement. Two dimensional echocardiography showed grossly dilated right atrium and right ventricle and continuous shunt opening into right atrium with peak systolic gradient of 37 mm Hg and end diastolic gradient of 13 mm Hg. Transesophageal echocardiography (TEE) showed aneurysmally dilated left sinus of Valsalva which was communicating into right atrium forming a tunnel with continuous flow into right atrium (figures 1 and 2). Subsequently he underwent cardiac catheterisation with oximetry and coronary angiography which confirmed aneurysm of left aortic sinus Valsalva rupturing into right atrium forming a tunnel (figures 3 and 4). Left main coronary artery had its origin from the aneurysm. Oximetry analysis showed step up of oxygen saturation by 17% in right atrium (table 1). The calculated Qp/Qs (pulmonary to systemic blood flow) ratio was 2.5 suggestive of large left-to-right shunt.
Figure 1.
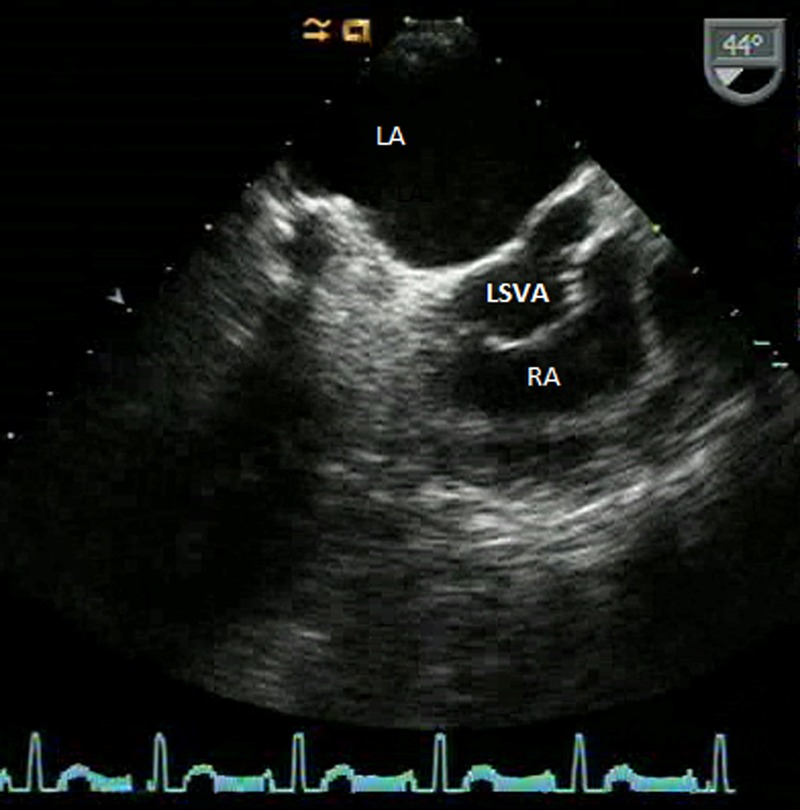
Transesophageal echocardiography showing sinus of Valsalva aneurysm from left coronary sinus rupturing into right atrium. LA, left atrium; RA, right atrium; LSVA, left sinus of Valsalva aneurysm rupturing into right atrium.
Figure 2.
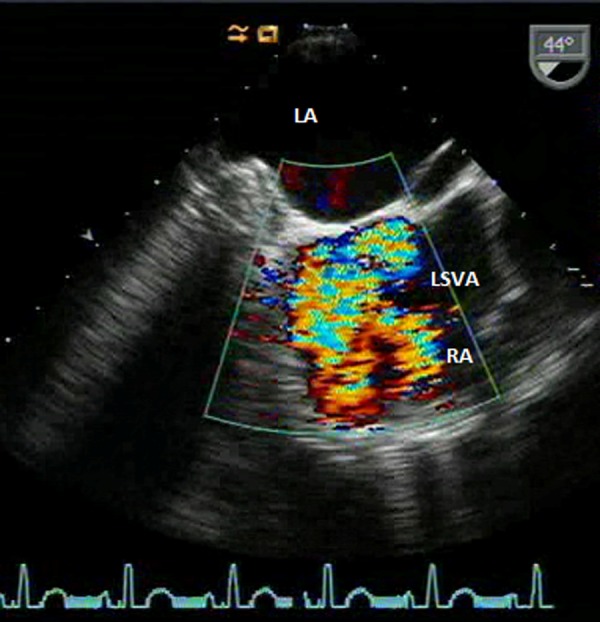
Colour Doppler imaging showing ruptured sinus of Valsalva aneurysm from left coronary sinus opening into right atrium. LA, left atrium; RA, right atrium; LSVA, left sinus of Valsalva aneurysm rupturing into right atrium.
Figure 3.

Angiographic picture showing left sinus of Valsalva aneurysm rupturing into right atrium. 1, Left coronary sinus aneurysm; 2, fistulous tract between aneurysmal sac and right atrium; 3, ruptured sinus of Valsalva aneurysm opening into right atrium; 4, right coronary artery.
Figure 4.

Left main coronary artery arising from the aneurysmal sac. 1, Left main coronary artery; 2, left coronary sinus aneurysm.
Table 1.
Oximetry and haemodynamic data
| SaO2 (%) | Pressure (mmHg) | |
|---|---|---|
| SVC | 66 | – |
| RA | 83 | a 15, v 1, mean 8 |
| RV | 85 | 34/8 |
| PA | 85 | 34/9, mean 21 |
| LV | 95 | 166/10 |
| Aorta | 95 | 166/71/112 |
RA, right atrium; RV, right ventricle; LA, left atrium; LV, left ventricle; PA, pulmonary artery; SVC, superior vena cava.
Outcome and follow-up
The patient was advised surgical correction and referred to surgical unit.
Discussion
RSOV is more common in males with mean age of rupture being 34 years.4 SVA is more often congenital than acquired in origin. Acquired causes include infective endocarditis, syphilis, trauma, connective tissue disorders, Marfan syndrome, atherosclerosis and cystic medial necrosis. SVA comes to clinical attention because of acute development of large perforation or gradual development of small perforation, or because of asymptomatic or symptomatic unruptured aneurysm. An acute large rupture announces itself by dramatic onset of severe retrosternal chest pain and intractable heart failure. Small insidious perforations progress gradually and initially go unnoticed. Death from congestive heart failure usually occurs within a year after rupture, however longer survival after small slow perforation is well described. SVA can present in various ways such as rupture into cardiac chamber with subsequent cardiac failure, acute coronary syndrome, cardiac tamponade, heart block, aortic regurgitation and right ventricular outflow tract obstruction.5
Majority of SVA arising from right coronary sinus ruptures in right ventricle and those arising from non-coronary sinus ruptures into RA.3 Left aortic sinus aneurysm commonly ruptures into left atrium or left ventricle, pulmonary artery, epicardium and pericardium owing to proximity. RSOV from LCS into RA is very rare and the literature is sparse in this regard.6–10 Unruptured SVA from LCS is unique as it can present as acute coronary syndrome or as sudden cardiac death owing to compression of left coronary artery.11–13 The left coronary artery can arise separately or it can originate from the aneurysmal sac itself as in our case.
Echocardiography remains the most commonly used diagnostic tool for RSOV. The gold standard for diagnosis of SVA is cardiac catheterisation with aortography, and oximetry analysis adds to the diagnostic yield. Other imaging techniques include MRI and CT angiography.14 SVA should be operated because of the risks associated with its rupture or compression of adjacent cardiac structures. Surgical closure is either by simple suture closure or by patch closure of RSOV and the recurrence rate varies from series to series from 0% to 20%.15 16 Recently device closure of RSOV has gained popularity, however it is feasible only in selected cases.
Learning points.
Congenital sinus of Valsalva aneurysm arising from left coronary sinus is a rare entity and rupturing into right atrium is still rare and can have varied presentations from asymptomatic detection in echocardiography to sudden cardiac death.
It requires high clinical suspicion and an Echocardiography can diagnose most of the cases.
Surgery is the gold standard but percutaneous closure can be tried in cases with good anatomic suitability.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Wells T, Byrd B, Neirste D, et al. Sinus of Valsalva aneurysm with rupture into the interventricular septum and left ventricular cavity. Circulation 1999;100:1843. [DOI] [PubMed] [Google Scholar]
- 2.Dong C, Wu QY, Tang Y. Ruptured sinus of Valsalva aneurysm: a Beijing experience. Ann Thorac Surg 2002;74:1621–4 [DOI] [PubMed] [Google Scholar]
- 3.Moustafa S, Mookadam F, Cooper L, et al. Sinus of Valsalva aneurysms—47 years of a single center experience and systematic overview of published reports. Am J Cardiol 2007;99:1159–64 [DOI] [PubMed] [Google Scholar]
- 4.Sakakibara S, Konno S. Congenital aneurysm of the sinus of Valsalva associated with ventricular septal defect: anatomical aspects. Am Heart J 1968;75:595–603 [DOI] [PubMed] [Google Scholar]
- 5.Viktorsson TV, Arnorsson T, Sigurdsson MI, et al. A giant unruptured aneurysm of the sinus of Valsalva together with ectasia of the left coronary artery. Ann Thorac Surg 92:354–6 [DOI] [PubMed] [Google Scholar]
- 6.Rosenberg H, Williams W, Trusler G, et al. Congenital aortico-right atrial communications. The dilemma of differentiation from coronary-cameral fistula. J Thorac Cardiovasc Surg 1986;91:841. [PubMed] [Google Scholar]
- 7.Arturi E, Gabrielli F, Alcini E. Aneurysm of the left sinus of Valsalva with fistula in the right atrium. A case report. G Ital Cardiol 1990;20:976. [PubMed] [Google Scholar]
- 8.Goldberg N, Zisbrod Z, Kipperman R, et al. Congenital aneurysm of the left coronary sinus and left main coronary artery with fistulous communication to the right atrium in pregnancy. J Am Soc Echocardiogr 1990;3:125. [DOI] [PubMed] [Google Scholar]
- 9.Tsai YC, Wang JN, Yang YJ, et al. Aortico-cameral communication from left sinus Valsalva aneurysm to right atrium via a tortuous tunnel with aneurysmal dilatation. Pediatr Cardiol 2002;23:108–9 [DOI] [PubMed] [Google Scholar]
- 10.Dwivedi S, Saran R, Sethi R. Ruptured left sinus of Valsalva aneurysm to right atrium. Indian Heart J 2005;57:73. [PubMed] [Google Scholar]
- 11.Lijoi A, Parodi E, Passerone GC, et al. Unruptured aneurysm of the left sinus of Valsalva causing coronary insufficiency: case report and review of the literature. Tex Heart Inst J 2002;29:40. [PMC free article] [PubMed] [Google Scholar]
- 12.Hiyamuta K, Ohtsuki T, Shimamatsu M, et al. Aneurysm of the left aortic sinus causing acute myocardial infarction. Circulation 1983;67:1151–4 [DOI] [PubMed] [Google Scholar]
- 13.Cuculi F, Rossi M, Bradley KM, et al. Rupture of a left sinus of Valsalva aneurysm with coronary compression: a rare cause of ischemic chest pain. Ann Thorac Surg 92:e97–9 [DOI] [PubMed] [Google Scholar]
- 14.Kulan K, Kulan C, Tuncer C. Echocardiography and magnetic resonance imaging of sinus of Valsalva aneurysm with rupture into the ventricle. J Cardiovasc Surg 1996;37:639. [PubMed] [Google Scholar]
- 15.Au WK, Chiu SW, Mok CK, et al. Repair of ruptured sinus of Valsalva aneurysm: determinants of long-term survival. Ann Thorac Surg 1998;66:1604–10 [DOI] [PubMed] [Google Scholar]
- 16.Barragry TP, Ring WS, Moller JH, et al. 15- to 30-year follow-up of patients undergoing repair of ruptured congenital aneurysms of the sinus of Valsalva. Ann Thorac Surg 1988;46:515. [DOI] [PubMed] [Google Scholar]