

Description
An 85-year-old man presented with 2 weeks of right-sided pleuritic chest pain, non-productive cough and low-grade fever. There was a history of pulmonary tuberculosis approximately 40 years earlier, but the patient did not know which medical treatment he had been through. He denied any previous surgery.
Physical examination showed no clinical signs of respiratory distress. The laboratory results showed an elevated C reactive protein of 8.02 mg/dl and increased erythrocyte sedimentation of 100 mm. A posteroanterior chest radiograph showed an air fluid level without a well-circumscribed border in the right lower lung zone (figure 1). The CT showed the right pleura extensively thickened and calcified, consistent with a calcified fibrothorax, with a hydropneumothorax, possibly corresponding to empyema, in the right lower hemithorax, and increased lung opacity and atelectasis in adjacent lung parenchyma (figures 2 and 3). The tuberculin skin test performed was strongly positive. The examination of sputum was positive for acid-fast bacilli, and the examination with PCR identified Mycobacterium tuberculosis.
Figure 1.
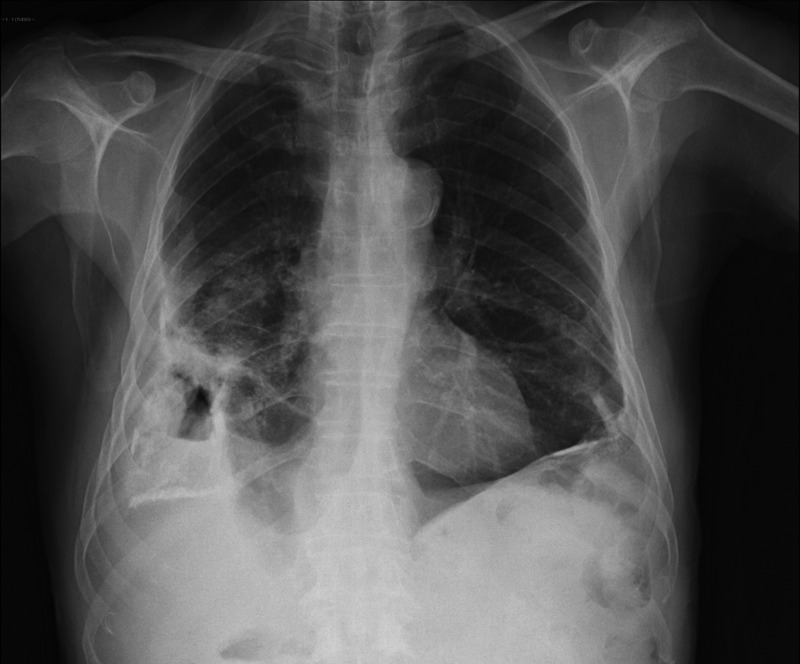
Posteroanterior chest radiograph—air fluid level without a well-circumscribed border in the right lower lung zone.
Figure 2.
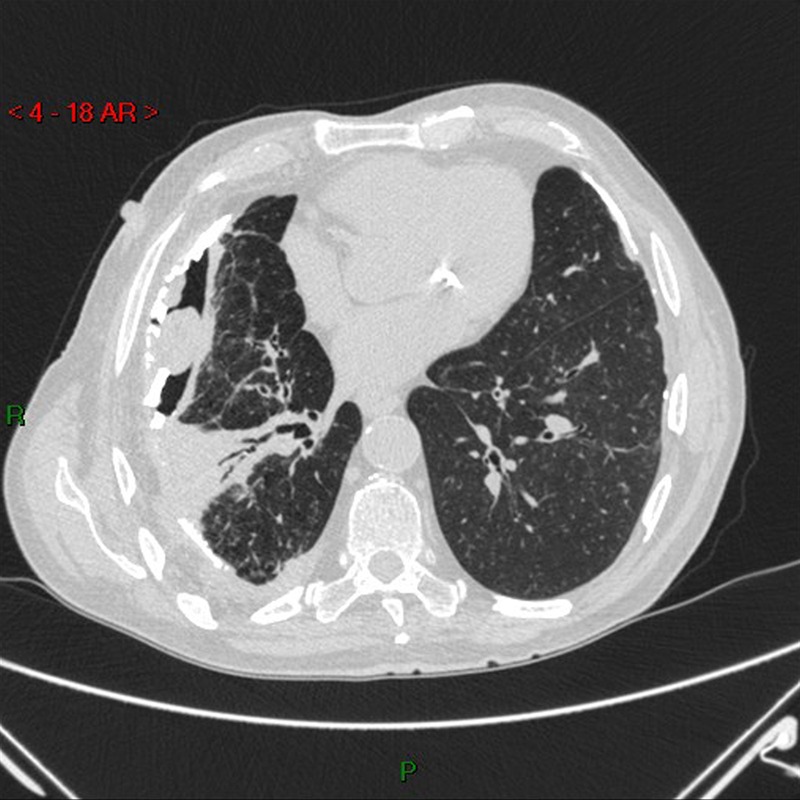
CT scan—right pleura extensively thickened and calcified with a hydropneunmothorax, possibly corresponding to empyema, in the right lower hemithorax.
Figure 3.
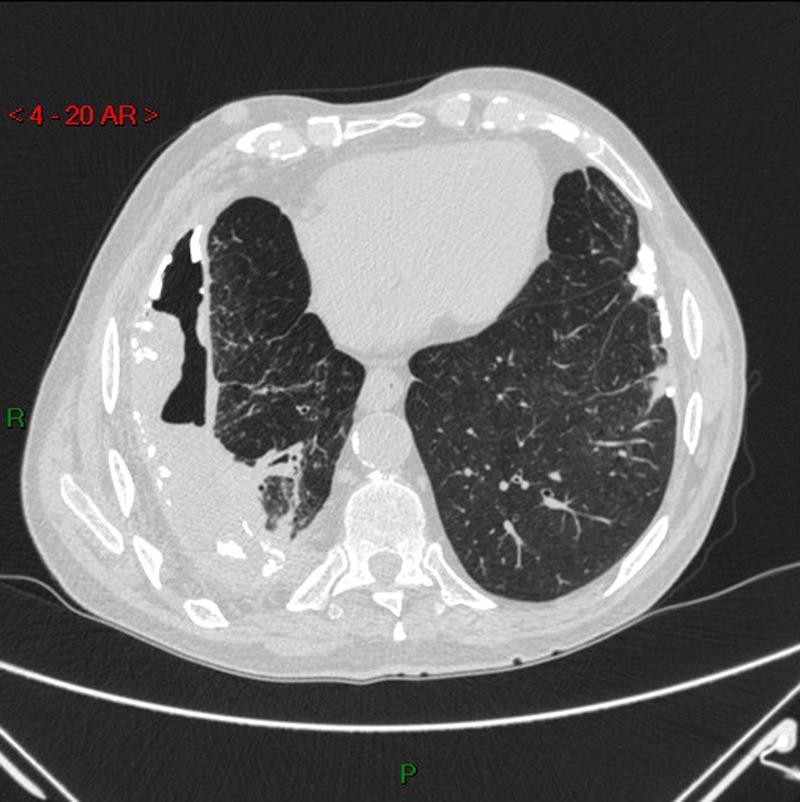
CT scan—right pleura extensively thickened and calcified, with a hydropneunmothorax, possibly corresponding to empyema, in the right lower hemithorax and increased lung opacity and atelectasis in adjacent lung parenchyma.
Reactivation of tuberculosis with empyema was diagnosed and antituberculosis standard regimen was performed.
Reactivation tuberculosis represents 90% of adult cases among HIV-negative individuals, and results from reactivation of a previously dormant focus seeded at the time of the primary infection. The original site of spread may have been previously visible as a small scar called a Simon focus.
In non-endemic countries, the incidence of pulmonary tuberculosis is two to three times higher among older adults. Cavitary disease is less common while multilobar and lower lobe involvement more common.
Tuberculous empyema represents a chronic, active infection of the pleural space that contains a large number of tubercle bacilli. It is rare compared with tuberculous pleural effusions that result from an exaggerated inflammatory response to a localised paucibacillary pleural infection with tuberculosis. The inflammatory process may be present for years with a paucity of clinical symptoms.
Learning points.
Reactivation tuberculosis refers to reactivation of a previously dormant focus seeded at the time of the primary infection.
The complications of tuberculosis pleuritis are as varied as its pulmonary manifestations. CT scans can be valuable in the diagnosis of the chronic complications or the late sequelae of tuberculous pleuritis.
Prevention of reactivation tuberculosis is accomplished by screening for and treatment of latent tuberculosis infection.
Footnotes
Patient consent: Obtained.
Competing interests: None.
Provenance and peer review: Not commissioned; externally peer reviewed.