

Abstract
Background
The American Cancer Society (ACS), the Centers for Disease Control and Prevention (CDC), the National Cancer Institute (NCI), and the North American Association of Central Cancer Registries (NAACCR) collaborate annually to provide updated information about cancer occurrence and trends in the United States (U.S.). This year’s report includes trends in colorectal cancer (CRC) incidence and death rates and highlights use of microsimulation modeling as a tool for interpreting past trends and projecting future trends to assist in cancer control planning and policy decisions.
Methods
Information on invasive cancers was obtained from the NCI, CDC, and NAACCR, and information on deaths from the CDC’s National Center for Health Statistics. Annual percentage changes in the age-standardized incidence and death rates (2000 U.S. population standard) for all cancers combined and for the top 15 cancers were estimated by joinpoint analysis of long-term (1975–2006) trends and short-term fixed interval (1997–2006) trends. All statistical tests were two-sided.
Results
Both incidence and death rates from all cancers combined significantly declined (P < .05) in the most recent time period for men and women overall and for most racial and ethnic populations. These decreases were driven largely by declines in both incidence and death rates for the 3 most common cancers in men (i.e., lung and prostate cancers and CRC) and for two of the 3 leading cancers in women (i.e., breast cancer and CRC). The long-term trends for lung cancer mortality in women showed smaller and smaller increases until 2003 when there was a change to a non-significant decline. Microsimulation modeling shows that declines in CRC death rates are consistent with a relatively large contribution from screening and with a smaller but demonstrable impact of risk factor reductions and improved treatments. These declines are projected to continue if risk factor modification, screening, and treatment remain at current rates, but could be further accelerated with favorable trends in risk factors and higher utilization of screening and optimal treatment.
Conclusions
Although the decrease in overall cancer incidence and death rates is encouraging, rising incidence and mortality for some cancers are of concern.
Keywords: cancer, incidence, mortality, SEER, NAACCR, NPCR, United States (U.S.), CISNET colon models, microsimulation models, colorectal cancers
INTRODUCTION
The American Cancer Society (ACS), the Centers for Disease Control and Prevention (CDC), the National Cancer Institute (NCI), and the North American Association of Central Cancer Registries (NAACCR) collaborate each year to produce a report to the nation on the current status of cancer in the U.S. The first report, published in 1998, documented the first sustained decline in cancer death rates since the 1930s.1 Subsequent reports have updated information on trends in incidence and death rates and featured in-depth analyses of selected topics,2–10 including incidence and mortality trends for colorectal cancer (CRC).11 The current report provides updated trends in incidence and death rates for all cancers combined and for the top 15 cancers among all races combined and among each of the 4 major racial/ethnic groups (white, black, Asian and Pacific Islander [API], and Hispanic) by sex; it also provides incidence and mortality data for American Indian/Alaska Natives (AI/AN) who reside in counties covered by the Indian Health Service (IHS) Contract Health Services Delivery Area (CHSDA). Further, this report provides an update on incidence and mortality trends for CRC and uses a microsimulation model of CRC to interpret past trends and project future trends. Our application of simulation modeling provides information on the relative impact of modifiable risk factors, screening use, and treatment patterns on cancer trends and compares different future scenarios. The methodology did not focus on applications comparing multiple strategies for a category of interventions (e.g., screening tests) nor multiple types of models. The report also highlights use of microsimulation models to assist in cancer prevention and control planning and in setting public policy (http://cisnet.cancer.gov/projections/colorectal/).
SUBJECTS AND METHODS
Cancers, Cancer Deaths, and Population Estimates
Information on newly diagnosed invasive cancers, including in situ cancers of the bladder, was obtained from population-based cancer registries that participate in NCI’s Surveillance, Epidemiology, and End Results (SEER) Program and/or the CDC’s National Program of Cancer Registries (NPCR). All participating cancer registries are members of NAACCR.
Site and histology for incidence cancers were coded according to the International Classification of Diseases for Oncology (ICD-O) edition in use at the time of diagnosis, converted to the Third Edition coding,12 and categorized according to SEER site groups.13 For cancer deaths, the underlying causes of death were selected according to the version of the International Classification of Diseases (ICD) codes and selection rules in use at the time of death (ICD-6 to ICD-10).14–18
Cause of death is based on death certificate information reported to state vital statistics offices; this information is consolidated through the CDC National Center for Health Statistics (NCHS) National Vital Statistics System19 and categorized according to SEER anatomic site groups13 to maximize comparability among ICD and ICD-O versions. County-level population estimates, summed to the state and national level, were used as denominators in rate calculations.20 Because the 2000 U.S. census allowed respondents to identify themselves as multiracial, the NCHS and the Census Bureau developed methods for bridging multiple-race population estimates to single-race estimates to describe long-term trends in disease rates by race.21 The Census Bureau has provided NCI with bridged, single-race annual population estimates from 1990–2007, with annual re-estimates calculated back to the most recent decennial census. NCI makes slight modifications to the Hawaii population estimates based on additional local information (http://seer.cancer.gov/popdata/methods.html).
For most states, population estimates as of July 1 of each year were used to calculate annual incidence and death rates because these estimates are presumed to reflect the average population of a defined geographic area for a calendar year. For Louisiana, Alabama, Mississippi, and Texas where residents were displaced in the fall of 2005 by hurricanes Katrina and Rita, incidence data for the first 6 months of 2005 and half of the July 1 population estimate were used to calculate state-specific incidence rates for 2005. For the 2005 death rate calculations, NCI made adjustments to the 2005 population estimates to account for the displacement and these data were made available for use by the cancer surveillance agencies. The national total population estimates are not affected by these adjustments. Further details on these calculations are provided at http://seer.cancer.gov/popdata/methods.html.
Incidence data are not uniformly available for every period, geographic area, and racial and ethnic group in the U.S. Therefore, analyses of long-term (1975–2006) and short-term fixed interval (1997–2006) trends in incidence rates and in 5-year (2002–2006) average age-standardized incidence rates for the top 15 cancer sites include different geographic areas and populations. To evaluate the long-term incidence trends (1975–2006) for all races and ethnicities combined, data were used from the 9 original SEER areas (Atlanta, Connecticut, Detroit, Hawaii, Iowa, New Mexico, San Francisco-Oakland, Seattle-Puget Sound, and Utah), which cover about 10% of the U.S. population (9% each of U.S. white and U.S. black, 8% of U.S. Hispanic, and 19% of U.S. Asian).22 Data from 33 population-based cancer registries were used to assess short-term trends (1997–2006), and data from 43 population-based cancer registries were used to estimate 5-year average annual (2002–2006) age-standardized incidence rates for all races and ethnicities combined and for each of the 5 major racial/ethnic populations (white, black, API, AI/AN residing in counties covered by IHS’s CHSDA, and Hispanic). The 33 and 43 registries met NAACCR’s data quality criteria for every year included in the analysis; these registries cover about 71% and 85% of the U.S. population, respectively. The 33 cancer registries cover 71% of the U.S. white population, 63% black, 88% Hispanic, 87% API, and 72% AI/AN (CHSDA); the 43 cancer registries cover 86% of the U.S. white population, 83% black, 92% Hispanic, 93% API, and 78% AI/AN (CHSDA). New incidence cases identified through IHS were incorporated into the pooled cancer registry analysis file.9
U.S. mortality data from NCHS were unavailable for every racial/ethnic group for all periods studied; notably the Hispanic ethnicity was not reported on death certificates in every state for all years during the period 1997–2006. For all races and ethnicities combined, we examined long-term (1975–2006) trends, short-term (1997–2006) trends, and 5-year (2002–2006) average annual age-standardized death rates for all cancer sites and for the top 15 cancer sites for men and women in each of the five major racial/ethnic populations (white, black, API, AI/AN CHSDA, and Hispanic). Mortality data for the AI/AN population were based on deaths in counties served by IHS’s CHSDA because estimated rates based on CHSDA counties have been reported to be more reliable than national data.9
Statistical Analysis
Age-specific and age-standardized rates were expressed per 100,000 population (based on 2000 U.S. standard population) and generated by using SEER*Stat Software, Version 6.5.2 (http://www.seer.cancer.gov/seerstat;23 http://seer.cancer.gov/popdata/methods.html). Rates for 2002–2006 were suppressed if the numerator was <16 observations consistent with our previous work.6–10
Long-term trends (1975–2006) in age-standardized SEER 9 cancer incidence and U.S. death rates were described using joinpoint regression analysis, which involves fitting a series of joined straight lines on a logarithmic scale to the trends in the annual age-standardized rates (http://seer.cancer.gov/csr/1975_2006/technotes/joinpoint.html). We allowed a maximum of 4 joinpoints in the model to better characterize emerging trends, which are expressed in up to 5 variable time intervals. The method is described in detail elsewhere.24 The resulting trends of varying time periods are described by annual percent change (APC), i.e., the slope of the line segment.24 Long-term incidence trends are based on both observed data and data adjusted for reporting delay (which mostly affects recent years).25 Our descriptions of long-term trends in incidence are based on the delay-adjusted data except when specifically noted. For short-term fixed interval (1997–2006) trend analyses, a joinpoint regression analysis with a maximum of 1 joinpoint was used to estimate APCs.
This year’s report provides the average annual percent change (AAPC) as an addendum to the underlying joinpoint trends and as a summary measure to compare fixed interval trends by race/ethnicity. AAPC quantifies the average trend over a period of multiple years. It can be estimated even if the joinpoint model indicates that changes in trends occurred during those years because AAPC is estimated as a geometric weighted average of the joinpoint APCs, with the weights equal to the lengths of each segment over the pre-specified fixed interval (http://srab.cancer.gov/joinpoint/aapcc.html).26–27 The APC was suppressed if the numerator was <10 cancers for any year within the designated time interval, consistent with our previous methods.6–10
In describing long- and short-term trends with estimates of APC and AAPC, the terms “increase” or “decrease” were used when the slope (APC or AAPC) of the trend was statistically significant (P < .05). When the trend was not significant, terms such as “level,” “stable,” “non-significant increase,” and “non-significant decrease” were used depending on the results.
Colorectal (CRC) Rates and Trends
Age-standardized CRC incidence rates for diagnosis years 2002–2006 and AAPC estimates of short-term trends for diagnosis years 1997–2006 were based on SEER and NPCR pooled data reported by NAACCR. For diagnosis years 2002–2006, we also present 5-year average age-specific CRC incidence rates for age groups <50, 50–64, and ≥65; for colorectal sub-sites (proximal colon, distal colon, rectum, and other), and for racial/ethnic groups (white, black, API, AI/AN CHSDA, Hispanic, non-Hispanic), as well as for combinations of these variables. Anatomic sub-site was based on the ICD-O-3 codes for broad categories: proximal colon (C18.0, C18.2–C18.5), distal colon (C18.6, C18.7), rectum (C19.9, C20.9), and other (C18.1, C18.8, C18.9, C26.0). Changes in coding rules for stage of cancer at diagnosis, particularly introduction of the Collaborative Stage (CS) Data Collection System (http://training.seer.cancer.gov/collaborative) for cases diagnosed in 2004 forward, caused a systematic shift in stage between 2003 and 2004 and thus precluded use of NAACCR pooled data to evaluate stage-specific cancer incidence trends. Stage-specific analyses were based on the SEER Extent of Disease (EOD) codes and CS for the SEER 9 registries (http://seer.cancer.gov). Long-term trends in stage-specific incidence rates and 5-year stage-specific relative survival for CRC used the SEER 9 data for diagnosis years 1975–2006, based on historic stage (localized, regional, distant, and unknown).
CRC Incidence and Mortality Models: Assessing the Impact of Risk Factors, Screening and Treatment
We used a microsimulation model,28 MISCAN-Colon, from NCI’s Cancer Intervention and Surveillance Modeling Network (CISNET) consortium (http://cisnet.cancer.gov/projections/colorectal) to estimate the impact of historical changes in risk factors, screening, and treatment on past CRC incidence and mortality trends and to project future mortality trends through 2020. The projections of future mortality trends have been previously published whereas the past trends are an intermediate result of this previously published work. Consequently, the model methodology, inputs and assumptions have been described previously.29–31 Briefly, the MISCAN-Colon model simulates the U.S. population from 1975 to 2020 at risk for CRC based on the sequence of developments as an adenoma becomes cancer.32–34 The model also distinguishes 3 types of interventions considered separately and as combined interventions that can affect the natural history of the adenoma-carcinoma sequence (Figure 1).29, 35–36 MISCAN-Colon models risk factor influence through changing the risk of developing adenomas. Screening is modeled as potentially affecting adenomas, preclinical and clinical disease (the effect depends on the screening test).
Figure 1.
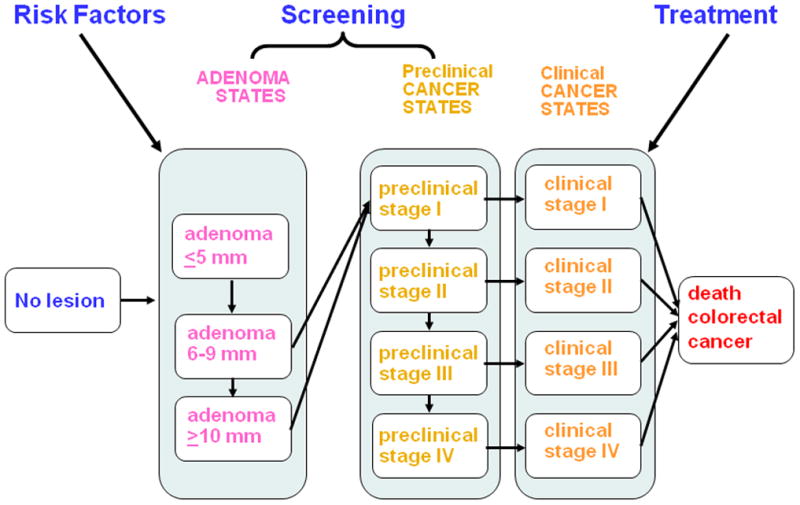
Natural History and Interventions on colorectal Cancer
The MISCAN-Colon model includes risk factors that can increase risk for CRC: smoking, obesity, and red meat consumption; and factors that may decrease risk for CRC: aspirin use, multivitamin use including supplemental folate and calcium, and physical activity. We modeled the impact of the risk factors by using the relative risk for adenomas associated with each factor in conjunction with the prevalence of the factor over time in the population, as has been described29 (http://cisnet.cancer.gov/projections/colorectal). Prevalence rates were obtained primarily from the Cancer Progress Report.37 We assumed a smoking rate of 42% in 1965, 23% in 2000, and a projected rate of 11% to 17% in 2020 depending on the future scenario. We assumed an obesity rate of 13% in 1965, 31% in 2000, and a projected rate of 34% to 45% in 2020. For CRC screening uptake, we used National Health Interview Survey (NHIS)38 data from 1987, 1992, 1998, and 2000 to estimate screening test rates for fecal occult blood testing (FOBT) for persons 50 and older who have had FOBT within past 2 years) and endoscopy (including flexible sigmoidoscopy and colonoscopy) for persons 50 and older who have had a sigmoidoscopy or colonoscopy (collectively known as endoscopy) at some point in their life, by 5-year age groups, and applied both screening rates and sensitivity and specificity of each screening test to the model. CRC screening rates by 5-year age groups were calculated separately for home-based FOBT and endoscopy (including proctoscopy, flexible sigmoidoscopy and colonoscopy). The NHIS did not distinguish between home-based FOBT and office-based FOBT or type of endoscopy prior to the 2000 survey. Since office-based FOBT is not an effective method for CRC screening,39 the proportion of home-based FOBT in 2000 was applied to the earlier years of data to calculate FOBT prevalence. Similarly, the proportions of endoscopies that were sigmoidoscopies and colonoscopies were derived from the 2000 data and applied to earlier years. For 2000, we assumed CRC screening rates with FOBT of 24% and endoscopy of 39% and a projected increase in screening rates in 2020: FOBT prevalence of 35% to 38%; endoscopy prevalence of 56% to 61% (Supplemental Table 1). We assumed no CRC screening prior to 1978.
To assess the effects of treatment, the model distinguished 4 chemotherapy regimens for stages III–IV CRC depending on the treatment available to U.S. patients diagnosed in different periods. These regimens were 1) 5-fluorouracil (available before 1996); 2) 5-fluorouracil and irinotecan (available 1996–2001); 3) 5-fluorouracil, irinotecan, and oxaliplatin (2002–2003); and 4) 5-fluorouracil + irinotecan + oxaliplatin + bevacizumab/cetuximab (2004 and afterwards). Hazard ratios for disease-free survival were obtained from published clinical trials for each of the treatment regimens40–52 and applied to the 1975–1979 stage-specific relative survival rates from SEER 9. Chemotherapy use by age and time for the U.S. population, were based on the SEER-Medicare linked database,53 survey data and patterns of care studies.54–55 We assumed increasing CRC treatment rates over time, with a projected rate of 8% in 2005 and 45% to 83% by 2020 being treated with combination therapy, including 5-FU, irinotecan, oxaliplatin, and biologics.
The key long-term outcomes measured in the MISCAN-Colon model are the change in CRC incidence and death rates as a result of the changes in risk factors, screening, and treatment in past and future time periods. To project future trends,29 we considered three hypothetical scenarios, including frozen trends (risk factor, screening and treatment rates plateau at year 2000); continued trends (risk factor, screening and treatment rates continue to increase annually at current rate); and optimistic trends where all three interventions of risk factors, screening and treatment improved at a rate that was considered optimistic but realistic.29 The prevalence assumptions of these factors from 1965–2000 as observed, and 2000 to 2020 as projected under each scenario are presented at www.seer.gov/report_to_nation/1975-2006 in Supplemental Table 1 and previous work.29
RESULTS
Long-Term Incidence Trends for All Races Combined, 1975–2006
Overall cancer incidence rates for all racial/ethnic groups combined decreased by 0.7% per year during 1999–2006 for both sexes combined, by 1.3% per year during 2000–2006 for men, and by 0.5% per year during 1998–2006 for women (Table 1). Trends during the most recent periods (last joinpoint segments), along with AAPCs for the most recent 5 years (2002–2006) and 10 years (1997–2006), are presented for the top 15 cancers by sex. Among men, rates decreased for cancers of the prostate, lung and bronchus (lung), oral cavity and pharynx (oral cavity), stomach, brain and other nervous system (brain), and for CRC. In contrast, rates increased for cancers of the kidney and renal pelvis (kidney), liver and intrahepatic bile duct (liver), and esophagus and for leukemia, myeloma, and melanoma of the skin (melanoma). Among women, incidence rates decreased during the most recent joinpoint segments for 6 of the top 15 cancers (i.e., breast, CRC, uterine corpus and uterus not otherwise specified [uterus], ovary, cervix uteri [cervix], and oral cavity). In contrast, rates increased for 8 of the top 15 cancers (i.e., lung, thyroid, pancreas, urinary bladder [bladder], kidney, non-Hodgkin lymphoma [NHL], melanoma, and leukemia) in women.
Table 1.
SEER Cancer Incidence Rate Trends With Joinpoint Analyses (Up to 4 Joinpoints Allowed) for 1975–2006 for the Top 15 Cancers, by Sex, for All Racesa
| Joinpoint analyses (1975–2006)b | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trend 1 | Trend 2 | Trend 3 | Trend 4 | Trend 5 | AAPCf | |||||||
| Sex/cancer site or type | Years | APCe | Years | APCe | Years | APCe | Years | APCe | Years | APCe | 1997–2006 | 2002–2006 |
| All sitesc | ||||||||||||
| Both sexes | 1975–1989 | 1.2g | 1989–1992 | 2.8g | 1992–1995 | −2.4 | 1995–1999 | 1.0 | 1999–2006 | −1.1g | −0.6h | −1.1h |
| (Delay-adjusted) | 1975–1989 | 1.2g | 1989–1992 | 2.8 | 1992–1995 | −2.4 | 1995–1999 | 0.9 | 1999–2006 | −0.7g | −0.4h | −0.7h |
| Males | 1975–1989 | 1.3g | 1989–1992 | 5.1g | 1992–1995 | −4.8g | 1995–2001 | 0.3 | 2001–2006 | −1.9g | −0.9h | −1.9h |
| (Delay-adjusted) | 1975–1989 | 1.3g | 1989–1992 | 5.2g | 1992–1995 | −4.9g | 1995–2000 | 0.5 | 2000–2006 | −1.3g | −0.7h | −1.3h |
| Females | 1975–1979 | −0.3 | 1979–1987 | 1.6g | 1987–1995 | 0.1 | 1995–1998 | 1.5 | 1998–2006 | −0.8g | −0.5h | −0.8h |
| (Delay-adjusted) | 1975–1979 | −0.3 | 1979–1987 | 1.6g | 1987–1995 | 0.1 | 1995–1998 | 1.4 | 1998–2006 | −0.5g | −0.3 | −0.5h |
| Top 15 cancers for malesd | ||||||||||||
| Prostate | 1975–1988 | 2.6g | 1988–1992 | 16.4g | 1992–1995 | −11.4g | 1995–2001 | 1.8 | 2001–2006 | −3.4g | −1.1 | −3.4h |
| (Delay-adjusted) | 1975–1988 | 2.6g | 1988–1992 | 16.5g | 1992–1995 | −11.7g | 1995–2000 | 2.4 | 2000–2006 | −2.4g | −0.8 | −2.4h |
| Lung and bronchus | 1975–1982 | 1.4g | 1982–1991 | −0.4 | 1991–2006 | −1.9g | −1.9h | −1.9h | ||||
| (Delay-adjusted) | 1975–1982 | 1.4g | 1982–1991 | −0.4 | 1991–2006 | −1.8g | −1.8h | −1.8h | ||||
| Colon and rectum | 1975–1986 | 1.1g | 1986–1995 | −2.1g | 1995–1998 | 1.1 | 1998–2004 | −2.6g | 2004–2006 | −5.7g | −2.9h | −4.2h |
| (Delay-adjusted) | 1975–1985 | 1.1g | 1985–1991 | −1.2g | 1991–1995 | −3.2g | 1995–1998 | 2.1 | 1998–2006 | −3.0g | −2.5h | −3.0h |
| Urinary bladder | 1975–1987 | 1.0g | 1987–1996 | −0.5 | 1996–1999 | 1.8 | 1999–2006 | −0.8g | −0.2 | −0.8h | ||
| (Delay-adjusted) | 1975–1987 | 0.9g | 1987–2006 | 0.0 | 0.0 | 0.0 | ||||||
| Melanoma of the skin | 1975–1986 | 5.5g | 1986–2006 | 2.9g | 2.9h | 2.9h | ||||||
| (Delay-adjusted) | 1975–1986 | 5.4g | 1986–2006 | 3.1g | 3.1h | 3.1h | ||||||
| Non-Hodgkin lymphoma | 1975–1991 | 4.3g | 1991–2006 | 0.1 | 0.1 | 0.1 | ||||||
| (Delay-adjusted) | 1975–1991 | 4.2g | 1991–2006 | 0.3 | 0.3 | 0.3 | ||||||
| Kidney and renal pelvis | 1975–2006 | 1.7g | 1.7h | 1.7h | ||||||||
| (Delay-adjusted) | 1975–2006 | 1.8g | 1.8h | 1.8h | ||||||||
| Leukemia | 1975–2004 | −0.1 | 2004–2006 | −6.6 | −1.6h | −3.4 | ||||||
| (Delay-adjusted) | 1975–2006 | 0.1g | 0.1h | 0.1h | ||||||||
| Oral cavity and pharynx | 1975–1983 | −0.2 | 1983–2006 | −1.4g | −1.4h | −1.4h | ||||||
| (Delay-adjusted) | 1975–2006 | −1.2g | −1.2h | −1.2h | ||||||||
| Pancreas | 1975–1993 | −0.9g | 1993–2006 | 0.3 | 0.3 | 0.3 | ||||||
| (Delay-adjusted) | 1975–1981 | −1.8g | 1981–1985 | 1.1 | 1985–1990 | −2.1 | 1990–2003 | 0.1 | 2003–2006 | 2.5 | 0.9 | 1.9 |
| Stomach | 1975–1988 | −1.2g | 1988–2006 | −2.0g | −2.0h | −2.0h | ||||||
| (Delay-adjusted) | 1975–1988 | −1.2g | 1988–2006 | −2.0g | −2.0h | −2.0h | ||||||
| Liver and intrahepatic bile duct | 1975–1986 | 2.1g | 1986–1996 | 4.9g | 1996–2006 | 2.6g | 2.6h | 2.6h | ||||
| (Delay-adjusted) | 1975–2006 | 3.6g | 3.6h | 3.6h | ||||||||
| Esophagus | 1975–2006 | 0.7g | 0.7h | 0.7h | ||||||||
| (Delay-adjusted) | 1975–2006 | 0.7g | 0.7h | 0.7h | ||||||||
| Brain and other nervous system | 1975–1991 | 1.1g | 1991–2006 | −0.7g | −0.7h | −0.7h | ||||||
| (Delay-adjusted) | 1975–1991 | 1.0g | 1991–2006 | −0.5g | −0.5h | −0.5h | ||||||
| Myeloma | 1975–2002 | 0.8g | 2002–2006 | −3.0 | −0.9 | −3.0 | ||||||
| (Delay-adjusted) | 1975–2006 | 0.7g | 0.7h | 0.7h | ||||||||
| Top 15 cancers for femalesd | ||||||||||||
| Breast | 1975–1980 | −0.5 | 1980–1987 | 4.0g | 1987–1994 | −0.2 | 1994–1999 | 1.6g | 1999–2006 | −2.2g | −1.3h | −2.2h |
| (Delay-adjusted) | 1975–1980 | −0.5 | 1980–1987 | 4.0g | 1987–1994 | −0.1 | 1994–1999 | 1.6g | 1999–2006 | −2.0g | −1.2h | −2.0h |
| Lung and bronchus | 1975–1982 | 5.5g | 1982–1990 | 3.5g | 1990–1998 | 1.0g | 1998–2006 | −0.1 | 0.0 | −0.1 | ||
| (Delay-adjusted) | 1975–1982 | 5.6g | 1982–1991 | 3.4g | 1991–2006 | 0.4g | 0.4h | 0.4h | ||||
| Colon and rectum | 1975–1985 | 0.3 | 1985–1995 | −1.9g | 1995–1998 | 2.0 | 1998–2006 | −2.4g | −1.9h | −2.4h | ||
| (Delay-adjusted) | 1975–1985 | 0.3 | 1985–1995 | −1.8g | 1995–1998 | 1.9 | 1998–2006 | −2.2g | −1.7h | −2.2h | ||
| Corpus and uterus, NOS | 1975–1979 | −6.0g | 1979–1988 | −1.7g | 1988–1997 | 0.7g | 1997–2006 | −0.6g | −0.6h | −0.6h | ||
| (Delay-adjusted) | 1975–1979 | −6.0g | 1979–1988 | −1.7g | 1988–1997 | 0.7g | 1997–2006 | −0.5g | −0.5h | −0.5h | ||
| Melanoma of the skin | 1975–1980 | 5.6g | 1980–2006 | 2.4g | 2.4h | 2.4h | ||||||
| (Delay-adjusted) | 1975–1981 | 5.7g | 1981–1993 | 1.9g | 1993–2006 | 3.0g | 3.0h | 3.0h | ||||
| Non-Hodgkin lymphoma | 1975–1990 | 2.8g | 1990–2004 | 1.2g | 2004–2006 | −2.5 | 0.3 | −0.7 | ||||
| (Delay-adjusted) | 1975–1990 | 2.9g | 1990–2006 | 1.1g | 1.1h | 1.1h | ||||||
| Thyroid | 1975–1977 | 6.5 | 1977–1980 | −5.3 | 1980–1995 | 2.3g | 1995–2006 | 6.0g | 6.0h | 6.0h | ||
| (Delay-adjusted) | 1975–1977 | 6.5 | 1977–1980 | −5.3 | 1980–1995 | 2.3g | 1995–2006 | 6.3g | 6.3h | 6.3h | ||
| Ovaryc | 1975–1985 | 0.1 | 1985–2001 | −0.7g | 2001–2006 | −2.6g | −1.8h | −2.6h | ||||
| (Delay-adjusted)c | 1975–1985 | 0.1 | 1985–2001 | −0.7g | 2001–2006 | −2.1g | −1.5h | −2.1h | ||||
| Pancreas | 1975–1984 | 1.5g | 1984–1995 | −0.6 | 1995–2006 | 0.6g | 0.6h | 0.6h | ||||
| (Delay-adjusted) | 1975–1984 | 1.3g | 1984–2000 | −0.3 | 2000–2006 | 1.7g | 1.0h | 1.7h | ||||
| Leukemia | 1975–2006 | 0.0 | 0.0 | 0.0 | ||||||||
| (Delay-adjusted) | 1975–2006 | 0.3g | 0.3h | 0.3h | ||||||||
| Kidney and renal pelvis | 1975–2006 | 2.3g | 2.3h | 2.3h | ||||||||
| (Delay-adjusted) | 1975–2006 | 2.4g | 2.4h | 2.4h | ||||||||
| Urinary bladder | 1975–2003 | 0.2g | 2003–2006 | −2.3 | −0.6 | −1.7 | ||||||
| (Delay-adjusted) | 1975–2006 | 0.2g | 0.2h | 0.2h | ||||||||
| Cervix uteri | 1975–1981 | −4.6g | 1981–1996 | −1.1g | 1996–2006 | −3.6g | −3.6h | −3.6h | ||||
| (Delay-adjusted) | 1975–1981 | −4.6g | 1981–1996 | −1.1g | 1996–2006 | −3.5g | −3.5h | −3.5h | ||||
| Oral cavity and pharynx | 1975–1980 | 2.6g | 1980–2006 | −1.0g | −1.0h | −1.0h | ||||||
| (Delay-adjusted) | 1975–1980 | 2.5 | 1980–2006 | −0.9g | −0.9h | −0.9h | ||||||
| Brain and other nervous system | 1975–1987 | 1.6g | 1987–2006 | −0.3 | −0.3 | −0.3 | ||||||
| (Delay-adjusted) | 1975–1987 | 1.6g | 1987–2006 | −0.1 | −0.1 | −0.1 | ||||||
SEER: Surveillance, Epidemiology and End Results; APC: annual percent change; NOS: not otherwise specified.
Source: SEER 9 areas covering about 10% of the U.S. population (Connecticut, Hawaii, Iowa, Utah, and New Mexico, and the metropolitan areas of San Francisco, Detroit, Atlanta, and Seattle-Puget Sound).
Joinpoint analyses with up to four joinpoints are based on rates per 100,000 persons and were age-adjusted to the 2000 U.S. standard population (19 age groups Census p25–1130). Joinpoint (JP) Regression Program, Version 3.3.1. April 2008, National Cancer Institute.
All sites excludes myelodysplastic syndromes and borderline tumors; ovary excludes borderline tumors.
The top 15 cancers were selected based on the sex-specific age-adjusted incidence rates for 2002–2006 for all races combined and are listed in rank order.
APC is based on rates that were age-adjusted to the 2000 U.S. standard population (19 age groups Census p25–1130).
The AAPC is the Average Annual Percent Change and is a weighted average of the APCs calculated by Joinpoint.
APC is statistically significantly different from zero (2-sided P < .05).
AAPC is statistically significantly different from zero.
Based on long-term trends (1975–2006), the AAPCs for the most recent 5-years, 2002–2006, were similar to the APCs for the most recent joinpoint segment (time period) (Table 1). As expected, when the incidence trend fluctuated over time, the 10-year (1997–2006) AAPCs differed from the most recent APCs, e.g., all sites combined for men and women, and cancers of the prostate, pancreas and CRC in men, and cancers of the breast, pancreas, uterus, and CRC in women. Specifically, the 10-year AAPC (1997–2006) for prostate cancer showed a small non-significant increase which reflected a non-significant increase during 1995–2000 attenuated by a more recent significant 2.4% decline observed over the period 2000–2006. Similarly, breast cancer incidence in women began to decline at the turn of the century after an increase in the latter part of the 1990s (1994–1999). The 10-year breast cancer AAPC for 1997–2006 was a smaller decline of 1.2% per year rather than the more recent annual decrease of 2.0% each year over the period of 1999–2006.
Long-Term Mortality Trends for All Races Combined, 1975–2006
Death rates for all cancers combined have decreased since the early 1990s for both men and women (Table 2). The decreases were slightly larger for men, who had declines of 1.5% per year during 1993–2001 and 2.0% per year during 2001–2006, compared with women, whose cancer death rates declined 0.8% per year during 1994–2002 and 1.5% per year during 2000–2006. Among the top 15 leading causes of cancer death, mortality decreased during the most recent period for the following sites: CRC, stomach, kidney, brain, leukemia, NHL, and myeloma in both men and women; lung, prostate, and oral cavity in men; and breast, ovary, and bladder in women. Cancers with increasing mortality during the most recent period include melanoma and esophageal cancer in men, pancreatic cancer in women, and liver cancer in both men and women.
Table 2.
U.S. Death Rate Trends With Joinpoint Analyses (Up to 4 Joinpoints Allowed) for 1975–2006 for the Top 15 Cancers, by Sex, for All Racesa
| Joinpoint analyses (1975–2006)b | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trend 1 | Trend 2 | Trend 3 | Trend 4 | Trend 5 | AAPCe | |||||||
| Sex/cancer site or type | Years | APCd | Years | APCd | Years | APCd | Years | APCd | Years | APCd | 1997–2006 | 2002–2006 |
| All sites | ||||||||||||
| Both sexes | 1975–1990 | 0.5f | 1990–1993 | −0.3 | 1993–2001 | −1.1f | 2001–2006 | −1.6f | −1.4g | −1.6g | ||
| Males | 1975–1979 | 1.0f | 1979–1990 | 0.3f | 1990–1993 | −0.5 | 1993–2001 | −1.5f | 2001–2006 | −2.0f | −1.8g | −2.0g |
| Females | 1975–1990 | 0.6f | 1990–1994 | −0.1 | 1994–2002 | −0.8f | 2002–2006 | −1.5f | −1.1g | −1.5g | ||
| Top 15 cancers for malesc | ||||||||||||
| Lung and bronchus | 1975–1978 | 2.5f | 1978–1984 | 1.2f | 1984–1990 | 0.4f | 1990–1994 | −1.3f | 1994–2006 | −2.0f | −2.0g | −2.0g |
| Prostate | 1975–1987 | 0.9f | 1987–1991 | 3.0f | 1991–1994 | −0.6 | 1994–2006 | −4.1f | −4.1g | −4.1g | ||
| Colon and rectum | 1975–1984 | −0.1 | 1984–1990 | −1.4f | 1990–2002 | −2.0f | 2002–2006 | −3.9f | −2.9g | −3.9g | ||
| Pancreas | 1975–1986 | −0.9f | 1986–2003 | −0.2f | 2003–2006 | 1.0 | 0.2 | 0.7 | ||||
| Leukemia | 1975–1995 | −0.2f | 1995–2006 | −0.8f | −0.8g | −0.8g | ||||||
| Non-Hodgkin lymphoma | 1975–1991 | 2.7f | 1991–1997 | 1.7f | 1997–2006 | −3.0f | −3.0g | −3.0g | ||||
| Esophagus | 1975–1985 | 0.7f | 1985–1994 | 1.2f | 1994–2006 | 0.4f | 0.4g | 0.4g | ||||
| Urinary bladder | 1975–1983 | −1.4f | 1983–1987 | −2.7f | 1987–1993 | 0.1 | 1993–2003 | −0.6f | 2003–2006 | 0.7 | −0.2 | 0.4 |
| Liver and intrahepatic bile duct | 1975–1979 | 0.3 | 1979–1987 | 2.3f | 1987–1996 | 3.9f | 1996–1999 | 0.5 | 1999–2006 | 2.4f | 2.0g | 2.4g |
| Kidney and renal pelvis | 1975–1991 | 1.1f | 1991–2002 | −0.1 | 2002–2006 | −1.5f | −0.7g | −1.5g | ||||
| Stomach | 1975–1994 | −2.1f | 1994–2006 | −3.7f | −3.7g | −3.7g | ||||||
| Brain and other nervous system | 1975–1977 | 4.4 | 1977–1982 | −0.4 | 1982–1991 | 1.3f | 1991–2006 | −1.0f | −1.0g | −1.0g | ||
| Myeloma | 1975–1994 | 1.5f | 1994–2006 | −1.1f | −1.1g | −1.1g | ||||||
| Oral cavity and pharynx | 1975–1980 | −0.9 | 1980–2006 | −2.2f | −2.2g | −2.2g | ||||||
| Melanoma of the skin | 1975–1987 | 2.4f | 1987–1998 | 0.7f | 1998–2002 | −1.5 | 2002–2006 | 2.0f | 0.3 | 2.0g | ||
| Top 15 cancers for femalesc | ||||||||||||
| Lung and bronchus | 1975–1982 | 6.0f | 1982–1990 | 4.2f | 1990–1995 | 1.7f | 1995–2003 | 0.3f | 2003–2006 | −0.9 | −0.1 | −0.6 |
| Breast | 1975–1990 | 0.4f | 1990–1995 | −1.8f | 1995–1998 | −3.3f | 1998–2006 | −1.9f | −2.0g | −1.9g | ||
| Colon and rectum | 1975–1984 | −1.0f | 1984–2001 | −1.8f | 2001–2006 | −3.4f | −2.7g | −3.4g | ||||
| Pancreas | 1975–1984 | .8f | 1984–2006 | 0.1f | 0.1g | 0.1g | ||||||
| Ovary | 1975–1982 | −1.2f | 1982–1992 | 0.3f | 1992–1998 | −1.2f | 1998–2002 | 0.7 | 2002–2006 | −1.4f | −0.4 | −1.4g |
| Non-Hodgkin lymphoma | 1975–1997 | 2.1f | 1997–2006 | −3.7f | −3.7g | −3.7g | ||||||
| Leukemia | 1975–1980 | 0.7 | 1980–2000 | −0.4f | 2000–2006 | −1.6f | −1.2g | −1.6g | ||||
| Corpus and uterus, NOS | 1975–1992 | −1.5f | 1992–2006 | 0.0 | 0.0 | 0.0 | ||||||
| Brain and other nervous system | 1975–1992 | 1.0f | 1992–2006 | −1.1f | −1.1g | −1.1g | ||||||
| Liver and intrahepatic bile duct | 1975–1978 | −1.5 | 1978–1988 | 1.4f | 1988–1995 | 4.0f | 1995–2000 | 0.2 | 2000–2006 | 1.8f | 1.3g | 1.8g |
| Myeloma | 1975–1993 | 1.5f | 1993–2001 | −0.4 | 2001–2006 | −2.4f | −1.5g | −2.4g | ||||
| Stomach | 1975–1987 | −2.8 f | 1987–1990 | −0.3 | 1990–2006 | −2.7f | −2.7g | −2.7g | ||||
| Kidney and renal pelvis | 1975–1992 | 1.3f | 1992–2006 | −0.6f | −0.6g | −0.6g | ||||||
| Cervix uteri | 1975–1982 | −4.4f | 1982–1996 | −1.6f | 1996–2003 | −3.8f | 2003–2006 | −0.7 | −2.8g | 1.5 | ||
| Urinary bladder | 1975–1986 | −1.7f | 1986–2006 | −0.4f | −0.4g | −0.4g | ||||||
APC: annual percent change; NOS: not otherwise specified.
Source: National Center for Health Statistics public-use data file for the total U.S.
Joinpoint analyses with up to 4 joinpoints are based on rates per 100,000 persons and were age-adjusted to the 2000 U.S. standard population (19 age groups–Census p25–1130). Joinpoint (JP) Regression Program, Version 3.2.0. January 2008, National Cancer Institute.
The top 15 cancers were selected based on the sex-specific age-adjusted death rates for 2001–2005 for all races combined and listed in rank order.
APC is based on rates that were age-adjusted to the 2000 U.S. standard population (19 age groups – Census p25–1130).
The AAPC is the Average Annual Percent Change and is a weighted average of the APCs calculated by Joinpoint.
APC is statistically significantly different from zero (2-sided P < .05).
AAPC is statistically significantly different from zero.
Similar to incidence trends, the AAPCs in death rates for 2002–2006 were generally similar to the APCs for the most recent joinpoint period. However, the use of long-term trends can often mask changes over the shorter term. Differences in the 5-year and 10-year AAPCs typically identify types of cancer where the 10-year trend may mask important recent changes. Some examples are the accelerated rate of decline for CRC mortality for men and for women and the recent shift to increasing mortality in melanoma among men.
Cancer Incidence Rates, 2002–2006, and Short-Term Fixed-Interval Trends by Race/Ethnicity, 1997–2006
For all cancer sites combined, for both men and women by race/ethnicity, black men had the highest incidence rate during 2002–2006 (Table 3). For men in each population group, the highest incidence rates were observed for prostate cancer, followed by lung cancer and CRC, except among Hispanic men, whose rate for CRC was slightly higher than for lung cancer. Except for these 3 sites, the rank order of the top 15 cancers varied considerably among the racial/ethnic groups. Among women, non-Hispanic women and white women had the highest and second highest, respectively, overall incidence rates during 2002–2006. It should be noted that non-Hispanic and white are not mutually exclusive population categories. The most common cancer site for all women, regardless of race/ethnicity, was breast cancer. Lung cancer was the second most common cancer and CRC ranked third for all races combined and for white, non-Hispanic, and AI/AN women. However, for black, API, and Hispanic women, CRC ranked second and lung cancer ranked third. For all women, cancer of the uterus ranked fourth.
Table 3.
Incidence Rates for 2002–2006 and Fixed-Interval Trends for 1997–2006 for the Top 15 Cancersb by Sex, Race, and Ethnicity, Selected Areas in the United Statesa
| All races/ethnicities | Whitec | Blackc | APIc | AI/AN (CHSDA Counties) c | Hispanicc | Non-Hispanicc | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex/cancer site or typeb | Rank | Rated | AAPCe | Rank | Rated | AAPCe | Rank | Rated | AAPCe | Rank | Rated | AAPCe | Rank | Rated | AAPCe | Rank | Rated | AAPCe | Rank | Rated | AAPCe |
| Males | |||||||||||||||||||||
| All sitesf | 556.5 | −0.9g | 550.1 | −0.9g | 626.0 | −1.8g | 334.5 | −1.6g | 441.2 | −1.5g | 430.3 | −1.3g | 567.7 | −0.8g | |||||||
| Prostate | 1 | 155.5 | −0.9 | 1 | 146.3 | −1.1 | 1 | 231.9 | −1.9g | 1 | 82.3 | −1.3 | 1 | 108.8 | −3.0 | 1 | 131.1 | −1.7g | 1 | 157.7 | −0.8 |
| Lung and bronchus | 2 | 86.4 | −2.0g | 2 | 85.9 | −1.8g | 2 | 104.8 | −2.7g | 2 | 50.6 | −2.0g | 2 | 78.0 | −3.2g | 3 | 49.2 | −2.5g | 2 | 89.4 | −1.9g |
| Colon and rectum | 3 | 59.0 | −2.7g | 3 | 58.2 | −2.7g | 3 | 68.4 | −2.1g | 3 | 44.1 | −2.4g | 3 | 55.0 | −2.9g | 2 | 50.0 | −1.3g | 3 | 59.8 | −2.7g |
| Urinary bladder | 4 | 37.9 | −0.5g | 4 | 40.1 | −0.5g | 5 | 18.6 | −0.6g | 6 | 15.4 | 0.2 | 5 | 19.1 | 0.2 | 4 | 21.1 | −0.7g | 4 | 39.2 | −0.4g |
| Non-Hodgkin lymphoma | 5 | 23.1 | 0.1 | 6 | 23.7 | 0.2 | 7 | 16.8 | −0.5 | 7 | 14.5 | −1.5g | 6 | 16.6 | 0.7 | 5 | 19.8 | −0.5 | 6 | 23.4 | 0.2 |
| Melanoma of the skin | 6 | 22.6 | 2.7g | 5 | 24.9 | 2.7g | 26 | 1.1 | −3.5 | 19 | 1.6 | 0.6 | 13 | 6.9 | 2.6 | 16 | 4.5 | 0.2 | 5 | 24.4 | 3g |
| Kidney and renal pelvis | 7 | 19.6 | 2.5g | 7 | 19.7 | 2.6g | 4 | 20.6 | 2.7g | 10 | 9.0 | 2.0g | 4 | 24.5 | 2.3g | 6 | 18.2 | 2.1g | 7 | 19.7 | 2.7g |
| Leukemia | 8 | 16.0 | −0.6 | 8 | 16.4 | −0.5 | 12 | 12.1 | −1.1g | 11 | 8.5 | −1.7 | 10 | 11.9 | −1.3 | 9 | 11.9 | −1.0g | 9 | 16.2 | −0.5 |
| Oral cavity and pharynx | 9 | 16.0 | −1.1g | 9 | 15.9 | −0.7g | 6 | 16.9 | −3.2g | 8 | 10.6 | −2.2g | 8 | 13.1 | −4.3g | 11 | 10.5 | −3.0g | 8 | 16.6 | −0.6g |
| Pancreas | 10 | 13.1 | 0.5g | 10 | 12.9 | 0.6g | 9 | 16.4 | −0.2 | 9 | 9.5 | −0.4 | 11 | 10.5 | 1.6 | 10 | 11.3 | −0.2 | 10 | 13.2 | 0.6g |
| Stomach | 11 | 10.0 | −2.7g | 11 | 8.9 | −2.6g | 8 | 16.7 | −2.8g | 5 | 17.5 | −3.1g | 7 | 14.7 | 0.3 | 8 | 14.3 | −3.2g | 11 | 9.6 | −2.9g |
| Liver and intrahepatic bile duct | 12 | 9.1 | 3.4g | 14 | 8.0 | 3.4g | 11 | 12.5 | 4.0g | 4 | 21.4 | −0.5 | 9 | 12.9 | 1.5 | 7 | 15.9 | 2.5g | 13 | 8.5 | 3.2g |
| Esophagus | 13 | 8.6 | 0.2 | 12 | 8.6 | 1.0g | 14 | 10.4 | −5.4g | 13 | 4.0 | −2.0 | 12 | 6.9 | −5.0 | 15 | 5.5 | −1.5g | 12 | 8.8 | 0.4 |
| Brain and other nervous system | 14 | 7.9 | −0.5g | 13 | 8.4 | −0.4g | 15 | 4.7 | −0.8 | 14 | 3.9 | −2.1g | 16 | 5.0 | 1.1 | 13 | 6.2 | −0.8g | 14 | 8.1 | −0.5g |
| Larynx | 15 | 7.1 | −3.0g | 15 | 6.9 | −2.8g | 13 | 11.2 | −3.0g | 17 | 2.6 | −5.5g | 14 | 6.2 | −2.1 | 14 | 6.0 | −4.0g | 15 | 7.2 | −2.9g |
| Myeloma | 16 | 7.0 | −0.3 | 16 | 6.5 | −0.1 | 10 | 13.3 | −0.3 | 15 | 3.8 | −2.3 | 15 | 6.0 | −5.6g | 12 | 6.5 | −0.2 | 16 | 7.1 | 0.0 |
| Thyroid | 18 | 4.9 | 5.8g | 18 | 5.1 | 5.9g | 19 | 2.6 | 4.7g | 12 | 4.3 | 4.3g | 18 | 3.0 | h | 18 | 3.8 | 4.7g | 18 | 5.0 | 6.0g |
| Females | |||||||||||||||||||||
| All sitesf | 414.8 | −0.5g | 420.0 | −0.5g | 389.5 | −0.4g | 276.3 | −0.5g | 369.3 | −0.3 | 326.8 | −0.6g | 422.9 | −0.4g | |||||||
| Breast | 1 | 121.8 | −1.5g | 1 | 123.5 | −1.6g | 1 | 113.0 | −0.5g | 1 | 81.6 | −0.3 | 1 | 91.7 | −1.5g | 1 | 90.2 | −0.9g | 1 | 124.7 | −1.4g |
| Lung and bronchus | 2 | 55.5 | 0.1 | 2 | 57.1 | 0.2g | 3 | 50.7 | 0.1 | 3 | 27.6 | −0.7 | 2 | 56.1 | 1.0 | 3 | 26.5 | −0.7g | 2 | 57.9 | 0.3g |
| Colon and rectum | 3 | 43.6 | −2.0g | 3 | 42.6 | −2.2g | 2 | 51.7 | −1.4g | 2 | 33.1 | −1.4g | 3 | 44.7 | −1.8 | 2 | 35.1 | −1.6g | 3 | 44.2 | −2.0g |
| Corpus and uterus, NOS | 4 | 23.6 | −0.1 | 4 | 24.1 | −0.3 | 4 | 20.8 | 1.3g | 4 | 15.4 | 1.4g | 4 | 19.5 | 0.4 | 4 | 19.1 | 0.8g | 4 | 24.0 | −0.2 |
| Non-Hodgkin lymphoma | 5 | 16.3 | −0.2 | 5 | 16.8 | −0.1 | 6 | 11.4 | 0.3 | 6 | 10.4 | −1.2 | 6 | 14.7 | −0.1 | 5 | 14.8 | −0.2 | 5 | 16.4 | −0.1 |
| Melanoma of the skin | 6 | 14.6 | 3.2g | 6 | 16.5 | 3.3g | 28 | 1.0 | −0.2 | 21 | 1.3 | 0.7 | 17 | 4.9 | h | 17 | 4.3 | 0.8 | 6 | 15.9 | 3.6g |
| Thyroid | 7 | 14.2 | 7.4g | 7 | 14.8 | 7.4g | 11 | 8.7 | 6.9g | 5 | 14.5 | 5.5g | 9 | 9.6 | 3.8g | 6 | 13.8 | 6.4g | 7 | 14.3 | 7.5g |
| Ovaryf | 8 | 13.0 | −1.7g | 8 | 13.5 | −1.7g | 9 | 9.9 | −2.4 | 8 | 9.3 | −1.7g | 7 | 11.2 | −3.2 | 8 | 11.3 | −0.9g | 8 | 13.2 | −1.7g |
| Kidney and renal pelvis | 9 | 10.2 | 3.1g | 9 | 10.3 | 3.2g | 8 | 10.6 | 2.8g | 14 | 4.5 | 2.9g | 5 | 15.6 | 4.3g | 9 | 10.3 | 2.5g | 10 | 10.2 | 3.1g |
| Pancreas | 10 | 10.2 | 0.7g | 11 | 9.9 | 0.8g | 5 | 13.5 | 0.0 | 10 | 7.8 | −0.1 | 8 | 10.2 | 0.3 | 10 | 9.7 | −0.1 | 9 | 10.2 | 0.7g |
| Leukemia | 11 | 9.6 | −0.4 | 12 | 9.9 | −0.4 | 13 | 7.5 | −1.1 | 12 | 5.7 | −1.2g | 11 | 7.7 | 2.2 | 12 | 8.2 | −1.0g | 12 | 9.6 | −0.3 |
| Urinary bladder | 12 | 9.6 | −0.6g | 10 | 10.1 | −0.6g | 14 | 6.9 | −0.4 | 15 | 3.8 | −1.2 | 16 | 5.1 | 2.2 | 14 | 5.5 | −1.3 | 11 | 9.9 | −0.4 |
| Cervix uteri | 13 | 8.3 | −3.1g | 13 | 7.9 | −2.8g | 7 | 11.1 | −4.4g | 11 | 7.6 | −4.4g | 10 | 9.4 | −1.6 | 7 | 12.7 | −4.0g | 13 | 7.8 | −3.1g |
| Oral cavity and pharynx | 14 | 6.1 | −1.0g | 14 | 6.1 | −0.9g | 15 | 5.5 | −2.1g | 13 | 5.2 | −1.1 | 14 | 5.6 | 0.1 | 18 | 3.9 | −1.7g | 14 | 6.3 | −0.8g |
| Brain and other nervous system | 15 | 5.7 | −0.5g | 15 | 6.1 | −0.5g | 17 | 3.6 | −0.4 | 16 | 3.1 | 0.4 | 19 | 3.7 | −0.3 | 16 | 4.8 | −1.3g | 15 | 5.8 | −0.3 |
| Stomach | 16 | 4.9 | −1.4g | 16 | 4.2 | −1.5g | 12 | 8.5 | −2.1g | 7 | 9.8 | −3.4g | 12 | 7.3 | −3.2g | 11 | 8.6 | −1.4g | 17 | 4.6 | −1.7g |
| Myeloma | 17 | 4.6 | −0.9g | 17 | 4.1 | −1.1g | 10 | 9.6 | −0.7g | 17 | 2.7 | −2.4g | 15 | 5.2 | −2.3 | 15 | 4.8 | −1.6 | 16 | 4.6 | −0.9g |
| Liver and intrahepatic bile duct | 18 | 3.1 | 1.5g | 18 | 2.8 | 1.1g | 16 | 3.8 | 1.9g | 9 | 8.1 | 0.0 | 13 | 6.8 | 6.3g | 13 | 6.2 | 1.2g | 18 | 2.9 | 1.1g |
API indicates Asian/Pacific Islander; AI/AN, American Indian/Alaska Native; HIS, Indian Health Service; CHSDA, IHS Contract Health Services Delivery Area; APC, annual percent change; NOS, not otherwise specified; SEER, Surveillance, Epidemiology, and End Results; NPCR, National Program of Cancer Registries; NAACCR, North American Association of Central Cancer Registries.
Source: SEER and NPCR areas reported by NAACCR as meeting high-quality data standards for the specified time periods.
Cancers are sorted in descending order according to sex-specific rates for all races/ethnicities. More than 15 cancers may appear under males and females to include the top 15 cancers in every race/ethnicity group.
White, black, API, and AI/AN include Hispanic and non-Hispanic; the race and ethnicity categories are not mutually exclusive.
Rates are per 100,000 persons and were age-adjusted to the 2000 U.S. standard population (19 age groups - Census p25-1130).
APC is based on rates that were age-adjusted to the 2000 U.S. standard population (19 age groups - Census p25-1130).
For all sites, myelodysplastic syndromes are included for the rate calculations but not for the APC calculations; they are excluded from cancer-specific analysis. Ovary excludes borderline tumors.
APC is statistically significantly different from zero (2-sided P < .05).
Statistic could not be calculated. The annual percent change is based on fewer than 10 cases for at least 1 year within the time interval.
2002–2006 rates for all races/ethnicities, white, black, AI/AN, API, Hispanic, and non-Hispanic (43 states): Alabama, Alaska, Arkansas, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Idaho, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Michigan, Minnesota, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, South Dakota, Texas, Utah, Virginia, Washington, West Virginia, Wyoming.
1997–2006 APCs for all races/ethnicities, white, black, AI/AN, API, Hispanic, and non-Hispanic (33 states): Alaska, California, Colorado, Connecticut, Delaware, Florida, Metropolitan Atlanta, Hawaii, Idaho, Illinois, Iowa, Kentucky, Louisiana, Maine, Massachusetts, Michigan, Minnesota, Montana, Nebraska, Nevada, New Jersey, New Mexico, New York, Oklahoma, Oregon, Pennsylvania, Rhode Island, South Carolina, Texas, Utah, Washington, West Virginia, Wyoming.
Among men, short-term trends in overall cancer incidence rates declined significantly during 1997–2006 for each racial/ethnic group, with the least decline observed for white and non-Hispanic men. Prostate cancer, the most frequently diagnosed cancer in men of all racial/ethnic groups, declined significantly for black men and Hispanic men. Lung cancer and CRC declined for men in each of the racial/ethnic population groups. Urinary bladder cancer declined for men in all races/ethnicities combined and for men who were white, black, non-Hispanic, and/or Hispanic. Cancer of the larynx declined for all groups of men except AI/AN. However, kidney cancers increased among men in all of the racial/ethnic groups, and thyroid cancer increased among each racial/ethnic group that had adequate numbers of cases on which to calculate rates for estimating trends.
Women also experienced declining trends in overall cancer incidence among each race/ethnicity except AI/AN. In contrast to men, the short-term AAPC in incidence rates for all cancers combined was similar among all races/ethnicities for women and showed less change. Trends in incidence rates for breast cancer declined during 1997–2006 except among API women. Rates of CRC and invasive cancer of the cervix declined among all women except AI/AN. Stomach cancer declined for all women. However, large increases in thyroid cancer were observed during this period for women in all racial/ethnic groups.
Cancer Death Rates, 2002–2006, and Short-Term Fixed Interval Trends by Race/Ethnicity, 1997–2006
Death rates for all cancers combined during 2002–2006 were highest for black men and women and lowest for API men and women (Table 4). Lung and prostate cancers and CRC were among the 3 leading causes of cancer death for men in each major racial/ethnic group, except for API men, for whom liver cancer ranked second. Among most women, the leading causes of cancer death were lung and breast cancers, CRC, and pancreas. However, among Hispanic women, breast cancer was the leading cause of cancer death. Specific rankings for the other 15 types of cancer also varied within the racial/ethnic groups by sex.
Table 4.
Death Rates for 2002–2006 and Fixed-Interval Trends for 1997–2006 for the Top 15 Cancers by Sex, Race, and Ethnicity in the United States
| All races/ethnicities | Whitec | Blackc | APIc | AI/ANc | AI/AN (CHSDA counties)c | Hispaniccd | Non-Hispaniccd | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex/cancer site or type b | Rank | Ratee | AAPCf | Rank | Ratee | AAPCf | Rank | Ratee | AAPCf | Rank | Ratee | AAPCf | Rank | Ratee | AAPCf | Rank | Ratee | AAPCf | Rank | Ratee | AAPCf | Rank | Ratee | AAPCf | |||
| Males | |||||||||||||||||||||||||||
| All sites | 229.9 | −1.7g | 226.7 | −1.5g | 304.2 | −2.5g | 135.4 | −2.1g | 146.4 | −2.8g | 183.3 | −1.2g | 154.8 | −2.2g | 235.0 | −1.6g | |||||||||||
| Lung and bronchus | 1 | 70.5 | −2.0g | 1 | 69.9 | −1.8g | 1 | 90.1 | −2.9g | 1 | 36.9 | −1.5g | 1 | 41.2 | −4.2g | 1 | 48.0 | −3.3g | 1 | 33.9 | −3.0g | 1 | 73.3 | −1.8g | |||
| Prostate | 2 | 25.6 | −4.0g | 2 | 23.6 | −3.9g | 2 | 56.3 | −4.2g | 4 | 10.6 | −3.9g | 2 | 16.8 | −3.9g | 3 | 20.0 | −1.2 | 2 | 19.6 | −3.5g | 2 | 25.9 | −4.0g | |||
| Colon and rectum | 3 | 21.9 | −2.8g | 3 | 21.4 | −3.0g | 3 | 31.4 | −1.7g | 3 | 13.8 | −2.7g | 3 | 15.3 | −3.3g | 2 | 20.0 | −1.1 | 3 | 16.1 | −1.8g | 3 | 2.4 | −2.7g | |||
| Pancreas | 4 | 12.3 | 0.1 | 4 | 12.2 | 0.3g | 4 | 15.4 | −1.0g | 6 | 8.1 | −0.4 | 5 | 7.1 | 0.6 | 6 | 9.1 | 3.2 | 5 | 9.1 | −0.1 | 4 | 12.5 | 0.2g | |||
| Leukemia | 5 | 9.8 | −0.8g | 5 | 10.1 | −0.7g | 8 | 8.5 | −1.1g | 8 | 5.0 | −0.8 | 9 | 4.5 | −0.8 | 9 | 5.9 | 1.4 | 8 | 6.2 | −1.6g | 5 | 10.0 | −0.7g | |||
| Non-Hodgkin lymphoma | 6 | 9.0 | −3.0g | 6 | 9.3 | −2.9g | 11 | 6.3 | −3.3g | 7 | 5.4 | −4.1g | 10 | 4.0 | −5.1g | 10 | 5.2 | −3.1 | 7 | 6.4 | −3.9g | 6 | 9.1 | −2.8g | |||
| Esophagus | 7 | 7.8 | 0.4g | 8 | 7.9 | 1.2g | 7 | 9.2 | −4.6g | 10 | 3.1 | −2.5 | 8 | 5.1 | 1.2 | 8 | 6.7 | 3.4 | 10 | 4.1 | −2.1g | 7 | 8.0 | 0.6g | |||
| Urinary bladder | 8 | 7.5 | −0.2 | 7 | 7.9 | 0.0 | 13 | 5.5 | −0.7 | 11 | 2.7 | −1.1 | 13 | 2.6 | h | 14 | 2.7 | h | 11 | 3.9 | −0.8 | 8 | 7.7 | 0.0 | |||
| Liver and intrahepatic bile duct | 9 | 7.5 | 2.1g | 9 | 6.8 | 2.2g | 6 | 10.8 | 2.6g | 2 | 15.0 | −1.3g | 4 | 7.9 | −0.2 | 4 | 10.3 | 1.2 | 4 | 11.3 | 1.3g | 9 | 7.2 | 2.1g | |||
| Kidney and renal pelvis | 10 | 6.0 | −0.6g | 10 | 6.1 | −0.5g | 12 | 6.0 | −0.9g | 13 | 2.4 | −2.7g | 6 | 6.6 | −1.2 | 7 | 9.0 | −0.5 | 9 | 5.2 | 0.0 | 10 | 6.0 | −0.6g | |||
| Stomach | 11 | 5.5 | −3.7g | 12 | 4.8 | −3.8g | 5 | 11.0 | −3.9g | 5 | 9.6 | −4.0g | 7 | 6.4 | −1.2 | 5 | 9.8 | 0.8 | 6 | 8.3 | −3.3g | 12 | 5.3 | −3.8g | |||
| Brain and other nervous system | 12 | 5.3 | −1.1g | 11 | 5.7 | −1.1g | 15 | 3.2 | −1.0g | 12 | 2.5 | 0.9 | 14 | 2.3 | −2.9g | 13 | 2.9 | −2.0 | 13 | 3.3 | −1.8g | 11 | 5.5 | −1.0g | |||
| Myeloma | 13 | 4.5 | −1.1g | 14 | 4.3 | −1.0g | 9 | 8.2 | −1.7g | 14 | 1.9 | −2.9g | 11 | 3.3 | −1.4 | 11 | 4.3 | −0.2 | 12 | 3.5 | −1.9 | 13 | 4.6 | −1.1g | |||
| Oral cavity and pharynx | 14 | 3.9 | −1.8g | 15 | 3.7 | −1.5g | 10 | 6.5 | −3.1g | 9 | 3.2 | −2.4g | 12 | 3.0 | −3.8 | 12 | 3.6 | −3.6 | 14 | 2.5 | −3.8g | 15 | 4.1 | −1.6g | |||
| Melanoma of the skin | 15 | 3.9 | 0.2 | 13 | 4.4 | 0.3 | 22 | 0.5 | 1.2 | 19 | 0.5 | h | 16 | 1.1 | h | 16 | 1.6 | h | 17 | 0.9 | −3.1g | 14 | 4.2 | 0.5 | |||
| Larynx | 16 | 2.3 | −2.2g | 16 | 2.1 | −1.9g | 14 | 4.7 | −3.2g | 17 | 0.7 | −2.7 | 15 | 1.5 | −7.0g | 15 | 1.9 | h | 15 | 1.9 | −4.2g | 16 | 2.3 | −2.0g | |||
| Soft tissue including heart | 17 | 1.4 | −1.5g | 18 | 1.4 | −1.2g | 16 | 1.4 | −3.5g | 15 | 0.9 | −1.7 | 19 | 0.8 | h | 19 | 1.0 | h | 16 | 1.0 | −3.2g | 18 | 1.5 | −1.3g | |||
| Females | |||||||||||||||||||||||||||
| All sites | 157.8 | −1.0g | 157.3 | −0.9g | 183.7 | −1.4g | 95.1 | −1.1g | 110.1 | −0.7g | 140.1 | 0.2 | 103.9 | −1.1g | 161.6 | −0.9g | |||||||||||
| Lung and bronchus | 1 | 40.9 | −0.1 | 1 | 41.9 | −0.1g | 1 | 40.0 | −0.2 | 1 | 18.2 | −0.8g | 1 | 28.3 | 1.1 | 1 | 33.5 | 2.6g | 2 | 14.4 | −0.8g | 1 | 42.8 | 0.1 | |||
| Breast | 2 | 24.5 | −1.9g | 2 | 23.9 | −2.0g | 2 | 33.0 | −1.5g | 2 | 12.5 | −0.2 | 2 | 14.3 | 0.2 | 2 | 17.6 | 1.3 | 1 | 15.5 | −2.1g | 2 | 25.2 | −1.8g | |||
| Colon and rectum | 3 | 15.4 | −2.6g | 3 | 14.9 | −2.6g | 3 | 21.6 | −2.3g | 3 | 10.0 | −1.7g | 3 | 10.2 | −3.4g | 3 | 13.7 | −2.4 | 3 | 10.7 | −0.6 | 3 | 15.7 | −2.6g | |||
| Pancreas | 4 | 9.3 | 0.5 | 4 | 9.1 | 0.5g | 4 | 12.4 | −0.6g | 4 | 7.0 | 1.6 | 4 | 6.6 | 2.0 | 4 | 7.8 | 1.7 | 4 | 7.5 | 0.8g | 4 | 9.4 | 0.6g | |||
| Ovary | 5 | 8.8 | −0.5g | 5 | 9.1 | −0.3 | 5 | 7.3 | −1.5 | 7 | 4.9 | 1.5g | 5 | 5.4 | 2.2 | 5 | 6.8 | 1.7 | 5 | 6.0 | 0.8 | 5 | 9.0 | −0.4g | |||
| Non-Hodgkin lymphoma | 6 | 5.7 | −3.3g | 6 | 5.9 | −3.3g | 11 | 4.1 | −2.4g | 8 | 3.7 | −2.6g | 7 | 3.3 | −3.1 | 8 | 4.4 | 0.3 | 8 | 4.6 | −3.3g | 6 | 5.8 | −3.4g | |||
| Leukemia | 7 | 5.5 | −1.0g | 7 | 5.7 | −0.7 | 9 | 5.1 | −1.9g | 9 | 2.9 | −2.3g | 9 | 3.1 | −0.8 | 10 | 3.6 | h | 9 | 4.0 | −1.2g | 7 | 5.6 | −1.0g | |||
| Corpus and uterus, NOS | 8 | 4.1 | 0.3g | 8 | 3.9 | 0.2 | 6 | 7.2 | 0.7g | 10 | 2.5 | 2.0g | 13 | 2.2 | −0.8 | 13 | 3.0 | h | 10 | 3.1 | 0.1 | 8 | 4.2 | 0.4g | |||
| Brain and other nervous system | 9 | 3.5 | −1.4g | 9 | 3.8 | −1.2g | 16 | 2.1 | −2.4g | 12 | 1.6 | 0.7 | 16 | 1.3 | h | 17 | 1.3 | h | 14 | 2.4 | 0.0 | 9 | 3.6 | −1.3g | |||
| Liver and intrahepatic bile duct | 10 | 3.2 | 1.2g | 10 | 2.9 | 1.2g | 12 | 3.9 | 0.4 | 5 | 6.6 | −0.3 | 6 | 4.6 | 1.1 | 6 | 6.5 | 1.6 | 6 | 5.1 | 1.1g | 10 | 3.0 | 1.1g | |||
| Myeloma | 11 | 3.0 | −1.3g | 12 | 2.7 | −1.2g | 7 | 5.8 | −2.3g | 13 | 1.5 | −1.3 | 11 | 2.5 | −0.4 | 12 | 3.3 | 0.0 | 12 | 2.6 | −1.1 | 11 | 3.0 | −1.3g | |||
| Stomach | 12 | 2.8 | −2.8g | 13 | 2.4 | −2.9g | 8 | 5.3 | −3.5g | 6 | 5.8 | −3.7g | 8 | 3.2 | −7.3g | 7 | 4.6 | −6.9g | 7 | 4.8 | −2.1g | 13 | 2.7 | −3.1g | |||
| Kidney and renal pelvis | 13 | 2.7 | −0.6g | 11 | 2.8 | −0.5g | 14 | 2.7 | −0.6 | 15 | 1.2 | −1.1 | 10 | 2.9 | −1.6 | 9 | 4.2 | 0.8 | 13 | 2.4 | 0.0 | 12 | 2.7 | −0.5g | |||
| Cervix uteri | 14 | 2.5 | −2.7g | 15 | 2.2 | −2.4g | 10 | 4.6 | −4.2g | 11 | 2.2 | −4.8g | 12 | 2.5 | −7.2 | 11 | 3.4 | −3.7 | 11 | 3.1 | −2.4g | 14 | 2.4 | −3.0g | |||
| Urinary bladder | 15 | 2.2 | −0.8g | 14 | 2.2 | −0.7g | 13 | 2.8 | −1.3g | 16 | 1.0 | −1.0 | 18 | 1.2 | h | 18 | 1.1 | h | 15 | 1.3 | −0.3 | 15 | 2.3 | −0.7g | |||
| Esophagus | 17 | 1.7 | −0.9g | 17 | 1.6 | −0.2 | 15 | 2.7 | −4.2g | 17 | 0.9 | −2.8 | 15 | 1.4 | h | 15 | 1.7 | h | 17 | 0.9 | −2.6g | 17 | 1.8 | −0.7g | |||
| Oral cavity and pharynx | 18 | 1.5 | −2.4g | 18 | 1.4 | −2.2g | 17 | 1.6 | −4.7g | 14 | 1.3 | −0.1 | 17 | 1.2 | h | 16 | 1.5 | h | 19 | 0.8 | −2.1 | 18 | 1.5 | −2.3g | |||
| Gallbladder | 20 | 0.8 | −1.8g | 20 | 0.8 | −1.8g | 19 | 1.0 | −0.6 | 18 | 0.8 | −3.8g | 14 | 1.5 | −3.3 | 14 | 2.4 | h | 16 | 1.3 | −1.7 | 20 | 0.8 | −1.9 | |||
API: Asian/Pacific Islander; AI/AN: American Indian/Alaska Native; IHS: Indian Health Service; CHSDA: IHS Contract Health Services Delivery Area; AAPC: average annual percent change; NOS: not otherwise specified.
Source: National Center for Health Statistics public-use data file for the total U.S.
Cancers are sorted in descending order according to sex-specific rates for all races/ethnicities. More than 15 cancers may appear under males and females to include the top 15 cancers in every race/ethnicity group.
White, black, API, AI/AN, and AI/AN (CHSDA counties) populations include Hispanic and non-Hispanic; the race and ethnicity categories are not mutually exclusive.
Data for Hispanic and non-Hispanic exclude the District of Columbia, Maine, Minnesota, New Hampshire, and North Dakota.
Rates are per 100,000 persons and were age-adjusted to the 2000 U.S. standard population (19 age groups – Census p25-1130).
The AAPC is the Average Annual Percent Change and is a weighted average of the APCs calculated by Joinpoint over the time period 1997–2006. Joinpoint analyses with up to 2 joinpoints are based on rates per 100,000 persons and were age-adjusted to the 2000 U.S. standard population (19 age groups - Census p25-1130). Joinpoint (JP) Regression Program, Version 3.3.1. April 2008, National Cancer Institute.
AAPC is statistically significantly different from zero.
Statistic could not be calculated. The average annual percent change is based on fewer than 10 cases for at least 1 year within the time interval.
During 1997–2006, short-term trends in death rates for all cancers combined decreased for all racial/ethnic groups and for both men and women, except for AI/AN women. Similarly, lung cancer mortality trends decreased for all racial/ethnic groups of men as did trends for prostate cancer and CRC except among AI/AN men. Liver cancer death rates increased for all men except API men whose rates decreased, and AI/AN men. Short-term trends for breast cancer death rates decreased in white, black, Hispanic, and non-Hispanic women and CRC death rates decreased for all women except those who were Hispanic or AI/AN. Among women, short-term lung cancer death rate trends decreased for white, API, and Hispanic women but increased for AI/AN women. Short-term mortality trends for most other types of cancer had considerable variability among racial/ethnic population groups of women. Trends in death rates of pancreatic cancer increased for white men and women, but decreased for black men and women.
CRC Incidence (by Age, Sub-site, and Stage), Mortality, and Stage-specific Survival Trends
Long-term incidence trends for CRC (based on SEER 9) have been fairly consistent in men and women (Table 1), increasing incidence (for men) during 1975–1985, marked declines during 1985–1995 for men and women followed by a short non-significant increase (1995–1998), and marked declines during 1998–2006. CRC death rates (Table 2) have declined since 1984 in both men and women, with an accelerated rate of decline since 2002 (for men) and 2001 (for women). During the most recent decade (1997–2006, based on pooled data, Table 3), short-term trends in CRC incidence declined for all racial/ethnic groups, and for men and for women (except AI/AN); the fastest annual rate of decline occurred among men and women ≥65 years of age (a data table is available at www.seer.gov/report_to_nation/1975_2006 [Supplemental Table 2]) as compared to younger ages. In contrast, short-term incidence trends increased annually for persons <50 years of age within most population groups with few exceptions. Incidence rates by major anatomic sub-sites (proximal colon, distal colon, rectum) varied considerably by race, sex, and age (see the data table at www.seer.gov/report_to_nation/1975_2006 [Supplemental Table 2]). Incidence rates for all ages combined for distal colon and rectal cancers decreased among men and women in every racial/ethnic group, except for distal colon cancer among AI/AN men and women. In contrast, among persons <50, incidence rates for distal colon and rectal cancers increased in men and women of all race/ethnicities combined, in white men and women, and in black men. Rates for proximal colon cancer decreased in men and women of all race/ethnicities combined, but decreased by subgroup only for white men and women, API men, and Hispanic women.
Trends in stage-specific incidence rates (Figure 2a, as well as a data table available at www.seer.gov/report_to_nation/1975_2006 [Supplemental Table 3]) for the SEER 9 data showed annual increases in incidence of localized cancer from 1975 to 1987 (APC=1.8%), declines from 1987 to 1995 (APC=−2.1%) and non-significant increases from 1995 to 1999, followed by decreases between 1999 and 2006 (APC=−2.2%). Incidence rates of regional cancer increased between 1975 and 1985 (APC=1.8%), decreased markedly but not significantly from 1985 to 1988 (APC=−5.0%), and decreased significantly thereafter, by 0.8% per year from 1988 to 2001 and by 5.0% per year between 2001 and 2006. Incidence rates of distant cancer have decreased steadily between 1975 and 2006 by 1.3% per year. Incidence rates of unstaged cancer decreased by 2.8% per year between 1975 and 1997 and by 5.7% per year during the 10-year interval 1997 to 2006. CRC 5-year relative survival has improved throughout the period of 1975–2001 (Figure 2b) for all patients within each stage category. Relative survival at 5 years for the most recent diagnosis years are 90% for localized disease, 70% for regional disease, and 12% for distant disease.
Figure 2.
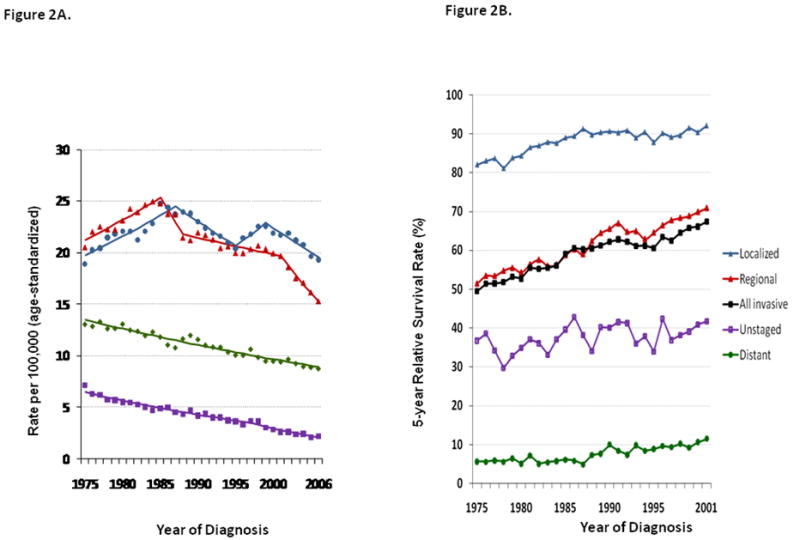
Figure 2A. Colorectal Cancer Age-Standardized Incidence Rates by Stage at Diagnosis SEER 9 Incidence, 1975–2006, All Races, Both Sexes
Figure 2B. Colorectal Cancer 5-year Relative Survival Rates by Stage at Diagnosis SEER 9 Incidence, 1975–2001, All Races, Both Sexes
Source: SEER 9 areas (San Francisco, connecticut, Detroit, Hawaii, Iowa, New Mexico, Seattle, Utah and Atlanta).
Incidence rates are age-adjusted to the 2000 US Std Population (19 age groups - Census P25-1103).
Regression lines with up to 4 Joinpoints are calculated using the Joinpoint Regression Program Version 3.3.1, April 2008, National Cancer Institute.
Stage analyses were based on SEER historic stage categories using extent of Disease codes and the Collaborative Stage Data Collection system. Relative survival was calculated with the SEER*stat software (www.seer.cancer.gov/seerstat) version 6.5.2: NCI; 2009.
Past and Future Trends in CRC Incidence and Death Rates: Impact of Risk Factors, Screening, and Treatment
Figure 3 shows the age-standardized CRC incidence rates by calendar year 1975–2000 for SEER 9 registries (adjusted to represent first primary CRC), and for the MISCAN-Colon model estimated rates. There are two lines with estimated rates for MISCAN. One line represents the model-predicted CRC incidence rates based on observed trends in risk factor prevalence and screening uptake. The other represents the model-predicted rates when only changes of risk factors would have occurred and no screening had taken place. The overall observed decline in CRC incidence was 22% for 1975–2000. The MISCAN model-predicted decline without screening was 11%, indicating that changes in risk factors accounted for 50% of the overall decline in incidence rates during 1975–2000. Screening affected the CRC incidence rates adversely in the short term but then accounted for 50% of the CRC incidence decline for the period.
Figure 3.
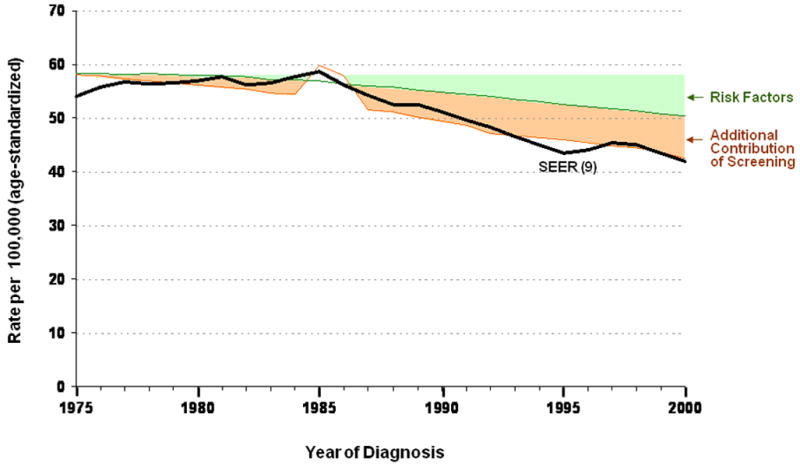
Partition of Past Trends in Colorectal Cancer Incidence* (1975–2000)
* Rates are based on the first primary colorectal cancer and include the primary sites of C18.0 C18.2–C18.9, C19.9, C20.9 and the ICD-03 histologies of: 8000–8001, 8010, 8020, 8140, 8210–8211. Rates do not include cases that are form a reporting source of death certificate only or autopsy only.
Figure 4 shows the age-standardized observed and MISCAN model-predicted CRC U.S. death rates by calendar year 1975–2000. There are three lines with estimated death rates. One line represents the model-predicted CRC mortality based on observed trends in risk factor prevalence, screening uptake and treatment use. Another represents the model-predicted death rates when only risk factors and screening changed over time, and the last line shows the model-predicted mortality for changes in risk factors only. The overall observed decline in CRC mortality was 26% for 1975–2000. The model predicted that with only changes in risk factors, CRC mortality would decrease by 9%, explaining 35% of the observed mortality decline. Screening decreased mortality by another 14%, explaining 53% of the mortality reduction, while treatment added another 3% decline, explaining the final 12% of the observed decline in CRC mortality.
Figure 4.
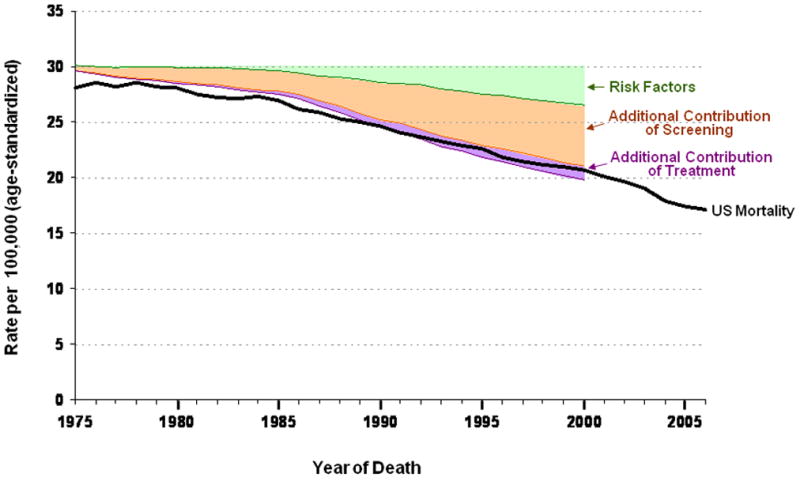
Partition of Past Trends in Colorectal Cancer Mortality (1975–2000)
Source: CDC National Center for Health Statistics (NCHS) National Vital Statistics System.
Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: Final data for 2006. National Vital Statistics Reports, Apr 17, 2009; 57(14).
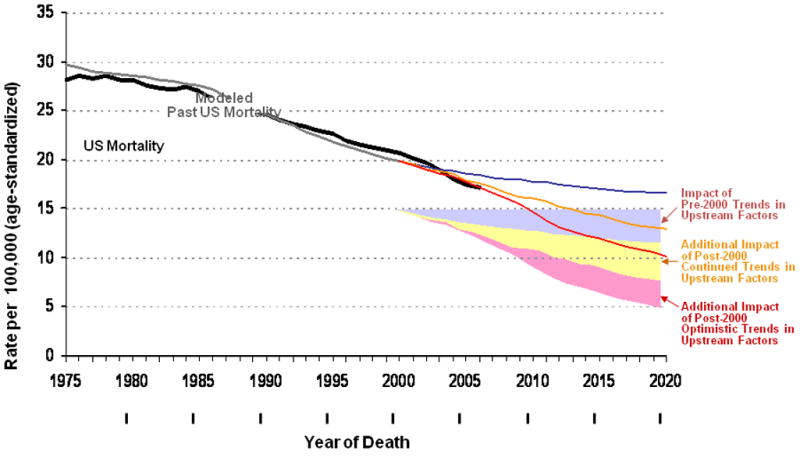
The microsimulation modeling also projected future CRC mortality based on differing intensities of cancer control including no change (pre-2000 frozen), continued trends, and optimistic trends in the prevalence of interventions,29 Figure 5. Without changes in risk factors, screening and treatment (frozen as of 2000), the decline in CRC mortality may only be 17%. However, the MISCAN-Colon model predicts a 36% overall decline in CRC mortality from 2000 to 2020 if current trends in risk factors, screening and treatment continue. If we can accelerate the projected trends, an overall mortality reduction of 50% by 2020 is possible. Figure 6 shows the contribution of the three types of intervention to this optimistic reduction in mortality. Risk factor modifications, although requiring the longest time to show an impact, will have a sizable effect by 2020. Increases in the proportion of adults screened and in the use of endoscopic CRC screening will provide the largest reduction in future death rates with application of current state of screening technologies, risk factor modification, and use of current treatment practices.
Figure 5.
Projections of Colorectal Cancer Mortality with Differing Intensities of Cancer Control (2000–2020)
Source: CDC National Center for Health Statistics (NCHS) National Vital Statistics System.
Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: Final data for 2006. National Vital Statistics Reports, Apr 17, 2009; 57(14).
Figure 6.

Contributions of Risk Factors, Screening and Treatment to Optimistic Projections of Colorectal Cancer Mortality (2000 – 2020)
Source: CDC National Center for Health Statistics (NCHS) National Vital Statistics System.
Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: Final data for 2006. National Vital Statistics Reports, Apr 17, 2009; 57(14).
DISCUSSION
This Annual Report to the Nation documents continued declines in incidence and mortality rates from all cancers combined among both men and women. However, cancer incidence and mortality vary by specific types of cancer and by sex and racial/ethnic group. Decreases in incidence and mortality rates are greater for men than for women (Tables 1 and 2), but overall rates continue to be much higher for men than for women (Tables 3 and 4). As in past years, incidence rates for the 3 leading causes of cancer for men (prostate and lung cancer and CRC) all declined along with 3 more of the top 15 cancers (i.e., oral cavity, stomach, and brain) (Table 1). However, incidence rates increased for kidney, liver, and esophageal cancers and for leukemia, myeloma, and melanoma; rates did not change for bladder and pancreatic cancer or for NHL. For the top 3 cancers among women, breast and CRC declined, but lung cancer incidence rates increased. Of the remaining 15 leading cancers for women, incidence rates also declined for cancers of the uterus, ovary, cervix, and oral cavity, but increased for cancers of the lung, thyroid, pancreas, bladder, and kidney and for NHL, melanoma, and leukemia.
The continued decline in death rates (Table 2) from all cancers combined for men and women reflects the impact of increased screening, reduction of risk factors, and improved treatment. Risk factors generally affect disease development over the long term, rather than short term, so education and prevention efforts begun decades ago may be reflected in the current decreased cancer mortality. Decreases in cancer mortality rates for men were greater than for women, but as with incidence rates, cancer mortality rates are generally much higher for men than for women. Of the 15 most frequently occurring cancers among men in the most recent time period (Table 2), decreases occurred in death rates for cancers of the stomach, kidney, brain, lung, prostate, and oral cavity and for CRC, leukemia, NHL, and myeloma. Death rates among men increased for melanoma and for liver and esophageal cancer. Among women in the most recent time period (Table 2), mortality rates decreased for CRC and for cancers of the stomach, kidney, brain, breast, ovary, and bladder as well as for leukemia, NHL, and myeloma; death rates for women increased for pancreatic and liver cancers. Liver cancer was the only cancer for which death rates increased for both men and women, suggesting a need to identify and implement interventions that can reduce mortality due to this cancer.
Of the leading cancers, prostate cancer is of special note because it is the most frequently diagnosed cancer and second leading cause of cancer death among men. Incidence for prostate cancer has fluctuated through the years, increasing during 1975–1992, decreasing during 1992–1995, increasing (non-significantly) during 1995–2000, and decreasing again during 2000–2006 (Table 1). The few randomized trials on prostate cancer screening show conflicting results with varying methodologies.56–57 Consequently, comparative microsimulation modeling is being used to better understand the progression of the disease, the impact of screening on mortality, and cost implications of expanded prostate screening.58–60 A CISNET prostate cancer project is using available data to model the impact of screening on prostate cancer incidence and mortality. Screening for breast cancer, the most frequently diagnosed cancer and second leading cause of cancer death among women, is already recommended for women.61 Breast cancer incidence has also fluctuated with increases and decreases over time (Table 1), but declined 1.5% per year during 2002–2006 (Table 3).
Among racial and ethnic groups, the highest cancer death rates occurred among black men and women, and the lowest rates occurred among API men and women (Table 4). However, pancreatic cancer death rates, the fourth most common cause of cancer death in the U.S., increased among white persons but decreased among black persons. The 3 leading causes of cancer deaths by racial and ethnic group for men were lung and prostate cancers and CRC. This ranking varied only for API men, for whom lung and liver cancers and CRC were the leading cancers. Among women by racial/ethnic group, the leading causes of cancer deaths were lung and breast cancers and CRC, except for Hispanic women, for whom breast cancer ranked first. Mortality for the top 3 cancers declined for men among all racial and ethnic groups, and breast and CRC declined for women. CRC death rates decreased for women in all racial and ethnic groups except AI/AN and Hispanic women. The differences and fluctuations in death rates for specific cancers for different racial and ethnic groups and for men and women suggest differences in risk behaviors, socioeconomic status, and access to and use of screening and treatment.62–64
This report highlights CRC, currently the third most frequently diagnosed cancer and the second leading cause of cancer deaths in the U.S. for men and women combined. Globally, CRC incidence in economically transitioning countries continues to rise due to increased exposure to risk factors, but in economically developed countries, rates have stabilized or are declining.65–66 In the U.S., an estimated 147,000 persons will be diagnosed with CRC in 2009 and about 50,000 will die of the disease.62, 67
Table 1 shows that since 1985, CRC incidence rates have declined for both men and women except during 1995–1998. The age-adjusted CRC incidence rates for 1997–2006 declined among both men and women ≥50 years of age but increased among those <50 (a data table is available at www.seer.gov/report_to_nation/1975_2006 [Supplemental Table 2]). Although men generally had slightly greater rates of decline than women, incidence rates for men remain considerably higher than for women. Although >90% of newly diagnosed cases of CRC occur among persons ≥50 years of age (a data table is available at www.seer.gov/report_to_nation/1975_2006 [Supplemental Table 2]), increasing incidence among younger men and women is of concern, suggesting future increases in CRC as these populations age that could be exacerbated by increasing prevalence of obesity and unfavorable dietary changes.68 Persons <50 years of age are also more likely to be diagnosed with later stage and less differentiated CRCs69 than older persons, likely reflecting the benefits of screening in older populations. Age-adjusted incidence rates for persons <50 years of age were highest among black persons and lowest for persons of Hispanic ethnicity, but are increasing most rapidly for the AI/AN population. For older adults, incidence rates were highest among black persons and were disproportionately high among those 50–64 years old. Persons ≥65 are more at risk for CRC, have higher incidence (with rapid annual declines in trends), and higher rates of CRC test use compared with persons <65.70–71 The burden of CRC mortality is concentrated in older individuals with 6% of deaths in 2006 among persons <50 years of age, 20% among persons 50–64 years of age, and 74% among persons ≥65 years.19, 22
Screening appears to have had considerable impact on reducing CRC incidence and mortality.36 CRC screening was introduced in the 1970s and 1980s when researchers showed the feasibility of testing for occult blood in stool and initiated randomized clinical trials. In 1985, the diagnosis of colon cancer in President Ronald Reagan increased public awareness of CRC, demonstrated by a documented increase in use of tests for early detection of CRC among Medicare recipients and an increase in CRC incidence, particularly for early stage disease.72 During 1987–1998, gradual increases in screening for CRC occurred.70 Results of randomized clinical trials of FOBT, which showed reductions in both CRC mortality and incidence, provided strong evidence for recommending this test;73–74 FOBT continues to be a recommended screening option if performed annually.75–77 Colonoscopy was introduced as a method for screening the entire colon in the 1990s and has been recommended as a screening test for average-risk persons ≥50 since 1997.77 Recent guidelines distinguish between screening tests that primarily detect cancer and those that are more likely to detect both cancer and adenomatous polyps.75 Rates of CRC screening have continued to increase from 2000 to 2008, with a marked shift from sigmoidoscopy to colonoscopy for endoscopic screening and a declining use of FOBT (C. Klabunde, [ klabundc@mail.nih.gov], unpublished data).70–71, 78–80
Research is ongoing regarding the most effective screening methods, persons most at risk, and optimal surveillance intervals. Simulation models and meta-analyses of published literature have provided insight and potential cost-effective guidelines for policy and health care. Although the organizations involved in CRC prevention and control have differing recommendations for specific aspects of CRC screening, there is consensus is that adults should begin screening at age 50, preferably by methods likely to detect cancer and adenomas before they develop into cancer.36 Recent data suggest that approximately 50% of persons ≥50 years of age have been screened according to recommended time intervals (C. Klabunde, [ klabundc@mail.nih.gov], unpublished data), with the highest rates of CRC screening (≈60% in 2008) among persons ≥65 years of age. The proportion screened remains <70%, the rate used by MISCAN-Colon when projecting CRC mortality reductions using optimistic changes in upstream factors; however, rates of colonoscopy screening have increased while rates of FOBT and sigmoidoscopy have declined70 (C. Klabunde, [ klabundc@mail.nih.gov], unpublished data).
A recent assessment of screening methods found that, with high rates of adherence for each method, similar gains in life-years resulted from several screening methods: colonoscopy every 10 years, annual high-sensitivity FOBT, and flexible sigmoidoscopy every 5 years with Hemoccult SENSA every 2–3 years.36 Also, computed tomographic colonography has been found to be potentially as effective as colonoscopy if conducted every 5 years with follow-up for those with polyps ≥6 mm.35 Although colonoscopy screening appears to have gained acceptance among healthcare professionals and patients, resources for colonoscopy may limit its use as a primary screening modality.78–79 For colonoscopy to be beneficial, downstream resources need to be available to patients who screen positive: follow-up colonoscopy following positive results of other screening tests, diagnostic colonoscopy for symptomatic patients, and surveillance colonoscopy after diagnosis of an adenoma or adenocarcinoma. Although risks for adverse events from colonoscopy are low, they increase with age in part because of comorbidities.81 Some guidelines suggest discontinuing screening of persons >75 years of age,77 but only about a third of surveyed physicians reported that they stop recommending screening when healthy patients reach a certain age, most commonly, at age 80.80
A family history of CRC and a personal history of CRC, colorectal polyps, or chronic inflammatory bowel disease are major risk factors for CRC.82–83 Risk for CRC is about twice that of an average person for those who have a first-degree relative (parent, sibling, or child) who has had CRC; risk is even greater if the relative was diagnosed at a young age or if more than one first-degree relative has had CRC.84–85 Individuals with these risk factors may be advised to begin screening before age 50, when screening is recommended for average risk individuals. Individuals with certain inherited genetic alterations, such as familial adenomatous polyposis (FAP) or hereditary nonpolyposis colorectal cancer (HNPCC) also known as Lynch syndrome,86 are at even higher risk of developing CRC and should be identified and carefully monitored.87
Other major risk factors for CRC which are potentially modifiable include physical inactivity, being overweight and obese, and a diet high in red and processed meats.88–101 Modification of these risk factors requires behavioral changes that are difficult but important to achieve and impact many health outcomes in addition to CRC. Decreasing the prevalence of these risk factors can be protective against CRC, although changes are expected to result in long-term, not short-term gains.102 Changes in community factors and health policy can be important tools for changing individual behaviors. The need for national policy and programs that engage communities in working towards improved nutrition and physical activity, smoking cessation, and decreased alcohol use has been widely recognized. CDC has proposed a program of 16 community-level initiatives to promote healthy lifestyles through increasing availability of affordable, healthy foods and beverages; encouraging physical activity among youth and adults; and promoting environments that support physical activity. The program fosters partnerships and collaborations to implement the strategies and evaluate outcomes to assess progress towards a healthier nation.103
Continued declines in tobacco use in the U.S. will likely contribute to declining trends in CRC incidence. Although neither the 2004 monograph on smoking from the International Agency for Research on Cancer104 nor the 2004 Surgeon General’s report on smoking105 classified CRC as a smoking-related cancer, consistent evidence shows that smoking increases the development of adenomatous polyps, particularly more aggressive adenomas.106 Also, increasingly strong and consistent evidence indicates that smoking is associated with CRC, especially with rectal cancer.107–109 Further, although more research is required to assess the benefits and risks of chemoprevention, use of anti-inflammatory drugs, dietary supplements (e.g., calcium), and multivitamins could be protective against this cancer.110–114
CRC incidence varies by state and county, presumably because of differences in screening resources and access to care if residence is in an underserved community. One study associates high CRC incidence rates for white persons and black persons with residence in counties having high uninsured or poverty rates, fewer primary physicians, and large proportions of rural or underserved areas.115 However, another U.S. study showed that white persons living in high-income counties had higher CRC incidence for proximal cancer than those living in mid- or high-poverty counties, suggesting that lifestyle factors such as diet, which is influenced by economic status, play a prominent role in geographic variations in CRC incidence.116
The simulation models created by CISNET estimate the extent to which CRC incidence and mortality can be reduced through interventions and treatment and can predict effects of various scenarios on CRC outcomes. This research shows that if 1995–2000 trends for risk factor prevalence, screening, and treatment continue, death rates from CRC could be reduced by 36% by 2020. However, adverse trends in some risk factors can neutralize gains in others, so gains must be assessed over a long period of time for observed impact.102 If intervention efforts are successful and increase beyond those of 1995–2000, deaths from CRC could be substantially reduced. CISNET modeling demonstrates what would be required to reduce the impact of CRC in the U.S. An estimated $8.4 billion is spent annually on CRC treatment,117 which will increase as CRC prevalence increases to an expected 1.5 million persons by 2020,118 with most health care cost being devoted to the initial year after diagnosis.119
Limitations
Cancer surveillance in the U.S. now covers the majority of the population for monitoring incidence and the entire population for monitoring mortality. However, certain limitations in data sources, data collection, and analyses may have influenced the findings of this report. First, state and national population estimates provided by the Census Bureau from 2000 forward and used initially with statistical reporting last year were developed by using improved and more accurate methodologies that had noticeable effects on age-specific rates for some counties and states. The net impact of those changes for 2006 was a downward shift in the current postcensus estimates (due primarily to net international migration estimation), compared with postcensus estimates used in the previous report. National incidence rates and death rates were not affected, but some state-level rates were. NCI also developed modifications to these census estimates to attempt to account for changes in 2005 county-level populations due to displacement of people after hurricanes Katrina and Rita in the most affected counties of Louisiana, Mississippi, Alabama, and Texas.
Second, we used three different statistical methods for two geographic sets of aggregate data to describe cancer trends: first, a single linear regression model was used to describe short-term trends (1997–2006) by race and ethnicity for geographic areas covering more than two-thirds of the U.S.; next, a joinpoint model was used to describe long-term trends (1975–2006) for all races and ethnicities combined in a subset of these geographic areas covering approximately one-tenth of the U.S. population; finally, the AAPC, a new summary measure of a trend over a prespecified fixed interval based on an underlying joinpoint model was introduced in this report. The joinpoint model is preferable to single linear regression when a sufficient number of years are available for analysis because it enables identification of recent changes in magnitude and direction of trends, although the trends may be unstable when based on rates with large variance and when statistical power is low for detecting joinpoint segments. The AAPC can be estimated even if the joinpoint model indicates changes in trends during those years because this measure is the geometric weighted average of the joinpoint segments over the interval. Enough years of data are now available to use joinpoint analysis for trends by race and ethnicity, and we have used the AAPC based on up to 2 line segments over the 10-year fixed period to report multiple sites and racial and ethnic groups. Methods have yet to be adapted for delayed reporting of aggregated data, except for incidence from the 9 oldest SEER registries. Delayed reporting may affect the most recent joinpoint segment for the national data.
Third, the Veteran’s Health Administration (VA) hospitals have traditionally been a critical source of data for cancers diagnosed among veterans eligible to receive care from these facilities, representing approximately 3% to 8% of cancer diagnoses among men. A 2007 policy change regarding transfer of VA cancer data to state central cancer registries has resulted in incomplete reporting of VA hospital cases in some registries. This change affected reporting beginning with the third quarter 2004 diagnosis year through the end of the 2006 diagnosis year (http://seer.cancer.gov/csr/1975_2006/resultsmerged/sect_33_VA_adjustment.pdf). As a result, cancer incidence rates among men for 2005 and 2006 in the SEER 17 registries that cover more than a quarter of the U.S. population were underestimated by 1% to 2% for all cancers combined. The level of underreporting varied from 0.5% to 4% according to cancer site, race and age group.13, 120 Using similar methods, cancer incidence rates for 2006 among men in the 31 NPCR registries that provided data were underestimated between 0.3% to 11.2% (C. Eheman [ cre1@cdc.gov], email, August 25, 2009). The amount of underestimation based on data from other geographic areas may vary by local VA facility reporting patterns and the VA’s contribution to the total number of cancers. In late 2008, data transfer agreements were being established between many VA facilities and states with central registries. Over time, as cancer registries receive these missing VA cases, national cancer incidence estimates will be more complete.
Fourth, assessment of stage-specific CRC incidence trends was limited by a change in methods used to collect information on stage beginning with 2004 diagnoses. The improvements in the use of the Coding System for Collaborative Stage (http://www.cancerstaging.org/cstage/index.html) created an artifact in the trend between the 2003 and the 2004 diagnosis years for most state registries funded by CDC (data not shown). The SEER 9 database was used to estimate stage-specific CRC incidence trends because the SEER Program has used Extent of Disease since 1988 and CS since 2004 for comparability of information on stage across changes in coding rules.
Fifth, the national estimates of prevalent use of CRC screening and early detection tests were based on trend data from respondents ≥50 years of age who participated in the NHIS. These estimates, although based on smaller sample sizes with substantially higher response rates than data from the Behavioral Risk Factor Surveillance Survey (BRFSS),121 tend to be slightly lower than BRFSS estimates.71 Differences in estimated prevalence may be due to differences in mode of administration and response rates from the telephone-based BRFSS compared with the interviewer-administered NHIS. NHIS in-person surveys also provide access to households without telephones and cell-phone-only households, which cannot be reached by means of random-digit-dial (RDD) surveys, such as that used by the BRFSS. These factors point to the importance of mixed-mode survey methodology and alternative frames for mitigating the increase in telephone survey nonresponse, which erodes coverage of RDD telephone sampling frames.122
Sixth, as routinely noted in the annual reports,1–11 the broad racial and ethnic groups categorized for our analyses may mask variations in the cancer burden by country of origin, e.g., Chinese and Vietnamese in the API group123 and Cubans and Mexicans in the Hispanic group8, 124 or by other unique characteristics of high-risk populations.125–128 Also, cancer rates for populations may be limited by difficulties in ascertaining race and ethnicity information from medical records, death certificates, and census reports.129
Finally, the MISCAN-Colon model inputs were constrained to those previously used in the published results29 (http://cisnet.cancer.gov/projections/colorectal). This report did not re-examine assumptions about risk factors, screening, and treatment interventions because the perspective was on their relative importance. Additional studies by the MISCAN-Colon modeling group will examine trends in screening modalities as well as other factors that were not incorporated into earlier models. The observed SEER 9 incidence data presented with the MISCAN-Colon model results were adjusted to reflect first primary incidence rates rather than any primary, with adjustments for apparent overreporting of first primary CRC tumors during the early years of the registry using information from the most recent diagnostic years reported in the cancer registries. Minor restrictions in histologic sub-sites and exclusion of death-only cases for CRC as reported by SEER were made for the MISCAN-Colon model with little impact on model predictions.
Future Directions
The observed decreases in incidence and death rates from all cancers combined in men and women overall and in nearly all racial and ethnic groups are highly encouraging. This progress must be viewed as part of a long-term strategy for substantial reductions in cancer incidence and mortality through improved risk factors, increased early detection, and better treatment. However, progress has been more limited for some types of cancer for which breakthroughs in prevention, early detection and treatment remain elusive. Cancer is multifaceted, and many approaches and aspects of this disease affect outcomes for cancer patients. This section summarizes key considerations for future directions in cancer research and interventions.
Microsimulation modeling provides evidence-based support for decisions about effective policy and resource allocation for cancer interventions. The models use available data to project outcomes of possible scenarios concerning risk factors, screening, and treatment and are important for decision making when observed data are unavailable or inadequate. For example, CISNET is working on models for prostate cancer to better understand the progression of this leading cause of cancer incidence among men and to assess the benefits of increased prostate screening.56–57
Cancer surveillance systems, which capture prevalence of cancers by age, sex, geographic locations, and other variables, also contribute to informed decision making by enabling an understanding of trends in various aspects of cancer, including diagnosis and treatment. Foundational for cancer prevention and control efforts, the enhancement of cancer registries and surveillance systems can enable a more comprehensive understanding and tracking of cancer and public health and medical interventions.
Many cancers have modifiable risk factors although risk factor reduction usually results in long-term, not short-term, improvements in cancer incidence. Thus, the impact of changing prevalence of CRC risk factors must be assessed over a long period of time to observe impact.102 For example, tobacco prevention efforts over the past decades are likely reflected in recent reductions in lung cancer incidence. Also, research shows that states with comprehensive tobacco control programs have more rapid decreases in lung cancer than those without such programs.130–131 Although much can be learned from the policy and program strategies used in comprehensive tobacco control, expanded current research is needed on the importance of lifestyle behaviors, particularly physical inactivity, poor diet and obesity, to cancer risk and survival.132–134 Extensive behavioral research, including randomized controlled trials, has demonstrated that individually focused behavioral interventions result in recommended changes in these health behaviors. However, a key challenge is to identify what is needed to ensure these behavioral changes are sustained. Research has identified that changes in the environments and policies that support recommended health behaviors are important to achieve and sustain beneficial lifestyle behaviors. Being overweight and failing to exercise are adverse trends that appear to increase risk for CRC,89–92 especially colon cancer.95–96, 98, 135 An estimated 33% of U.S. adults are overweight, and another 34% are obese.103 Increasing CRC incidence among young adults (<50) may be an early indicator of the adverse impact of these risk factors. CDC has recently published policy and communication strategies to decrease obesity and physical inactivity,103 including recommended policies to facilitate better nutrition and environments conducive to physical activities such as walking or biking. In 2009, a Weight of the Nation conference136 addressed the need for multiple approaches to curbing obesity-related illness137 and containing the rising cost of obesity for the nation, estimated at $147 billion in 2007.138
Several risk factors associated with cancer appear to act over a long time, although some changes in risk factors can impact cancer incidence in a shorter period of time. For example, declines in breast cancer in 2002 following lower use of combined hormonal therapy among women.139–141 Beyond risk factor reduction, chemoprevention is a growing research area, especially because several medications used for other purposes appear to be protective against CRC; however, some substances such as aspirin have adverse side effects, so additional research is needed to clarify the effectiveness, appropriate dose, and potential toxicity of potential chemopreventive therapies.110–112 Recent concerns are also focused on an increased risk of CRC142 from nationwide fortification of cereal grains with folic acid in the late 1990s to reduce neural tube birth defects.
Disparities in cancer incidence and mortality need further investigation, including ways to decrease disparities related to race or ethnicity, socioeconomic status, insurance status, geographic location, and access to health care. Eliminating these disparities will require increased access to screening and advanced treatment modalities, which place demands on health care delivery systems. Short-term and long-term impact on the health care provider workforce, facilities and technology, and financial resources for cancer interventions to improve health outcomes for all segments of the population must be considered. Modifiable risk factors have been identified (e.g., obesity, poor diet, alcohol consumption, and lack of physical activity), that require effective culturally sensitive interventions targeting specific populations to reduce these risk factors.
CRC has been the highlight of this report. Although great progress has been made in reducing the impact of CRC, improved application of currently available knowledge and ongoing research are needed to make further inroads. CRC research priorities were established by the NCI Progress Review Group and have guided a decade of activities, including biologic and etiologic research in CRC.143 Genome-wide association studies recently have implicated multiple loci across the genome that may contribute to CRC susceptibility.144
Research is also needed to enhance screening technologies as well as strategies to increase screening and early detection; such strategies include community and agency collaborations to implement screening,145 enhanced screening in primary care settings and rural areas,146 and removal of cultural and language barriers to screening.146 Screening has increased considerably since 2000, yet only about 50% of adults 50 and older were screened in 2005.71 Studies have suggested possible reasons for less-than-optimal use of CRC screening: variability in physicians’ interpretation and use of CRC screening guidelines;80 lack of insurance coverage, regular health provider, or awareness;71 and a slight increase in adverse events associated with colonoscopy as the age of screened patients increases.81 CDC’s new Colorectal Cancer Control program will provide direct screening services to populations at greatest need and focus attention to increasing colorectal cancer screening rates among the US population 50 years of age and older nationwide (www.cdc.gov/cancer/colorectal and www.cdc.gov/screenforlife).
A number of public, private, and voluntary organizations have targeted CRC screening as one of their most important cancer control priorities and have been working to educate the public and medical providers about the importance of screening.147 Advocacy efforts at the state and federal levels have encouraged state legislation requiring coverage for the full range of CRC screening tests and the development of federal programs to enhance access to screening and treatment of medically underserved populations. A state-of-the-science conference hosted by the NIH in 2010 will focus on ways to enhance use and quality of CRC screening.148 Also, a CDC-CISNET collaboration is working to assess the capacity of the U.S. health care system to increase CRC screening of persons 50–64 years of age and to determine cost implications for Medicare, Medicaid, and private payors, taking into consideration increased costs for early detection yet savings in treatment costs.
Researchers have also made great strides in developing treatment regimens to optimize patient response and performance, particularly for patients with metastatic CRC. Some treatments that have positively impacted morbidity, quality of life, and survival for CRC patients include multimodality therapy for rectal cancer and use of surgical approaches that result in higher rates of sphincter preservation.149 Also, surgical resection of hepatic metastases and, more recently, development of new chemotherapies appear to increase survival for patients with metastatic disease.150–151 Targeted therapy with monoclonal antibodies have been developed152 as well as more individualized CRC therapies based on genetic characteristics of the patient’s tumor.153 A CRC patient’s survival as well as quality of life depends on treatment decisions, and improved treatments and optimal combination of therapies continue to be goals.154 Some patients do not tolerate chemotherapy well, and enhanced quality-of-life research is needed for CRC patients, including palliative care. Best practices for treatments based on a patient’s needs, staging, preferences, and performance status (response to chemotherapy) need to be promoted and adopted. Research into treatment options that result in even small gains in CRC patient survival and performance requires large clinical trials before the treatment can be made available for general use,154 so ways to facilitate cancer drug approval are also needed.155
Disparities exist for CRC as well. Men have higher rates than women, and black persons have higher rates than other racial/ethnic groups. Geographic disparities have also been reported and may be influenced by access to health care and screening (in low-poverty areas) and by lifestyle factors (in high-poverty and urban areas).116, 156 Studies also indicate that black CRC patients are diagnosed more often at late stages and less often receive standard therapies than white patients;157 they also have less follow-up surveillance158 and poorer survival rates.159 More research is needed regarding the systemic, clinical, social, cultural, biological, environmental, and behavioral factors that influence CRC incidence, mortality, and disparities.
Although much progress can be achieved by better applying what we know about cancer causation, prevention, and treatment (e.g., tobacco control, vaccination for human papillomavirus, chemoprevention of breast cancer in high-risk groups), more research is needed across the spectrum of cancers in all areas: prevention, early detection, treatment, and palliation. Further etiologic research is needed for particularly lethal cancer sites (e.g., pancreatic), those with unexplained increased incidence (i.e., cancers of the thyroid, liver, pancreas, kidney and melanoma, Table 4), and cancers for which limited progress has been made. Extensive research efforts are also needed to develop personalized/targeted cancer therapies that involve a better understanding of the genetic and epigenetic changes that occur in cells during progression to cancer, the molecular composition of cancer subtypes, gene expression, and proteomics.160–163 A combination of policy, health care service delivery, communication, and engineering and technology interventions can further reduce the impact of cancer.
Supplementary Material
Acknowledgments
We thank Andrew Lake, Martin Krapcho, Rick Firth, and Neil Nayman of Information Management Services, Inc. for assisting in statistical analyses; Dr. Eric J. (Rocky) Feuer, Chief of the Statistical Research Applications Branch, Surveillance Research Program, National Cancer Institute and Program Director of the Colorectal CISNET collaborators for providing general guidance and technical review of material on models and their use for interpreting cancer trends. In addition we acknowledge the following programs for their efforts in data collection and distribution: hospital and population-based cancer registries, the SEER-Medicare and related linked data systems, CDC-NCHS National Vital Statistics System, and CDC-NCHS health survey systems of the NHIS, BRFSS, and the National Health and Nutrition Examination Survey (NHANES), Dr. Rhonda Ray contributed expertise as a public health science writer and Terri Harshman was an invaluable coordinating research assistant throughout development of this trans-agency report.
Footnotes
The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official positions of the Centers for Disease Control and Prevention.
References
- 1.Wingo PA, Ries LA, Rosenberg HM, Miller DS, Edwards BK. Cancer incidence and mortality, 1973–1995: a report card for the U.S. Cancer. 1998 Mar 15;82(6):1197–1207. doi: 10.1002/(sici)1097-0142(19980315)82:6<1197::aid-cncr26>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 2.Wingo PA, Ries LA, Giovino GA, et al. Annual report to the nation on the status of cancer, 1973–1996, with a special section on lung cancer and tobacco smoking. J Natl Cancer Inst. 1999 Apr 21;91(8):675–690. doi: 10.1093/jnci/91.8.675. [DOI] [PubMed] [Google Scholar]
- 3.Howe HL, Wingo PA, Thun MJ, et al. Annual report to the nation on the status of cancer (1973 through 1998), featuring cancers with recent increasing trends. J Natl Cancer Inst. 2001 Jun 6;93(11):824–842. doi: 10.1093/jnci/93.11.824. [DOI] [PubMed] [Google Scholar]
- 4.Edwards BK, Howe HL, Ries LA, et al. Annual report to the nation on the status of cancer, 1973–1999, featuring implications of age and aging on U.S. cancer burden. Cancer. 2002 May 15;94(10):2766–2792. doi: 10.1002/cncr.10593. [DOI] [PubMed] [Google Scholar]
- 5.Weir HK, Thun MJ, Hankey BF, et al. Annual report to the nation on the status of cancer, 1975–2000, featuring the uses of surveillance data for cancer prevention and control. J Natl Cancer Inst. 2003 Sep 3;95(17):1276–1299. doi: 10.1093/jnci/djg040. [DOI] [PubMed] [Google Scholar]
- 6.Jemal A, Clegg LX, Ward E, et al. Annual report to the nation on the status of cancer, 1975–2001, with a special feature regarding survival. Cancer. 2004 Jul 1;101(1):3–27. doi: 10.1002/cncr.20288. [DOI] [PubMed] [Google Scholar]
- 7.Edwards BK, Brown ML, Wingo PA, et al. Annual report to the nation on the status of cancer, 1975–2002, featuring population-based trends in cancer treatment. J Natl Cancer Inst. 2005 Oct 5;97(19):1407–1427. doi: 10.1093/jnci/dji289. [DOI] [PubMed] [Google Scholar]
- 8.Howe HL, Wu X, Ries LA, et al. Annual report to the nation on the status of cancer, 1975–2003, featuring cancer among U.S. Hispanic/Latino populations. Cancer. 2006 Oct 15;107(8):1711–1742. doi: 10.1002/cncr.22193. [DOI] [PubMed] [Google Scholar]
- 9.Espey DK, Wu XC, Swan J, et al. Annual report to the nation on the status of cancer, 1975–2004, featuring cancer in American Indians and Alaska Natives . Cancer. 2007 Oct 15;:2119–2152. doi: 10.1002/cncr.23044. [DOI] [PubMed] [Google Scholar]
- 10.Jemal A, Thun MJ, Ries LA, et al. Annual report to the nation on the status of cancer, 1975–2005, featuring trends in lung cancer, tobacco use, and tobacco control. J Natl Cancer Inst. 2008 Dec 3;100(23):1672–1694. doi: 10.1093/jnci/djn389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ries LA, Wingo PA, Miller DS, et al. The annual report to the nation on the status of cancer, 1973–1997, with a special section on colorectal cancer. Cancer. 2000 May 15;88(10):2398–2424. doi: 10.1002/(sici)1097-0142(20000515)88:10<2398::aid-cncr26>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- 12.Fritz A, Percy C, Jack A. International classification of diseases of oncology. Geneva, Switzerland: World Health Organization; 2000. [Google Scholar]
- 13.Horner MJ, Ries LAG, Krapcho M, et al. SEER Cancer Statistics Review 1975–2006. National Cancer Institute; May 29, 2009. [accessed August 17, 2009]. Available from: http://seer.cancer.gov/csr/1975_2006/index.html. [Google Scholar]
- 14.International statistical classification of diseases and related health problems. Geneva, Switzerland: World Health Organization; 1992. tenth revision. [Google Scholar]
- 15.Manual of the international statistical classification of diseases, injuries, and causes of death, adapted for use in the United States. Geneva, Switzerland: World Health Organization; 1948. 6th revision. 1948. [Google Scholar]
- 16.Manual of the international statistical classification of diseases, injuries, and causes of death, adapted for use in the United States. Geneva, Switzerland: World Health Organization; 1955. 7th revision. 1955. [Google Scholar]
- 17.Manual of the international statistical classification of diseases, injuries, and causes of death, adapted for use in the United States. Washington, DC: US Department of Health Education and Welfare, National Center for Health Statistics, Public Health Service; 1968. 8th revision, 1968. [Google Scholar]
- 18.Manual of the international statistical classification of diseases, injuries, and causes of death, based on the recommendations of the ninth revision conference, 1975. Geneva, Switzerland: World Health Organization; 1977. [Google Scholar]
- 19.Heron M, Hoyert DL, Murphy SL, Xu J, Kochanek KD, Tejada-Vera B. Deaths: final data for 2006. Natl Vital Stat Rep. 2009 Apr 17;57(14):1–134. [PubMed] [Google Scholar]
- 20.National Cancer Institute. Surveillance Epidemiology and End Results (SEER) Program. Population estimates used in NCI’s SEER*Stat software. Available from URL: http://seer.cancer.gov/popdata/methods.html.
- 21.Centers for Disease Control and Prevention. National Center for Health Statistics. National Vital Statistics System. U.S. census populations with bridged race categories. [Accessed on March 20, 2008]. Available from URL: http://www.cdc.gov/nchs/about/major/dvs/popbridge/popbridge.htm.
- 22.Surveillance, Epidemiology, and End Results (SEER) Program. www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER 9 Regs Public-Use, Nov 2008 Sub (1973–2006), National Cancer Institute, DCCPS, Surveillance Research Program, Cancer Statistics Branch, released April 2009, based on the November 2008 submission.; 2008.
- 23.Surveillance Research Program, National Cancer Institute SEER*Stat software ( NCI; 2009. www.seer.cancer.gov/seerstat) version 6.5.2. [Google Scholar]
- 24.Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000 Feb 15;19(3):335–351. doi: 10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 25.Clegg LX, Feuer EJ, Midthune DN, Fay MP, Hankey BF. Impact of reporting delay and reporting error on cancer incidence rates and trends. J Natl Cancer Inst. 2002 Oct 16;94(20):1537–1545. doi: 10.1093/jnci/94.20.1537. [DOI] [PubMed] [Google Scholar]
- 26.NCI. Average Annual Percent Change (AAPC) [accessed 09/09/09]. Available from: http://srab.cancer.gov/joinpoint/aapc.html.
- 27.Clegg LX, Hankey BF, Tiwari R, Feuer EJ, Edwards BK. Estimating average annual percent change in trend analysis. Statistics in Medicine. 2009 doi: 10.1002/sim.3733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Feuer EJ, Etzioni R, Cronin KA, Mariotto A. The use of modeling to understand the impact of screening on U.S. mortality: examples from mammography and PSA testing. Stat Methods Med Res. 2004 Dec;13(6):421–442. doi: 10.1191/0962280204sm376ra. [DOI] [PubMed] [Google Scholar]
- 29.Vogelaar I, van Ballegooijen M, Schrag D, et al. How much can current interventions reduce colorectal cancer mortality in the U.S.? Mortality projections for scenarios of risk-factor modification, screening, and treatment. Cancer. 2006 Oct 1;107(7):1624–1633. doi: 10.1002/cncr.22115. [DOI] [PubMed] [Google Scholar]
- 30.NCI. Colorectal Cancer Mortality Projections. Bethesda: 2007. [Google Scholar]
- 31.NCI. Cancer Intervention and Surveillance Modeling Network (CISNET) [accessed August 20, 2009]. Available from: http://cisnet.cancer.gov/
- 32.Morson B. President’s address. The polyp-cancer sequence in the large bowel. Proc R Soc Med. 1974 Jun;67(6 Pt 1):451–457. [PMC free article] [PubMed] [Google Scholar]
- 33.Morson BC. Evolution of cancer of the colon and rectum. Cancer. 1974 Sep;34(3):845–849. doi: 10.1002/1097-0142(197409)34:3+<845::aid-cncr2820340710>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 34.Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975 Dec;36(6):2251–2270. doi: 10.1002/cncr.2820360944. [DOI] [PubMed] [Google Scholar]
- 35.Lansdorp-Vogelaar I, van Ballegooijen M, Zauber AG, Boer R, Wilschut J, Habbema JD. At what costs will screening with CT colonography be competitive? A cost-effectiveness approach. Int J Cancer. 2009 Mar 1;124(5):1161–1118. doi: 10.1002/ijc.24025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zauber AG, Lansdorp-Vogelaar I, Knudsen AB, Wilschut J, van Ballegooijen M, Kuntz KM. Evaluating test strategies for colorectal cancer screening: a decision analysis for the U.S. Preventive Services Task Force. Ann Intern Med. 2008 Nov 4;149(9):659–669. doi: 10.7326/0003-4819-149-9-200811040-00244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.NCI . Cancer progress report - 2003 update. NCI, NIH, DHHS; Feb, 2004. [Google Scholar]
- 38.National Center for Health Statistics. Data File Documentation, National Health Interview Survey, 2003 (machine-readable data file and documentation) [monograph online] [accessed May 22, 2006]. Available from: http://www.cdc.gov/nchs/nhis.htm.
- 39.Winawer SJ. The multidisciplinary management of gastrointestinal cancer. Colorectal cancer screening. Best Pract Res Clin Gastroenterol. 2007;21(6):1031–1048. doi: 10.1016/j.bpg.2007.09.004. [DOI] [PubMed] [Google Scholar]
- 40.Andre T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004 Jun 3;350(23):2343–2351. doi: 10.1056/NEJMoa032709. [DOI] [PubMed] [Google Scholar]
- 41.Efficacy of adjuvant fluorouracil and folinic acid in B2 colon cancer. International Multicentre Pooled Analysis of B2 Colon Cancer Trials (IMPACT B2) Investigators. J Clin Oncol. 1999 May;17(5):1356–1363. [PubMed] [Google Scholar]
- 42.Cunningham D, Humblet Y, Siena S, et al. Cetuximab monotherapy and cetuximab plus irinotecan in irinotecan-refractory metastatic colorectal cancer. N Engl J Med. 2004 Jul 22;351(4):337–345. doi: 10.1056/NEJMoa033025. [DOI] [PubMed] [Google Scholar]
- 43.de Gramont A, Figer A, Seymour M, et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J Clin Oncol. 2000 Aug;18(16):2938–2947. doi: 10.1200/JCO.2000.18.16.2938. [DOI] [PubMed] [Google Scholar]
- 44.Efficacy of adjuvant fluorouracil and folinic acid in colon cancer. International Multicentre Pooled Analysis of Colon Cancer Trials (IMPACT) investigators. Lancet. 1995 Apr 15;345(8955):939–944. [PubMed] [Google Scholar]
- 45.Goldberg RM, Sargent DJ, Morton RF, et al. A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol. 2004 Jan 1;22(1):23–30. doi: 10.1200/JCO.2004.09.046. [DOI] [PubMed] [Google Scholar]
- 46.Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004 Jun 3;350(23):2335–2342. doi: 10.1056/NEJMoa032691. [DOI] [PubMed] [Google Scholar]
- 47.Moertel CG, Fleming TR, Macdonald JS, et al. Fluorouracil plus levamisole as effective adjuvant therapy after resection of stage III colon carcinoma: a final report. Ann Intern Med. 1995 Mar 1;122(5):321–326. doi: 10.7326/0003-4819-122-5-199503010-00001. [DOI] [PubMed] [Google Scholar]
- 48.Moertel CG, Fleming TR, Macdonald JS, et al. Intergroup study of fluorouracil plus levamisole as adjuvant therapy for stage II/Dukes’ B2 colon cancer. J Clin Oncol. 1995 Dec;13(12):2936–2943. doi: 10.1200/JCO.1995.13.12.2936. [DOI] [PubMed] [Google Scholar]
- 49.Saltz LB, Cox JV, Blanke C, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med. 2000 Sep 28;343(13):905–914. doi: 10.1056/NEJM200009283431302. [DOI] [PubMed] [Google Scholar]
- 50.Saltz LB, Niedzwiecki D, Hollis D, et al. Irinotecan plus fluorouracil/leucovorin (IFL) versus fluorouracil/leucovorin alone (FL) in stage III colon cancer (intergroup trial CALGB C89803) J Clin Oncol. 2004;22 (Supplement):1. [Google Scholar]
- 51.Tournigand C, Andre T, Achille E, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004 Jan 15;22(2):229–237. doi: 10.1200/JCO.2004.05.113. [DOI] [PubMed] [Google Scholar]
- 52.Gill S, Loprinzi CL, Sargent DJ, et al. Pooled analysis of fluorouracil-based adjuvant therapy for stage II and III colon cancer: who benefits and by how much? J Clin Oncol. 2004 May 15;22(10):1797–1806. doi: 10.1200/JCO.2004.09.059. [DOI] [PubMed] [Google Scholar]
- 53.Warren JL, Harlan LC, Fahey A, et al. Utility of the SEER-Medicare data to identify chemotherapy use. Med Care. 2002 Aug;40(8 Suppl):IV-55–61. doi: 10.1097/01.MLR.0000020944.17670.D7. [DOI] [PubMed] [Google Scholar]
- 54.Ayanian JZ, Zaslavsky AM, Fuchs CS, et al. Use of adjuvant chemotherapy and radiation therapy for colorectal cancer in a population-based cohort. J Clin Oncol. 2003 Apr 1;21(7):1293–1300. doi: 10.1200/JCO.2003.06.178. [DOI] [PubMed] [Google Scholar]
- 55.Potosky AL, Harlan LC, Kaplan RS, Johnson KA, Lynch CF. Age, sex, and racial differences in the use of standard adjuvant therapy for colorectal cancer. J Clin Oncol. 2002 Mar 1;20(5):1192–1202. doi: 10.1200/JCO.2002.20.5.1192. [DOI] [PubMed] [Google Scholar]
- 56.Andriole GL, Crawford ED, Grubb RL, 3rd, et al. Mortality results from a randomized prostate-cancer screening trial. N Engl J Med. 2009 Mar 26;360(13):1310–1319. doi: 10.1056/NEJMoa0810696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Schroder FH, Hugosson J, Roobol MJ, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med. 2009 Mar 26;360(13):1320–1328. doi: 10.1056/NEJMoa0810084. [DOI] [PubMed] [Google Scholar]
- 58.Tsodikov A, Szabo A, Wegelin J. A population model of prostate cancer incidence. Stat Med. 2006 Aug 30;25(16):2846–2866. doi: 10.1002/sim.2257. [DOI] [PubMed] [Google Scholar]
- 59.Etzioni R, Tsodikov A, Mariotto A, et al. Quantifying the role of PSA screening in the US prostate cancer mortality decline. Cancer Causes Control. 2008 Mar;19(2):175–181. doi: 10.1007/s10552-007-9083-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Draisma G, Etzioni R, Tsodikov A, et al. Lead time and overdiagnosis in prostate-specific antigen screening: importance of methods and context. J Natl Cancer Inst. 2009 Mar 18;101(6):374–383. doi: 10.1093/jnci/djp001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Berry DA, Cronin KA, Plevritis SK, et al. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005 Oct 27;353(17):1784–1792. doi: 10.1056/NEJMoa050518. [DOI] [PubMed] [Google Scholar]
- 62.ACS. Cancer Facts & Figures 2009. Atlanta: American Cancer Society; 2009. [Google Scholar]
- 63.Sloane D. Cancer epidemiology in the United States: racial, social, and economic factors. Methods Mol Biol. 2009;471:65–83. doi: 10.1007/978-1-59745-416-2_4. [DOI] [PubMed] [Google Scholar]
- 64.Kolb B, Wallace AM, Hill D, Royce M. Disparities in cancer care among racial and ethnic minorities. Oncology (Williston Park) 2006 Sep;20(10):1256–1261. discussion 1261, 1265, 1268–1270. [PubMed] [Google Scholar]
- 65.Center MM, Jemal A, Ward E. International trends in colorectal cancer incidence rates. Cancer Epidemiol Biomarkers Prev. 2009 Jun;18(6):1688–1694. doi: 10.1158/1055-9965.EPI-09-0090. [DOI] [PubMed] [Google Scholar]
- 66.Umar A, Greenwald P. Alarming colorectal cancer incidence trends: a case for early detection and prevention. Cancer Epidemiol Biomarkers Prev. 2009 Jun;18(6):1672–1623. doi: 10.1158/1055-9965.EPI-09-0320. [DOI] [PubMed] [Google Scholar]
- 67.Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics. CA Cancer J Clin. 2009 Jul-Aug;59(4):225–249. doi: 10.3322/caac.20006. [DOI] [PubMed] [Google Scholar]
- 68.Siegel RL, Jemal A, Ward EM. Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol Biomarkers Prev. 2009 Jun;18(6):1695–1698. doi: 10.1158/1055-9965.EPI-09-0186. [DOI] [PubMed] [Google Scholar]
- 69.Fairley TL, Cardinez CJ, Martin J, et al. Colorectal cancer in U.S. adults younger than 50 years of age, 1998–2001. Cancer. 2006 Sep 1;107(5 Suppl):1153–1161. doi: 10.1002/cncr.22012. [DOI] [PubMed] [Google Scholar]
- 70.Meissner HI, Breen N, Klabunde CN, Vernon SW. Patterns of colorectal cancer screening uptake among men and women in the United States. Cancer Epidemiol Biomarkers Prev. 2006 Feb;15(2):389–394. doi: 10.1158/1055-9965.EPI-05-0678. [DOI] [PubMed] [Google Scholar]
- 71.Shapiro JA, Seeff LC, Thompson TD, Nadel MR, Klabunde CN, Vernon SW. Colorectal cancer test use from the 2005 National Health Interview Survey. Cancer Epidemiol Biomarkers Prev. 2008 Jul;17(7):1623–1630. doi: 10.1158/1055-9965.EPI-07-2838. [DOI] [PubMed] [Google Scholar]
- 72.Brown ML, Potosky AL. The presidential effect: the public health response to media coverage about Ronald Reagan’s colon cancer episode. Public Opin Q. 1990 Fall;54(3):317–329. doi: 10.1086/269209. [DOI] [PubMed] [Google Scholar]
- 73.Mandel JS, Bond JH, Church TR, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study. N Engl J Med. 1993 May 13;328(19):1365–1371. doi: 10.1056/NEJM199305133281901. [DOI] [PubMed] [Google Scholar]
- 74.Mandel JS, Church TR, Bond JH, et al. The effect of fecal occult-blood screening on the incidence of colorectal cancer. N Engl J Med. 2000 Nov 30;343(22):1603–1607. doi: 10.1056/NEJM200011303432203. [DOI] [PubMed] [Google Scholar]
- 75.Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology. 2008 May;134(5):1570–1595. doi: 10.1053/j.gastro.2008.02.002. [DOI] [PubMed] [Google Scholar]
- 76.Winawer SJ, Zauber AG, Fletcher RH, et al. Guidelines for colonoscopy surveillance after polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer and the American Cancer Society. Gastroenterology. 2006 May;130(6):1872–1885. doi: 10.1053/j.gastro.2006.03.012. [DOI] [PubMed] [Google Scholar]
- 77.Screening for colorectal cancer: U. S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008 Nov 4;149(9):627–637. doi: 10.7326/0003-4819-149-9-200811040-00243. [DOI] [PubMed] [Google Scholar]
- 78.Seeff LC, Richards TB, Shapiro JA, et al. How many endoscopies are performed for colorectal cancer screening? Results from CDC’s survey of endoscopic capacity. Gastroenterology. 2004 Dec;127(6):1670–1677. doi: 10.1053/j.gastro.2004.09.051. [DOI] [PubMed] [Google Scholar]
- 79.Seeff LC, Nadel MR, Klabunde CN, et al. Patterns and predictors of colorectal cancer test use in the adult U.S. population. Cancer. 2004 May 15;100(10):2093–2103. doi: 10.1002/cncr.20276. [DOI] [PubMed] [Google Scholar]
- 80.Klabunde CN, Lanier D, Nadel MR, McLeod C, Yuan G, Vernon SW. Colorectal cancer screening by primary care physicians: recommendations and practices, 2006–2007. Am J Prev Med. 2009 Jul;37(1):8–16. doi: 10.1016/j.amepre.2009.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Warren JL, Klabunde CN, Mariotto AB, et al. Adverse events after outpatient colonoscopy in the Medicare population. Ann Intern Med. 2009 Jun 16;150(12):849–857. W152. doi: 10.7326/0003-4819-150-12-200906160-00008. [DOI] [PubMed] [Google Scholar]
- 82.Schatzkin A, Freedman LS, Dawsey SM, Lanza E. Interpreting precursor studies: what polyp trials tell us about large-bowel cancer. J Natl Cancer Inst. 1994 Jul 20;86(14):1053–1057. doi: 10.1093/jnci/86.14.1053. [DOI] [PubMed] [Google Scholar]
- 83.Bernstein CN, McKeown I, Embil JM, et al. Seroprevalence of Helicobacter pylori, incidence of gastric cancer, and peptic ulcer-associated hospitalizations in a Canadian Indian population. Dig Dis Sci. 1999 Apr;44(4):668–674. doi: 10.1023/a:1026689103952. [DOI] [PubMed] [Google Scholar]
- 84.Johns LE, Houlston RS. A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol. 2001 Oct;96(10):2992–3003. doi: 10.1111/j.1572-0241.2001.04677.x. [DOI] [PubMed] [Google Scholar]
- 85.Butterworth AS, Higgins JP, Pharoah P. Relative and absolute risk of colorectal cancer for individuals with a family history: a meta-analysis. Eur J Cancer. 2006 Jan;42(2):216–227. doi: 10.1016/j.ejca.2005.09.023. [DOI] [PubMed] [Google Scholar]
- 86.Lynch HT, de la Chapelle A. Hereditary colorectal cancer. N Engl J Med. 2003 Mar 6;348(10):919–932. doi: 10.1056/NEJMra012242. [DOI] [PubMed] [Google Scholar]
- 87.Recommendations from the EGAPP Working Group: genetic testing strategies in newly diagnosed individuals with colorectal cancer aimed at reducing morbidity and mortality from Lynch syndrome in relatives. Genet Med. 2009 Jan;11(1):35–41. doi: 10.1097/GIM.0b013e31818fa2ff. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Danaei G, Ding EL, Mozaffarian D, et al. The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med. 2009 Apr 28;6(4):1–23. doi: 10.1371/journal.pmed.1000058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Samad AK, Taylor RS, Marshall T, Chapman MA. A meta-analysis of the association of physical activity with reduced risk of colorectal cancer. Colorectal Dis. 2005 May;7(3):204–213. doi: 10.1111/j.1463-1318.2005.00747.x. [DOI] [PubMed] [Google Scholar]
- 90.Tomeo CA, Colditz GA, Willett WC, et al. Harvard Report on Cancer Prevention. Volume 3: prevention of colon cancer in the United States. Cancer Causes Control. 1999 Jun;10(3):167–180. doi: 10.1023/a:1017117109568. [DOI] [PubMed] [Google Scholar]
- 91.Colditz GA, Cannuscio CC, Frazier AL. Physical activity and reduced risk of colon cancer: implications for prevention. Cancer Causes Control. 1997 Jul;8(4):649–667. doi: 10.1023/a:1018458700185. [DOI] [PubMed] [Google Scholar]
- 92.Larsson SC, Wolk A. Obesity and colon and rectal cancer risk: a meta-analysis of prospective studies. Am J Clin Nutr. 2007 Sep;86(3):556–565. doi: 10.1093/ajcn/86.3.556. [DOI] [PubMed] [Google Scholar]
- 93.Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003 Apr 24;348(17):1625–1638. doi: 10.1056/NEJMoa021423. [DOI] [PubMed] [Google Scholar]
- 94.Hu FB, Willett WC, Li T, Stampfer MJ, Colditz GA, Manson JE. Adiposity as compared with physical activity in predicting mortality among women. N Engl J Med. 2004 Dec 23;351(26):2694–2703. doi: 10.1056/NEJMoa042135. [DOI] [PubMed] [Google Scholar]
- 95.Wang Y, Jacobs EJ, Patel AV, et al. A prospective study of waist circumference and body mass index in relation to colorectal cancer incidence. Cancer Causes Control. 2008 Sep;19(7):783–792. doi: 10.1007/s10552-008-9141-x. [DOI] [PubMed] [Google Scholar]
- 96.Pischon T, Lahmann PH, Boeing H, et al. Body size and risk of colon and rectal cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC) J Natl Cancer Inst. 2006 Jul 5;98(13):920–931. doi: 10.1093/jnci/djj246. [DOI] [PubMed] [Google Scholar]
- 97.Hawley ST, Volk RJ, Krishnamurthy P, Jibaja-Weiss M, Vernon SW, Kneuper S. Preferences for colorectal cancer screening among racially/ethnically diverse primary care patients. Med Care. 2008 Sep;46(9 Suppl 1):S10–16. doi: 10.1097/MLR.0b013e31817d932e. [DOI] [PubMed] [Google Scholar]
- 98.Hu F. Obesity Epidemiology. New York: Oxford University Press; 2008. [Google Scholar]
- 99.Giovannucci E. Metabolic syndrome, hyperinsulinemia, and colon cancer: a review. Am J Clin Nutr. 2007 Sep;86(3):836–842S. doi: 10.1093/ajcn/86.3.836S. [DOI] [PubMed] [Google Scholar]
- 100.Larsson SC, Orsini N, Wolk A. Diabetes mellitus and risk of colorectal cancer: a meta-analysis. J Natl Cancer Inst. 2005 Nov 16;97(22):1679–1687. doi: 10.1093/jnci/dji375. [DOI] [PubMed] [Google Scholar]
- 101.Chao A, Thun MJ, Connell CJ, et al. Meat consumption and risk of colorectal cancer. JAMA. 2005 Jan 12;293(2):172–182. doi: 10.1001/jama.293.2.172. [DOI] [PubMed] [Google Scholar]
- 102.Cronin KA, Krebs-Smith SM, Feuer EJ, Troiano RP, Ballard-Barbash R. Evaluating the impact of population changes in diet, physical activity, and weight status on population risk for colon cancer (United States) Cancer Causes Control. 2001 May;12(4):305–316. doi: 10.1023/a:1011244700531. [DOI] [PubMed] [Google Scholar]
- 103.Khan LK, Sobush K, Keener D, et al. Recommended community strategies and measurements to prevent obesity in the United States. MMWR Recomm Rep. 2009 Jul 24;58(RR-7):1–26. [PubMed] [Google Scholar]
- 104.IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans: Tobacco Smoke and Involuntary Smoking. Lyon: 2004. [PMC free article] [PubMed] [Google Scholar]
- 105.DHHS. The Health Consequences of Smoking: A Report from the Surgeon General. Washington, DC: 2004. [Google Scholar]
- 106.Botteri E, Iodice S, Raimondi S, Maisonneuve P, Lowenfels AB. Cigarette smoking and adenomatous polyps: a meta-analysis. Gastroenterology. 2008 Feb;134(2):388–395. doi: 10.1053/j.gastro.2007.11.007. [DOI] [PubMed] [Google Scholar]
- 107.Chao A, Thun MJ, Jacobs EJ, Henley SJ, Rodriguez C, Calle EE. Cigarette smoking and colorectal cancer mortality in the cancer prevention study II. J Natl Cancer Inst. 2000 Dec 6;92(23):1888–1896. doi: 10.1093/jnci/92.23.1888. [DOI] [PubMed] [Google Scholar]
- 108.Giovannucci E. An updated review of the epidemiological evidence that cigarette smoking increases risk of colorectal cancer. Cancer Epidemiol Biomarkers Prev. 2001 Jul;10(7):725–731. [PubMed] [Google Scholar]
- 109.Paskett ED, Reeves KW, Rohan TE, et al. Association between cigarette smoking and colorectal cancer in the Women’s Health Initiative. J Natl Cancer Inst. 2007 Nov 21;99(22):1729–1735. doi: 10.1093/jnci/djm176. [DOI] [PubMed] [Google Scholar]
- 110.Cuzick J, Otto F, Baron JA, et al. Aspirin and non-steroidal anti-inflammatory drugs for cancer prevention: an international consensus statement. Lancet Oncol. 2009 May;10(5):501–507. doi: 10.1016/S1470-2045(09)70035-X. [DOI] [PubMed] [Google Scholar]
- 111.Chan AT, Ogino S, Fuchs CS. Aspirin use and survival after diagnosis of colorectal cancer. JAMA. 2009 Aug 12;302(6):649–658. doi: 10.1001/jama.2009.1112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Flossmann E, Rothwell PM. Effect of aspirin on long-term risk of colorectal cancer: consistent evidence from randomised and observational studies. Lancet. 2007 May 12;369(9573):1603–1613. doi: 10.1016/S0140-6736(07)60747-8. [DOI] [PubMed] [Google Scholar]
- 113.Thun MJ, Henley SJ, Patrono C. Nonsteroidal anti-inflammatory drugs as anticancer agents: mechanistic, pharmacologic, and clinical issues. J Natl Cancer Inst. 2002 Feb 20;94(4):252–266. doi: 10.1093/jnci/94.4.252. [DOI] [PubMed] [Google Scholar]
- 114.Cho E, Smith-Warner SA, Spiegelman D, et al. Dairy foods, calcium, and colorectal cancer: a pooled analysis of 10 cohort studies. J Natl Cancer Inst. 2004 Jul 7;96(13):1015–1022. doi: 10.1093/jnci/djh185. [DOI] [PubMed] [Google Scholar]
- 115.Hao Y, Jemal A, Zhang X, Ward EM. Trends in colorectal cancer incidence rates by age, race/ethnicity, and indices of access to medical care, 1995–2004 (United States) Cancer Causes Control. 2009 Jun 19; doi: 10.1007/s10552-009-9379-y. [DOI] [PubMed] [Google Scholar]
- 116.Wu X, Cokkinides V, Chen VW, et al. Associations of subsite-specific colorectal cancer incidence rates and stage of disease at diagnosis with county-level poverty, by race and sex. Cancer. 2006 Sep 1;107(5 Suppl):1121–1117. doi: 10.1002/cncr.22009. [DOI] [PubMed] [Google Scholar]
- 117.NCI. A snapshot of colorectal cancer. NCI-Office of Science Planning and Assessment (OSPA) Sep, 2008. [accessed August 21, 2009]. Available from: http://planning.cancer.gov/disease/Colorectal-Snapshot.pdf.
- 118.Mariotto AB, Yabroff KR, Feuer EJ, De Angelis R, Brown M. Projecting the number of patients with colorectal carcinoma by phases of care in the US: 2000–2020. Cancer Causes Control. 2006 Dec;17(10):1215–1226. doi: 10.1007/s10552-006-0072-0. [DOI] [PubMed] [Google Scholar]
- 119.Yabroff KR, Davis WW, Lamont EB, et al. Patient time costs associated with cancer care. J Natl Cancer Inst. 2007 Jan 3;99(1):14–23. doi: 10.1093/jnci/djk001. [DOI] [PubMed] [Google Scholar]
- 120.Howlader N, Ries LA, Stinchcomb DG, Edwards BK. The impact of underreported Veterans Affairs data on national cancer statistics: analysis using population-based SEER registries. J Natl Cancer Inst. 2009 Apr 1;101(7):533–536. doi: 10.1093/jnci/djn517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Nelson DE, Powell-Griner E, Town M, Kovar MG. A comparison of national estimates from the National Health Interview Survey and the Behavioral Risk Factor Surveillance System. Am J Public Health. 2003 Aug;93(8):1335–1341. doi: 10.2105/ajph.93.8.1335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Link MW, Battaglia MP, Frankel MR, Osborn L, Mokdad AH. Address-based versus random-digit-dial surveys: comparison of key health and risk indicators. Am J Epidemiol. 2006 Nov 15;164(10):1019–1025. doi: 10.1093/aje/kwj310. [DOI] [PubMed] [Google Scholar]
- 123.Miller BA, Chu KC, Hankey BF, Ries LA. Cancer incidence and mortality patterns among specific Asian and Pacific Islander populations in the U.S. Cancer Causes Control. 2008 Apr;19(3):227–256. doi: 10.1007/s10552-007-9088-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Howe HL, Lake A, Schymura MJ, Edwards BK. Indirect method to estimate specific Hispanic group cancer rates. Cancer Causes Control. 2009 Sep;20:1215–1226. doi: 10.1007/s10552-009-9398-8. [DOI] [PubMed] [Google Scholar]
- 125.Espey DK, Wiggins C, Jim MA, Miller BA, Johnson CJ, Becker TM. Methods for improving cancer surveillance data in American Indian and Alaska Native Populations, CANCER, 2008, in press. Cancer. 2008 Sep 1;113(S5):1120–1130. doi: 10.1002/cncr.23724. [DOI] [PubMed] [Google Scholar]
- 126.Wingo PA, Tucker TC, Jamison PM, et al. Cancer in Appalachia, 2001–2003. Cancer. 2008 Jan 1;112(1):181–192. doi: 10.1002/cncr.23132. [DOI] [PubMed] [Google Scholar]
- 127.Lengerich EJ, Tucker TC, Powell RK, et al. Cancer incidence in Kentucky, Pennsylvania, and West Virginia: disparities in Appalachia. J Rural Health. 2005 Winter;21(1):39–47. doi: 10.1111/j.1748-0361.2005.tb00060.x. [DOI] [PubMed] [Google Scholar]
- 128.Becker TM, DKE, Lawson H, Saraiya M, Jim M, Waxman A. Regional differences in cervical cancer incidence among American Indians and Alaska Natives, 1999–2004. Cancer. 2008 doi: 10.1002/cncr.23736. In press. [DOI] [PubMed] [Google Scholar]
- 129.Arias E, Schauman WS, Eschbach K, Sorlie PD, Backlund E. The validity of race and Hispanic origin reporting on death certificates in the United States. National Center for Health Statistics, CDC; Oct, 2008. [PubMed] [Google Scholar]
- 130.Institute of Medicine. Ending the Tobacco Problem: A Blueprint for the Nation. Washington, D.C: National Academy Press; 2007. [Google Scholar]
- 131.Centers for Disease Control and Prevention. Best Practices for Comprehensive Tobacco Control Programs-2007. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; Oct, 2007. [Google Scholar]
- 132.IARC. Weight control and physical activity. Lyon: International Agency for Research on Cancer; 2002. [Google Scholar]
- 133.WCRF/AICR. Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Washington, DC: World Cancer Research Fund/American Institute for Cancer Research; 2007. [Google Scholar]
- 134.Kushi LH, Byers T, Doyle C, et al. American Cancer Society Guidelines on Nutrition and Physical Activity for cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin. 2006 Sep-Oct;56(5):254–281. doi: 10.3322/canjclin.56.5.254. quiz 313–254. [DOI] [PubMed] [Google Scholar]
- 135.Harriss DJ, Atkinson G, Batterham A, et al. Lifestyle factors and colorectal cancer risk (2): a systematic review and meta-analysis of associations with leisure-time physical activity. Colorectal Dis. 2009 Sep;11(7):689–701. doi: 10.1111/j.1463-1318.2009.01767.x. [DOI] [PubMed] [Google Scholar]
- 136.CDC. CDC Weight of the Nation Conference. [accessed August 19, 2009]. Available from: http://www.cdc.gov/media/transcripts/2009/t090727.htm.
- 137.Finkelstein EA, Brown DS, Wrage LA, Allaire BT, Hoerger TJ. Individual and Aggregate Years-of-Life-Lost Associated With Overweight and Obesity. Obesity (Silver Spring) 2009 Aug 13; doi: 10.1038/oby.2009.253. [DOI] [PubMed] [Google Scholar]
- 138.Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual Medical Spending Attributable To Obesity: Payer- And Service-Specific Estimates. Health Aff (Millwood) 2009 Jul 29; doi: 10.1377/hlthaff.28.5.w822. [DOI] [PubMed] [Google Scholar]
- 139.Ravdin PM, Cronin KA, Howlader N, et al. The decrease in breast-cancer incidence in 2003 in the United States. N Engl J Med. 2007 Apr 19;356(16):1670–1674. doi: 10.1056/NEJMsr070105. [DOI] [PubMed] [Google Scholar]
- 140.Cronin KA, Ravdin PM, Edwards BK. Sustained lower rates of breast cancer in the United States. Breast Cancer Res Treat. 2009 Sep;117(1):223–224. doi: 10.1007/s10549-008-0226-8. [DOI] [PubMed] [Google Scholar]
- 141.Katalinic A, Rawal R. Decline in breast cancer incidence after decrease in utilisation of hormone replacement therapy. Breast Cancer Res Treat. 2008 Feb;107(3):427–430. doi: 10.1007/s10549-007-9566-z. [DOI] [PubMed] [Google Scholar]
- 142.Mason JB, Dickstein A, Jacques PF, et al. A temporal association between folic acid fortification and an increase in colorectal cancer rates may be illuminating important biological principles: a hypothesis. Cancer Epidemiol Biomarkers Prev. 2007 Jul;16(7):1325–1329. doi: 10.1158/1055-9965.EPI-07-0329. [DOI] [PubMed] [Google Scholar]
- 143.NCI. Colorectal Cancer: Six Years of Research Progress. 2008 Mar; [Google Scholar]
- 144.Houlston RS, Webb E, Broderick P, et al. Meta-analysis of genome-wide association data identifies four new susceptibility loci for colorectal cancer. Nat Genet. 2008 Dec;40(12):1426–1435. doi: 10.1038/ng.262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Taplin SH, Haggstrom D, Jacobs T, et al. Implementing colorectal cancer screening in community health centers: addressing cancer health disparities through a regional cancer collaborative. Med Care. 2008 Sep;46(9 Suppl 1):S74–83. doi: 10.1097/MLR.0b013e31817fdf68. [DOI] [PubMed] [Google Scholar]
- 146.Zapka J. Innovative provider- and health system-directed approaches to improving colorectal cancer screening delivery. Med Care. 2008 Sep;46(9 Suppl 1):S62–67. doi: 10.1097/MLR.0b013e31817fdf57. [DOI] [PubMed] [Google Scholar]
- 147.NCCRT. National Colorectal Cancer Roundtable. [accessed September 16, 2009]. Available from: http://www.nccrt.org/
- 148.NIH. NIH State-of-the Science Conference: Enhancing use and quality of colorectal cancer screening NIH. Aug 26, 2009. Available from: http://consensus.nih.gov/ [PubMed]
- 149.Hosein PJ, Rocha-Lima CM. Role of combined-modality therapy in the management of locally advanced rectal cancer. Clin Colorectal Cancer. 2008 Nov;7(6):369–375. doi: 10.3816/CCC.2008.n.049. [DOI] [PubMed] [Google Scholar]
- 150.Kopetz S, Chang GJ, Overman MJ, et al. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J Clin Oncol. 2009 Aug 1;27(22):3677–3683. doi: 10.1200/JCO.2008.20.5278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Grothey A, Marshall JL. Optimizing palliative treatment of metastatic colorectal cancer in the era of biologic therapy. Oncology (Williston Park) 2007 Apr;21(5):553–564. 566. discussion 566–568, 577–578. [PubMed] [Google Scholar]
- 152.Hamilton SR. Targeted therapy of cancer: new roles for pathologists in colorectal cancer. Mod Pathol. 2008 May;21 (Suppl 2):S23–30. doi: 10.1038/modpathol.2008.14. [DOI] [PubMed] [Google Scholar]
- 153.Jiang Y, Kimchi ET, Staveley-O’Carroll KF, Cheng H, Ajani JA. Assessment of K-ras mutation: a step toward personalized medicine for patients with colorectal cancer. Cancer. 2009 Jun 12;115(16):3609–3617. doi: 10.1002/cncr.24434. [DOI] [PubMed] [Google Scholar]
- 154.Segal NH, Saltz LB. Evolving treatment of advanced colon cancer. Annu Rev Med. 2009;60:207–219. doi: 10.1146/annurev.med.60.041807.132435. [DOI] [PubMed] [Google Scholar]
- 155.Marshall JL, Gehan EA. The development of novel agents for the treatment of colorectal cancer: a critical review of current practice and some suggestions for the future. Clin Adv Hematol Oncol. 2007 Mar;5(3):167–172. [PubMed] [Google Scholar]
- 156.Lang K, Korn JR, Lee DW, Lines LM, Earle CC, Menzin J. Factors associated with improved survival among older colorectal cancer patients in the US: a population-based analysis. BMC Cancer. 2009;9:227. doi: 10.1186/1471-2407-9-227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Berry J, Bumpers K, Ogunlade V, et al. Examining racial disparities in colorectal cancer care. J Psychosoc Oncol. 2009;27(1):59–83. doi: 10.1080/07347330802614840. [DOI] [PubMed] [Google Scholar]
- 158.Rolnick S, Hensley Alford S, Kucera GP, et al. Racial and age differences in colon examination surveillance following a diagnosis of colorectal cancer. J Natl Cancer Inst Monogr. 2005(35):96–101. doi: 10.1093/jncimonographs/lgi045. [DOI] [PubMed] [Google Scholar]
- 159.Alexander DD, Waterbor J, Hughes T, Funkhouser E, Grizzle W, Manne U. African-American and Caucasian disparities in colorectal cancer mortality and survival by data source: an epidemiologic review. Cancer Biomark. 2007;3(6):301–313. doi: 10.3233/cbm-2007-3604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Chanock SJ, Hunter DJ. Genomics: when the smoke clears. Nature. 2008 Apr 3;452(7187):537–538. doi: 10.1038/452537a. [DOI] [PubMed] [Google Scholar]
- 161.Chin L, Gray JW. Translating insights from the cancer genome into clinical practice. Nature. 2008 Apr 3;452(7187):553–563. doi: 10.1038/nature06914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Carr KM, Rosenblatt K, Petricoin EF, Liotta LA. Genomic and proteomic approaches for studying human cancer: prospects for true patient-tailored therapy. Hum Genomics. 2004 Jan;1(2):134–140. doi: 10.1186/1479-7364-1-2-134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Feero WG, Guttmacher AE, Collins FS. The genome gets personal--almost. JAMA. 2008 Mar 19;299(11):1351–1312. doi: 10.1001/jama.299.11.1351. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.