

INTRODUCTION
Over the past decade, the concept of surgical care as a population-based, affordable, and globally relevant issue has gradually begun to emerge.[24,28,34,37] The facts are startling: more people die each year due to the inability to access surgical care than from human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS), tuberculosis, and malaria combined.[6] The highest incidence results from (in descending order) accidental trauma (bone and soft-tissue injuries), tumors, obstetrical complications (including obstetrical fistula), cataracts and glaucoma, perinatal conditions and congenital anomalies, male circumcision (prevention of HIV transmission) and a large group (19%) under the heading of “Other,” which include a variety of diagnoses such as hernia, gall bladder disease, infections requiring surgical care, etc.[4,6] However, the global burden of disease (GBD) associated with surgical and obstetrical care has yet to be adequately defined; current numbers are likely to be artificially low.[27,36] While the total volume of actual surgical cases can be tallied, the unmet surgical need is only beginning to be measured.[29] It is not without reason that surgery has been termed the “neglected stepchild” of global public health and the “neglected specialty in the current global health arena.”[7,8]
Historically, the primary barrier to developing surgical services has been the (mis)perception that surgery is overly expensive for the majority of lower and middle income countries (LMICs).[3] However, the World Bank published the 2nd edition of Disease Control Priorities in Developing Countries (DCP, 2006), which provided the first clear economic evidence that surgical care could be a cost-effective strategy under certain circumstances when compared with other types of care, such as antiretroviral medications, vaccinations, and other primary treatments. This economic impact was calculated on the basis of Disability Adjusted Life Years (DALYs), which is the sum of Years of Life Lost (YLL) plus the Years Lost due to Disability (YLDs) or simply: DALY = YLL + YLD. The purpose of surgery, however, is to alleviate or mitigate against certain physical conditions and the resultant “DALYs averted” reflects the reduction in calculated DALY as a consequence of the timely institution of appropriate surgical care. Surgical conditions account for 11% of global DALYs lost each year, with LMICs carrying the greatest burden; Southeast Asia plus Africa alone, accounted for 54% of DALYs in 2004.[6,9]
Emergency and essential surgical care is increasingly recognized as a critical element to improving primary health care delivery. In the World Health Report 2008—Primary Health Care (Now more than Ever), the World Health Organization (WHO) included Surgery for the first time within the Primary Healthcare Sphere of Care.[22,35] This report emphasized the creation of primary care teams responsible for defined populations with access to all aspects of care, which was not splintered by economic concerns or differences. While inserting one word on an organizational chart appears to be a small step, it was a huge leap forward that required years of continual effort.
Additionally, WHO has made surgical care a priority.[1,20] The Emergency and Essential Surgical care (EESC) of the WHO, has been active in the Global Initiative for Emergency and Essential Surgical Care (GIEESC), a forum of surgical experts. EESC has published the volume Surgical Care at the District Hospital (SCDH) in seven languages and produced the Integrated Management of Emergency and Essential Surgical Care (IMEESC) toolkit, a Compact Disc that contains the SCDH, a long list of best-practice protocols (including disaster management), multiple point-of-contact posters, and a number of instructional videos. Ongoing research within EESC includes a large database of surgical hospital capacity throughout the developing world (>700), capacity building through educational programs, and periodic follow-up of existing programs. Within the WHO, other areas of relating to surgery include Violence and Injury Prevention, Maternal and Child Health, HIV/AIDS (male circumcision), and transplantation.
Surgery is credited with providing a critical role in achieving the United Nations Millennium Development Goals (MDGs) and is most closely involved with numbers 4, 5, and 6.[23] Although most directly linked to these MDGs, surgical care also indirectly, but significantly contributes to MDG 1: The eradication of poverty and hunger. This is due to the fact that restoring health to the man who is a primary provider (such as repairing an inguinal hernia so that he can return to work) and/or the woman who provides for the home and children (such as relieving obstructed labor or repairing a vesico-vaginal fistula), greatly reduces economic loss and/or emotional hardship.
MDG 4: REDUCE CHILDHOOD MORTALITY
Both the 5% mortality of children under the age of 5 years resulting from injuries (approximately 345,000 children, 95% in LMICs, 2011) and the 7.6% mortality seen in neonatals (0-27 days) secondary to congenital anomalies (272,940, 2008), can be reduced by timely surgical intervention. Additionally, there is a 10-fold increased risk of premature death for over 1 million children left motherless each year, simply by not having a mother to provide sufficient care.[17,19]
MDG 5: IMPROVE MATERNAL HEALTH
Although declining, there are over 350,000 deaths per year due to complications of pregnancy, mainly postpartum hemorrhage and infection, both mainly treated with basic surgical techniques. In 2010, about 800 women died per day, (of these, 440 in Sub-Saharan Africa, 230 in Southern Asia, 5 in high-income countries). Additionally, 8% maternal deaths are due to obstructed labor (1-5/1000 live births), resulting in 50-100,000 women developing disabling obstetric fistulae annually. There are currently an estimated 1-2 million women permanently disabled as a result of fistulae, resulting in being outcast from family and society. The only tangible hope of returning to an acceptable quality of life and to their community is through surgery. Additionally, approximately 68,000 women die annually from unsafe abortions.[18,21]
MDG 6: COMBAT HIV/AIDS
Male circumcision has been shown to reduce the risk of men acquiring HIV through heterosexual intercourse by 60%.[2,10]
Significant other challenges to global surgical care are accessibility to care and the constricted surgical workforce. An estimated 234 million surgical and obstetrical procedures are performed globally each year, yet it is estimated that the wealthiest 4 billion people undergo 96.5% of the procedures, while the world's poorest 2 billion undergo the remaining mere 3.5%.[5,25] On average, only 46% of births are attended by skilled personnel in Sub-Saharan Africa, while Europe enjoys approximately 96% birthing assistance. This represents an enormous health care disparity for surgical care, which is similarly reflected in the requisite surgical personnel: Sub-Saharan Africa bears 24% of the GBD, yet contains only 11% of the global population, and only 3% of the world's health workers. Currently in Sub-Saharan Africa, on average, there is 1 surgeon per 2.5 million people (WHO guideline: 1 surgeon/20,000 population) and 1 trained physician anesthesiologist per 25 million people.[30]
For example, Uganda has 75 general surgeons for 27 million people (1 per 360,000); anesthesia is provided by 350 “anesthetic officers” who have received 18 months of training to complement a high-school qualification. Uganda also has 20 orthopedic surgeons, 3 cardiothoracic surgeons, 3 pediatric surgeons, 6 neurosurgeons, 3 plastic surgeons, and 3 urologists, yet this fills only 7.4% of projected need met [Figure 1].
Figure 1.
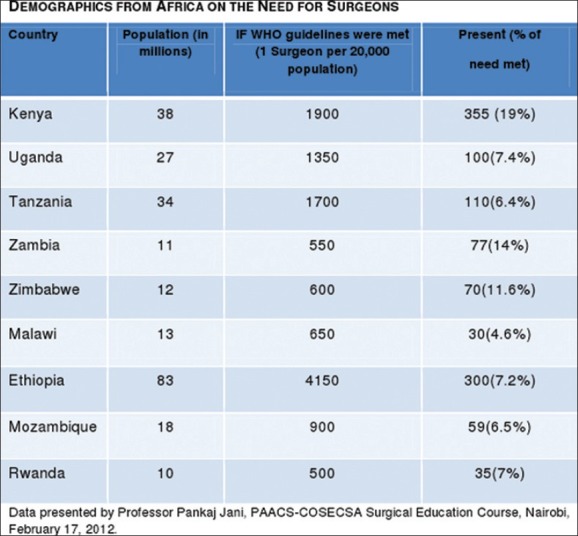
Demographics from Africa on the need for surgeons
METHODS
There are currently several methods that have been utilized to provide surgical care to LMICs. The traditional model has been to send a Western trained surgeon (generally Caucasian) to the country's interior, generally a very remote setting with a small, ill-equipped hospital, hoping that the surgeon would make a career of it as it is often impossible for him or her to be replaced. This model has been in existence for well over a hundred years; excellent examples would be Dr. Albert Schweitzer and his hospital in Lambaréné, Gabon and Dr. David Livingstone in central and southern Africa. This model is still, unfortunately, the prevailing paradigm throughout the developing world, especially among faith-based organization (FBO) hospitals.
An extension of this model and the basis for its continued survival has been the utilization of short-term (ST) surgeons who provided varying interims of service as either a stop-gap measure or as recurring, but intermittent service. While this satisfies acute necessities, it often fails to provide long-term results, more often positively impacting the ST surgeon much more than the local hospital or population.
More recently, the concept of institutional “twinning” has become prevalent, where a Western university (often a single department) partners with a similar institution (or department) within an LMIC and develops academic relationships in surgical expertise and/or research.[31,32] Good examples are the University of California San Francisco's Program in Surgery and Global Health;[14,26] Harvard's Department of Global Health and Social Medicine, including the Program in Global Surgery and Social Change;[12] Duke Global Surgery, partnering with Duke Global Health Institute;[11,15] University of North Carolina Institute for Global Health and Infectious Diseases;[13] and Loma Linda University Global Health Institute, among others.[16]
A newer model is one of developing surgical training programs within LMICs for training local physicians as surgeons to care for their own people in their own country. These individuals are much more culturally aware, communicate in local dialects, become excellent role models to local young people, and may not suffer the frequent psychological strains that ex-patriots are prone to exhibit. An excellent example this is the Pan-African Academy of Christian Surgeons (PAACS) that began general surgery training programs in Africa in 1996. PAACS now consists of eight 5-year programs, training a total of 43 residents in six countries, with a stated goal of training 100 African surgeons by 2020.[33] Each of these programs has full accreditation from College of Surgery of Eastern, Central and South Africa (COSECSA) and/or the West African College of Surgeons (WACS). There are plans for additional training programs to become active in Malawi (2013), and Tanzania (2013), and later, possibly in Togo, Nigeria, Egypt, and Zimbabwe. There is enormous, unmet additional need for training programs in every specialty, but particularly in Obstetrics and Gynecology, Orthopedic Surgery, and Anesthesia.
RESULTS
To date, the results of training surgical residents in LMICs have been immensely encouraging. This year, all finishing residents in the PAACS programs passed the fellowship (5th year) examination in COSECSA. They are highly skilled in surgical techniques, although a different blend of skills from Western trained surgeons. These finishing residents have a large experience in general surgery, but also possess expertise in simple craniotomies, radical prostatectomies, intramedullary rod placements, C-sections and deliveries, among many others. They have a somewhat more limited exposure to Laparoscopic/minimally invasive techniques, and endovascular procedures.
Furthermore, as both twinning opportunities and ST programs have demonstrated, there is increase in capacity within local hospitals when these programs have been given a chance to mature and are effective.[11]
Future prospects
The majority of surgical care in LMICs is charity care, which by definition is not sustainable by itself; therefore, the concept that all of these hospitals should have the goal of self-sustainability is unrealistic. Additional resources are necessary to continue any significant surgical training and care in these institutions, in these countries. Currently, reimbursement from local governments is grossly inadequate. Organizational support is realized from nongovernmental organizations (NGOs), foreign governments, and FBOs, as well as large donor organizations, such as Gates Foundation, mostly through research and program grants funneled and implemented through university programs or through the WHO.
Unfortunately, surgical care has been eclipsed by the global attention of infectious disease, its treatment and expectant eradication. Additionally, disproportionally more effort is placed on acquiring surgical equipment and supplies than for surgical research. As greater attention is brought on surgical issues, particularly violence and injury, maternal and pediatric issues, and surgical requirements of infectious processes, greater efforts at requesting and obtaining research support can and will greatly facilitate the growth of surgical services. This should be done at all levels: Governments, NGOs, FBOs, and both large and small donors.
In addition, at each level of involvement, further emphasis must be placed on postgraduate training. Young physicians in LMICs have a keen thirst for knowledge and skills, and possess the requisite education for advanced training. Unless our current paradigm shifts from single interventions and ST engagements, continuing to ignore the component of long-term training, such interventions and associated limitations will be perpetuated indefinitely; “the unsung volunteer heroes cannot carry the burden of developing surgical capacity alone.”[8] However, as stronger institutional collaboration is established, more training programs are implemented throughout LMICs and exceptional candidates graduated and mentored into becoming trainers, the growth of surgical capacity can become exponential and surgical training become sustainable.
ADDENDUM
For readers interested in becoming involved in international work, but initially unsure where to turn, several possibilities exist. All are invited to join the WHO Global Initiative for Emergency and Essential Surgical Care (GIEESC) referenced below. This is a forum of surgeons, anesthesiologists, interested individuals and Ministries of Health that meets biannually; the next meeting is hosted by the Ministry of Health of Trinidad and Tobago, October 13-14, 2013. WHO also has many international partners listed on the website below that accept volunteers.
Venturing out of one's comfort zone to medical meetings on an unfamiliar continent is invigorating and allows one to meet and network with a large cadre of individuals. Similarly, working with one of several different groups will expose the volunteer to new situations without long-term commitment. A limited listing of some groups is included below, but others can be found through NGOs, church groups, university affiliations, etc. Any of the programs mentioned in this manuscript have associated individuals that will be very helpful in suggesting first-rate venues for service. Another excellent resource for those wishing to contribute to academic programs is the Fellowship for International Education in Neurological Surgery (FIENS), although this will generally require a one month commitment. Anyone unable to find an appropriate place to volunteer is welcome to contact me directly.
For practicing neurosurgeons, bringing your level of expertise to other countries and contributing in meaningful ways with local healthcare and surgical training is profoundly rewarding. It most frequently changes the volunteer in much more significant and enduring respects than the volunteer changes the hosting institution.
APPENDIX

Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2013/4/1/47/110030
REFERENCES
- 1.Abdullah F, Troedsson H, Cherian M. The World Health Organization program for emergency surgical, obstetric and anesthetic care. Arch Surg. 2011;146:620–3. doi: 10.1001/archsurg.2011.84. [DOI] [PubMed] [Google Scholar]
- 2.Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, Puren A. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: The ANRS 1265 Trial. PLoS Med. 2005;2:e298. doi: 10.1371/journal.pmed.0020298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bae JY, Groenb RS, Kushner AL. Surgery as a public health intervention: Common misconceptions vs the truth. Bull World Health Organ. 2011;89:395–401. doi: 10.2471/BLT.11.088229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bickler S, Ozgediz D, Gosselin R, Weiser T, Spiegel D, Hsia R, et al. Key concepts for estimating the burden of surgical conditions and the unmet need for surgical care. World J Surg. 2010;34:374–80. doi: 10.1007/s00268-009-0261-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bickler SW, Spiegel D. Improving surgical care in low- and middle-income countries: A pivotal role for the World Health Organization. World J Surg. 2010;34:386–90. doi: 10.1007/s00268-009-0273-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Debas HT, Gosselin R, McCord C, Thind A. Surgery. In: Jamison DT, Breman JG, Measham AR, editors. Disease control priorities in developing countries. Washington DC: International Bank for Reconstruction and Development/World Bank; 2006. pp. 1245–60. [PubMed] [Google Scholar]
- 7.Farmer PE, Kim JY. Surgery and global health: A view from beyond the OR. World J Surg. 2008;32:533–6. doi: 10.1007/s00268-008-9525-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Global surgery-the final frontier? Lancet. 2012;379:194. doi: 10.1016/S0140-6736(12)60083-X. [DOI] [PubMed] [Google Scholar]
- 9.Gosselin RA, Heitto M. Cost-effectiveness of a district trauma hospital in Battambang, Cambodia. World J Surg. 2008;32:2450–3. doi: 10.1007/s00268-008-9708-4. [DOI] [PubMed] [Google Scholar]
- 10.Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, Nalugoda F, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: A randomised trial. Lancet. 2007;369:657–66. doi: 10.1016/S0140-6736(07)60313-4. [DOI] [PubMed] [Google Scholar]
- 11.Haglund MM, Kiryabwire J, Parker S, Zomorodi A, MacLeod D, Schoeder R, et al. Surgical capacity building in Uganda through twinning, technology, and training camps. World J Surg. 2011;35:1175–82. doi: 10.1007/s00268-011-1080-0. [DOI] [PubMed] [Google Scholar]
- 12. [Last accessed on 2013 Mar 18]. Available from: http://ghsm.hms.harvard.edu/
- 13. [Last accessed on 2013 Mar 18]. Available from: http://globalhealth.unc.edu/
- 14. [Last accessed on 2013 Mar 18]. Available from: http://gpas.surgery.ucsf.edu .
- 15. [Last accessed on 2013 Mar 18]. Available from: http://surger y.duke.edu/about-department/divisions-and-programs/duke-global-surgery .
- 16. [Last accessed on 2013 Mar 18]. Available from: http://www.lluglobal.com/site/c.msKRL6PNLrF/b. 5550847/k.BEEA/Home.htm .
- 17. [Last accessed on 2013 Mar 18]. Available from: http://www.who.int/gho/child_health/mortality/causes/en/index.html .
- 18. [Last accessed on 2013 Mar 18]. Available from: http://www.who.int/gho/maternal_health/en/
- 19. [Last accessed on 2013 Mar 18]. Available from: http://www.who.int/healthinfo/statistics/mortality_child_cause/en/index.html .
- 20. [Last accessed on 2013 Mar 18]. Available from: http://www.who.int/surgery .
- 21. [Last accessed on 2013 Mar 18]. Available from: http://www.who.int/surgery/challenges/esc_pregnancy_more/en/index.html .
- 22. [Last accessed on 2013 Mar 18]. Available from: http://www.who.int/whr/2008/chapter3/en/index.html .
- 23.Kushner AL, Cherian MN, Noel L, Spiegel D, Groth S, Etienne C. Addressing the millennium development goals from a surgical perspective. Arch Surg. 2010;145:154–9. doi: 10.1001/archsurg.2009.263. [DOI] [PubMed] [Google Scholar]
- 24.Laxminarayan R, Ashford L. Using evidence about “best buys” to advance global health. In: Jamison DT, Breman JG, Measham AR, editors. Disease control priorities in developing countries. Disease Control Priorities Project. Washington DC: International Bank for Reconstruction and Development/World Bank; 2006. [PubMed] [Google Scholar]
- 25.Luboga S, Macfarlane SB, von Schreeb J, Kruk ME, Cherian MN, Bergstrom S, et al. Increasing access to surgical services in Sub-Saharan Africa: Priorities for national and international agencies recommended by the Bellagio essential surgery group. PLoS Med. 2009;6:1–5. doi: 10.1371/journal.pmed.1000200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Macfarlane SB, Agabian N, Novotny TE, Rutherford GW, Stewart CC, Debas HT. Think globally, act locally, and collaborate internationally: Global health sciences at the University of California, San Francisco. Acad Med. 2008;83:173–9. doi: 10.1097/ACM.0b013e31816096e3. [DOI] [PubMed] [Google Scholar]
- 27.Mock C, Cherian M. The global burden of musculoskeletal injuries. Clin Orthop Relat Res. 2008;466:2306–16. doi: 10.1007/s11999-008-0416-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ozgediz D, Dunbar P, Mock C, Cherian M, Rogers SO, Riviello R, et al. Bridging the gap between public health and surgery: Access to surgical care in low- and middle-income countries. Bull Amer Coll Surg. 2009;94:14–20. [PubMed] [Google Scholar]
- 29.Ozgediz D, Jamison D, Cherian M, McQueen K. The burden of surgical conditions and access to surgical care in low- and middle-income countries. Bull World Health Org. 2008;86:646–7. doi: 10.2471/BLT.07.050435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ozgediz D, Kijjambu S, Galukande M, Dubowitz G, Mabweijano J, Mijumbi C, et al. Africa's neglected surgical workforce crisis. Lancet. 2008;371:627–8. doi: 10.1016/S0140-6736(08)60279-2. [DOI] [PubMed] [Google Scholar]
- 31.Ozgediz D, Roayale K, Debas H, Schecter W, Farmer D. Surgery in developing countries: Essential training in residency. Arch Surg. 2005;140:795–800. doi: 10.1001/archsurg.140.8.795. [DOI] [PubMed] [Google Scholar]
- 32.Ozgediz D, Wang J, Jayaraman S, Ayzengart A, Jamshidi R, Lipnick M, et al. Surgical training and global health: Initial results of a 5-year partnership with a surgical training program in a low-income country. Arch Surg. 2008;143:860–5. doi: 10.1001/archsurg.143.9.860. [DOI] [PubMed] [Google Scholar]
- 33.Pollock JD, Love TP, Steffes BC, Thompson DC, Mellinger J, Haisch C. Is it possible to train surgeons for rural Africa. A report of a successful international program? World J Surg. 2011;35:493–9. doi: 10.1007/s00268-010-0936-z. [DOI] [PubMed] [Google Scholar]
- 34.Spiegel DA, Gosselin RA. Surgical services in low-income and middle-income countries. Lancet. 2007;370:1013–5. doi: 10.1016/S0140-6736(07)61457-3. [DOI] [PubMed] [Google Scholar]
- 35.Tollefson TT, Larrabee WF. Global surgical initiatives to reduce the surgical burden of disease. JAMA. 2012;307:667–8. doi: 10.1001/jama.2012.158. [DOI] [PubMed] [Google Scholar]
- 36.Weiser TG, Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, Berry WR, et al. An estimation of the global volume of surgery: A modeling strategy based on available data. Lancet. 2008;372:139–44. doi: 10.1016/S0140-6736(08)60878-8. [DOI] [PubMed] [Google Scholar]
- 37.The global burden of disease: 2004 Update. Geneva: 2008. World Health Organization. [Google Scholar]