

Abstract
This paper combines relational perspectives on gender identity with social network structural perspectives on health to understand men’s sexual functioning. We argue that network positions that afford independence and control over social resources are consistent with traditional masculine roles and may therefore affect men’s sexual performance. For example, when a heterosexual man’s female partner has more frequent contact with his confidants than he does–a situation that we refer to as partner betweenness – his relational autonomy, privacy, and control are constrained. Analyses of data from the National Social Life, Health, and Aging Project (NSHAP) show that about a quarter of men experience partner betweenness, and that these men are 92 percent more likely to report problems getting and/or maintaining an erection (95% CI: 1.274, 2.881). This association is strongest among the youngest men in the sample, which may reflect changing conceptions of masculinity in later life. We close by considering several explanations for these findings, and urge additional research on the linkages between health, gender, and network structure.
INTRODUCTION
Feminist conceptualizations of masculinity emphasize men’s power, authority, and control, and more generally any circumstance or practice that perpetuates their dominance over women (Cheng 1999; Connell 1987, 1995; Connell and Messerschmidt 2005). Much of this gendered behavior is relational in nature, as is widely recognized in gender research which focuses on the role of social interaction in the maintenance of cultural beliefs and experiences that support male privilege (Ridgeway 1997; Ridgeway and Smith-Lovin 1999; West and Zimmerman 1987). Many sociologists who do not work on the problem of gender also recognize the importance of advantages that are rooted in social network structure for things such as autonomy and influence (e.g., Burt 1992; Emerson 1962; Freeman 1979). One of our goals is to bring these perspectives closer together by theorizing the sexual consequences of social network positions that shape men’s access to structural advantages in their everyday lives.
This is a paper about being a man in our society, and the ways in which men’s social networks can shape their private sexual experiences. Our starting point is the idea that because social network position has implications for men’s capacities to exercise independence, influence, and other masculine traits, it may have consequences for heterosexual men’s psychological well-being and/or for the quality of their intimate relationships with female partners. Our strategy for illustrating the importance to men of having independent access to network resources is not merely theoretical or logical. Rather, we aim to demonstrate empirically some of the negative consequences heterosexual men experience when their access to positions of advantage in social networks is compromised. Some research notes a connection between men’s material and positional advantage and their sexual attractiveness to women (e.g., Martin 2005). Expanding on this, we focus on men’s sexual performance – specifically, heterosexual men’s abilities to get and maintain an erection during sexual encounters with women. If we can show that men have greater difficulty performing sexually when some of their most meaningful social connections are accessed more frequently by their female partners–a circumstance that we refer to as “partner betweenness”–it will help to demonstrate some of the implications of access to network resources for men.
A key theoretical foundation of this study is the large body of work in medical sociology on the link between social relationships and health. Most of this research emphasizes the benefits of being socially connected in terms of access to high-quality network ties that provide instrumental and socio-emotional support, social capital and informal social control, as well as sense of belonging and self-esteem (e.g., see Berkman et al. 2000; House, Landis, and Umberson 1988; Thoits 1995; Umberson 1987). As some scholars have noted, however, one must consider the content and structure of social connections before one can understand how they affect health (for a review, see Smith and Christakis 2008). This work has yielded valuable insights regarding the extent to which individuals’ social network ties involve negative affect (Rook 1984; Krause 2005), if they include individuals who also have health problems or engage in certain behaviors (Christakis and Fowler 2007), to what extent network members impose excessive demands (Silverstein, Chen, and Heller 1996), how well-connected network members are to each other (Cattell 2001), and how one is positioned within network structures (Laumann and Youm 1999).
Our study expands on this line of research by suggesting a relational circumstance that can negatively affect men’s sexual health – specifically, partner betweenness. We examine this idea using recent data on sexual health and egocentric social network ties from the National Social Life, Health, and Aging Project (NSHAP), a nationally representative study of older Americans that was conducted in 2005–2006. We discuss several psychological and relational mechanisms through which this network structural circumstance could give rise to erectile dysfunction. We also consider several factors which may alter the relationship between partner betweenness and erectile dysfunction among older men, including the possibility that aging prompts a shift away from traditional ideals of hegemonic masculinity in favor of a softer model of manhood that involves conveying experience, wisdom, and nurturance (Mann 2007; Ribeiro, Paúl, and Nogueira 2007). We close by discussing some important empirical limitations and the need for more research on the link between social networks and sexual health in both men and women.
SOCIAL NETWORKS, GENDER, AND SEXUAL FUNCTION IN OLDER MEN
Many scholars have theorized gender in general relational terms (see Ridgeway and Smith-Lovin 1999; Smith-Lovin and McPherson 1993). Empirical network research focuses on how the structure of interaction between men and women – for example, gender homophily in networks – perpetuates gender status differences (e.g., see McPherson, Smith-Lovin, and Cook 2001; Popielarz 1999; Rotolo and Wilson 2007; Smith-Lovin & McPherson 1993). Social network composition, which affects access to resources, is one important factor in this respect. Women’s networks are generally thought to be more kin-centered, while men’s networks are thought to be more comprised of coworkers and weak ties (Marsden 1987; Moore 1990; Pugliesi and Shook, 1998; but see Cornwell Laumann, and Schumm 2008)– the kinds of ties that are more relevant to occupational attainment and mobility. Some scholars point to evidence of such differences in network composition to help explain gender differences in advancement in the workplace, labor market outcomes, and entrepreneurial success (Burt 1998; Fernandez and Sosa 2005; Ibarra 1993; McGuire, 2000; Renzulli, Aldrich, and Moody 2000; van Emmerik 2006). From this perspective, networks are important because they indirectly reinforce traditional gender roles by perpetuating gender status differences.
We are interested in the possibility that men’s positions within social networks yield more subtle relational advantages that are associated with traditionally masculine traits. Scholarly treatments of masculinity emphasize self-reliance, control, and independence (e.g., see Connell 1995; Riska 2002). Little gender research has explored the possibility that networks play a role in supporting these aspects of men’s gender identity, despite the fact that research suggests a direct connection between social network position and autonomy and influence. Network betweenness and bridging are particularly important in this regard (Burt 1992; Freeman 1979). Bridging occurs when a person maintains connections with at least two other actors who otherwise would be poorly connected. Social resource frameworks (Lin 2001; Wellman and Wortley 1990) suggest that maintaining connections to actors in separate domains is advantageous because it yields access to heterogeneous social resources that are suited to different purposes. This, in turn, gives those who occupy bridging positions more resources and more independence from exchange partners (e.g., see Burt 1992; Emerson 1962).It also enhances one’s ability to manipulate relationships and resource flow and to influence others’ access to resources.
The Role of the Female Partner
It is impossible to understand the relationship between social network connectedness and gender, however, without considering the position of the most important member of a heterosexual man’s social network; his female partner. She introduces a key source of tension in the relational genesis of masculinity. On one hand, her presence and visibility within the network is essential to his identity as a heterosexual man. On the other hand, she is one of the most highly embedded members of his network – increasingly so as the relationship progresses (Kalmijn 2003; Milardo 1982) – and therefore often has access to his social contacts.
Figure 1 shows the five most likely contact patterns between a given man (“ego”), his partner (“partner”) and one of his comrades (“confidant”). It does not matter how “frequent” contact is defined. What is important is how frequently the partner interacts with the confidant relative to the frequency with which ego interacts with the confidant. Ego is likely to have very frequent contact with the partner, especially if it is his spouse. If so, then it is a strong tie, and we can also assume that his partner must have at least a weak tie (infrequent contact) with that confidant (Granovetter 1973). This gives us the five triad forms shown in Figure 1. Triad A represents a situation in which ego is only weakly connected to the confidant, while his partner is not connected to the confidant. This is probably a rare configuration, since confidant relationships are usually strong. Both this case and Triad B depict situations in which ego has greater access to the confidant than his partner has. Triads C and D represent situations in which ego and his partner share equal access to the confidant.
Figure 1. Five Possible Ego-Partner-Confidant Triads, Based on Contact Frequency.
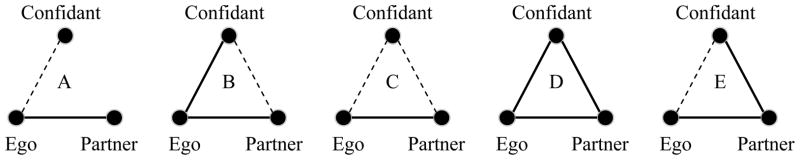
Note: Solid lines represent frequent contact. Dashed lines represent (relatively) infrequent contact.
Triad E is a special case that depicts the circumstance where ego has less contact with his confidant than his partner does. The partner has more access to both parties than they have to each other. Drawing on social network approaches to bridging and betweenness, we refer to this circumstance as partner betweenness. In network terms, ego’s partner can (inadvertently) constrain his bridging potential in the joint network (see Burt 1992 for a discussion of this idea as it relates to conjugal relationships), and is in a position to act as a mediator or broker in the ego-confidant relationship. Situations of betweenness could reflect a number of different circumstances, ranging from an ill ego who has a very helpful partner who facilitates communication between ego and his confidants, to a domineering female partner who insists on acting as a gatekeeper for the household, to an ego who is poorly connected in the first place and whose main source of social contact is through his spouse’s own confidants.
Regardless of its cause, given what we know from relational perspectives on gender, it is plausible that partner betweenness has important implications for men. It signals lack of access to unique resources through contacts. Beyond this, it implies lack of autonomy, greater dependence on the partner for social contact, and reduced control over the flow of resources between the confidant and partner. Lack of privacy is also a concern, as the confidant may not be seen by ego as the best person to go to with a confidential concern– especially if it is about his partner. In sum, partner betweenness indexes a number of circumstances that may impede the realization of key components of traditional masculinity.
Consequences for Intimacy and Sex
Research suggests that intimate relationships last longer and are more satisfying when partners’ social networks overlap. Embeddedness within a joint network enhances partners’ sense of “couplehood,” decreases role strain, and increases the social costs of dissolving the relationship (Julien, Chartrand & Bégin 1999; Kalmijn & Bernasco 2001; Stein et al. 1992; Youm and Laumann 2003). But this may not be the case when network overlap is complete or when it engenders partner betweenness. Reduced autonomy and the loss of exclusive social contacts could negatively affect individuals whose network relations are accessed more frequently by their partners.
This is especially true of men, given the centrality of qualities like autonomy and control in masculine gender identity. One study of young couples found that men who perceive that they and their partners are too dependent on their relationship have lower self-esteem, while perceived dependence does not bother women in the same way (Galliher et al. 1999). Research has shown not only that access to diverse, separate network contacts (in informal networks) is associated with psychological well-being (e.g., see Fiori, Antonucci, and Cortina 2006), but also that men are especially negatively affected by the loss of such resources due to life-course events like divorce (Gerstel, Riessman, and Rosenfield 1985). To the extent that partner betweenness indexes lack of involvement with other social contacts, this could lower men’s self-esteem, sense of control and autonomy, and more directly their sense of masculinity (e.g., see Avison and Cairney 2003). This could also have negative consequences for the quality of men’s relationships with their female partners by engendering feelings of resentment toward and lack of satisfaction with the female partner, strained relations, and reduced mutual attraction (see Foreman and Dallos 1992).
The implications of partner betweenness for psychological and relational outcomes such as self-esteem and relationship quality are important for understanding gender identity, as these factors are known to negatively impact one of the most direct physical expressions of masculinity; sexual function (Hale and Strassberg 1990; Laumann, Paik, and Rosen 1999; Laumann et al. 2006; Rosen 2001; Sand et al. 2008). For men, reduced autonomy, sense of control, self-efficacy, and related psychological constructs have direct associations with sexual function, as masculine identity is inextricably tied to the penis (Martino and Pallotta-Chiarolli 2003; Zilbergeld 1992). In the context of sexual relationships, masculinity is expressed through “erection, penetration and climax,” so it is possible that threats to gender identity– relational and –otherwise sometimes manifest as sexual problems, including erectile dysfunction (Oliffe 2005:2250; see also Lee and Owens 2002). This may be one of the most subtle downstream implications of network connectedness for heterosexual men, and yet one of the most consequential for gender identity. Indeed, erectile dysfunction (“ED”) has been theorized as a loss of manhood and masculinity that is closely linked to feelings of inadequacy and weakness (Edgar 1997; Kimmel 1987; Lee and Owens 2002; Leiblum and Rosen 1991; Oliffe 2005; Sand et al. 2008; Zilbergeld 1992).
Pathways to Erectile Dysfunction
The etiology of ED can involve organic (e.g., vascular, neurologic, hormonal), psychological, and relational factors –usually in some combination (e.g., see DeLamater and Sill 2005; Laumann et al. 2007; Dean and Lue 2005). Organic causes of ED include low testosterone, reduced blood flow to the penis, and nerve damage – problems which can result from a number of serious conditions such as diabetes, kidney disease, cardiovascular disease, and neurological disease. It is possible that life-course-based changes in older men’s networks could relate to ED through organic mechanisms. For example, partner betweenness may reduce testosterone levels.1 There is evidence that testosterone levels respond to social factors such as conflict and competition (Wagner, Flinn, and England 2002), but there is only mixed support for the hypothesis that low levels of testosterone result in ED (e.g., see Kupelian et al. 2006). Furthermore, there is no known connection between social networks and testosterone.
Other causes of ED are probably more relevant in light of network-relational arguments. Some researchers claim that psychological factors are central to ED because they relate directly to the processing of stimulatory and inhibitory messages in the brain, the relaxation of penile muscles, and other processes which occur between the introduction of stimuli and the onset of erection (see Dean and Lue 2006 for a detailed discussed of the brain’s role in ED). ED that results from interference in this process is usually referred to as “psychogenic” ED. It was originally hypothesized that 90% of cases of ED were psychogenic (Masters and Johnson 1966), though medical researchers now recognize the larger role of organic causes. The most frequently examined factors that are known to give rise to psychogenic ED include stress, anxiety, low self-esteem, and depression. Given its psychological implications for men who subscribe to traditional models of gender identity, it is possible that partner betweenness produces ED through this psychogenic pathway.
Other factors that may give rise to psychogenic ED are even more relational in nature. Some studies point to relationship qualities that diminish arousal response, including incompatible sexual scripts between partners, partner discord, and low physical and emotional partner satisfaction (Corona et al. 2006; Laumann, Paik, and Rosen 1999; McCabe and Cobain 1998; for a review, see McCabe 2008). To the extent that women’s positions in men’s personal social networks are perceived by men as threats to their autonomy and control over social resources, this could introduce strain into the relationship, increase men’s resentment of their partners, decrease partner satisfaction, and/or decrease men’s sense of privacy– all of which may reduce their interest in sex and their responsiveness to partner-initiated sexual stimuli.
Before moving forward, we would like to stress that the main goal of this paper is to establish whether there is an association between female partners’ positions within men’s social networks and men’s experiences with ED, not to isolate the mechanisms through which such an association arises. As is the case with research on the link between social support, networks, and various health outcomes (see Smith and Christakis 2008), most research on relational causes of ED focuses on the intimate partner dyad. Supradyadic influences on ED that stem from a broader network have remained largely unexplored.
Gender and ED in Later Life
We draw on the relational gender perspective by focusing on the implications of connections that exist between partners and their joint network members. We focus our examination on older men for two reasons. For one, this is the group among whom erectile dysfunction is most prevalent. It is estimated that more than one-third of older men in the United States suffer from ED (Laumann, Das, and Waite 2008; Laumann, Paik, and Rosen 1999; Lindau et al. 2007).
Second, partner betweenness is likely to be especially common among older adults. Social networks evolve in such a way that intimate partners’ contacts converge over the life course. Couples that have been together longer have more overlapping social circles (Johnson and Leslie 1982; Kalmijn 2003; Milardo 1982). Partners increasingly share in each other’s social resources as they become more embedded in each other’s lives. Some of these changes are due to later-life experiences. Retirement reduces contact with people who are loosely connected to family (e.g., coworkers). Severe health problems have a similar effect, especially when caregiving is involved. In these cases, close network members may increase contact with each other and with the partner to facilitate information sharing, monitoring, and coordination of support. This is less often the case with weak ties that are independent of the partner, especially when caregiving involves difficult or potentially embarrassing tasks such as helping a person go to the toilet (Stoller and Pugliesi 1991). The partner is usually the primary caregiver, though some research suggests that women are more likely to take on primary caregiving responsibilities than men (for a meta-analysis of this issue, see Pinquart and Sörensen 1996). As one’s health declines, then, one’s partner becomes increasingly involved in one’s other social relationships. These processes combine to create denser core confidant networks, and therefore less network bridging potential for those experiencing health problems (Cornwell 2009a, b). Thus, through a number of processes, men tend to lose partner-independent social ties as they grow older.
There is evidence that men are particularly sensitive to threats to independence and mastery that accompany aging (Krause 2007; Mansfield, Addis, and Mahalik 2003; Mirowsky 1995; Silverstein, Chen, and Heller 1996; Smith et al. 2007; Stephenson et al. 1999). At the same time, our arguments concerning the link between social network structure and ED make assumptions about the importance of traditional models of masculinity to men that may not be universally applicable. Recent work suggests that the same later-life experiences that challenge masculinity by reducing autonomy also change men’s relational priorities in fundamental ways. The realities and challenges of later life –including retirement and health decline, but also grandfatherhood and, in some cases, the need to take care of an ailing spouse –are in tension with hegemonic qualities like autonomy and control (Connell 2005; Mann 2007; Moss and Moss 2007; Ribeiro, Paúl, and Nogueira 2007). These priorities become both less appropriate to older men’s social circumstances and more difficult to sustain. Furthermore, experiences like grandparenthood elicit more nurturance from men, which manifests most of all through closer relationships with family (Mann 2007; Ribeiro, Paúl, and Nogueira 2007).
Thus, recent work at the intersection of social-gerontology and gender studies suggests that older men –those in retirement, for example –may develop new priorities which are based not on instrumental control and independence, but on “softer” forms of influence that derive from teaching and mentoring. Older men place more emphasis on transferring values and giving advice about things like interpersonal relationships (Mann 2007; Waldrop et al. 1999). Kin relations become particularly important to older men according to this perspective because they provide the greatest opportunity to exercise this form of influence (Davidson, Daly, and Arber 2003). This observation dovetails with social-psychological research which shows that older adults adopt a more emotional approach to their social relationships, as they focus less on instrumental ties that aid individual accomplishment and more on ties that provide socio-emotional fulfillment (for a review, see Adams and Ueno 2006).
One consequence of these relational shifts is that close ties, kin, and partners play a larger role in men’s social lives than ever before. An interesting question, then, is whether any negative consequences partner betweenness has for men’s sense of autonomy and control are as prevalent among the oldest men, many of whom have completed transitions into retirement and grandparenthood. It is possible that as they grow older, partner betweenness is less bothersome to these men and thus has fewer direct consequences for psychological well-being, for the quality of their intimate relationships, and ultimately for their sexual function. We consider this possibility in the course of our investigation into the relationship between partner betweenness and ED.
DATA AND MEASURES
We use data from the National Social Life, Health, and Aging Project (NSHAP), a nationally representative, population-based study funded by the National Institutes on Health and conducted by the National Opinion Research Center (NORC). The study consists of interviews with 3,005 non-institutionalized older adults (ages 57–85), conducted between autumn 2005 and spring 2006. The sample was selected from a multi-stage area probability design screened by the Institute for Social Research (ISR). NSHAP identified 4,400 potential respondents in the desired age range. The design oversampled by race/ethnicity. NSHAP retained this design and also oversampled by age and gender to produce approximately equal cell sizes by gender across three age categories. The final response rate for the entire sample is 75.5%.2 NSHAP interviewed 1,455 men, but not all of these men are relevant to the study. Details about inclusion criteria for the analysis and efforts to address selection that arises as a result are provided below.
Erectile Dysfunction
NSHAP included a module that asked respondents about problems they may have had with sexual function during the past year.3 The 906 men who NORC could verify, based on their responses to previous questions, had had sex within the past year were asked about their experiences with sexual dysfunction during that time with specific partners. The sexual dysfunction module was prefaced with the following statement:
Sometimes people go through periods in which they are not interested in sex or are having trouble with sexual gratification. We have just a few questions about whether during the last 12 months there has ever been a period of several months or more when you…
As part of this module, male respondents indicated if, during this time, they had trouble getting or maintaining an erection. Men were also asked if they were unable to climax (experience an orgasm), a form of dysfunction that is sometimes referred to as anorgasmia. Cooperation on these items was high, with only 3 percent of men refusing to answer either question.4 We focus our main analysis on difficulty achieving/maintaining an erection, but include an analysis of anorgasmia and compound dysfunction (having experienced both erectile dysfunction and anorgasmia) in appendix tables. These measures, as well as the key predictors of these measures, are described in Table 1.
Table 1.
Descriptions of Some Key Variables Used in the Analyses (N = 678)a
| Variable | Weighted Mean | Standard Deviation | |
|---|---|---|---|
| Dependent variables | |||
| Erectile dysfunction | R had trouble getting/maintaining an erection {1= Yes, 0 =No} | .362 | .483 |
| Anorgasmiab | R had trouble achieving orgasm {1= Yes, 0 =No} | .207 | .407 |
| Compound dysfunctionb | R experienced both of the above sexual problems {1= Yes, 0 =No} | .163 | .363 |
| Independent variables | |||
| Partner betweenness | R's spouse/partner has more contact with at least one of R's core confidants than R himself {1= Yes, 0 =No} | .252 | .449 |
| Number of confidants | Number of non-partner confidants in the network. Range 1 to 5. | 2.738 | 1.214 |
| Proportion kin | Proportion of confidants who are kin. Range 0 - 1. | .570 | .387 |
| Proportion female | Proportion of confidants who are female. Range 0 - 1. | .344 | .325 |
| Age group | (Ref) R is between 57 and 64 years of age {1 =Yes, 0 =No} | .546 | .500 |
| R is between 65 and 74 years of age {1 =Yes, 0 =No} | .322 | .484 | |
| R is between 75 and 85 years of age {1 =Yes, 0 =No} | .131 | .349 | |
| Retired | R is retired {1= Yes, 0 =No} | .539 | .495 |
| Married | R and partner are married {1 =Yes, 0 =No} | .869 | .338 |
| Frequency of sex | (Ref) R and partner have sex monthly or less often {1 =Yes, 0 =No} | .351 | .468 |
| R and partner have sex 2–3 times a month {1 =Yes, 0 =No} | .310 | .463 | |
| R and partner have sex 1–2 times a week {1 =Yes, 0 =No} | .264 | .452 | |
| R and partner have sex >2 times a week {1 =Yes, 0 =No} | .076 | .273 | |
| Spend time together | R and partner usually spend free time together {1 =Yes, 0 =No} | .537 | .499 |
| Average of 3 standardized items assessing relationship happiness, | |||
| Partner satisfaction | emotional satisfaction, and pleasure (α =.78). Range: −2.31 to 1.04. | .220 | .753 |
| Partner demanding | Partner often makes too many demands on R {1 =Yes, 0 =No} | .093 | .305 |
| Prostate trouble | R reports having an enlarged prostate {1 =Yes, 0 =No} | .267 | .442 |
| Diabetes | R has diabetes {1 =Yes, 0 =No} | .195 | .407 |
| Self-rated health | R reports being in “poor” or “fair” health {1 =Yes, 0 =No} | .180 | .369 |
| R reports being in “good” health {1 =Yes, 0 =No} | .260 | .443 | |
| R reports being in “very good” health {1 =Yes, 0 =No} | .395 | .492 | |
| (Ref) R reports being in “excellent” health {1 =Yes, 0 =No} | .165 | .370 | |
| Partner's health | R reports partner is in “poor” or “fair” health {1 =Yes, 0 =No} | .198 | .399 |
| R reports partner is in “good” health {1 =Yes, 0 =No} | .297 | .454 | |
| R reports partner is in “very good” health {1 =Yes, 0 =No} | .334 | .477 | |
| (Ref) R reports partner is in “excellent” health {1 =Yes, 0 =No} | .171 | .370 | |
| Depression | Average of standardized responses to 10 ordinal items from the | ||
| CES-D scale assessing depressive symptoms. Range: −.602 to 2.462. | −.146 | .472 | |
| Self-esteemc | (Ref) R does not say it is true that s/he has high SE {1 =Yes, 0 =No} | .162 | .378 |
| R says “somewhat true” that s/he has high SE {1 =Yes, 0 =No} | .308 | .464 | |
| R says “very true” that s/he has high SE {1 =Yes, 0 =No} | .530 | .500 | |
| Anxietyc | Average of standardized responses to 7 ordinal items from the HAD scale assessing anxiety. Range: −.625 to 3.140. |
−.008 | .556 |
Means are estimated using NSHAP person-level weights, with post-stratification adjustments for non-response and adjustments for probability of inclusion in the main analysis.
Includes cases with data on this variable and the independent variables used to predict it (N = 670 and 667, respectively).
Includes cases with data on this and other variables used in multivariate analyses of ED (N = 633 and 637, respectively).
Partner Betweenness
We are interested in understanding to what extent older men’s erectile dysfunction is associated with their female partners’ involvement in men’s confidant relationships. NSHAP collected information about all respondents’ egocentric social networks. Following the General Social Survey, interviewers asked respondents to list people with whom they discuss “things that were important to you.” Respondents could name up to five discussion partners. Following this, those who did not include a spouse or romantic/sexual partner among their core confidants were asked if they had a spouse/partner.5
The “important things” question is thought to elicit names of strong, frequently accessed, long-term contacts (Marin 2004; Ruan 1998) –ties through which normative pressures and social influence are likely to operate and which are thought to be particularly important to older adults (Cornwell et al. 2008). Bearman and Parigi (2004) raise some concerns about the extent to which this is true, especially with respect to content being discussed. Our data show, however, that frequency of contact with named alters is fairly high, with 83.6 percent being contacted at least once a week, 80.3 percent being described as at least “very close,” and 98.1 percent being described as at least “somewhat close.” Also, respondents noted that they would be at least somewhat likely to discuss a health problem that they were concerned about, or an important decision about medical treatment with 89.1 percent of the alters named. All things considered, the “forbidden triad” assumption (Granovetter 1973) is largely defensible in this case.
Following the enumeration of network members, respondents were asked about the frequency with which they interact with each of their network members, as well as how frequently each of their network members interacts with each of their other network members. Each respondent (“ego”) reported frequency on a nine-level scale, ranging from “have never spoken to each other” to “every day.” We use responses to these questions to assess how connected ego’s spouse/partner is to each of their confidants. We are interested in instances in which the ego’s partner has greater contact with ego’s confidants than ego has– specifically, whether a triad of form E, discussed above, appears anywhere in ego’s network.6 This indicates a situation in which the female partner has greater contact with a joint confidant. In the remainder of this paper, we will refer to this as “partner betweenness.”7
Relationship Quality
We include several measures of the quality of men’s relationships with their partners. First, we include an indicator of whether the partnership is a marital or non-marital partnership. Second, we include a series of dummy variables which reflect respondents’ approximation of how frequently they have sex with their partner (four categories, ranging from “once a month or less” to “3 or more times a week”). Third, we construct a scale that taps satisfaction with the partner, based on three items: 1) an ordinal rating of how emotionally satisfying the relationship is (“not at all”/”moderately,” “very,” or “extremely”); 2) a numerical rating of how “happy” the relationship is (range from 1 to 4); and 3) a rating of how physically pleasurable it is (“not at all”/”moderately,” “very,” or “extremely”). These measures combine into a scale with satisfactory reliability (α = .78). Fourth, we include an indicator of whether men spend most of their free time “together” with their partner (as opposed to spending some or most of it apart). Finally, we include a dichotomous variable which indicates whether men report feeling that their partner often (as opposed to sometimes or never) makes “too many demands” on them. Including this measure helps distinguish partner network betweenness from partner dominance. These measures capture several things, but the overarching assumption is that stronger relationships are negatively associated with erectile dysfunction.8
Health
It is important to consider health both because some health problems account for organic causes of ED and because health problems create the need for caregiving. That is, health problems may be associated with ED directly or indirectly, through their effect on the frequency of partner contact with confidants. Partner betweenness in this case would merely index a broader loss of independence on the part of the individual. This makes it necessary to control numerous dimensions of health in our analysis.
Prostate problems are a common cause of lower urinary tract symptoms (LUTS), such as urinary incontinence, in older men –symptoms which are closely associated with sexual dysfunction (Ponholzer et al. 2004). Thus, we include indicators of whether men reported any history of having an enlarged prostate gland. Diabetes and vascular diseases also can lead to sexual dysfunction (Laumann et al. 2007; McVary 2007). Therefore, we consider indicators of whether respondents report ever having had: 1) diabetes; or 2) heart attack, heart failure, stroke, hypertension, or clogged arteries. Obesity is also a risk factor for erectile dysfunction (Esposito et al. 2008). NSHAP measured respondents’ body mass index, but this variable is missing for 7 percent of the sample due to equipment and technical problems. So, we use the interviewer’s subjective assessment of the respondent’s body shape (ranging from “thin” to “obese”) as a proxy. (Results are not affected by this substitution.) We also include an indicator of whether the respondent has cancer, which could indirectly lead to ED and create the need for caregiving and support. We measure functional health as well (based on respondents’ self reports of how well they can perform activities of daily living, or ADLs), because it captures health problems that are most likely to require social support and caregiving, which directly reduce independence.
We also include an ordinal measure of overall self-reported health (originally five levels ranging from “poor” to “excellent,” but “poor” and “fair” are combined due to small Ns) because it may capture other unobserved health problems. Female partners’ health problems could also affect men’s sexual function, so we include an ordinal measure capturing men’s perceptions of their partners’ health (four levels, ranging from “poor” or “fair” to “excellent”).
Several health-related behaviors are associated with sexual dysfunction, including smoking, drinking alcohol, and lack of exercise (see McVary 2007). We tested three controls for health-related behavior: A dichotomous indicator of whether the respondent smokes; a variable measuring the number of drinks respondents report having in a given day; and a five-category ordinal measure of how frequently the respondent participates in physical activity. These variables were non-significant in all of the models and are not included in the final analyses.
Cognitive health may also play a role. Cornwell (2009a) reports that cognitive impairment is a significant predictor of older adults’ likelihood of having confidants who are not connected to each other, which would reduce the likelihood of partner betweenness. We measure cognitive function using the Short Portable Mental Status Questionnaire (SPMSQ), which consists of questions such as “What day of the week is it?” and “What is your phone number?” The SPMSQ is scored as a count of the number of such items the respondent answered correctly, with a maximum of 10 (Pfeiffer 1975).9
Psychological Factors
Like relationship quality, psychological factors may contribute to psychogenic ED. Depression and other psychological problems like anxiety and low self-esteem are closely related to sexual dysfunction (Goldstein 2000; Laumann et al. 1999; Van Minnen and Kampman 2000). Depression is measured using a modified CES-D scale (CES-D-ml), which is the average of standardized responses to 10 ordinal items assessing R’s depressive symptomology, such as not feeling like eating or feeling sad “most of the time” as opposed to less frequently (α = .780).The CES-D-ml scale does not include a measure typically included in the CES-D which asks respondents how often they feel lonely. Leaving this item in the original scale would give it a social dimension that is partially captured in other measures of connectedness, such as number of non-partner confidants (see Cornwell and Waite 2009).
Anxiety is assessed using a seven-item subscale of the Hospital Anxiety and Depression (HAD) scale (Zigmond and Snaith 1983). Respondents are asked how often, during the past week, they “felt tense or ‘wound up,’” felt restless, could sit still and relax, and four other questions designed to tab generalized anxiety. These items are reverse-coded as necessary, standardized, and then averaged together to form a reliable scale (α = .761). A final psychological measure assesses self-esteem. NSHAP asked respondents how true the statement “I have high self-esteem” is for them. We use a collapsed three-category measure that indicates whether respondents answered “very true,” “somewhat true,” or one of the following three responses: “neither true nor untrue,” “somewhat untrue” or “not very true.” Both the items measuring self-esteem and anxiety were administered to a random subset of respondents on a leave-behind questionnaire, so it has more missing values than the other key predictors. They are therefore analyzed in supplementary analyses presented in the appendix. Unfortunately, NSHAP does not include other measures which would directly capture aspects of masculine identity (e.g., sense of control, sense of autonomy, mastery) which may relate the structure of men’s networks to their sexual health. We revisit this issue later.
Medications
Use of specific medications has been linked to ED, including diuretics, antihypertensives, cardiac and cholesterol drugs, antidepressants, hormones, and several other medications and recreational drugs (see McVary 2007). Comprehensive medication data were collected by interviewers with the aid of a computer-based log, and drug names were subsequently coded using a drug database that matches to the hierarchical classifications of the American Hospital Formulary Service. Approximately 97% of all medications were successfully coded (for details, see Qato et al. 2009). We include a dichotomous indicator of whether respondents were using any one of the following types of medications that have been linked to ED: medications for diseases like cardiovascular disease and diabetes, which are closely associated with ED, sex hormones, sedatives/narcotics, psychological/neurological drugs, and sex-enhancing medications.
Life Course
Partner betweenness may be associated with ED not only because of its implications for masculine identity, but also because it is correlated with later-life experiences (e.g., retirement) that also affect depression, low self esteem, and anxiety, which are known to affect sexual function (Laumann et al. 2008). We first included a measure of age in years, and it had a significant association with ED. But for the sake of consistency with other work on ED and analyses of social and health conditions among older adults, and to keep age-specific estimates of ED reliable, we operationalize age in three categories (57–64, 65–74, 75–85). We also include a measure of education in terms of whether the respondent attended college. Alternative operationalizations of education based on the available data on degree attainment yielded no improvements in the models. Finally, employment status is measured using indicators of whether the respondent is retired and whether he is out of the labor force for some other reason.
Covariates
In addition to partner betweenness, health, relationship quality, and life course measures, we take into account several factors which are associated with ED. Previous work (Laumann et al. 2007) shows that ED varies by race/ethnicity, but it suggests that this is largely due to health differences between groups. We included race/ethnicity in initial models, but removed it after it became clear that it neither relates to ED directly nor influences covariates. Remaining covariates relate to network structure. We consider network composition in terms of proportion kin, as kin relations are often joint contacts for partners. Both masculinity and partner betweenness could be related to the gender composition of men’s networks, so we include a measure of proportion confidants who are female. Finally, because there is simply greater potential for partner betweenness when men have large networks, we include a control for the number of confidants in the network. Supplementary analyses (not shown, but available upon request) show that the main results hold both in small networks (≤2 non-partner confidants) and large networks (≥3 non-partner confidants).
Analysis
Our goal is to assess the association between older men’s female sexual partners’ connectedness to men’s confidants and those men’s experiences with ED. Our analysis is concerned only with those men who reported whether they experienced problems with ED during sexual relations with their partner and who reported having at least one core confidant. A variety of factors exclude men from the analysis, including not having a spouse/partner, not having had sex within the past year, having sex with a partner who was not named in the network roster, and not having any confidants. Frequency of contact between spouses and confidants could not be ascertained for three other respondents. Data on other variables in the analysis were missing for some men as well. All things considered, the total number of men with valid data on all variables is 678.
Our theory is that older men’s sexual function is adversely affected by partner betweenness. However, we do not have sufficient data to establish causality. Therefore, we merely set out to determine whether the existing data are consistent with our argument and suggest its plausibility. We conduct a series of logistic regression analyses predicting whether ED is reported by the men in the study. We begin with a model which predicts ED using the partner betweenness variable. Life course measures – including age, education, and employment status – are also included, along with the measures of network structure controls. The second and third models are used to assess whether any association between partner betweenness and ED that is observed in the first model persists when controlling for relationship quality (marital status, frequency of sex, partner satisfaction, whether their partner is demanding, and whether they spend their free time with their partner) and health (obesity, prostate trouble, diabetes, cardiovascular disease, cancer, overall self-rated health, depression, and cognitive function, use of potentially problematic medications, and perceived health of the partner), respectively. The fourth model includes all variables simultaneously. All tests are two-sided. We expect the coefficient representing partner betwenness to be significantly positively related to ED, net of all other measures in all models. Model fit is assessed using the squared correlation between the predicted probability and the observed outcome (Fleiss, Williams, and Dubro 1986).
As our analysis pertains only to men who had partners and other confidants, selection problems are a valid concern. To adjust for selection issues arising from our focus on this subsample, we employ a complete-case weighting form of missing data adjustment (see Morgan and Todd 2008). We begin by calculating each man’s probability of inclusion in the main model. Predictor variables in a first-stage model included the main life-course measures, marital status, respondent’s health/medication use, network size, whether respondents reported having any male, female, kin, and non-kin confidants, respectively (using the network composition measures would have kicked out those with small networks), household size, and whether the respondent reported having had sex in the past year (N = 1,418). We then take the inverse of the predicted probability that is derived from this first-stage analysis, multiply it by the NSHAP-supplied survey weight, and use the product as person-weight in all models.10 This procedure gives disproportionate weight to those cases who were least likely to be observed in the final models, thus helping to reduce any potential selection effects caused by exclusion of those men who, for instance, did not have sex within the past year.
RESULTS
Erectile dysfunction is common among older men, as 36.2 percent of these respondents reported having had some trouble getting and/or maintaining an erection during the past year. Figure 2 displays the prevalence of erectile dysfunction by age group. The prevalence of ED is higher in older age groups. The prevalence of ED is 28.7 percent among those between 57 and 64 years of age, and 45.1 and 45.7 percent among the older two age groups.
Figure 2. Observed Prevalence of Erectile Dysfunction in Different Age Groups.

Note: Means are estimated using NSHAP person-level weights, with post-stratification adjustments for non-response and adjustments for probability of inclusion in the main analysis. Estimates are calculated for all cases for which data are available on all key variables in the multivariate analysis.
Our main hypothesis is that some men’s erectile difficulties stem from the psychological and/or relational consequences of partner betweenness. It is important to emphasize at this point the relative infrequency of this relational circumstance. Figure 3 shows the distribution of sexually active older men who experience partner betweenness, disaggregated by network size. For example, of the men included in the main analysis, 147 have just two confidants apart from their partner, and in 30 of these cases the partner has more contact with at least one of those two confidants than the respondent has. In general, while the majority of men have more contact with all of their confidants than their partners do, an estimated 25.2 percent experience partner betweenness in at least one of their confidant relationships. The likelihood of partner betweenness is greater among men who have larger networks, in part because the random chance that one’s partner has a strong relationship with one of those confidants is greater.
Figure 3. Prevalence of Partner Betweenness among Older Men with Different Numbers of Confidants (N = 678).

Note: Includes all male respondents who are known to have had sex in the past year, who have a current spouse/partner, and who have at least one confidant apart from their spouse/partner.
Our main goal is to understand how this feature of network structure relates to ED. Table 2 presents odds ratios from logistic regression analyses predicting whether men reported ED in the past year, adjusting for a number of key risk factors. The first model includes partner betweenness, network structure controls, and life course measures. From this and subsequent models, we find that older men are more likely to have experienced ED. Models 2 and 4 highlight the importance of relationship factors. In general, men who are married to their partners are less likely to experience ED. Also, as expected, frequency of sexual intercourse is negatively associated with ED. Other measures of relationship quality appear to be less relevant. Satisfaction with partner, whether the partner is demanding, and the amount of free time partners spend together have no significant association with ED. Overall, these findings highlight the importance of high-quality intimate partnerships to men’s sexual health.
Table 2.
Odds Ratios from Logistic Regression Models Predicting Erectile Dysfunction (N = 678)a
| Predictor | Model 1 | Model 2b | Model 3c | Model 4b,c |
|---|---|---|---|---|
| Partner betweenness | 1.759** (.342) | 1.864** (.375) | 1.711** (.327) | 1.916** (.389) |
| Proportion kin | .659 (.207) | .770 (.229) | .697 (.213) | .785 (.240) |
| Proportion female | 1.205 (.402) | 1.140 (.380) | 1.122 (.340) | 1.064 (.335) |
| Age (ref: 57–64): | ||||
| 65 – 74 | 2.282*** (.456) | 2.393*** (.558) | 2.326** (.543) | 2.284** (.565) |
| 75 – 85 | 2.393** (.737) | 2.290* (.769) | 2.261* (.694) | 2.229* (.755) |
| Retired | .892 (.260) | .828 (.242) | .756 (.194) | .747 (.196) |
| Married to partner | -- | .695 (.178) | -- | .555* (.143) |
| Frequency of sex (ref: monthly or less): | ||||
| 2–3 times a month | -- | .372*** (.097) | -- | .402** (.118) |
| 1–2 times a week | -- | .320*** (.089) | -- | .394** (.127) |
| > 2 times a week | -- | .256** (.114) | -- | .247** (.106) |
| Partner satisfaction | -- | .872 (.133) | -- | .870 (.148) |
| Partner demanding | -- | 1.536 (.446) | -- | 1.693 (.501) |
| Prostate trouble | -- | -- | 2.189*** (.401) | 2.134*** (.380) |
| Diabetes | -- | -- | 2.898** (.970) | 2.873** (.909) |
| Self-rated health (ref: excellent) | ||||
| Poor/Fair | -- | -- | 4.184*** (1.392) | 4.002*** (1.321) |
| Good | -- | -- | 2.984** (1.063) | 3.101** (.982) |
| Very good | -- | -- | 3.267** (1.280) | 3.154** (1.101) |
| F (d.f.) | 3.83** (9,43) | 4.25*** (16,36) | 4.29*** (24,28) | 4.47*** (31,21) |
| Fleiss, Williams, Dubro R2 | .044 | .087 | .132 | .159 |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, education, and whether R is out of the labor force.
Includes control for amount of time spent with partner.
Controls for obesity, cardiovascular problems, cancer, CES-D-ml, functional health, SPMSQ, use of medications, and rating of partner's health.
Models 3 and 4 confirm that health is important to consider. Men who report having had prostate trouble and those who have diabetes are more likely to report ED. Likewise, men who report being in poor/fair, good, or even very good overall health are more likely to report ED than those who report being in excellent health. These associations are strong. Comparing extreme ends of the spectrum, men who are in poor or fair health are four times as likely to report having had ED as men who are in excellent health. These findings are consistent with medical research which emphasizes organic causes and risk factors of ED, likely reflecting the consequences of things like reduced blood flow and nerve damage. Several measures of health are not significantly associated with ED, however, net of other factors. These include obesity, cardiovascular problems, cancer, and functional health, as well as medication use.
It is also important to note that measures of psychological and cognitive well-being –depressive symptoms as measured by the CES-D-ml and cognitive function as measured by the SPSMQ –are not significantly associated with ED. An analysis of smaller subsamples of men (for whom data were available) also shows that neither self-esteem nor anxiety are significantly associated with ED (see Appendix Table A2). All other predictors remain associated with ED in the same way in these analyses as in the main analysis that is shown in Table 2.
Appendix Table A2.
Odds Ratios from Logistic Regression Models Predicting Erectile Dysfunctiona
| Self-Esteem Models (N = 633)
|
Anxiety Models (N = 637)
|
|||
|---|---|---|---|---|
| Predictor | Model 1 | Model 2 | Model 1 | Model 2 |
| Partner betweenness | 1.694* (.370) | 1.690* (.364) | 1.703* (.347) | 1.694* (.346) |
| Age (ref: 57–64): | ||||
| 65 – 74 | 2.264** (.527) | 2.270** (.527) | 2.354** (.542) | 2.325** (.541) |
| 75 – 85 | 2.181* (.755) | 2.211* (.771) | 2.259* (.764) | 2.222* (.747) |
| Married to partner | .522* (.144) | .527* (.146) | .510* (.140) | .519* (.146) |
| Frequency of sex (ref: monthly or less): | ||||
| 2–3 times a month | .439* (.135) | .436* (.136) | .427** (.130) | .427** (.130) |
| 1–2 times a week | .405* (.138) | .408* (.139) | .403** (.134) | .401** (.132) |
| > 2 times a week | .247** (.119) | .241** (.118) | .244** (.118) | .246** (.119) |
| Partner satisfaction | .858 (.146) | .852 (.147) | .865 (.147) | .865 (.147) |
| Partner demanding | 1.593 (.499) | 1.532 (.482) | 1.501 (.474) | 1.501 (.473) |
| Prostate trouble | 2.072*** (.370) | 2.073*** (.372) | 2.202*** (.398) | 2.191*** (.390) |
| Diabetes | 2.654** (.854) | 2.667** (.850) | 2.647** (.850) | 2.631** (.855) |
| Self-rated health (ref: excellent) | ||||
| Poor/Fair | 3.458** (1.179) | 3.644** (1.330) | 3.154** (1.088) | 3.143** (1.084) |
| Good | 3.303** (1.073) | 3.479** (1.171) | 3.134** (1.038) | 3.129** (1.031) |
| Very good | 3.224** (1.183) | 3.333** (1.249) | 3.222** (1.179) | 3.206** (1.168) |
| Self-esteem (ref: Not true that R has high SE) | ||||
| ”Somewhat true” that R has high SE | -- | 1.049 (.379) | -- | -- |
| ”Very true” that R has high SE | -- | 1.223 (.427) | -- | -- |
| Anxiety | -- | -- | -- | .912 (.178) |
| F (d.f.) | 4.07*** (31,20) | 3.91** (33,18) | 4.02*** (31,20) | 4.54*** (32,19) |
| Fleiss, Williams, Dubro R2 | .144 | .142 | .146 | .145 |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and include all of the same controls as are included in the final model in Table 2. Both sets of models include all cases for which data are available on all variables.
Of greatest interest to us, partner betweenness is a significant predictor of erectile dysfunction. From the final model, a man whose female partner has greater contact with some of his confidants than he does is about 92 percent more likely to have had trouble getting or maintaining an erection than a man who has greater access than his partner does to all of his confidants (OR = 1.916; 95% CI, 1.274 – 2.881; p = .002). Thus, it does not appear that the positive association between partner betweenness and ED shown in model 1 is due to the other factors measured here, including generalized relationship troubles (e.g., having an unsatisfying relationship), psychological troubles (e.g., depression), or health problems that may bring one’s intimate partner in greater contact with one’s confidants. The significance of partner betweenness is neither explained nor appreciably reduced by the inclusion of these measures.
Nonetheless, we think that several mechanisms along these lines contribute to the relationship between partner betweenness and ED. As argued earlier, partner betweenness is connected to a number of circumstances which can trigger psychogenic ED by reducing men’s responsiveness to physical and erotic stimuli. NSHAP provides only limited measures along these lines, none of which are directly associated with ED. It is possible, however, that these factors are associated with similar, unmeasured factors that lie on psychogenic pathways between partner betweenness and ED. These may include psychological factors such as low sense of control or low sense of masculinity, as well as relational factors like partner conflict, partner resentment, or lack of interest in one’s partner.
Bivariate tests show that depression is significantly positively associated with ED (r = .113, p < .003) and that partner satisfaction is significantly negatively associated with ED (r = −.092, p < .02). Thus, although the available measures do not constitute mechanisms that relate partner betweenness to ED, it is possible that related psychogenic factors are relevant. We conducted additional analyses predicting self-esteem, anxiety, depression, and partner satisfaction using partner betweenness and other relevant measures (see Appendix Table A3). This analysis reveals that of these four factors, only partner satisfaction is significantly predicted by partner betweenness (b = −.127, SE = .063, p < .05). We cannot detect any other relevant psychological or identity-related consequences of partner betweenness (e.g., for sense of masculinity). This provides some support for the idea that men are less satisfied with partners who are in positions of betweenness in their confidant relationships, and that this may have further consequences for the relationship that give rise to ED. We are unable to assess how partner betweenness affects other, potentially more relevant relational factors such as resentment of one’s partner, lack of attraction to one’s partner (or vice versa), or partner conflict –all of which may reduce men’s interest in sex and /or responsiveness to erotic stimuli.
Appendix Table A3.
Unstandardized Coefficients from Regression Models Predicting Self-Esteem, Depression, and Satisfaction with Partnera
| Predictor | Self-Esteemb (Ordered Logistic) | Anxietyc (OLS) | Depressiond (OLS) | Partner Satisfactione (OLS) |
|---|---|---|---|---|
| Partner betweenness | 1.086 (.234) | −.066 (.050) | .039 (.052) | −.128* |
| Age (ref: 57–64): | ||||
| 65 – 74 | 1.105 (.270) | −.138* (.052) | .015 (.039) | −.038 (.060) |
| 75 – 85 | 1.163 (.481) | −.221** (.063) | −.087 (.057) | −.103 (.085) |
| Frequency of sex (ref: monthly or less): | ||||
| 2–3 times a month | 1.322 (.320) | .000 (.075) | −.028 (.050) | .042 (.062) |
| 1–2 times a week | .942 (.230) | −.073 (.071) | −.053 (.043) | .162** (.059) |
| > 2 times a week | 1.362 (.578) | .111 (.081) | .088 (.100) | .153* (.075) |
| Partner satisfaction | 1.369* (.187) | −.090* (.039) | −.087** (.031) | −- |
| Partner demanding | 2.171 (.838) | .020 (.114) | .105 (.090) | −.215* (.102) |
| Partner critical | 1.192 (.470) | −.088 (.107) | −.041 (.082) | −.496*** (.087) |
| Openness with partner | 1.429 (.327) | −.028 (.076) | −.083 (.047) | .210** (.077) |
| Reliability of partner | 1.009 (.385) | −.073 (.122) | −.039 (.084) | .252** (.086) |
| Free time spent with partner | .627* (.137) | −.013 (.048) | −.039 (.030) | .194** (.059) |
| Intercept | -- | .184 (.350) | −.021 (.258) | −.554 (.333) |
| F(d.f.) | 2.50* (26,25) | 5.21*** (32,19) | 10.35*** (32,20) | 34.18*** (30,22) |
| N | 630 | 633 | 674 | 674 |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, gender/kin composition of network, partner's average frequency of contact with confidants, marital status, whether partner is coresident, education, employment status, and SPMSQ. All cases with valid data are included. All cases from main analysis that have valid data are included.
Odds ratios are presented. A likelihood ratio test does not suggest that the proportional odds assumption is violated (χ2 = 32.63, df = 25, p = .141). Controls for functional health and self-rated health are included.
Anxiety measured using HADS subscale. Controls for functional health, overall self-rated health, and partner's mental and overall health are included.
Depressed measured as CES-D-ml. Controls for functional health, overall self-rated health, and partner's mental and overall health are included.
Controls for CES-D-ml, self-rated happiness, and partner's mental and overall health are included.
Other Erectile Difficulties
It is worth noting that similar findings emerge in parallel analyses predicting whether men experienced trouble achieving climax (anorgasmia) as well as whether they experienced the combination of that condition with ED (compound dysfunction). These analyses are presented in Appendix Tables A4 and A5. Fewer variables are predictive of these forms of dysfunction. However, it is apparent that the prevalence of both problems is higher among older men, lower among men who are married, and higher among those who have sex less frequently. Health has more scattered associations with these forms of dysfunction. Prostate trouble is positively associated with both forms, while self-rated health has a significant association only with compound dysfunction.
Appendix Table A4.
Odds Ratios from Logistic Regression Models Predicting Anorgasmia (N=670)a
| Predictor | Model 1 | Model 2b | Model 3c | Model 4b,c |
|---|---|---|---|---|
| Partner betweenness | 1.515 (.366) | 1.678* (.410) | 1.539 (.362) | 1.780* (.453) |
| Proportion kin | .548 (.187) | .635 (.217) | .533 (.171) | .605 (.205) |
| Proportion female | 1.602 (.623) | 1.514 (.622) | 1.642 (.648) | 1.574 (.671) |
| Age (ref: 57–64): | ||||
| 65 – 74 | 2.203** (.594) | 2.221** (.632) | 2.070** (.545) | 2.057* (.576) |
| 75 – 85 | 3.736*** (1.017) | 3.168*** (.917) | 3.460*** (1.034) | 3.060** (.996) |
| Retired | .994 (.264) | .994 (.272) | .857 (.250) | .865 (.264) |
| Married to partner | -- | .454* (.149) | -- | .435* (.150) |
| Frequency of sex (ref: monthly or less): | ||||
| 2–3 times a month | -- | .346*** (.093) | -- | .342** (.102) |
| 1–2 times a week | -- | .260*** (.070) | -- | .288*** (.082) |
| > 2 times a week | -- | .474 (.202) | -- | .488 (.222) |
| Partner satisfaction | -- | 1.094 (.159) | -- | 1.131 (.168) |
| Partner demanding | -- | 1.014 (.419) | -- | 1.085 (.406) |
| Prostate trouble | -- | -- | 1.910** (.378) | 1.869** (.373) |
| Diabetes | -- | -- | 1.292 (.436) | 1.260 (.440) |
| Self-rated health (ref: excellent) | ||||
| Poor/Fair | -- | -- | 1.873 (.945) | 1.551 (.849) |
| Good | -- | -- | 1.512 (.733) | 1.452 (.715) |
| Very good | -- | -- | 1.328 (.581) | 1.185 (.513) |
| F (d.f.) | 4.07*** (9,42) | 5.03*** (16,35) | 5.87*** (24,27) | 5.98*** (31,20) |
| Fleiss, Williams, Dubro R2 | .041 | .077 | .084 | .109 |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, education, and whether R is out of the labor force.
Includes control for amount of time spent with partner.
Controls for obesity, cardiovascular problems, cancer, CES-D-ml, functional health, SPMSQ, use of medications, and rating of partner's health.
Appendix Table A5.
Odds Ratios from Logistic Regression Models Predicting Compound ErectileDysfunction (N=667)a
| Predictor | Model 1 | Model 2b | Model 3c | Model 4b,c |
|---|---|---|---|---|
| Partner betweenness | 1.778* (.506) | 1.954* (.544) | 1.965* (.564) | 2.316** (.705) |
| Proportion kin | .597 (.245) | .742 (.304) | .541 (.221) | .651 (.283) |
| Proportion female | 1.777 (.708) | 1.645 (.702) | 2.063 (.785) | 1.951 (.839) |
| Age (ref: 57–64): | ||||
| 65 – 74 | 1.949* (.554) | 1.996* (.578) | 1.754* (.466) | 1.764 (.504) |
| 75 – 85 | 3.321*** (1.004) | 2.890** (.956) | 2.939** (.874) | 2.628** (.921) |
| Retired | 1.269 (.322) | 1.197 (.335) | 1.126 (.319) | 1.125 (.321) |
| Married to partner | -- | .427* (.157) | -- | .365* (.139) |
| Frequency of sex (ref: monthly or less): | ||||
| 2–3 times a month | -- | .318** (.096) | -- | .330** (.121) |
| 1–2 times a week | -- | .265*** (.081) | -- | .306** (.106) |
| > 2 times a week | -- | .388* (.179) | -- | .353* (.172) |
| Partner satisfaction | -- | 1.060 (.180) | -- | 1.078 (.188) |
| Partner demanding | -- | 1.116 (.533) | -- | 1.454 (.589) |
| Prostate trouble | -- | -- | 2.665*** (.627) | 2.658*** (.604) |
| Diabetes | -- | -- | 1.344 (.503) | 1.314 (.513) |
| Self-rated health (ref: excellent) | ||||
| Poor/Fair | -- | -- | 5.856** (3.817) | 5.426* (3.691) |
| Good | -- | -- | 3.369* (1.727) | 3.617* (1.923) |
| Very good | -- | -- | 3.227* (1.684) | 3.086* (1.595) |
| F (d.f.) | 4.49*** (9,42) | 5.54*** (16,35) | 3.12** (24,27) | 3.44** (31,20) |
| Fleiss, Williams, Dubro R2 | .034 | .068 | .121 | .147 |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, education, and whether R is out of the labor force.
Includes control for amount of time spent with partner.
Controls for obesity, cardiovascular problems, cancer, CES-D-ml, functional health, SPMSQ, use of medications, and rating of partner's health.
Partner betweenness is significantly associated with both anorgasmia and compound dysfunction, net of other factors. From the final model of Table A4, men whose networks involve partner betweenness are about 78 percent more likely to have had difficulty achieving climax during sex than men whose partners have less frequent contact with all of their confidants. This estimate is somewhat less reliable than the association that is evident in the analysis of ED (OR = 1.780; 95% CI, 1.067–2.968; p =. 028). Likewise, from the final model of Table A5, we find that men who experience partner betweenness are about 2.3 times as likely to report compound dysfunction (OR = 2.316; 95% CI, 1.256–4.270; p =. 008).
Partner Betweenness in Specific Types of Relationships
An important question is: Does partner betweenness in specific types of confidant relationships matter more than non-specific partner betweenness? For example, one might expect that partner betweenness in a man’s relationship with one of his male confidants poses a greater threat to masculinity, or causes partner conflict for other reasons (e.g., jealousy over the female partner’s involvement with the confidant), more than female partner betweenness in a relationship with a female confidant does. And there are conflicting expectations with respect to kin. Non-kin ties may yield more access to external resources and are less likely to be joint members of the couple’s network. Therefore, non-kin ties might reflect more on men’s autonomy and sense of control. On the other hand, recent work in social gerontology suggests that kin relations (especially blood relations, such as children and grandchildren) play a greater role in a new kind of masculinity that emerges in later life, and may help men feel as if they “matter” even more than non-kin ties do.
To explore these issues, we constructed indicators of the presence of different forms of partner betweenness with respect to the gender and kin status of confidants: 1) female kin confidant; 2) male kin confidant; 3) female non-kin confidant; or 4) male non-kin confidant. We then used these variables instead of the general indicator of betweenness (see Appendix Table A6). Regardless of whether we entered these indicators simultaneously or separately, none of the variables is significant. Therefore, it appears that what matters is not partner betweenness with respect to any specific type of confidant, but rather the experience of partner betweenness in general and what it says about a man’s network and his partner’s role in it. As we will see below, however, overall access to different types of confidants matters.
Appendix Table A6.
Odds Ratios from Logistic Regression Models Assessing Associations between Specific Types of Partner Betweenness and Erectile Dysfunction (N = 678)a
| Partner Betweenness with Respect to: | Betweenness indicators entered simultaneously | Betweenness indicators entered separately |
|---|---|---|
| Female kin | 1.583 (.531) | 1.546 (.515) |
| Male kin | 1.464 (.502) | 1.525 (.520) |
| Female non-kin | .848 (.430) | .970 (.477) |
| Male non-kin | 1.964 (.961) | 1.937 (.892) |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for all variables included in Table 2.
The Role of the Life Course
Our main models suggest that age is positively associated with ED, whereas retirement is not. To push this further, a related question is whether the challenges of later life reduce or amplify the potential impact of partner betweenness on ED. To test this idea, we considered interactions between age and partner betweenness. This analysis is shown in Table 3, model 2. It shows that the positive association between partner betweenness and ED is smaller among the older age groups as compared to the youngest age group– significantly so among men between 65 and 74 years of age. This relationship is illustrated in Figure 4. The upshot is that partner betweenness is more closely related to ED among the youngest men in the sample. We tested additional models, but found only a marginal interaction between partner betweenness and retirement status (p = .073), and no significant interaction with various health measures. Thus, the interaction shown in model 2 of Table 3 is likely driven by a combination of factors that change throughout later life, including unmeasured facets of health, new social activities, bereavement, and grandparenthood. Age may work in the interaction because it indexes this broader complex of factors.
Table 3.
Log Odds from Logistic Regression Models Assessing Interactions between Retirement, Age, and Partner Betweenness with Respect to Erectile Dysfunction (N = 678)a
| Predictor | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Partner betweenness | 1.916** (.389) | 3.227*** (.894) | 1.968** (.402) |
| Proportion kin | .785 (.240) | .776 (.234) | 1.681 (.648) |
| Age (ref: 57–64): | |||
| 65 –74 | 2.284** (.565) | 3.160*** (.863) | 5.106*** (2.189) |
| 75 – 85 | 2.229* (.755) | 2.798* (1.079) | 5.970** (3.236) |
| Partner betweenness x age (65–74) | .334* (.141) | -- | |
| Partner betweenness x age (75–85) | .469 (.302) | -- | |
| Proportion kin x age (65–74) | -- | -- | .240* (.132) |
| Proportion kin x age (75–85) | -- | -- | .162* (.131) |
| F (d.f.) | 4.47*** (31,21) | 4.08** (33,19) | 3.88** (33,19) |
| Fleiss, Williams, Dubro R2 | .159 | .164 | .167 |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for all variables included in Table 2.
Figure 4. Predicted Probability of Erectile Dysfunction among Older Men, by Age Group and Partner Betweenness.

Note: Estimates are predicted probabilities derived from the final model predicting difficulty getting and/or maintaining an erection, presented in Table 3. Covariates are held at their median values.
Finally, we also found that while the kin composition of a network is not associated with erectile difficulties in an additive sense, it has a conditional association with ED that depends on age. As shown in Figure 5, kin composition is most closely associated with ED among the oldest men. In the youngest age group, kin composition has only a slight positive association with ED in that younger men who have more kin in their networks evince greater likelihood of ED. But the opposite holds for the older age groups. In the older men, having fewer kin in one’s network is a risk factor for ED. Among men between 65 and 74 years of age, those who have no kin in their networks are twice as likely to suffer from ED as those whose networks are comprised entirely of kin confidants. This difference is even stronger in the oldest age group, where those who have no kin in their networks are three times as likely to report erectile dysfunction.
Figure 5. Predicted Probability of Erectile Dysfunction among Older Men, by Age and Network Kin Composition.
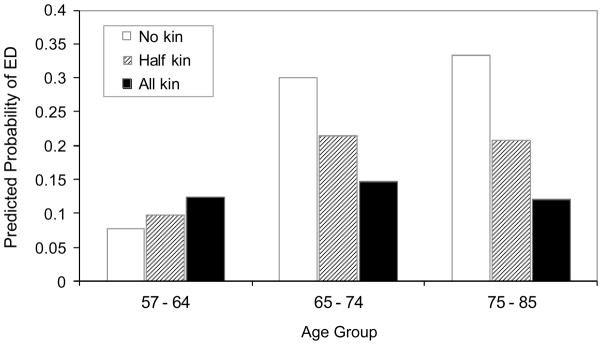
Note: Estimates are predicted probabilities derived from the final model predicting difficulty getting and/or maintaining an erection, presented in Table 3. Covariates are held at their median values (assuming no partner betweenness).
CONCLUSION
We have shown that there is a strong association between older men’s erectile difficulties and their positions in social networks vis-à-vis their female partners. Men who experience partner betweenness in their (joint) confidant relationships are more likely to have trouble getting or maintaining an erection, and are also more likely to experience difficulty achieving orgasm during sex. These findings are consistent with the notion that ED partly reflects men’s embeddedness within networks that limit opportunities for autonomy, control, and privacy. Among the youngest age group in this sample, this relational circumstance has an association with ED that rivals that of prostate trouble.
Gender and sexuality theories that link masculinity to sexual function might interpret these findings as indicative of some men’s insecurity about their independence and sense of control, which are central to traditional ideals of masculinity. This relational gender theory interpretation adds a novel twist to existing theories in sexual health research that point to psychogenic causes of ED. It is possible that partner betweenness in confidant relationships indirectly leads to ED by affecting psychological factors such as self-esteem and depression. Our analyses provide little or no evidence that partner betweenness operates through this particular pathway, but we repeat our caution that we do not have the data necessary to test the role of men’s sense of masculinity or insecurity about gender identity.
The association between partner betweenness and ED could also occur through pathways that involve the quality of men’s relationships with their female partners. The only data we have to support this explanation is that partner betweenness is negatively associated with partner satisfaction, which is significantly associated with ED in bivariate analyses. The satisfaction measure may partially capture more relevant relational factors such as men’s negative attitudes toward the female partner, decreased sexual interest in and attractiveness to her, increased partner conflict, and problems with dyadic adjustment (Spanier 1976). We also lack data on the implications partner betweenness has for the female partner, including how it affects the quality of her emotional relationships with her male partner, her attitudes toward him, and her efforts to arouse him.
Whatever the case, the results point to the importance of social network factors that are rarely considered in medical research– network structure and the individual’s position within it. Research on the link between networks and health typically conflate social networks with related concepts like social support (Smith and Christakis 2008). The mechanisms that are likely at play in the particular relationship examined here involve a structural network feature– partner betweenness –which operates net of network composition, size, and various dyadic factors that are more commonly addressed in health research. Furthermore, this is a supradyadic process which depends not on partner betweenness with respect to any specific type of confidant, but rather on the experience of partner betweenness in any form. Because we are trained in structural phenomena and social relationships, sociologists are uniquely positioned to inject a level of methodological rigor into health research that draws on “social network” imagery and language.
The fact that the association between partner betweenness and ED all but disappears among the older men in the sample may be an indication that extensive partner involvement in confidant relations cease to represent a threat to men’s gender identities at older ages. We were surprised to find that the association between partner betweenness and ED depends on age. The most extreme conceptions of masculinity, which emphasize “hegemonic” traits (Connell 1995), allow little flexibility in the emphasis on male dominance in all aspects of men’s lives. One might therefore expect that the threats to independence and control posed by some later-life transitions –especially retirement –prompt men to tighten control over their remaining social resources. Partner betweenness could play an even greater role in this heightened circumstance. But the opposite appears to be the case. Partner betweenness has little association with sexual problems among the oldest men. This finding might reveal something about the changing implications of network position for gender identity through the life course. It could reflect shifting relational priorities among older men, from individualistic to familial. Or it could be that the independence and control that men can gain through weak ties become less important to them as they experience later-life changes like health decline, which may increase the value of their connections to people who are deeply embedded in their support network. Either way, older men’s focus on close, kin-oriented relationships increases their likelihood of adopting new definitions of masculinity that emphasize conveying experience and mentoring (Davidson, Daly, and Arber 2003; Mann 2007; Waldrop et al. 1999). Under these circumstances, partner betweenness would be less likely to trigger psychogenic ED.
Unaddressed Issues
Women’s Social Networks
Unaddressed here (due to lack of data) is what role the female partner’s social network plays in men’s sexual function. It would help to be able to identity other aspects of the link between both partners’ network ties and their sexual relationship. It is possible, for instance, that partner betweenness indexes dyadic withdrawal, a situation in which long-term partners’ social circles converge over time (Kalmijn 2003), and which is therefore more common among older adults. If this is true, we might expect men to have betweenness in their female partners’ networks as well. To what extent this has consequences for men’s sense of control or for the quality of a couple’s intimate relationship which offset any negative consequences of the female partner’s betweenness is a worthy research topic. Unfortunately, we cannot tell much about partner network overlap with these data.
Women’s Sexual Function
This paper does not speak to women’s sexual problems. A sociological perspective on female sexual dysfunction may follow the argument that women’s sexual problems reflect tensions within intimate heterosexual relationships that arise from institutionalized gender inequalities (Duncombe and Marsden 1996). Some feminist scholars argue that these inequalities extend to sexual relations as well, such that heterosexual encounters are vital to men’s dominance over and oppression of women. This might be illustrated, for instance, in the normalization of unreciprocated sexual satisfaction, especially with respect to orgasm (Braun, Gavey, and McPhillips 2003). Because sense of control and autonomy are not central to femininity like they are to masculinity, the extent to which male partners are embedded within heterosexual women’s social networks may not have a close association with women’s sexual experiences. However, Martin (2005) argues that women are less attracted to men who have less power than they do, which may affect some women’s levels of interest in sex. Thus, a network approach to women’s sexual problems that relates back to this issue of male partners’ masculinity is feasible.
Selection
Sample selection bias may be an issue here. The present study applies only to men who have confidants, and therefore offers little insight into the sexual problems of men whose social lives revolve entirely around their partners. For those men, the connectedness of the female partner may be even more important. Older men who do not have other confidants –perhaps because they prefer spending their free time with their partner or because their closest friends have died – may not be adversely affected by their partners’ social connectedness. Having a female partner who is just as isolated from confidants could enhance the intensity of the emotional and sexual relationship, as implied by dyadic withdrawal research. At the same time, such isolation could have negative psychological and social (and ultimately sexual) consequences for both partners.
There are also potential issues with selection among those who have larger networks. Only longitudinal data will make it possible to assess the duration of partner betweenness, for example, and whether it indexes very recent shifts in partners’ involvement with confidants as opposed to more static network configurations to which men have been accustomed for years. If the latter, the findings reported here may reflect not the influence of injured masculine identity on psychogenic ED, but rather the selection into certain kinds of network configurations by men who are for some reason predisposed to ED – for example, men who had preexisting chronic health problems who restricted their networks to shared kin relations years ago.
Endogeneity
A final and repeated caution regarding the limitations of our data is in order. Our models are likely plagued by endogeneity that we cannot remedy. The models may suffer from omitted variable bias, which would be most severe if partner betweenness captures partners’ efforts to coordinate support among network members in response to health problems for which we have no measures. Dual causation may also be present in our models in several respects, such as in the relationship between frequency of sex and ED. Another concern is that ED affects social relationships outside of the intimate partnership, perhaps by causing men to withdraw from other social ties. Their erectile difficulties may also prompt their female partners to seek advice from, to confide in, or to seek comfort in the couple’s joint contacts. ED does predict partner betweenness in a reversed model, so this will require further scrutiny. But supplementary analyses (not shown) suggest that this reversal does not hold up as universally as the models presented here (e.g., difficulty climaxing is only marginally significant). Furthermore, we would expect this kind of confiding to occur mainly with joint female confidants, but none of the forms of erectile difficulties explored here are even marginally significant in models predicting this specific form of partner betweenness. This is an interesting direction for research on the consequences of sexual experiences for social network structure. In any case, additional work is needed to determine whether the association between partner betweenness and ED is causal.
Hopefully, future work related to this topic will demonstrate the usefulness of network theories in clarifying the conceptualization and measurement of social connections that matter for older adults. This age group has been examined with great interest by health researchers, but sociologists are uniquely positioned to explore the role of specific structural features of networks for older adults’ health. Additional insight into the link between networks and successful aging among both men and women will be gained also by exploring how structural features of older adults’ joint networks affect their gender identities, dyadic adjustment, and the overall quality of their intimate relationships.
Appendix Table A1.
Odds Ratios from Logistic Regression Models Predicting Erectile Dysfunction, Including Men Who Report No Sexual Activity within the Past Year (N=923)a
| Predictor | Model 1 | Model 2b | Model 3c | Model 4b,c |
|---|---|---|---|---|
| Partner betweenness | 1.521* (.241) | 1.538* (.262) | 1.492* (.256) | 1.548* (.280) |
| Proportion kin | .815 (.208) | .889 (.236) | .916 (.230) | .978 (.259 |
| Proportion female | 1.358 (.439) | 1.254 (.411) | 1.227 (.397) | 1.147 (.391) |
| Age (ref: 57–64): | ||||
| 65 – 74 | 2.513*** (.456) | 2.578*** (.504) | 2.645*** (.584) | 2.613*** (.579) |
| 75 – 85 | 4.906*** (1.211) | 5.172** (1.310) | 4.880*** (1.388) | 4.963*** (1.395) |
| Retired | 1.137 (.319) | 1.086 (.307) | .933 (.237) | .901 (.235) |
| Married to partner | -- | 1.228 (.292) | -- | .999 (.247) |
| Partner satisfaction | -- | .659** (.089) | -- | .713* (.118) |
| Partner demanding | -- | 1.438 (.350) | -- | 1.573 (.427) |
| Prostate trouble | -- | -- | 1.546** (.245) | 1.618** (.255 |
| Diabetes | -- | -- | 2.473** (.674) | 2.488** (.635) |
| Self-rated health (ref: excellent) | ||||
| Poor/Fair | -- | -- | 3.470*** (.953) | 3.410*** (.891) |
| Good | -- | -- | 2.505** (.686) | 2.432** (.661) |
| Very good | -- | -- | 2.423* (.864) | 2.336* (.842) |
| F (d.f.) | 7.41*** (9,44) | 6.75*** (13,40) | 6.64*** (24,29) | 6.49*** (28,25) |
| Fleiss, Williams, Dubro R2 | .094 | .117 | .195 | .209 |
p < .05,
p < .01,
p < .001 (two-tailed tests)
Estimates are weighted to adjust for probability of inclusion in the analysis and differential non-response. All models are survey-adjusted, and control for network size, education, and whether R is out of the labor force.
Includes control for amount of time spent with partner.
Controls for obesity, cardiovascular problems, cancer, CES-D-ml, functional health, SPMSQ, use of medications, and rating of partner's health.
Acknowledgments
The National Social Life, Health, and Aging Project is supported by the National Institutes of Health (5R01AG021487), which also provided partial funding for this research. Earlier versions of this paper were presented at Sunbelt XXVIII, the annual meeting of the International Network for Social Network Analysis, St. Pete Beach, Florida, January 2008, and at the annual meeting of the International Academy of Sex Research, Prague, Czech Republic, July 2010. We thank Matthew E. Brashears, Erin York Cornwell, William Dale, Stephen L. Morgan, Michael A. Perelman, L. Philip Schumm, Linda J. Waite, the AJS editors, and four anonymous reviewers for providing valuable suggestions and guidance.
Footnotes
We are grateful to an anonymous reviewer for suggesting this mechanism to us.
Most of the data for the NSHAP study were collected during a two-hour in-home interview. To minimize the length of the in-home portion of the study, some questions were asked via a paper questionnaire that interviewers left behind for respondents to complete and mail in at their leisure (84% response rate). However, none of those items are used here. Additional information about the design of NSHAP can be found at: http://www.norc.org/NSHAP.
Valid data on who had had sex within the past year are available for 1,381 of the 1,455 men who were interviewed.
Following the in-home interview, NORC interviewers were asked to provide an ordinal subjective assessment of how candid respondents were, ranging from 1 = “probably not candid at all” to 4 = “entirely candid.” Some reassurance that honesty does not play a large role in responses to questions about sexual problems comes from the fact that there are no significant associations between the interviewer rating and respondents’ reports of trouble reaching climax (χ2 = 1.497, d.f. = 3, p = .749) or trouble getting/maintaining an erection (χ2 = 5.350, d.f. = 3, p = .345)
Respondents were also asked to identify any other (one) person to whom they felt “especially close” and who had not already been identified as a confidant or spouse/partner. We do not include these close contacts in the network because doing so corrupts the conceptual significance of the network. We are interested in core confidants, not necessarily emotionally “close” contacts who are not confidants. However, including these close contacts in the assessment of partner betweenness does not change the main findings.
Because the network data are based on self-reports, it is possible that respondents misperceive their partners’ ties. In many ways, what we are concerned about is the respondent’s perception of their partners’ embeddedness. These perceptions have psychological implications for individuals above and beyond the “true” structure of the network being reported (Krackhardt 1987). The mere perception that one’s partner has more contact with a core confidant could affect a man’s sense of autonomy, self-esteem, sense of privacy, and other relevant factors.
We experimented with alternative operationalizations of this concept, including a count of the number of triads in ego’s network of form, and the proportion. Neither worked as well as the dichotomous version reported on here, possibly because both are highly dependent on the size of the network.
One reviewer suggested that we test whether partner age matters. Supplementary analyses (not shown) suggest that those with young partners are more likely to experience ED. Tested another way, those whose partners are much younger than them (relative age) are more likely to experience ED. We do not include this in our analysis, however, as it is somewhat peripheral to our theory, and including it results in a loss of 10 percent of our cases (because NSHAP did not collect age for non-coresident partners).
Field interviewers recorded respondents’ responses to these items, and the responses were coded as either correct or incorrect by NORC after comparing them to information NORC had on file (e.g., the date the interview actually took place). The accuracy of responses was also ascertained and coded as being either correct or incorrect by field interviewers as they were provided. There were some discrepancies between these assessments. We use NORC’s coding of responses, but using field interviewers’ assessments does not change the results.
We conducted several analyses to probe sensitivity of findings to modeling strategy. In one analysis, we assume that men who reported that they had a partner but did not have sex in the past year did have problems such as ED and simply had no opportunity to report it. We recode these men as having had ED, and conduct the main analysis with this large sample (N = 923). Results are reported in Appendix Table A1.
We also conducted a two-stage probit heckman selection model in which the probability of selection into the main model (not having missing data on any of the key variables) is predicted in the first stage and erectile dysfunction is predicted in the second (N = 1,437). This approach models the probability of erectile dysfunction as conditional on all of the factors that make men eligible for the analysis in the first place (i.e., having at least one non-partner confidant, having a partner, and having had sex recently), effectively treating selection bias as a form of omitted variable bias (Heckman 1979) The original NSHAP weights are used in this analysis. The findings (available upon request) do not differ substantively from the main findings of the analysis presented here.
Contributor Information
Benjamin Cornwell, Email: btc49@cornell.edu, Department of Sociology, 354 Uris Hall, Cornell University, Ithaca, NY 14853.
Edward O. Laumann, Email: e-laumann@uchicago.edu, Department of Sociology, University of Chicago, 1126 E. 59thStreet, Chicago, IL 60637
References
- Adams Rebecca G, Ueno Koji. Middle-Aged and Older Adult Men’s Friendships. In: Bedford Victoria Hilkevitch, Turner Barbara F., editors. Men in Relationships: A New Look from a Life Course Perspective. New York: Springer; 2006. pp. 103–24. [Google Scholar]
- Avison William R, Cairney John. Social Structure, Stress, and Personal Control. In: Zarit Steven H, Pearlin Leonard I, Warner Schaie K., editors. Personal Control in Social and Life Contexts. New York: Springer; 2003. pp. 127–64. [Google Scholar]
- Bearman Peter S, Parigi Paolo. Cloning Headless Frogs and Other Important Matters: Conversation Topics and Network Structure. Social Forces. 2004;83:535–57. [Google Scholar]
- Berkman Lisa F, Glass Thomas, Brissette Ian, Seeman Teresa E. From Social Integration to Health: Durkheim in the New Millennium. Social Science & Medicine. 2000;51:843–57. doi: 10.1016/s0277-9536(00)00065-4. [DOI] [PubMed] [Google Scholar]
- Braun Virginia, Gavey Nicola, McPhillips Kathryn. The ‘Fair Deal’? Unpacking Accounts of Reciprocity in Heterosex. Sexualities. 2003;6:237–61. [Google Scholar]
- Burt Ronald S. Structural Holes: The Social Structure of Competition. Cambridge: Harvard University Press; 1992. [Google Scholar]
- Burt Ronald S. The Gender of Social Capital. Rationality and Society. 1998;10:5–47. [Google Scholar]
- Cattell Vicky. Poor People, Poor Places, and Poor Health: The Mediating Role of Social Networks and Social Capital. Social Science & Medicine. 2001;52:1501–1516. doi: 10.1016/s0277-9536(00)00259-8. [DOI] [PubMed] [Google Scholar]
- Cheng Cliff. Marginalized Masculinities and Hegemonic Masculinity: An Introduction. Journal of Men’s Studies. 1999;7:295–315. [Google Scholar]
- Christakis Nicholas A, Fowler James H. The Spread of Obesity in a Large Social Network over 32 Years. The New England Journal of Medicine. 2007;357:370–379. doi: 10.1056/NEJMsa066082. [DOI] [PubMed] [Google Scholar]
- Connell RW. Gender and Power: Society, the Person and Sexual Politics. Sydney, Australia: George Allen & Unwin; 1987. [Google Scholar]
- Connell RW. Masculinities. Berkeley: University of California Press; 1995. [Google Scholar]
- Connell RW, Messerschmidt James W. Hegemonic Masculinity: Rethinking the Concept. Gender & Society; 2005. [Google Scholar]
- Cornwell Benjamin. Good Health and the Bridging of Structural Holes. Social Networks. 2009a;31:92–103. doi: 10.1016/j.socnet.2008.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornwell Benjamin. Network Bridging Potential in Later Life: Life-Course Experiences and Social Network Position. Journal of Aging and Health. 2009b;21:129–54. doi: 10.1177/0898264308328649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornwell Benjamin, Laumann Edward O, Philip Schumm L. The Social Connectedness of Older Adults: A National Profile. American Sociological Review. 2008;73:185–203. doi: 10.1177/000312240807300201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cornwell Erin York, Waite Linda J. Social Disconnectedness, Perceived Isolation, and Health among Older Adults. Journal of Health and Social Behavior. 2009;50:31–48. doi: 10.1177/002214650905000103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corona Giovanni, Petrone Luisa, Mannucci Edoardo, Magini Angela, Lotti Francesco, Ricca Valdo, Chiarini Valerio, Forti Gianni, Maggi Mario. Assessment of the Relational Factor in Male Patients Consulting for Sexual Dysfunction: The Concept of Couple Sexual Dysfunction. Journal of Andrology. 2006;25:795–801. doi: 10.2164/jandrol.106.000638. [DOI] [PubMed] [Google Scholar]
- Davidson Kate, Daly Tom, Arber Sara. Exploring the Social Worlds of Older Men. In: Arber Sara, Davidson Kate, Ginn Jay., editors. Gender and Ageing: Changing Roles and Relationships. Buckingham: Open University Press; 2003. pp. 168–85. [Google Scholar]
- Dean Robert C, Lue Tom F. Physiology of Penile Erection and Pathophysiology of Erectile Dysfunction. Urologic Clinics of North America. 2005;32:379–95. doi: 10.1016/j.ucl.2005.08.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeLamater John D, Sill Morgan. Sexual Desire in Later Life. Journal of Sex Research. 2005;42:138–49. doi: 10.1080/00224490509552267. [DOI] [PubMed] [Google Scholar]
- Duncombe Jean, Marsden Dennis. Whose Orgasm Is this Anyway? ‘Sex Work’ in Long-term Hetereosexual Relationships. In: Weeks J, Holland J, editors. Sexual Cultures, Communities, Values and Intimacy. London: Macmillan; 1996. pp. 220–38. [Google Scholar]
- Edgar Donald. Men, Mateship, Marriage. Sydney, Australia: HarperCollins; 1997. [Google Scholar]
- Emerson Richard M. Power-Dependence Relations. American Sociological Review. 1962;27:31–41. [Google Scholar]
- Esposito K, Giugliano F, Ciotola M, De Sio M, D’Armiento M, Giugliano D. Obesity and Sexual Dysfunction, Male and Female. International Journal of Impotence Research. 2008;20:358–65. doi: 10.1038/ijir.2008.9. [DOI] [PubMed] [Google Scholar]
- Fernandez Roberto M, Lourdes Sosa M. Gendering the Job: Networks and Recruitment at a Call Center Gendering the Job: Networks and Recruitment at a Call Center. The American Journal of Sociology. 2005;111:859–904. [Google Scholar]
- Fiori Katherine L, Antonucci Toni C, Cortina Kai S. Social Network Typologies and Mental Health among Older Adults. Journals of Gerontology: Psychological Sciences. 2006;61B:25–32. doi: 10.1093/geronb/61.1.p25. [DOI] [PubMed] [Google Scholar]
- Fleiss Joseph L, Williams Janet BW, Dubro Alan F. The Logistic Regression Analysis of Psychiatric Data. Journal of Psychiatric Research. 1986;20:195–209. doi: 10.1016/0022-3956(86)90003-8. [DOI] [PubMed] [Google Scholar]
- Foreman Sally, Dallos Rudi. Inequalities of Power and Sexual Problems. Journal of Family Therapy. 1992;14:349–69. [Google Scholar]
- Freeman Linton C. Centrality in Social Networks: Conceptual Clarification. Social Networks. 1979;1:215–39. [Google Scholar]
- Galliher Renee V, Rostosky Sharon S, Welsh Deborah P, Kawaguchi Myra C. Power and Psychological Well-Being in Late Adolescent Romantic Relationships. Sex Roles. 1999;40:689–710. [Google Scholar]
- Gerstel Naomi, Riessman Catherine Kohler, Rosenfield Sarah. Explaining the Symptomatology of Separated and Divorced Women and Men: The Role of Material Conditions and Social Networks. Social Forces. 1985;64:84–101. [Google Scholar]
- Goldstein Irwin. The Mutually Reinforcing Triad of Depressive Symptoms, Cardiovascular Disease, and Erectile Dysfunction. American Journal of Cardiology. 2000;86(2A):41F–45F. doi: 10.1016/s0002-9149(00)00892-4. [DOI] [PubMed] [Google Scholar]
- Granovetter Mark S. The Strength of Weak Ties. The American Journal of Sociology. 1973;78:1360–380. [Google Scholar]
- Hale Valerie E, Strassberg Donald S. The Role of Anxiety on Sexual Arousal. Archives of Sexual Behavior. 1990;19:569–58. doi: 10.1007/BF01542466. [DOI] [PubMed] [Google Scholar]
- Heckman James J. Sample Selection Bias as a Specification Error. Econometrica. 1979;47:153–61. [Google Scholar]
- House James S, Landis Karl, Umberson Debra. Social Relationships and Health. Science. 1988;241:540–45. doi: 10.1126/science.3399889. [DOI] [PubMed] [Google Scholar]
- Ibarra Herminia. Personal Networks of Women and Minorities in Management: A Conceptual Framework. Academy of Management Review. 1993;18:56–87. [Google Scholar]
- Johnson Michael P, Leslie Leigh. Couple Involvement and Network Structure: A Test of the Dyadic Withdrawal Hypothesis. Social Psychology Quarterly. 1982;45:34–43. [Google Scholar]
- Julien Danielle, Chartrand Elise, Bégin Jean. Social Networks, Structural Interdependence, and Conjugal Adjustment in Heterosexual, Gay, and Lesbian Couples. Journal of Marriage and the Family. 1999;61:516–30. [Google Scholar]
- Kalmijn Matthijs. Shared Friendship Networks and the Life Course: An Analysis of Survey Data on Married and Cohabiting Couples. Social Networks. 2003;25:231–49. [Google Scholar]
- Kalmijn Matthijs, Bernasco Wim. Separated Lifestyles in Married and Cohabiting Relationships. Journal of Marriage and the Family. 2001;63:639–54. [Google Scholar]
- Kimmel Michael S. Changing Men: New Directions in Research on Men and Masculinity. Newbury Park, CA: Sage; 1987. [Google Scholar]
- Krackhardt David. Cognitive Social Structures. Social Networks. 1987;9:109–34. [Google Scholar]
- Krause Neal. Negative Interaction and Heart Disease in Late Life: Exploring Variations by Socioeconomic Status. Journal of Aging and Health. 2005;17:28–55. doi: 10.1177/0898264304272782. [DOI] [PubMed] [Google Scholar]
- Krause Neal. Age and Decline in Role-Specific Feelings of Control. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences. 2007;62:S28–35. doi: 10.1093/geronb/62.1.s28. [DOI] [PubMed] [Google Scholar]
- Kupelian Varant, Shabsigh Ridwan, Travison Thomas G, Page Stephanie T, Araujo Andre B, McKinlay John B. Is There a Relationship Between Sex Hormones and Erectile Dysfunction? Results From the Massachusetts Male Aging Study. Journal of Urology. 2006;176:2584–2588. doi: 10.1016/j.juro.2006.08.020. [DOI] [PubMed] [Google Scholar]
- Laumann Edward O, Das Aniruddha, Waite Linda J. Sexual Dysfunction among Older Adults: Prevalence and Risk Factors from a Nationally Representative U.S. Probability Sample of Men and Women 57–85 Years of Age. Journal of Sexual Medicine. 2008;5:2300–2311. doi: 10.1111/j.1743-6109.2008.00974.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laumann Edward O, Paik Anthony, Glasser Dale B, Kang Jeong-Han, Wang Tianfu, Levinson Bernard, Moreira Edson D, Jr, Nicolosi Alfredo, Gingell Clive. A Cross-National Study of Subjective Sexual Well-Being among Older Women and Men: Findings From the Global Study of Sexual Attitudes and Behaviors. Archives of Sexual Behavior. 2006;35:143–59. doi: 10.1007/s10508-005-9005-3. [DOI] [PubMed] [Google Scholar]
- Laumann Edward O, Paik Anthony, Rosen Raymond C. Sexual Dysfunction in the U.S.: Prevalence and Predictors. Journal of the American Medical Association. 1999;281:537–44. doi: 10.1001/jama.281.6.537. [DOI] [PubMed] [Google Scholar]
- Laumann Edward O, West Suzanne, Glasser Dale, Carson Culley, Rosen Raymond, Kang Jeong-han. Prevalence and Correlates of Erectile Dysfunction by Race and Ethnicity among Men Aged 40 or Older in the United States: From the Male Attitudes Regarding Sexual Health Survey. Journal of Sexual Medicine. 2007;4:57–65. doi: 10.1111/j.1743-6109.2006.00340.x. [DOI] [PubMed] [Google Scholar]
- Laumann Edward O, Youm Yoosik. Racial/Ethnic Group Differences in the Prevalence of Sexually Transmitted Diseases in the United States: A Network Explanation. Sexually Transmitted Diseases. 1999;26:250–61. doi: 10.1097/00007435-199905000-00003. [DOI] [PubMed] [Google Scholar]
- Lee Christina, Glynn Owens R. The Psychology of Men’s Health. Philadelphia, PA: Open University Press; 2002. [Google Scholar]
- Leiblum Sandra R, Rosen Raymond C. Couples Therapy for Erectile Disorder: Conceptual and Clinical Considerations. Journal of Sex & Marital Therapy. 1991;17:147–59. doi: 10.1080/00926239108404956. [DOI] [PubMed] [Google Scholar]
- Lin Nan. Social Capital: A Theory of Social Structure and Action. Cambridge: Cambridge University Press; 2001. [Google Scholar]
- Lindau, Stacy Tessler L, Schumm Philip, Laumann Edward O, Levinson Wendy, O’Muircheartaigh Colm A, Waite Linda J. A Study of Sexuality and Health among Older Adults in the United States. The New England Journal of Medicine. 2007;357(8):22–34. doi: 10.1056/NEJMoa067423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mann Robin. Out of the Shadows?: Grandfatherhood, Age and Masculinities. Journal of Aging Studies. 2007;21:281–91. [Google Scholar]
- Mansfield Abigail K, Addis Michael E, Mahalik James R. Why Won’t He Go to the Doctor?: The Psychology of Men’s Help Seeking. International Journal of Men’s Health. 2003;22:93–109. [Google Scholar]
- Marin Alexandra. Are Respondents More Likely to List Alters with Certain Characteristics? Implications for Name Generator Data. Social Networks. 2004;26:289–307. [Google Scholar]
- Marsden Peter V. Core Discussion Networks of Americans. American Sociological Review. 1987;52:122–31. [Google Scholar]
- Martin John Levi. Is Power Sexy? American Journal of Sociology. 2005;111:408–46. [Google Scholar]
- Martino Wayne, Pallotta-Chiarolli Maria. ‘So What’s a Boy?’ Addressing Issues of Masculinity in Schooling. London: Open University Press; 2003. [Google Scholar]
- Masters William H, Johnson Virginia E. Human Sexual Response. Boston: Little, Brown, and Company; 1966. [Google Scholar]
- McCabe Marita P. Relationship Factors in the Development and Maintenance of ED: Implications for Treatment Effectiveness. Journal of Sexual Medicine. 2008;5:1795–1804. doi: 10.1111/j.1743-6109.2008.00878.x. [DOI] [PubMed] [Google Scholar]
- McCabe Marita P, Cobain Marilyn J. The Impact of Individual and Relationship Factors on Sexual Dysfunction among Men and Females. Sexual and Marital Therapy. 1998;3:131–43. [Google Scholar]
- McGuire Gail M. Gender, Race, Ethnicity, and Networks. Work and Occupations. 2000;27:500–23. [Google Scholar]
- McPherson J Miller, Smith-Lovin Lynn, Cook James M. Birds of a Feather: Homophily in Social Networks. Annual Review of Sociology. 2001;27:415–44. [Google Scholar]
- McVary Kevin T. Erectile Dysfunction. The New England Journal of Medicine. 2007;357:2472–481. doi: 10.1056/NEJMcp067261. [DOI] [PubMed] [Google Scholar]
- Milardo Robert M. Friendship Networks in Developing Relationships: Converging and Diverging Social Environments. Social Psychological Quarterly. 1982;45:162–72. [Google Scholar]
- Mirowsky John. Age and Sense of Control. Social Psychology Quarterly. 1995;58:31–43. [Google Scholar]
- Moore Gwen. Structural Determinants of Men's and Women's Personal Networks. American Sociological Review. 1990;55:726–35. [Google Scholar]
- Morgan Stephen L, Todd Jennifer J. A Diagnostic Routine for the Detection of Consequential Heterogeneity of Causal Effects. Sociological Methodology. 2008;38:231–81. [Google Scholar]
- Moss Sidney Z, Moss Miriam S. Being a Man in Long Term Care. Journal of Aging Studies. 2007;21:43–54. [Google Scholar]
- Oliffe John. Constructions of Masculinity Following Prostatectomy-Induced Impotence. Social Science & Medicine. 2005;60:2249–2259. doi: 10.1016/j.socscimed.2004.10.016. [DOI] [PubMed] [Google Scholar]
- Pfeiffer E. A Short Portable Mental Status Questionnaire for the Assessment of Organic Brain Deficit in Elderly Patients. Journal of the American Geriatrics Society. 1975;23:433–41. doi: 10.1111/j.1532-5415.1975.tb00927.x. [DOI] [PubMed] [Google Scholar]
- Pinquart Martin, Sörensen Silvia. Gender Differences in Caregiver Stressors, Social Resources, and Health: An Updated Meta-Analysis. The Journals of Gerontology Series B: Psychological Sciences. 2006;61B:33–45. doi: 10.1093/geronb/61.1.p33. [DOI] [PubMed] [Google Scholar]
- Ponholzer Anton, Temml Christian, Obermayr Rudolf, Madersbacher Stephan. Association between Lower Urinary Tract Symptoms and Erectile Dysfunction. Urology. 2004;64:772–76. doi: 10.1016/j.urology.2004.05.025. [DOI] [PubMed] [Google Scholar]
- Popielarz Pamela A. (In) Voluntary Association: A Multilevel Analysis of Gender Segregation in Voluntary Organizations. Gender and Society. 1999;13:234–50. [Google Scholar]
- Pugliesi Karen, Shook Scott L. Gender, Ethnicity, and Network Characteristics: Variations in Social Support Resources. Sex Roles. 1998;38:215–38. [Google Scholar]
- Qato Dima, Lindau Stacy Tessler, Philip Schumm L, Johnson Michael. Medication Data Collection and Coding in a Home-Based Survey of Older Adults. Journal of Gerontology: Social Sciences. 2009 doi: 10.1093/geronb/gbp036. forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Renzulli Linda A, Aldrich Howard, Moody James. Family Matters: Gender, Networks, and Entrepreneurial Outcomes. Social Forces. 2000;79:523–46. [Google Scholar]
- Ribeiro Oscar, Paúl Constança, Nogueira Conceição. Real Men, Real Husbands: Caregiving and Masculinities in Later Life. Journal of Aging Studies. 2007;21:302–13. [Google Scholar]
- Ridgeway Cecilia L. Interaction and the Conservation of Gender Inequality: Considering Employment. American Sociological Review. 1997;62:218–35. [Google Scholar]
- Ridgeway Cecilia L, Smith-Lovin Lynn. The Gender System and Interaction. Annual Review of Sociology. 1999;25:191–216. [Google Scholar]
- Riska Elianne. From Type A Man to the Hardy Man: Masculinity and Health. Sociology of Health & Illness. 2002;24:347–58. [Google Scholar]
- Rook Karen S. The Negative Side of Social Interaction: Impact on Psychological Well-Being. Journal of Personality and Social Psychology. 1984;46:1097–1108. doi: 10.1037//0022-3514.46.5.1097. [DOI] [PubMed] [Google Scholar]
- Rosen Raymond C. Psychogenic Erectile Dysfunction. Classification and Management. Urologic Clinics of North America. 2001;28:269–78. doi: 10.1016/s0094-0143(05)70137-3. [DOI] [PubMed] [Google Scholar]
- Rotolo Thomas, Wilson John. Sex Segregation in Volunteer Work. Sociological Quarterly. 2007;48:559–85. [Google Scholar]
- Ruan Danching. The Content of the General Social Survey Discussion Networks: An Exploration of the General Social Survey Discussion Name Generator in a Chinese Context. Social Networks. 1998;20:247–26. [Google Scholar]
- Sand Michael S, Fisher William, Rosen Raymond, Heiman Julia, Eardley Ian. Erectile Dysfunction and Constructs of Masculinity and Quality of Life in the Multinational Men’s Attitudes to Life Events and Sexuality (MALES) Study. Journal of Sexual Medicine. 2008;5:583–94. doi: 10.1111/j.1743-6109.2007.00720.x. [DOI] [PubMed] [Google Scholar]
- Silverstein Merril, Chen Xuan, Heller Kenneth. Too Much of a Good Thing? Intergenerational Social Support and the Psychological Well-Being of Older Parents. Journal of Marriage and the Family. 1996;58:970–82. [Google Scholar]
- Smith James A, Braunack-Mayer Annette, Wittert Gary, Warin Megan. ‘I’ve Been Independent for So Damn Long!’: Independence, Masculinity and Aging in a Help Seeking Context. Journal of Aging Studies. 2007;21:325–35. [Google Scholar]
- Smith Kirsten P, Christakis Nicholas A. Social Networks and Health. Annual Review of Sociology. 2008;34:405–29. [Google Scholar]
- Smith-Lovin Lynn, McPherson Miller. You Are Who You Know: A Network Perspective on Gender. In: England Paula., editor. Theory on Gender/Feminism on Theory. New York: Aldine; 1993. pp. 223–41. [Google Scholar]
- Spanier Graham B. Measuring Dyadic Adjustment: New Scales for Assessing the Quality of Marriage and Similar Dyads. Journal of Marriage and Family. 1976;38:15–28. [Google Scholar]
- Stein Catherine H, Bush Ellen G, Ross Ronald R, Ward Marcia. Mine, Yours, and Ours: A Configural Analysis of the Networks of Married Couples in Relation to Marital Satisfaction and Individual Well-being. Journal of Social and Personal Relationships. 1992;9:365–83. [Google Scholar]
- Stephenson Peter H, Wolfe Nuala K, Coughlan Rory, Koehn Sharon D. A Methodological Discourse on Gender, Independence, and Frailty: Applied Dimensions of Identity Construction in Old Age. Journal of Aging Studies. 1999;13:391–401. [Google Scholar]
- Stoller Eleanor Palo, Pugliesi Karen L. Size and Effectiveness of Informal Helping Networks: A Panel Study of Older People in the Community. Journal of Health and Social Behavior. 1991;32:180–91. [PubMed] [Google Scholar]
- Thoits Peggy. Stress, Coping, and Social Support Processes: Where Are We? What Next? Journal of Health and Social Behavior. 1995;35:53–79. [PubMed] [Google Scholar]
- Umberson Debra. Family Status and Health Behaviors: Social Control as a Dimension of Social Integration. Journal of Health and Social Behavior. 1987;28:306–19. [PubMed] [Google Scholar]
- van Emmerik IJ Hetty. Gender Differences in the Creation of Different Types of Social Capital: A Multilevel Study. Social Networks. 2006;28:24–37. [Google Scholar]
- Van Minnen A, Kampman M. The Interaction between Anxiety and Sexual Functioning: A Controlled Study of Sexual Functioning in Women with Anxiety Disorders. Sexual & Relationship Therapy. 2000;15:47–57. [Google Scholar]
- Wagner John D, Flinn Mark V, England Barry G. Hormonal Response to Competition among Male Coalitions. Evolution and Human Behavior. 2002;23:437–42. [Google Scholar]
- Waldrop Deborah P, Weber Joseph A, Herald Shondel L, Pruett Julie, Cooper Kathy, Juozapavicius Kevin. Wisdom and Life Experiences: How Grandfathers Mentor Their Grandchildren. Journal of Aging and Identity. 1999;4:33–46. [Google Scholar]
- Wellman Barry, Wortley Scot. Different Strokes from Different Folks: Community Ties and Social Support. The American Journal of Sociology. 1990;96:558–88. [Google Scholar]
- West Candace, Zimmerman Don H. Doing Gender. Gender and Society. 1987;1:125–51. [Google Scholar]
- Youm Yoosik, Laumann Edward O. The Effect of Structural Embeddedness on the Division of Household Labor: A Game-Theoretic Model with a Network Approach. Rationality and Society. 2003;15:243–80. [Google Scholar]
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica. 1983;67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- Zilbergeld Bernie. The New Male Sexuality. New York: Bantam Books; 1992. [Google Scholar]