

Abstract
Background/Aims
The widespread use of cytotoxic chemotherapy and immunosuppressants has resulted in reactivation of hepatitis B virus (HBV) recently becoming an issue. Although rituximab (an anti-CD20 monoclonal antibody) has revolutionized the treatment of lymphoma, recent reports have suggested that rituximab therapy increases the risk of viral-mediated complications, and particularly HBV reactivation. This study analyzed real clinical practice data for rituximab-related HBV reactivation.
Methods
Between January 2005 and December 2011, 169 patients received treatment with rituximab. Screening status of the HBV infection and frequency of preemptive therapy were determined in these patients, and the clinical features of HBV reactivation were analyzed.
Results
Seventy-nine of the 169 patients with chronic or past HBV infection were selected for evaluation of HBV reactivation. Of the 90 patients who were excluded, 22 (13.0%) were not assessed for HBsAg and anti-HBc, and 14 (8.3%) were not assessed for anti-HBc due to seronegativity for HBsAg. The selected patients were divided into those with chronic HBV infection (n=12) and those with past HBV infection (n=67); six patients (7.6%) experienced HBV reactivation. Eight patients received preemptive therapy, but three patients (37.5%) underwent HBV reactivation. Although HBsAg seropositivity was an independent risk factor for HBV reactivation (P=0.038), of the six patients with HBV reactivation, two (33.3%) had past HBV infection and three (50%) died of liver failure.
Conclusions
The findings of this study demonstrate that adherence to guidelines for screening and preemptive therapy for HBV reactivation was negligent among the included cohort. Attention should be paid to HBV reactivation in patients with past as well as chronic HBV infection during and after rituximab therapy.
Keywords: Hepatitis B virus, Immunosuppressant, Rituximab
INTRODUCTION
Although vaccination for the prevention of hepatitis B virus (HBV) infection has been effectively used for over 25 years, HBV infection is still one of the most important and fatal infectious liver diseases, with approximately 400 million chronically infected people worldwide.1 The prevalence of chronic HBV infection in developed countries such as Western Europe and the USA is currently less than 1-2%, however in Asia, Africa, and some Mediterranean countries, the prevalence exceeds as high as 10%. Above all, in these high prevalence areas, past or remote HBV infection as well as overt HBV infection may cause serious health problems.
Recently, with wide-spread use of cytotoxic chemotherapy or immunosuppressants such as high-dose corticosteroids and biologic agents, reactivation of HBV is becoming an issue. Because the goal of newly invented drugs is mostly to control human immune system, this issue becomes more important. In particular, rituximab is a human/murine chimeric monoclonal antibody directed against the CD20 antigen expressed on the surface of normal and malignant B lymphocytes. It was approved by the U.S. Food and Drug Administration (FDA) in 2006, primarily for the treatment of B-cell malignancies such as non-Hodgkin's lymphomas.2 Since then, its use has expanded to the treatment of many other diseases, including rheumatoid arthritis, systemic lupus erythematosis, idiopathic thrombocytopenic purpura, autoimmune hemolytic anemia, Sjogren's syndrome, multiple sclerosis, graft vs. host disease, autoimmune hepatitis, and dermatomyositis.3
Several reports have suggested that rituximab therapy may increase the risk of viral-mediated complications, particularly HBV reactivation. HBV reactivation associated with rituximab therapy is usually subclinical, however, frequently it can result in the development of severe complications, including acute liver failure and death. In October 2004, the U.S. FDA reported that the use of rituximab might be associated with episodes of fulminant hepatitis.4 In endemic areas such as Korea, Taiwan and China, there are many patients with current or past HBV infection. Therefore, reactivation of HBV induced by rituximab therapy can be a serious clinical problem in these areas. The aim of this study was to inquire the actual condition of preparation for HBV reactivation prior to rituximab therapy in clinical practice, and to investigate clinical features and risk factors for HBV reactivation during or after rituximab-based therapy at a single tertiary institute in an area with a high prevalence of HBV infection.
MATERIALS AND METHODS
From January 2005 to December 2011, a total of 169 patients received treatment with rituximab at Yeungnam University hospital. The subjects for this study were selected regardless of treatment departments. All medical records were retrospectively reviewed. Of 169 patients, 79 patients with chronic HBV infection or past HBV infection were selected for evaluation of HBV reactivation in this study. The demographic characteristics of the patients, the incidence of HBV reactivation and its risk factors in association with rituximab therapy were analyzed. Assessments of the frequency and results for hepatitis B surface antigen (HBsAg), antibody to HBsAg (anti-HBs), hepatitis B e antigen (HBeAg), antibody to HBeAg (anti-HBe), antibodies to hepatitis B core (anti-HBc), serum alanine aminotransferase (ALT), albumin, total bilirubin, alkaline phosphatase (ALP), lactate dehydrogenase (LDH), prothrombin time (PT), white blood cell, hemoglobin, platelet and HBV DNA polymerase chain reaction (PCR) were performed for all patients before or during rituximab therapy. The HBV DNA load was measured by quantitative real-time PCR assay (Cobas Taqman HBV-DNA Test, Roche Diagnostics Systems, CA, USA) with a minimal sensitivity of 20 IU/mL. Measurement of HBsAg, anti-HBs, anti-HBc, HBeAg, and anti-HBe was performed using commercially available enzyme immunoassays (Architect i2000SR, Abbott Diagnostics, IL, USA). We calculated the total dose and the mean dose per cycle of rituximab. This study was conducted in accordance with the Helsinki Declaration. The medical ethical committee of our medical center approved the study protocol.
Definition
HBV reactivation and hepatitis were defined as follows. HBV reactivation was defined as reappearance or an increase in serum HBV DNA over 10 folds (1 log10 IU/mL), compared with the pretreatment level. Hepatitis was defined as a threefold or greater increase in serum ALT level that exceeded 120 IU/L (reference range, <40 IU/L). Chronic HBV infection was defined as HBsAg seropositivity over a period of six months, irrespective of HBeAg and HBV DNA seropositivity, including chronic inactive carriers. Past or resolved HBV infection was defined as HBsAg and HBV DNA seronegative, anti-HBc seropositive, and/or anti-HBs seropositive. Liver cirrhosis was defined by histologic, clinical or radiological evidence. Clinical signs of liver cirrhosis included lower platelet count (<1.4×105 cell/µL), the existence of varix, or the development of ascites. Patients with fever or hypothermia, leukocytosis or leukopenia, tachypnea, or tachycardia, with a proven or suspected infectious condition, were regarded as having sepsis. Preemptive antiviral therapy was defined as the administration of an antiviral agent prior to the start of rituximab therapy.
Statistical analysis
Quantitative data were presented as the mean value ± standard deviation (range). The independent-samples t test was used if parametric assumptions were met for numerical data. Mann-Whitney U test was used when parametric assumptions were not met. For categorical measures, Pearson χ2 or Fisher's exact tests were used for non-continuous variables. Univariate analysis was performed on significant variables. The binary logistic regression model was used to identify independent risk factors. A P-value of less than 0.05 was considered statistically significant. PASW statistics version 18.0 for Windows (SPSS Inc., Chicago, Illinois, USA) and Microsoft Excel 2007 (Microsoft corp., Redmond, Washington, USA) were used for analysis of all data.
RESULTS
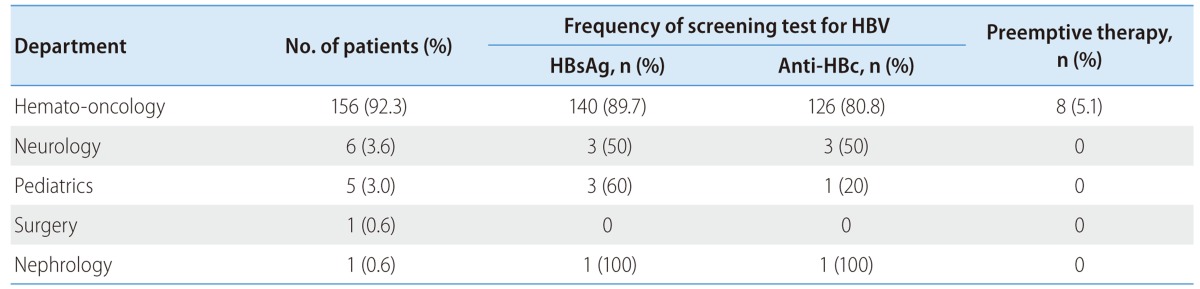
The patients who received rituximab therapy included 101 men and 68 women, with the mean (±standard deviation) age of 61.8 (±18.1 years). The baseline characteristics of all patients received rituximab therapy are shown in Table 1. Rituximab was administered to patients in the department of hemato-oncology (156/169, 92.3%), neurology (6/169, 3.6%), pediatrics (5/169, 3.0%), general surgery (1/169, 0.6%) and nephrology (1/169, 0.6%) (Table 2). In the department of hemato-oncology, the serologic test for current HBV infection or HBsAg prior to rituximab therapy was not performed in even 16 patients (10.3%). The rate of assessment for serology of HBsAg in department of neurology and pediatrics was 50% (3/6) and 60% (3/5), respectively. Rituximab was used in the treatment of diffuse large B cell lymphoma (139/169, 82.2%) and other lymphomas (18/169, 10.7%). The remaining 12 cases included acute graft rejection, neuromyelitis optica, multiple sclerosis, graft vs. host disease, immune thrombocytopenic purpura, and aplastic anemia. Hepatitis developed after rituximab therapy in thirty five patients (35/169, 20.7%). The most common cause of hepatitis was unknown etiology (57.1%). The remaining causes included sepsis (22.9%), HBV reactivation (17.1%), hepatitis A virus (2.9%) and so on.
Table 1.
Baseline characteristics of patients who received rituximab-based therapy

Table 2.
Comparative screening analysis for HBV serology and preemptive therapy according to treatment department
Of 169 patients, ninety patients were excluded from this study based on HBV serology results; 54 patients didn't have a history of HBV infection; 22 patients (13.0%) were not assessed for HBsAg and anti-HBc; 14 patients (8.3%) were not assessed for anti-HBc due to seronegativity for HBsAg (Fig. 1). The rest of 79 patients were divided into two groups, a group with chronic HBV infection (n=12) and a group with past HBV infection (n=67). Baseline characteristics and clinical features of 79 patients with HBV infection are shown in Table 3. None of the patients had co-infection with both HBV and HCV. Of 79 patients, six patients were confirmed to have developed HBV reactivation by the definition mentioned above (6/79, 7.6%). There were two patients with past HBV infection in a total of six patients with HBV reactivation (2/6, 33.3%). All six patients with HBV reactivation had undergone treatment for diffuse large B cell lymphoma. These six patients received intravenous rituximab therapy along with cyclophosphamide, doxorubicin, vincristine and prednisolone as an R-CHOP regimen.
Figure 1.

Flow chart of the enrolled patients.
Table 3.
Baseline characteristics and clinical features of patients with chronic or past HBV infection

*Baseline test.
ALT, alanine aminotransferase; PT, prothrombin time.
Based on the definition of HBV reactivation, the subjects were divided into two groups: a patient group (n=6) with HBV reactivation and a patient group (n=73) without HBV reactivation. Assessments of baseline characteristics, seropositive viral markers of HBV infection, and baseline liver function for both groups were performed. There was a significant difference in the seropositivity for HBsAg, HBeAg, and HBV DNA between two groups (P<0.05). There were also statistical difference in age, the total dose of rituximab, the total number of therapy cycles, baseline hemoglobin level and albumin level between two groups P<0.05). The major comparative analyses of both groups are shown in Table 4. The mean interval from the initial administration of rituximab to HBV reactivation was approximately 47.0±19.3 (24-70) weeks, and the mean interval from the last administration of rituximab in a cycle to HBV reactivation was approximately 24.3±20.6 (0-46) weeks. The mean durations of rituximab administration of each group were not significantly different one another (22.3 weeks vs. 18.8 weeks; P=0.102). Of six patients with HBV reactivation, five patients (5/6, 83.3%) were treated with antiviral rescue therapy and the remaining patient did not receive specific treatment. Among those six patients, three patients (3/6, 50.0%) died of hepatic failure, and the other three patients survived (Table 5).
Table 4.
Comparative analysis of patients with HBV reactivation vs. without HBV reactivation
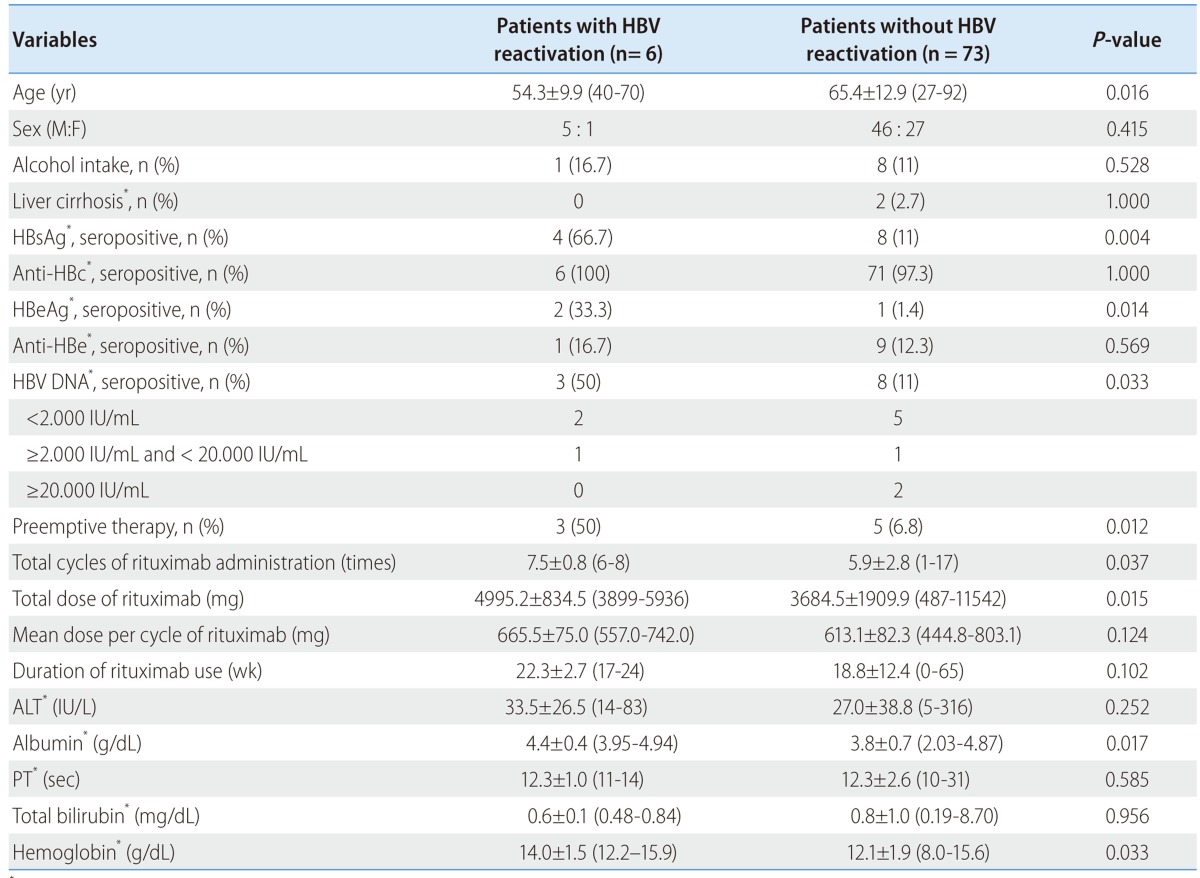
*Baseline test.
ALT, alanine aminotransferase; PT, prothrombin time.
Table 5.
Clinical features of six patients with HBV reactivation secondary to rituximab therapy
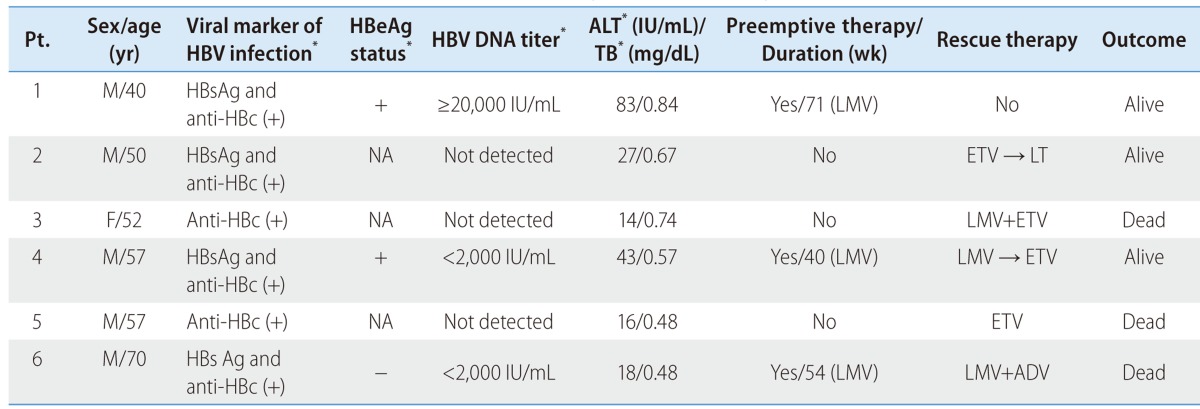
*Baseline test.
Pt., patient; M, male; F, female; ALT, alanine aminotransferase; TB, total bilirubin; NA, not available; LMV, lamivudine; ETV, entacavir; ADV, adefovir; LT, liver transplantation.
Among 79 patients with HBsAg seropositive status or anti-HBc seropositive status, preemptive antiviral therapy was administered to only eight patients (8/79, 10.1%). All these eight patients were HBsAg seropositive. Lamivudine was administered to seven patients (87.5%) and clevudine was administered to one patient (12.5%) for preemptive therapy. The mean duration of preemptive therapy was 38.0±22.8 weeks. However, three of them (3/8, 37.5%) experienced HBV reactivation. The mean duration of preemptive therapy of these patients with reactivation was 55.0±15.5 weeks. All these three patients received preemptive treatment with lamivudine and experienced HBV reactivation under preemptive therapy.
For detection of risk factors for rituximab-related HBV reactivation, univariate analyses were performed on factors associated with occurrence of HBV reactivation. Univariate analyses revealed that seropositivity for HBsAg and HBeAg were statistically significant (P=0.019, and P=0.008) but seropositivity for HBV DNA, patient's age, the total dose of rituximab, the total cycles of rituximab therapy, baseline hemoglobin level and albumin level were not statistically significant (P>0.05) (Table 6). A binary logistic regression analysis was performed to identify independent risk factors for HBV reactivation. The result revealed that seropositivity for HBsAg (OR, 9.286; 95% CI, 1.127-76.541, P=0.038) was the only independent risk factor for HBV reactivation (Table 7).
Table 6.
Univariate analysis for significant factors of patients with or without HBV reactivation
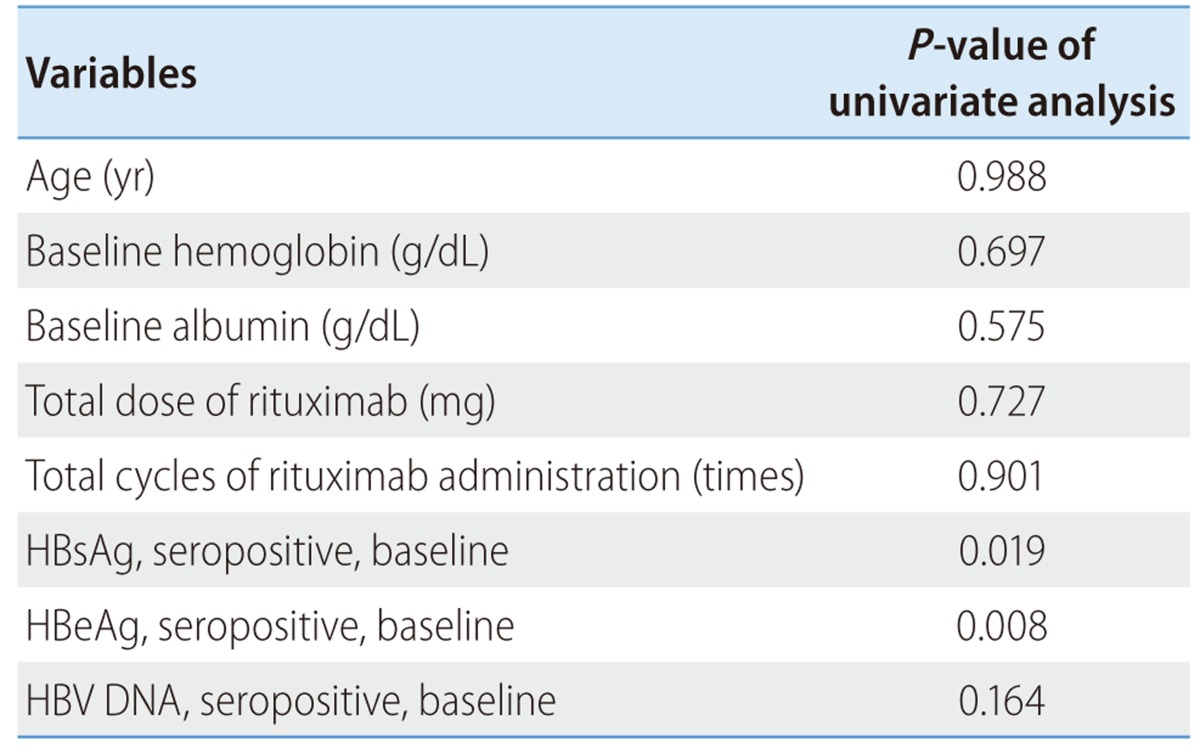
Table 7.
Binary logistic regression analysis for factors related to HBV reactivation induced by rituximab therapy

DISCUSSION
Though many guidelines established in the Europe, US, and Asia-Pacific including Korea have already warned risk of HBV reactivation, and recommended preemptive therapy associated with immunosuppressants therapy, in particular rituximab, there is still a lack of awareness among clinicians regarding cytotoxic agents and immunosuppressant-induced HBV reactivation. Even in tertiary care institutions, the assessment of hepatitis B serologies prior to the administration of rituximab-based therapy is infrequently conducted and the frequency of preemptive therapy and HBV reactivation rates are unclear. In our study, it was found that assessments of viral markers for chronic HBV infection or assessment of past HBV infection were not performed in 22 patients (13%). Even hemato-oncologists failed to perform the baseline assessment of viral markers for overt hepatitis B virus infection (HBsAg) in 16 patients (16/156, 10.3%). Neurologists administered rituximab to six patients to treat neuromyelitis optica and multiple sclerosis. Of these six patients, three patients (3/6, 50%) were not assessed for viral markers of HBV infection and none of the patients were assessed for liver function. Despite the use of a lower dosage of rituximab in department of pediatrics, pediatricians also neither check the viral markers (2/5, 40%) nor perform liver function test. In our study, rituximab was mostly administered to patients with hematologic diseases or lymphoma. Thus, complete blood cell counts including hemoglobin and lactate dehydrogenase level were selected for analysis to investigate association between immunologic status or disease progression and HBV reactivation. Unexpectedly, baseline hemoglobin levels of patients with HBV reactivation were higher than those of patients without HBV reactivation (14.0 vs. 12.1 g/dL). Among analyzed parameters, only baseline hemoglobin level differed statistically, but there was no relation between baseline hemoglobin level and HBV reactivation at univariate analysis.
It has been reported that both patients with past HBV infection and patients with chronic HBV infection are at high risk of HBV reactivation.5 Lee et al reported that one third of the world's population has serologic evidence of previous hepatitis B infection (hepatitis B core antibodies).6 A recent report suggested that at least one-half of the population has prior exposure to HBV infection in endemic area such as Hong Kong.7 East Asian countries including Korea, Taiwan and China, are areas of high prevalence. Therefore, the incidence of past HBV infection is estimated to be between one third and one-half of the world population. In this study, there were two patients with past HBV infection in a total of six patients with HBV reactivation (33.3%). It was thought that Patient No. 3 and No. 5 (shown in Table 5) were ones with past HBV infection prior to the therapy and underwent the seroreversion, the change from HBsAg seronegative status to seropositive status due to HBV reactivation. However, there is no agreed guideline regarding preemptive antiviral therapy for patients with past HBV infection. The most recent European and US guidelines recommend close monitoring of HBV DNA during rituximab therapy and initiation of antiviral therapy if HBV DNA is positive or at low level,8,9 which implies the existence and importance of HBV carrier with a low HBV DNA level. In this study, all baseline HBV DNA levels of patients experienced HBV reactivation with a history of past HBV infection were not detected. The reason may be related to the system used for HBV DNA detection in this study was able to detect only a value of HBV DNA over 20 IU/mL correctly. Therefore, special attention should be paid to the detection of an HBV DNA carrier with lower HBV DNA level.
The HBV reactivation rate in patients with chronic or past HBV infection was 7.6% (6/79) in our study. The reported HBV reactivation rates of patients with inactive carriers or patients with past HBV infection who underwent immunosuppressive chemotherapy in other studies widely ranged from 16.3 to 55%.10-13 The reason for the lower incidence of HBV reactivation in this study may be explained by unknown origin hepatitis and hepatic failure. Among 20 patients with unknown origin of hepatitis, eight patients were HBsAg or anti-HBc seropositive (40%). Despite these eight patients had the elevated liver enzymes, seropositivity for HBV DNA was not evaluated for them. Of those eight patients, two patients died of fulminant hepatitis and hepatic failure with ALT values greater than 2,000 IU/mL. Despite of the absence of data on HBV DNA, it was possible to infer the occurrence of HBV reactivation. There was a 69-year-old male patient who was found to be HBsAg seronegative and was subsequently excluded from anti-HBc serology. His ALT and total bilirubin were elevated to 49 IU/L and 3.64 mg/dL after 2.5 years of withdrawal of rituximab therapy and HBV serology tests were subsequently performed. The results showed seropositivity for HBsAg and anti-HBc and HBV DNA was greater than 107 IU/ml. It was estimated that the patient underwent HBV reactivation due to rituximab therapy resulting in the seroreversion of HBsAg. This patient was excluded from our study because serology of anti-HBc had not been checked. If all these cases had been considered, HBV reactivation rate of this study would have been noted between 11.3 and 18.8%.
In the present study, the mean intervals from the last administration of rituximab to the occurrence of hepatitis and the reactivation of HBV were 20 weeks, and 24 weeks, respectively. In some studies, it has been suggested that HBV DNA titers begin to rise before 2-3 weeks of elevation of liver enzymes and decrease down to an undetectable level.4,10 It is thought that the difference in the reported duration of this change is owing to infrequent assessment of HBV DNA levels. In general, clinicians failed to routinely assess HBV DNA levels for patients with chronic or past HBV infection. They only tested HBV DNA levels for the differential diagnosis of hepatitis.
In our study, of eight patients who received preemptive therapy, three patients experienced reactivation of HBV. The reactivation of HBV was occurred in the course of preemptive therapy as lamivudine. The mean duration of preemptive therapy of patients with reactivation was 55 weeks. Long-term preemptive therapy might have an influence on emergence of lamivudine-resistant mutation. Thus, we had no choice but to doubt association between development of HBV reactivation and lamivudine-resistant mutation. However, unfortunately, there were no patients who had undergone assessment for lamivudine resistance. The optimal duration of preemptive treatment for patients with HBV reactivation remains uncertain. The general recommendation is that preemptive therapy should be continued for a period of at least 3 months (range, 3-6 months) after the withdrawal of immunosuppresants.8,9,14 However, the authors propose that the preemptive therapy should be at least 12 months or longer after the withdrawal of rituximab therapy because HBV reactivation occurs between 0-46 weeks after the cessation of rituximab therapy (the mean duration: 24 weeks). This proposal is corresponding to recommendations in other studies. A longer period of preemptive therapy (>12 months) has been also suggested in some previous studies because patients receiving monoclonal antibodies such as rituximab or alemtuzumab make a slow recovery until their immunity is reinforced.4,15,16 Considering the possibility of emergence of lamivudine-resistance and necessity of long-term preemptive therapy during or after rituximab therapy, new antiviral agent such as entecavir and tenofovir will be able to become an alternative.
In the present study, of six patients with HBV reactivation, three patients (50.0%) died of hepatic decompensation resulting from HBV reactivation. Above all, patient No. 6 (shown in Table 5) received preemptive therapy as lamivudine, and rescue therapy with combination of lamivudine and adefovir. The patient was diagnosed as a hepatitis B carrier 10 years ago, and regularly checked for HBV serology and liver function without specific antiviral therapy. However, the patient died of hepatic failure by rituximab-induced HBV reactivation, pneumonia and renal failure at the time of admission 109 days. The mortality rate of cancer patients with viral reactivation is reported to vary from 3.7 to 71.4%.17-20 In general, the mortality rate is higher than overall liver-related mortality.21 In addition, most cases of rituximab-related HBV reactivation found in literature are severe or fatal cases.22-24 Hui et al investigated the association between intrahepatic covalently closed circular DNA (cccDNA) and HBV reactivation after chemotherapy.25 Levels of intrahepatic viral cccDNA of patients with HBV reactivation was significantly higher than those of patients without HBV reactivation. Severity of hepatocyte destruction was related to the viral load in liver, and intrahepatic cccDNA was identified as a key inducer increasing viral load. Thus, it was estimated that the increase of intrahepatic viral cccDNA in patients with HBV DNA reactivation might have a strong influence on more severe hepatic failure.
In this study, rituximab was administered along with corticosteroids to all subjects. Both corticosteroids and rituximab affect viral replication and the anti-HBV immune response of a host.26 Among immnosuppressants, corticosteroids have the unique ability to directly enhance HBV replication by binding to specific receptors in the viral genome (Glucocorticoid Responsive Element, GRE). Suzuki et al reported about the impact of mutations in the GRE region of HBV DNA on the response of glucocorticoid and a relationship between viral replication and mutations in the GRE region.27 Yeo et al reported that a high dose of corticosteroids in chemotherapeutic regimens was associated with an increased risk for HBV reactivation.4 Hence, further studies regarding the risk of HBV reactivation during or after rituximab single therapy and the combined therapy of rituximab and corticosteroids will be required in the future.
There are two limitations which need to be acknowledged and addressed regarding this study. The first limitation is that twenty patients (20/169, 11.8%) received only single rituximab therapy. Of these 20 patients, 10 patients (50%) had a history of chronic or past HBV infection but none of the patients experienced either HBV reactivation or hepatitis. The mean dose of rituximab used in those 20 patients was no more than 560.6±72.1 mg. The other limitation is the inability to determine the true number of patients who were actually positive for HBsAg due to the existence of unscreened patients resulting in the failure to establish a true reactivation rate. Although the HBV reactivation rate of this study might have been underestimated, the identification of six HBV reactivation cases including three deaths is significant.
In conclusion, the results of this study have demonstrated the lack of compliance with guidelines on HBV screening and preemptive therapy for patients undergoing rituximab-based therapy. Efforts should be made to screen all patients undergoing rituximab therapy for HBV infection and to administer preemptive antiviral therapy to patients with HBsAg seropositivity. In patients with past HBV infection (anti-HBc, seropositive), regular assessments of HBV serology, HBV DNA level, and liver biochemical tests are essential and should be performed during or after rituximab therapy. Also, trials to detect low level HBV DNA carriers are required. It is suggested that administration of preemptive antiviral therapy should be conducted at least for a period of 12 months after the cessation of rituximab. Further well-designed studies on risk factors for HBV reactivation induced by rituximab will be required in the future.
Abbreviations
- HBV
hepatitis B virus
- FDA
Food and Drug Administration
- HBsAg
hepatitis B surface antigen
- anti-HBs
antibody to HBsAg
- HBeAg
hepatitis B e antigen
- anti-HBe
antibody to HBeAg
- anti-HBc
antibody to hepatitis B core
- ALT
alanine aminotransferase
- ALP
alkaline phosphatase
- LDH
lactate dehydrogenase
- PT
prothrombin time
- PCR
polymerase chain reaction
- HCV
hepatitis C virus
- OR
odds ratio
- CI
confidence interval
- cccDNA
covalently closed circular DNA
- GRE
glucocorticoid responsive element
Footnotes
The authors have no conflicts to disclose.
References
- 1.Lai CL, Yuen MF. Chronic hepatitis B--new goals, new treatment. N Engl J Med. 2008;359:2488–2491. doi: 10.1056/NEJMe0808185. [DOI] [PubMed] [Google Scholar]
- 2.Lim SH, Beers SA, French RR, Johnson PW, Glennie MJ, Cragg MS. Anti-CD20 monoclonal antibodies: historical and future perspectives. Haematologica. 2010;95:135–143. doi: 10.3324/haematol.2008.001628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gürcan HM, Keskin DB, Stern JN, Nitzberg MA, Shekhani H, Ahmed AR. A review of the current use of rituximab in autoimmune diseases. Int Immunopharmacol. 2009;9:10–25. doi: 10.1016/j.intimp.2008.10.004. [DOI] [PubMed] [Google Scholar]
- 4.Yeo W, Johnson PJ. Diagnosis, prevention and management of hepatitis B virus reactivation during anticancer therapy. Hepatology. 2006;43:209–220. doi: 10.1002/hep.21051. [DOI] [PubMed] [Google Scholar]
- 5.Watanabe M, Shibuya A, Tsunoda Y, Danbara M, Ishii R, Ohsaka M, et al. Re-appearance of hepatitis B virus following therapy with rituximab for lymphoma is not rare in Japanese patients with past hepatitis B virus infection. Liver Int. 2011;31:340–347. doi: 10.1111/j.1478-3231.2010.02417.x. [DOI] [PubMed] [Google Scholar]
- 6.Lee WM. Hepatitis B virus infection. N Engl J Med. 1997;337:1733–1745. doi: 10.1056/NEJM199712113372406. [DOI] [PubMed] [Google Scholar]
- 7.Liang R. How I treat and monitor viral hepatitis B infection in patients receiving intensive immunosuppressive therapies or undergoing hematopoietic stem cell transplantation. Blood. 2009;113:3147–3153. doi: 10.1182/blood-2008-10-163493. [DOI] [PubMed] [Google Scholar]
- 8.Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661–662. doi: 10.1002/hep.23190. [DOI] [PubMed] [Google Scholar]
- 9.European Association For The Study Of The Liver. EASL Clinical Practice Guidelines: management of chronic hepatitis B. J Hepatol. 2009;50:227–242. doi: 10.1016/j.jhep.2008.10.001. [DOI] [PubMed] [Google Scholar]
- 10.Hui CK, Cheung WW, Zhang HY, Au WY, Yueng YH, Leung AY, et al. Kinetics and risk of de novo hepatitis B infection in HBsAg-negative patients undergoing cytotoxic chemotherapy. Gastroenterology. 2006;131:59–68. doi: 10.1053/j.gastro.2006.04.015. [DOI] [PubMed] [Google Scholar]
- 11.Yeo W, Chan TC, Leung NW, Lam WY, Mo FK, Chu MT, et al. Hepatitis B virus reactivation in lymphoma patients with prior resolved hepatitis B undergoing anticancer therapy with or without rituximab. J Clin Oncol. 2009;27:605–611. doi: 10.1200/JCO.2008.18.0182. [DOI] [PubMed] [Google Scholar]
- 12.Katz LH, Fraser A, Gafter-Gvili A, Leibovici L, Tur-Kaspa R. Lamivudine prevents reactivation of hepatitis B and reduces mortality in immunosuppressed patients: systematic review and meta-analysis. J Viral Hepat. 2008;15:89–102. doi: 10.1111/j.1365-2893.2007.00902.x. [DOI] [PubMed] [Google Scholar]
- 13.Loomba R, Rowley A, Wesley R, Liang TJ, Hoofnagle JH, Pucino F, et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann Intern Med. 2008;148:519–528. doi: 10.7326/0003-4819-148-7-200804010-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Liaw YF, Leung N, Kao JH, Piratvisuth T, Gane E, Han KH, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008;2:263–283. doi: 10.1007/s12072-008-9080-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yeo W, Steinberg JL, Tam JS, Chan PK, Leung NW, Lam KC, et al. Lamivudine in the treatment of hepatitis B virus reactivation during cytotoxic chemotherapy. J Med Virol. 1999;59:263–269. doi: 10.1002/(sici)1096-9071(199911)59:3<263::aid-jmv1>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]
- 16.Lau GK, Yiu HH, Fong DY, Cheng HC, Au WY, Lai LS, et al. Early is superior to deferred preemptive lamivudine therapy for hepatitis B patients undergoing chemotherapy. Gastroenterology. 2003;125:1742–1749. doi: 10.1053/j.gastro.2003.09.026. [DOI] [PubMed] [Google Scholar]
- 17.Lok AS, Liang RH, Chiu EK, Wong KL, Chan TK, Todd D. Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy. Report of a prospective study. Gastroenterology. 1991;100:182–188. doi: 10.1016/0016-5085(91)90599-g. [DOI] [PubMed] [Google Scholar]
- 18.Markovic S, Drozina G, Vovk M, Fidler-Jenko M. Reactivation of hepatitis B but not hepatitis C in patients with malignant lymphoma and immunosuppressive therapy. A prospective study in 305 patients. Hepatogastroenterology. 1999;46:2925–2930. [PubMed] [Google Scholar]
- 19.Lim LL, Wai CT, Lee YM, Kong HL, Lim R, Koay E, et al. Prophylactic lamivudine prevents hepatitis B reactivation in chemotherapy patients. Aliment Pharmacol Ther. 2002;16:1939–1944. doi: 10.1046/j.1365-2036.2002.01364.x. [DOI] [PubMed] [Google Scholar]
- 20.Aksoy S, Harputluoglu H, Kilickap S, Dede DS, Dizdar O, Altundag K, et al. Rituximab-related viral infections in lymphoma patients. Leuk Lymphoma. 2007;48:1307–1312. doi: 10.1080/10428190701411441. [DOI] [PubMed] [Google Scholar]
- 21.Liang R, Lau GK, Kwong YL. Chemotherapy and bone marrow transplantation for cancer patients who are also chronic hepatitis B carriers: a review of the problem. J Clin Oncol. 1999;17:394–398. doi: 10.1200/JCO.1999.17.1.394. [DOI] [PubMed] [Google Scholar]
- 22.Sanchez MJ, Buti M, Homs M, Palacios A, Rodriguez-Frias F, Esteban R. Successful use of entecavir for a severe case of reactivation of hepatitis B virus following polychemotherapy containing rituximab. J Hepatol. 2009;51:1091–1096. doi: 10.1016/j.jhep.2009.07.012. [DOI] [PubMed] [Google Scholar]
- 23.Dillon R, Hirschfield GM, Allison ME, Rege KP. Fatal reactivation of hepatitis B after chemotherapy for lymphoma. BMJ. 2008;337:a423. doi: 10.1136/bmj.39490.680498.BE. [DOI] [PubMed] [Google Scholar]
- 24.Law JK, Ho JK, Hoskins PJ, Erb SR, Steinbrecher UP, Yoshida EM. Fatal reactivation of hepatitis B post-chemotherapy for lymphoma in a hepatitis B surface antigen-negative, hepatitis B core antibody-positive patient: potential implications for future prophylaxis recommendations. Leuk Lymphoma. 2005;46:1085–1089. doi: 10.1080/10428190500062932. [DOI] [PubMed] [Google Scholar]
- 25.Hui CK, Bowden S, Jackson K, Au WY, Fong DY, Lie AK, et al. Clinical significance of intrahepatic hepatitis B virus covalently closed circular DNA in chronic hepatitis B patients who received cytotoxic chemotherapy. Blood. 2005;105:2616–2617. doi: 10.1182/blood-2004-09-3402. [DOI] [PubMed] [Google Scholar]
- 26.Calabrese LH, Zein NN, Vassilopoulos D. Hepatitis B virus (HBV) reactivation with immunosuppressive therapy in rheumatic diseases: assessment and preventive strategies. Ann Rheum Dis. 2006;65:983–989. doi: 10.1136/ard.2005.043257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Suzuki H, Sata M, Sasaki M, Murashima S, Akiyoshi F, Noguchi S, et al. Mutations of glucocorticoid responsive element of HBV DNA. Kurume Med J. 1998;45:171–174. doi: 10.2739/kurumemedj.45.171. [DOI] [PubMed] [Google Scholar]