

Abstract
A randomized, double blind placebo controlled study was conducted to evaluate the efficacy of GutGard (root extract of Glycyrrhiza glabra) in the management of Helicobacter pylori (H. pylori) gastric load. Participants diagnosed with H. pylori infection were randomly assigned to two groups to orally receive 150 mg of GutGard (n = 55) or placebo (n = 52) once daily for 60 days. H. pylori infection was assessed using 13C-urea breath test (13C-UBT) at days 0, 30, and 60. Stool Antigen test (HpSA) was also performed on days 0, 30, and 60. Repeated measures of analysis of variance (RMANOVA), chi-square, and Fisher's exact probability tests were used to compare the treatment outcomes. A significant interaction effect between group and time (P = 0.00) and significant difference in mean Delta Over Baseline (DOB) values between GutGard (n = 50) and placebo (n = 50) treated groups after intervention period were observed. On day 60, the results of HpSA test were negative in 28 subjects (56%) in GutGard treated group whereas in placebo treated group only 2 subjects (4%) showed negative response; the difference between the groups was statistically significant. On day 60, the results of 13C-UBT were negative in 24 (48%) in GutGard treated group and the difference between the groups was statistically significant. The findings suggest GutGard is effective in the management of H. pylori.
1. Introduction
Helicobacter pylori (H. pylori) is a gram-negative spiral, or helical shaped bacteria inhabiting the gastric epithelial cells [1], of half the world human population, with prevalence rates reported to be highly variable in different regions of the industrialized and developing countries ranging from nearly 7% to greater than 95% [2]. Presence of H. pylori is associated with an increased risk of developing upper gastrointestinal tract diseases, namely, peptic ulcer disease [3–5], gastric carcinoma [6, 7], and gastric MALT lymphoma. Also, World Health Organization classified H. pylori as a type I carcinogen for gastric carcinoma [8, 9].
Maastricht III Consensus and American College of Gastroenterology recommended standard triple therapy (a proton pump inhibitor (PPI), clarithromycin, and amoxicillin/or metronidazole) and Bismuth-based quadruple therapy (Bismuth with PPI and two antibiotics) as first line treatments in subjects infected with H. pylori [10, 11]. However, the success rates of these therapies have not been very encouraging. Despite the large number of studies, identifying an optimal regimen for H. pylori, treatment still remains a challenging clinical problem. The primary cause for failure reported in systematic review and meta-analysis reports is H. pylori resistance to the antibiotics [12, 13]. Although use of molecular test systems can detect the resistance, this does not provide long term solution to rising tendency of resistance to antibiotics [14, 15]. Besides resistance, adverse effects and poor patient compliance limit the efficacy of these regimens. Considering the limitations in treatment regimens, development of alternative remedies remains constant need. With the growing popularity for naturally occurring medicinal plants, herbal preparations have been evaluated for the management of H. pylori and one such medicinal plant that holds promise for H. pylori management is licorice [16]. Licorice (Glycyrrhiza glabra Linn; Family: Leguminosae) has been in traditional use for several centuries. The roots and rhizomes of G. glabra have been reported for antipyretic, antimicrobial, hepatoprotective, antioxidant, antiadhesive, anxiolytic, expectorant, laxative, and diuretic properties [17–20]. In addition G. glabra has antiviral, antiinflammatory, anticancer, anti-ulcer activities [21, 22].
G. glabra was reported to exhibit antimicrobial activity against several gram-negative and gram-positive bacterial strains including H. pylori [23]. Besides these, licorice also demonstrated beneficial effects on H. pylori through its antiadhesive properties [20]. Activity against ulcer and cancer, clinical outcomes of H. pylori infection were also exhibited by licorice. Curative effect of deglycyrrhizinated licorice (DGL) on ulcer has been reported in vivo and in clinical studies [24–26], whereas, anti-cancer effect of licorice extract was established in in vitro study [27].
GutGard is a deglycyrrhizinated root extract of G. glabra, the safety and efficacy of which was evaluated in several studies conducted earlier. In vitro battery of genotoxicity tests showed no evidence of clastogenic and mutagenic effects and in acute oral toxicity study GutGard was found to be safe up to 5000 mg/kg rat body weight [28]. A randomized, double-blind, placebo-controlled clinical study reported significant decrease in symptoms scores of functional dyspepsia and also did not report any major trial related adverse effects [29]. Furthermore, GutGard exhibited anti-inflammatory activity likely through inhibition of COX and LOX pathways [28] and anti-ulcer activity was demonstrated in pylorus ligation, cold-restraint stress, and indomethacin induced ulcer in albino Wistar rats in which at 12.5, 25, and 50 mg/kg dose levels, the effects were found in dose dependent manner [30].
From the above considerations G. glabra is found to have potential activity against gastrointestinal related disorders and this study in particular was aimed to assess the efficacy of GutGard, in the management of H. pylori in a randomized double blind placebo controlled trial.
2. Methods
2.1. Subjects
Subjects, aged between 18–45 years with positive response in H. pylori stool antigen test (HpSA) and 13C-urea breath test (13C-UBT), were enrolled. Subjects were excluded if they (i) had history of bleeding duodenal ulcer, MALT lymphoma, gastroesophageal reflux, surgery for ulcers; (ii) had advanced chronic illness, mental illness, dementia, or suffering with concomitant symptoms of the irritable bowel syndrome, (iii) were first level relatives to gastric cancer patients, (iv) were taking antibiotics and/or PPIs and/or H 2 -antagonists 2 weeks prior to the administration of the investigational product and were using nonsteroidal anti-inflammatory drugs, steroids, bismuth preparation, (v) were participating in other clinical trials, (vi) were pregnant/lactating, (vii) were engaged in drug or alcohol abuse.
2.2. Study Intervention
Each capsule of GutGard contains 150 mg of actives of G. glabra. GutGard is a flavonoid rich, root extract of G. glabra developed by Natural Remedies, Bangalore, India. GutGard has the following phytochemical specifications, namely, glabridin (≥3.5% w/w), glabrol (≥0.5% w/w), eicosanyl caffeate (≥0.1% w/w), docosyl caffeate (≥0.1% w/w), glycyrrhizin (≤0.5% w/w), and total flavonoids (≥10% w/w).
2.3. Study Protocol
The double blind placebo controlled trial was conducted in D2L Pharma Research Centre, Bangalore, Karnataka, India, from July 2011 to November 2011. Ethics Committee approval was obtained for the conduct of the trial. A total of 215 subjects were screened and 107 subjects with positive response to HpSA test and 13C-UBT were recruited. The investigator clearly explained the purpose and methodology of the clinical trial in a simple, explicable language before taking consent from the subjects for participation in the trial. In addition the queries/doubts of trial subjects if any were clarified by the investigator prior to signing the consent form. The subjects were asked to completely understand and sign the informed consent form. The subjects were informed that they can withdraw from the study at any point without any prior notice. It was informed, if the subject volunteers to provide the reasons for opting out, consent to use this information will be taken from the subject. Following the consent, the subjects were randomly assigned to GutGard (n = 55) and placebo (n = 52) groups. A computer aided programme was used to generate randomization list and the random numbers were considered as subject code. As per the random allocation sequence, the containers (either GutGard or placebo) were labeled with unique random numbers. The entire process was carried out in a confidential manner and all the study related personnel, namely, investigators, subjects, and other supportive staff were unaware of the random allocation sequence.
The study medication was dispensed by the pharmacist to the subjects taking into consideration the order of enrollment and as per the random allocation sequence. Both GutGard and placebo capsules were similar in appearance (size, shape, and color) and flavor including packaging. The study interventions were packaged and labeled identically to maintain blinding. The personnel (investigator, pharmacist, and subjects) involved in the trial were blinded during the trial period. Each subject was given a container of 30 capsules and was advised to take one capsule daily with a glass of water before food in the morning for 30 days. The subjects were informed to visit the trial centre on day 30 along with the container and the study diary card. The compliance to study medication was recorded by counting the leftover capsules in the container and from the diary card. After recording the compliance, another container of 30 capsules was provided to the subjects and the same procedure was followed at the scheduled followup on day 60.
2.4. Outcome Measures
The gastric load of H. pylori was assessed on days 0, 30, and 60. Decrease in H. pylori gastric load was assessed using 13C-UBT and HpSA test as outcome measures. The proportion of subjects with initial positive 13C-UBT and HpSA test results found to be negative at day 30 and day 60 was measured.
2.5. Data Analysis
The required sample size for the GutGard clinical study in the management of H. pylori was calculated using the formula n = (8(CV)2/(PC)2)(1 + (1 − PC)2) [31] where proportionate change in means (PC) of 20% [32] with 35% of coefficient of variation (CV) was considered. Assuming a possibility of lost to followup or dropouts as 20% at least 50 subjects were needed for each group. Hence, the required sample size was calculated as 100 subjects for the entire study.
At baseline, the characteristics of the subjects of the two groups were compared by independent sample t-test. The cure rates and the interaction effects between group and time were determined using per protocol (PP) analysis. The Delta Over Baseline (DOB) values were expressed as mean ± SD at days 0, 30, and 60 and were analyzed by repeated measures of analysis of variance (RMANOVA) and the statistical significance was set at P ≤ 0.05. Positive and negative responses from the HpSA test and 13C-UBT were assessed. The proportion of individuals showing positive and negative response to 13C-UBT in GutGard and placebo treated groups was analyzed using Fisher's exact probability test, and chi-square test was used to analyze the proportion of individuals showing positive and negative response to HpSA test. The statistical analysis of side effects was performed with the chi-square analysis.
3. Results
A total of 215 subjects were screened initially, and 107 subjects were recruited. Seven out of the 107 enrolled were excluded from the study as they did not satisfy the inclusion criteria for age (subjects were over 45 years of age); finally, 100 subjects per protocol were analyzed (Figure 1). At baseline mean characteristics of treated group versus placebo were found to be comparable (Table 1). A significant interaction effect between group and time (df = 2,196; F = 1120.27; P = 0.00) and time effect was observed between the groups. Significant difference in mean DOB values was observed between GutGard and placebo treated groups after intervention period. The magnitude of decrease in the H. pylori load is summarized in Table 2. The proportion of subjects turned from positive to negative response status is elucidated in Table 3. At day 0 and day 30 all the subjects in placebo and GutGard treated groups showed positive response to HpSA test and 13C-UBT. On day 60, the results of HpSA test were negative in 28 subjects (56%) in GutGard treated group and 2 subjects (4%) in placebo treated group; the difference between the groups was statistically significant. On day 60, the results of 13C-UBT were negative in 24 (48%) in GutGard and one (2%) in placebo consumed subjects; the difference was statistically significant.
Figure 1.
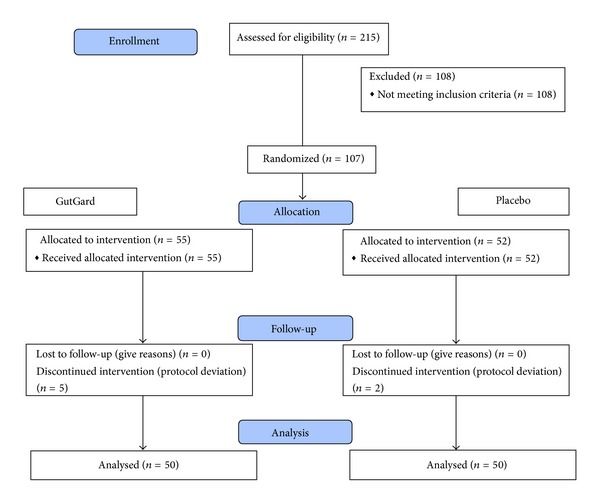
Flow chart of disposition of subjects.
Table 1.
Characteristics of the subjects at baseline (mean ± SD).
| Parameters | GutGard (n = 50) | Placebo (n = 50) |
|---|---|---|
| Subjects (male/female) |
23/27 | 23/27 |
| Age (years) |
32.86 ± 6.50 |
33.10 ± 5.59 |
| Weight (kg) |
62.60 ± 7.43 |
62.31 ± 7.79 |
| Height (cms) | 166.12 ± 8.45 | 165.56 ± 7.67 |
| Heart rate/min |
69.34 ± 4.30 |
69.08 ± 4.26 |
| BP systolic (mmHg) |
116.72 ± 6.44 |
115.40 ± 6.98 |
| BP diastolic (mmHg) |
80.80 ± 5.29 |
80.28 ± 4.43 |
| HpSA |
Positive | Positive |
|
δ (means) |
7.12 ± 1.36 |
6.88 ± 1.34 |
P ≤ 0.05 versus placebo.
δ: delta over baseline value of 13C urea breath test.
Table 2.
Effect of GutGard on H. pylori gastric load (mean ± SD).
| Parameter | Groups | Day 0 | Day 30 | Day 60 | Significance | |||
|---|---|---|---|---|---|---|---|---|
| Variables | df | F value | P value | |||||
| DOB | GutGard | 7.12 ± 1.36 | 6.24 ± 1.24 | 4.21 ± 1.15 | Group | 1,98 | 5.63 | 0.02 |
| Placebo | 6.88 ± 1.34 | 6.40 ± 1.31 | 6.10 ± 1.30 | Time | 2,196 | 3047.10 | 0.00 | |
| Group × time | 2,196 | 1120.27 | 0.00 | |||||
Table 3.
Proportion of subjects turned from H. pylori—positive (Hp+) to negative (Hp−) status as measured by HpSA and 13C-UBT.
| Groups | Days | n | HpSA | 13C-UBT | ||
|---|---|---|---|---|---|---|
| Hp+ | Hp− (%) | Hp+ | Hp− (%) | |||
| GutGard | 0 | 50 | 50 | 0 (0) | 50 | 0 (0) |
| Placebo | 50 | 50 | 0 (0) | 50 | 0 (0) | |
| GutGard | 30 | 50 | 50 | 0 (0) | 50 | 0 (0) |
| Placebo | 50 | 50 | 0 (0) | 50 | 0 (0) | |
| GutGard | 60 | 50 | 22 | 28* (56) | 26 | 24* (48) |
| Placebo | 50 | 48 | 2 (4) | 49 | 1 (2) | |
n: no. of subjects; Hp−: H. pylori negative; Hp+: H. pylori positive.
%: percentage of subjects turned from Hp Positive to Hp Negative.
*Significant difference compared to placebo.
Safety. Regarding the overall tolerability of interventions, in total 22 subjects (22%) showed at least one side-effect. One subject (1%) experienced moderate side-effect (fever); 21 subjects (21%) experienced mild side-effects, but none stopped the treatment and all have completed the study. The incidences of side-effects were considered to be not related to treatment. The profiles and frequencies of side-effects were listed in Table 4. On comparison, the frequencies of side-effects between GutGard and placebo treated groups were non-significant (Table 4).
Table 4.
Side effects during intervention period.
| Side effect | GutGard (n = 50) n (%) |
Placebo (n = 50) n (%) |
P value |
|---|---|---|---|
| Mild diarrhoea | 5 (10) | 2 (4) | 0.24 |
| Mild headache | 1 (2) | 1 (2) | 1.00 |
| Mild vomiting | 3 (6) | 1 (2) | 0.30 |
| Mild nausea | 1 (2) | 1 (2) | 1.00 |
| Mild throat pain | 1 (2) | 1 (2) | 1.00 |
| Mild cold and cough | 1 (2) | 1 (2) | 1.00 |
| Mild body pain | 1 (2) | 1 (2) | 1.00 |
| Mild fever | 2 (4) | 0 | 0.15 |
| Moderate fever | 1 (2) | 0 | 0.31 |
| Acidity | 1 (2) | 1 (2) | 1.00 |
| Mild pain in stomach | 1 (2) | 0 | 0.31 |
| Mild body heat | 1 (2) | 3 (6) | 0.30 |
4. Discussion
Extensive research in the past few decades since the discovery of H. pylori indicated that it is the major risk factor for gastrointestinal disorders and the research guidelines recommended that all H. pylori positive individuals be treated irrespective of the clinical outcome. The eradication of H. pylori in the infected subjects will not only prevent H. pylori associated diseases but also limit the spread of infection [33]. Albeit, different regimens are available for the treatment of H. pylori, the success rates of these regimens are low due to the rising prevalence of antimicrobial resistance and an effective regimen for H. pylori still remains elusive. Use of herbal supplements as alternative sources has attracted the researchers worldwide over the past few years and several studies on medicinal plants have been undertaken to evaluate the anti-H. pylori effects [34–37]. From the published preclinical studies, G. glabra is reported to possess activity against H. pylori [23, 38, 39]; however, the major concern is the validation of these effects in well designed clinical settings. In the present study, GutGard, an extract of G. glabra, has been evaluated in a double blind placebo controlled trial for its efficacy in the management of H. pylori representing one of the pioneering studies in this aspect.
In the present study, effectiveness of GutGard supplementation for 60 days was evaluated in subjects positive for H. pylori based on the HpSA and 13C-UBT results pre- and posttreatment. An interaction effect with significant difference in mean DOB values between GutGard and placebo treated groups after intervention period was observed. DOB is increasingly recognized as a quantitative measure of H. pylori gastric load [40]. The bacterial urease activity, which correlates with DOB values, mainly depends on the overall bacterial load [41] and some studies have suggested that high DOB values are associated with a high bacterial load in the stomach [42–44] as well as with H. pylori virulence factors, such as CagA [45, 46]. The data on GutGard indicates that the H. pylori load was significantly decreased in GutGard treated subjects as compared to placebo treatment. Apart from decrease in gastric load of H. pylori, the GutGard treated subjects showed negative response in 13C-UBT and tested negative in HpSA test. The results of HpSA and 13C-UBT in terms of number of subjects with negative H. pylori test findings are in concordance with earlier study outcomes which demonstrated that 13C-UBT and HpSA are absolutely equivalent in terms of sensitivity and specificity in the evaluation of eradication therapy [47–49].
Several studies have evaluated the effects of supplementation of extracts of medicinal herbs along with standard treatment regimens in the management of H. pylori [50, 51], and only few studies evaluated the effect of herbal preparations as a stand alone or along with antacids. Zhang et al. reported that 14.43% of the subjects evaluated in a double-blind randomized placebo-controlled trial showed negative results for H. pylori after 90 days of supplementation with Cranberry juice [32]. Administration of 5 g of vitamin C for 4 weeks in H. pylori positive patients with chronic gastritis resulted in recovery of 30% of the patients treated with vitamin C [52]. Treatment effects with 1 g, 2 g, and 3 g Nigella sativa administered with omeprazole were 47.6%, 66.7%, and 47.8% [53], respectively, while as a stand alone supplement GutGard showed 56% cure rate. Results of earlier clinical studies provide insights on the eradication rates of mono-, dual, and triple therapies. The eradication rates reported for monotherapy was 0–54%, and dual therapies revealed recovery rate of 50–85%. Further the triple therapies that are recommended as first line option were reported to have a cure rate of 95% [54, 55]. However, in actual clinical settings even the triple therapies have been reported to have shown eradication rates of less than 80% [56, 57]. The results of acid stable effective monotherapy for the treatment of H. pylori as a stand alone were comparable to GutGard cure rates. The fact that the eradication rates in clinical settings for antibiotic regimens are very low indicates preexisting resistance of H. pylori to antibiotics due to wide spread use of antibiotics for other indications, side effects, and premature discontinuation of antibiotic use. In such a scenario, GutGard that is well tolerated, safe, and with effective cure rates would be a better alternative for the management of H. pylori. As there are genetic differences in H. pylori strains in east and west [58], further research in different locations and investigating the effect of GutGard in subjects resistant to antibiotics, subjects with treatment failure to triple therapy, or evaluating effectiveness of GutGard in combination with proton pump inhibitors/other antibiotics as dual or triple therapy will further establish the effectiveness of GutGard.
The activity of GutGard on gastric H. pylori may be explained by various possible mechanisms. Based on the findings by Fukai et al. [38], about the anti-H. pylori activity of licorice, the anti-microbial activity of GutGard was investigated using in vitro assays such as DNA gyrase inhibition, protein synthesis inhibition, and dihydrofolate reductase (DHFR) enzyme inhibition. DNA gyrase is an essential bacterial enzyme that catalyzes the ATP-dependent negative supercoiling of double-stranded closed-circular DNA. DNA gyrase is vital for transcription and replication of bacteria [59]; inhibition of DNA gyrase appears to be an opt target for anti-microbials. GutGard has shown activity by inhibiting DNA gyrase [60]; the results are in accordance with the study published by Hui et al. [61]. Interestingly, GutGard also inhibited protein synthesis and DHFR enzyme in vitro [60]. Blockade of DHFR causes cell death through inhibition of DNA synthesis and is considered suitable target for inhibition of H. pylori replication [62]. The aforementioned mechanisms may attribute to the effect of GutGard on H. pylori management.
GutGard was found to be safe and well tolerated. Few side effects, namely, nausea, diarrhoea, headache, throat pain, vomiting, cold and cough, body pain, acidity, body heat, fever, and pain in stomach were observed mostly in both placebo and GutGard treated groups. However, side-effects recorded did not reveal any significant differences between treatment groups and were found to be non-treatment-related. The published literature on clinical studies of licorice formulations also did not report any significant adverse events that indicate the safe nature of the dietary supplement [24]. The safety on present intake levels of GutGard is also affirmed in the study by Raveendra et al. [29].
5. Conclusion
In conclusion, the findings of the randomized double blind placebo controlled trial on GutGard, extract of G. glabra revealed significant decrease in the H. pylori, gastric load as compared to placebo and was found to be safe and well tolerated. In the present study, treatment with GutGard was found to be 73.2% or 3.73 times more effective than placebo. Hence GutGard supplementation can be considered an effective alternative remedy for the management of H. pylori.
Acknowledgment
The authors thankfully acknowledge the financial assistance provided by NICS Co., Ltd., Seoul, Republic of Korea for the project.
References
- 1.Marshall JB. One Hundred Years of Discovery and Rediscovery of Helicobacter pylori and Its Association With Peptic Ulcer Disease Chapter 3. Washington, DC, USA: ASM Press; 2001. [PubMed] [Google Scholar]
- 2.Hunt RH, Xiao SD, Megraud F, et al. Helicobacter pylori in developing countries. Journal of Gastrointestinal and Liver Diseases. 2011;20(3):299–304. [PubMed] [Google Scholar]
- 3.Nomura A, Stemmermann GN, Chyou PH, Perez-Perez GI, Blaser MJ. Helicobacter pylori infection and the risk for duodenal and gastric ulceration. Annals of Internal Medicine. 1994;120(12):977–981. doi: 10.7326/0003-4819-120-12-199406150-00001. [DOI] [PubMed] [Google Scholar]
- 4.Adamu MA, Schottker B, Weck MN, Brenner H. Helicobacter pylori infection is strongly associated with gastric and duodenal ulcers in a large prospective study. Clinical Gastroenterology and Hepatology. 2012;10(5):487–493. doi: 10.1016/j.cgh.2011.12.036. [DOI] [PubMed] [Google Scholar]
- 5.Dai WQ, Zhou YQ, Xu L, et al. The Eradicating Helicobacter pylori infection in duodenal ulcer patients by three short-term triple therapies in China: a multicenter clinical comparative study. Hepato-Gastroenterology. 2012;59(133):296–299. doi: 10.5754/hge11241. [DOI] [PubMed] [Google Scholar]
- 6.Uemura N, Okamoto S, Yamamoto S, et al. Helicobacter pylori infection and the development of gastric cancer. The New England Journal of Medicine. 2001;345(11):784–789. doi: 10.1056/NEJMoa001999. [DOI] [PubMed] [Google Scholar]
- 7.Fuccio L, Zagari RM, Eusebi LH, et al. Meta-analysis: can Helicobacter pylori eradication treatment reduce the risk for gastric cancer? Annals of Internal Medicine. 2009;151(2):121–128. doi: 10.7326/0003-4819-151-2-200907210-00009. [DOI] [PubMed] [Google Scholar]
- 8.Montalban C, Castrillo JM, Abraira V, et al. Gastric B-cell mucosa-associated lymphoid tissue (MALT) lymphoma. Clinicopathological study and evaluation of the prognostic factors in 143 patients. Annals of Oncology. 1995;6(4):355–362. doi: 10.1093/oxfordjournals.annonc.a059184. [DOI] [PubMed] [Google Scholar]
- 9.Owens SR, Smith LB. Molecular aspects of H. pylori-related MALT lymphoma. Pathology Research International. 2011;2011:8 pages. doi: 10.4061/2011/193149.193149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Malfertheiner P, Megraud F, O'Morain C, et al. Current concepts in the management of Helicobacter pylori infection: the maastricht III consensus report. Gut. 2007;56(6):772–781. doi: 10.1136/gut.2006.101634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chey WD, Wong BC. American College of Gastroenterology guideline on the management of Helicobacter pylori infection. The American Journal of Gastroenterology. 2007;102(8):1808–1825. doi: 10.1111/j.1572-0241.2007.01393.x. [DOI] [PubMed] [Google Scholar]
- 12.Fischbach L, Evans EL. Meta-analysis: The effect of antibiotic resistance status on the efficacy of triple and quadruple first-line therapies for Helicobacter pylori . Alimentary Pharmacology and Therapeutics. 2007;26(3):343–357. doi: 10.1111/j.1365-2036.2007.03386.x. [DOI] [PubMed] [Google Scholar]
- 13.De Francesco V, Giorgio F, Hassan C, et al. Worldwide H. pylori antibiotic resistance: a systematic review. Journal of Gastrointestinal and Liver Diseases. 2010;19(4):409–414. [PubMed] [Google Scholar]
- 14.Basset C, Holton J, Gatta L, et al. Helicobacter pylori infection: anything new should we know? Alimentary Pharmacology and Therapeutics. 2004;20(2):31–41. doi: 10.1111/j.1365-2036.2004.02040.x. [DOI] [PubMed] [Google Scholar]
- 15.Mégraud F. H. pylori antibiotic resistance: prevalence, importance, and advances in testing. Gut. 2004;53(9):1374–1384. doi: 10.1136/gut.2003.022111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.O’Mahony R, Al-Khtheeri H, Weerasekera D, et al. Bactericidal and anti-adhesive properties of culinary and medicinal plants against Helicobacter pylori . World Journal of Gastroenterology. 2005;11(47):7499–7507. doi: 10.3748/wjg.v11.i47.7499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hikino H. Recent research on oriental medicinal plants. In: Wagner H, Hikino H, Farnsworth NR, editors. Economic and Medicinal Plant Research. London, UK: Academic Press; 1985. pp. 53–85. [Google Scholar]
- 18.Vaya J, Belinky PA, Aviram M. Antioxidant constituents from licorice roots: isolation, structure elucidation and antioxidative capacity toward LDL oxidation. Free Radical Biology and Medicine. 1997;23(2):302–313. doi: 10.1016/s0891-5849(97)00089-0. [DOI] [PubMed] [Google Scholar]
- 19.Lata S, Kakkar S, Srivastava VK, Saxena KK, Saxena RS, Kumar A. Comparative antipyretic activity of Ocimum sanctum, Glycyrrhiza glabra and aspirin in experimentally-induced pyrexia in rats. Indian Journal of Pharmacology. 1999;31(1):71–75. [Google Scholar]
- 20.Wittschier N, Faller G, Hensel A. Aqueous extracts and polysaccharides from Liquorice roots (Glycyrrhiza glabra L.) inhibit adhesion of Helicobacter pylori to human gastric mucosa. Journal of Ethnopharmacology. 2009;125(2):218–223. doi: 10.1016/j.jep.2009.07.009. [DOI] [PubMed] [Google Scholar]
- 21.Dong S, Inoue A, Zhu Y, Tanji M, Kiyama R. Activation of rapid signaling pathways and the subsequent transcriptional regulation for the proliferation of breast cancer MCF-7 cells by the treatment with an extract of Glycyrrhiza glabra root. Food and Chemical Toxicology. 2007;45(12):2470–2478. doi: 10.1016/j.fct.2007.05.031. [DOI] [PubMed] [Google Scholar]
- 22.Zore GB, Winston UB, Surwase BS, et al. Chemoprofile and bioactivities of Taverniera cuneifolia (Roth) Arn.: a wild relative and possible substitute of Glycyrrhiza glabra L. Phytomedicine. 2008;15(4):292–300. doi: 10.1016/j.phymed.2007.01.006. [DOI] [PubMed] [Google Scholar]
- 23.Gupta VK, Fatima A, Faridi U, et al. Antimicrobial potential ofGlycyrrhiza glabraroots. Journal of Ethnopharmacology. 2008;116(2):377–380. doi: 10.1016/j.jep.2007.11.037. [DOI] [PubMed] [Google Scholar]
- 24.Larkworthy W, Holgate PF. Deglycyrrhizinized liquorice in the treatment of chronic duodenal ulcer. A retrospective endoscopic survey of 32 patients. Practitioner. 1975;215(1290):787–792. [PubMed] [Google Scholar]
- 25.Bennett A, Clark-Wibberley T, Stamford IF, Wright JE. Aspirin-induced gastric mucosal damage in rats: cimetidine and deglycyrrhizinated liquorice together give greater protection than low doses of either drug alone. Journal of Pharmacy and Pharmacology. 1980;32(2):p. 151. doi: 10.1111/j.2042-7158.1980.tb12879.x. [DOI] [PubMed] [Google Scholar]
- 26.Feldman RA. Epidemiologic observations and open questions about disease and infection caused by Helicobacter pylori . In: Achtman M, Suerbaum S, editors. Helicobacter pylori: Molecular and Cellular Biology. Wymondham, UK: Horizon Scientific Press; 2001. pp. 29–51. [Google Scholar]
- 27.Zhang LI, Yan-li GE, Yong-hui Lin, Zhi-rong Wang, Qiong Wu, Jun-jie Zhang. Experimental study of the effect of Glycyrrhiza flavonoids on gastric cancer in vivo. Journal of Tongji University. 2010 [Google Scholar]
- 28.Chandrasekaran CV, Sundarajan K, Gupta A, Srikanth HS, Edwin J, Agarwal A. Evaluation of the genotoxic potential of standardized extract of Glycyrrhiza glabra (GutGard) Regulatory Toxicology and Pharmacology. 2011;61(3):373–380. doi: 10.1016/j.yrtph.2011.10.002. [DOI] [PubMed] [Google Scholar]
- 29.Raveendra KR, Jayachandra, Srinivasa V. An extract of Glycyrrhiza glabra (GutGard) alleviates symptoms of functional dyspepsia: a randomized, double-blind, placebo-controlled study. Evidence-Based Complementary and Alternative Medicine. 2012;2012 doi: 10.1155/2012/216970.216970 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mukherjee M, Bhaskaran N, Srinath R, et al. Anti-ulcer and antioxidant activity of GutGard. Indian Journal of Experimental Biology. 2010;48(3):269–274. [PubMed] [Google Scholar]
- 31.van Belle G, Millard StevenP. STRUTS Statistical Rules of Thumb. Seattle, Wash, USA: University of Washington; [Google Scholar]
- 32.Zhang L, Ma J, Pan K, Go VL, Chen J, You WC. Efficacy of cranberry juice on Helicobacter pylori infection: a double-blind, randomized placebo-controlled trial. Helicobacter. 2005;10(2):139–145. doi: 10.1111/j.1523-5378.2005.00301.x. [DOI] [PubMed] [Google Scholar]
- 33.Asaka M, Kato M, Takahashi S, et al. Guidelines for the management of Helicobacter pylori infection in Japan: 2009 revised edition. Helicobacter. 2010;15(1):1–20. doi: 10.1111/j.1523-5378.2009.00738.x. [DOI] [PubMed] [Google Scholar]
- 34.Iimuro M, Shibata H, Kawamori T, et al. Suppressive effects of garlic extract on Helicobacter pylori-induced gastritis in Mongolian gerbils. Cancer Letters. 2002;187(1-2):61–68. doi: 10.1016/s0304-3835(02)00401-9. [DOI] [PubMed] [Google Scholar]
- 35.Matsubara S, Shibata H, Ishikawa F, et al. Suppression of Helicobacter pylori-induced gastritis by green tea extract in Mongolian gerbils. Biochemical and Biophysical Research Communications. 2003;310(3):715–719. doi: 10.1016/j.bbrc.2003.09.066. [DOI] [PubMed] [Google Scholar]
- 36.Nariman F, Eftekhar F, Habibi Z, Falsafi T. Anti-Helicobacter pylori activities of six Iranian plants. Helicobacter. 2004;9(2):146–151. doi: 10.1111/j.1083-4389.2004.00211.x. [DOI] [PubMed] [Google Scholar]
- 37.Lengsfeld C, Titgemeyer F, Faller G, Hensel A. Glycosylated compounds from Okra inhibit adhesion of Helicobacter pylori to human gastric mucosa. Journal of Agricultural and Food Chemistry. 2004;52(6):1495–1503. doi: 10.1021/jf030666n. [DOI] [PubMed] [Google Scholar]
- 38.Fukai T, Marumo A, Kaitou K, Kanda T, Terada S, Nomura T. Anti-Helicobacter pylori flavonoids from licorice extract. Life Sciences. 2002;71(12):1449–1463. doi: 10.1016/s0024-3205(02)01864-7. [DOI] [PubMed] [Google Scholar]
- 39.Krausse R, Bielenberg J, Blaschek W, Ullmann U. In vitro anti-Helicobacter pylori activity of Extractum liquiritiae, glycyrrhizin and its metabolites. Journal of Antimicrobial Chemotherapy. 2004;54(1):243–246. doi: 10.1093/jac/dkh287. [DOI] [PubMed] [Google Scholar]
- 40.Kobayashi D, Eishi Y, Ohkusa T, et al. Gastric mucosal density of Helicobacter pylori estimated by real-time PCR compared with results of urea breath test and histological grading. Journal of Medical Microbiology. 2002;51(4):305–311. doi: 10.1099/0022-1317-51-4-305. [DOI] [PubMed] [Google Scholar]
- 41.De Francesco V, Zullo A, Perna F, et al. Helicobacter pylori antibiotic resistance and [13C] urea breath test values. Journal of Medical Microbiology. 2010;59(5):588–591. doi: 10.1099/jmm.0.018077-0. [DOI] [PubMed] [Google Scholar]
- 42.Perri F, Clemente R, Pastore M, et al. The 13C-urea breath test as a predictor of intragastric bacterial load and severity of Helicobacter pylori gastritis. Scandinavian Journal of Clinical and Laboratory Investigation. 1998;58(1):19–27. doi: 10.1080/00365519850186797. [DOI] [PubMed] [Google Scholar]
- 43.Zagari RM, Pozzato P, Martuzzi C, et al. 13C-urea breath test to assess Helicobacter pylori bacterial load. Helicobacter. 2005;10(6):615–619. doi: 10.1111/j.1523-5378.2005.00358.x. [DOI] [PubMed] [Google Scholar]
- 44.Cremonini F, Bartolozzi F, Armuzzi A, et al. Can 13C urea breath test predict resistance to therapy in Helicobacter pylori infection? Hepato-Gastroenterology. 2005;52(64):1119–1121. [PubMed] [Google Scholar]
- 45.Zullo A, Sanchez-Mete L, Hassan C, et al. Helicobacter pylori density and cagA status in cirrhotic patients: a case-control study. Journal of Gastroenterology and Hepatology. 2004;19(10):1174–1178. doi: 10.1111/j.1440-1746.2004.03440.x. [DOI] [PubMed] [Google Scholar]
- 46.Sarker SA, Nahar S, Rahman M, et al. High prevalence of cagA and vacA seropositivity in asymptomatic Bangladeshi children with Helicobacter pylori infection. Acta Paediatrica. 2004;93(11):1432–1436. doi: 10.1080/08035250410033088. [DOI] [PubMed] [Google Scholar]
- 47.Vaira D, Malfertheiner P, Mégraud F, et al. Diagnosis of Helicobacter pylori infection with a new non-invasive antigen-based assay. The Lancet. 1999;354(9172):30–33. doi: 10.1016/s0140-6736(98)08103-3. [DOI] [PubMed] [Google Scholar]
- 48.Vaira D, Malfertheiner P, Megraud F, et al. Noninvasive antigen-based assay for assessing Helicobacter pylori eradication: a European multicenter study. The American Journal of Gastroenterology. 2000;95(4):925–929. doi: 10.1111/j.1572-0241.2000.01931.x. [DOI] [PubMed] [Google Scholar]
- 49.Vaira D, Vakil N, Menegatti M, et al. The stool antigen test for detection of Helicobacter pylori after eradication therapy. Annals of Internal Medicine. 2002;136(4):280–287. doi: 10.7326/0003-4819-136-4-200202190-00007. [DOI] [PubMed] [Google Scholar]
- 50.Myllyluoma E, Veijola L, Ahlroos T, et al. Probiotic supplementation improves tolerance to Helicobacter pylori eradication therapy: a placebo-controlled, double-blind randomized pilot study. Alimentary Pharmacology and Therapeutics. 2005;21(10):1263–1272. doi: 10.1111/j.1365-2036.2005.02448.x. [DOI] [PubMed] [Google Scholar]
- 51.Lee SJ, Park JY, Choi KS, et al. Efficacy of Korean red ginseng supplementation on eradication rate and gastric volatile sulfur compound levels after Helicobacter pylori eradication therapy. Journal of Ginseng Research. 2010;34(2):122–131. [Google Scholar]
- 52.Jarosz M, Dzieniszewski J, Dabrowska-Ufniarz E, Wartanowicz M, Ziemlanski S, Reed P. Effects of high dose vitamin C treatment on Helicobacter pylori infection and total vitamin C concentration in gastric juice. European Journal of Cancer Prevention. 1998;7(6):449–454. doi: 10.1097/00008469-199812000-00004. [DOI] [PubMed] [Google Scholar]
- 53.Salem EM, Yar T, Bamosa AO, et al. Comparative study of Nigella Sativa and triple therapy in eradication of Helicobacter pylori in patients with non-ulcer dyspepsia. Saudi Journal of Gastroenterology. 2010;16(3):207–214. doi: 10.4103/1319-3767.65201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Peterson WL, Graham DY, Marshall B, et al. Clarithromycin as monotherapy for eradication of Helicobacter pylori: a randomized, double-blind trial. The American Journal of Gastroenterology. 1993;88(11):1860–1864. [PubMed] [Google Scholar]
- 55.Joshi YK. Helicobacter pylori infection: current status. Journal of Indian Academy of Clinical Medicine. 2000;5(2):148–155. [Google Scholar]
- 56.Thyagarajan SP, Ray P, Das BK, et al. Geographical difference in antimicrobial resistance pattern of H. pylori clinical isolates from Indian patients: multicentric study. Journal of Gastroenterology and Hepatology. 2003;18(12):1373–1378. doi: 10.1046/j.1440-1746.2003.03174.x. [DOI] [PubMed] [Google Scholar]
- 57.Talaie R, Zojaji H, Mirsattari D, Kaboli A, Alizadeh AHM, Zali MR. Comparison of two different eradication regimens for H. pylori: amoxicillin, metronidazole, bismuth and omeprazole (OMAB) versus the new regimen of penbactam, clarithromycin and omeprazole (OPC), a randomized clinical trial. Journal of Gastroenterology and Hepatology. 2008;1(3):19–22. [Google Scholar]
- 58.Jang S, Jones KR, Olsen CH, et al. Epidemiological link between gastric disease and polymorphisms in VacA and CagA. Journal of Clinical Microbiology. 2010;48(2):559–567. doi: 10.1128/JCM.01501-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Chatterji M, Unniraman S, Mahadevan S, Nagaraja V. Effect of different classes of inhibitors on DNA gyrase from Mycobacterium smegmatis . Journal of Antimicrobial Chemotherapy. 2001;48(4):479–485. doi: 10.1093/jac/48.4.479. [DOI] [PubMed] [Google Scholar]
- 60.Asha MK, Debraj D, Prashanth D, et al. In vitro anti-Helicobacter pylori activity of a flavonoid rich extract of Glycyrrhiza glabra and its probable mechanisms of action. Journal of Ethnopharmacology. 2013;145(2):581–586. doi: 10.1016/j.jep.2012.11.033. [DOI] [PubMed] [Google Scholar]
- 61.Hui XU, Pan YAO, Guodong LIN, Weiwen CHEN. In-vitro inhibitory effect of methanol extracts of Chinese herbal drugs on supercoiling activity of bacterial DNA Gyrase [OL] 2011, http://www.paper.edu.cn/index.php/default/en_releasepaper/content/4411791.
- 62.Mendz GL, Shepley AJ, Hazell SL, Smith MA. Purine metabolism and the microaerophily of Helicobacter pylori . Archives of Microbiology. 1997;168(6):448–456. doi: 10.1007/s002030050521. [DOI] [PubMed] [Google Scholar]