

Abstract
Adolescence represents a developmental period for children with attention-deficit hyperactivity disorder (ADHD) during which the severity of mental health problems may change at a time when teens are consolidating their self identify and possibly questioning the label of an ADHD diagnosis, treatment, and types of interventions. This study investigates the shared critical events related to help-seeking reported by eight teenagers with ADHD, their mothers, and teachers and how the reported events and constructed shared focus on specific problems might explain teenagers’ transitions in their illness careers. Data collected through a qualitative application of the experience sampling method illuminated diverse illness career transitions including continuing treatment, transitioning from being treated to untreated, from being untreated to treated, and remaining untreated. Our findings support a model of shifting perspectives on illness and wellness among adolescents with ADHD, rather than a staged progression of adaptation to a chronic disorder.
Keywords: adolescents, attention deficit-hyperactivity disorder (ADHD), illness and disease, social construction
Adolescence represents a particularly salient transition period for children with attention-deficit hyperactivity disorder (ADHD). ADHD is characterized by childhood onset of symptoms of hyperactivity (e.g., fidgeting, out of seat, running, acting like driven by a motor), impulsivity (e.g., blurting out, interrupting), and/or inattention (e.g., difficulty focusing, distractibility, forgetfulness, disorganization) that are maladaptive, not consistent with the child’s developmental level and present in at least two settings, such as school and home (American Psychiatric Association, 1994). Most children with ADHD will experience some symptom decline as they grow older, particularly of hyperactive/impulsive symptoms and some may even be considered to completely “outgrow” the disorder (Mick, Faraone, & Biederman, 2004). A minority may continue to exhibit a full array of ADHD symptoms (i.e., inattention, hyperactivity, impulsivity), and some will experience more severe mental health problems as they grow older, for example due to adolescent onset of depression, eating disorders or substance abuse (Biederman et al., 1996; Jensen et al., 2007; Rasmussen & Gillberg, 2000).
In community samples, ADHD has been shown to be associated with poor academic and educational outcomes, including poor grades, low standardized test scores in reading and math, increased rates of detention and expulsion and increased rates of referral to special education (LeFever, Villers, Morrow, & Vaughn, 2005; Loe & Feldman, 2007). These undesirable academic outcomes in part reflect the high co-occurrence of learning disorders, particularly dyslexia, among children with ADHD (Fletcher et al.,1999). Historically ADHD and reading disorders were not always viewed as separate entities, but recent studies indicate that the latter are characterized by phonological processing problems not apparent in children with ADHD only, whereas ADHD is a behavioral disorder associated with deficits in executive functions (Shaywitz, Fletcher, & Shaywitz,1995; Sonuga-Barke, 2005). ADHD is also associated with lower performance on intelligence testing. In a meta-analytic study of 137 studies assessing ADHD and intelligence scores, Frazier et al. (2004) reported that IQ scores of children with ADHD are on average 9 points lower than those of peers without ADHD. Yet, the coexistence of ADHD and high IQ (IQ > 120) is also clearly documented (Antshel et al., 2007), countering assertions that ADHD symptoms in gifted children only represent academic under challenge and resulting boredom.
Empirically supported treatments for ADHD include behavior management techniques and medications; however, in head-to-head comparisons medications are more effective in reducing core symptoms of ADHD (The MTA Cooperative Group, 1999). In a recent study, social stigma and feeling different from peers were frequently cited reasons for stopping ADHD medications (Meaux, Hester, Smith, & Shoptaw, 2006). In general, adolescents have a strong desire to be accepted as “normal” by their peers, and they may discard the “ADHD patient role” previously assigned by parents, the school system and treatment providers to achieve this goal. Furthermore, Hansen and Hansen (2006) found that parents themselves perceived the use of stimulate medication as a balancing act, “as they considered the medication’s desirable and undesirable effects on various settings” (p. 1267).
Children with ADHD may also qualify for educational interventions under the Individuals with Disabilities Education Act as reauthorized in 2004 (IDEA) if they meet criteria for the other health impairment category because problems of limited alertness impede their academic performance (U.S. Department of Education, 2004), or under Section 504 of the Vocational Rehabilitation Act if ADHD limits a major life activity like learning (Office of Special Education, 1992). Examples of commonly used educational interventions are modifications to instruction, assignments or test taking. The impact of such interventions has not been studied extensively, as most outcome studies have not been conducted in educational settings, and parental awareness of educational intervention options for ADHD appears to be low (Bussing, Gary, Mills, & Garvan, 2007).
Models of chronic illness interpreted this discarding of the patient role as “active-denial” through which illness is opposed by engagement in life activities and restricted communication (Bury, 1991; Williams, 2000), but recent research examining adult adaptation to chronic illness has offered useful alternative perspectives (Kralik, 2002; Paterson, 2001, 2003; Telford, Kralik, & Koch, 2006). Paterson (2001, 2003) suggested a process of shifting perspective. She argued that a shifting perspectives model creates alternative and individualized understandings about why chronically ill individuals exhibit behaviors that might to others seem harmful, uninformed, or ill-advised. Additionally, she emphasized that the experience of illness contains elements of both wellness and illness, with shifts according to whether illness or wellness are in the experiential “foreground.” In other words, the shifting perspectives model illustrated complex dynamics and interactions between individuals with chronic illness and their environments by taking into account people’s situational needs, and seeking to link it to specific life events, and the larger socio-political context. The illness in the foreground perspective focused on loss, burden, and potential destructiveness of the illness, whereas a wellness in the foreground perspective appraised the illness as an opportunity for meaningful change, focusing on the self, not a diseased body, as the source of identity. Although the shifting perspectives model of chronic illness did not directly address adolescent illness experiences, it offered very useful applications for the exploration of their illness career transitions. It suggested the importance of potential contextual stimuli for shifts in the foregrounding of illness or wellness perspectives, rather than focusing exclusively on internal psychological processes of understanding illnesses or role acceptance, in order to better understand processes of access to care.
Whereas models of illness adaptation focused on predictors of internal psychological processes, models of help-seeking aimed to explain decisions to utilize health services. These models have taken a public health perspective, and one of their important functions being to enable detection of disparities in access and quality of care (Snowden, 2003). Several help-seeking models have evolved from Andersen’s Behavioral Model of Health Service Use (Andersen, 1995), with an underlying presumption that an individual needs to first recognize that something is wrong (problem recognition), followed by the decision to seek help, service selection, and service utilization (Eiraldi, 2006). A recent help-seeking model that addressed the complexities of adolescent mental health care use is Pescosolido’s Family Network-Based Model of Access to Child Mental Health Services (see Costello et al., 1998, p. 172 for details of the model). Pescosolido (1991) initially developed a dynamic social network model of mental health service utilization and compliance applicable to adults with mental illness. She emphasized that structural (number, type, and strength of network ties), functional (advice, material aid, emotional support), and cultural characteristics (attitudes and beliefs toward illness and medical care) of network interactions are the key to understanding health and illness behavior. Pescosolido proposed that interaction in social networks is one of the basic mechanisms through which individuals recognize problems, contact health providers, and comply with medical advice. Furthermore, the model has been subsequently adapted to provide a framework within which to organize the many factors that affect children’s access to mental health care and the patterns of that care, referred to as children’s illness careers (Costello et al., 1998). The most fundamental modification was to account for power differences between adults and children in decision making about their own access to care, and for the role of schools in problem recognition and service provision.
Using an adaptation of Pescosolido’s model presented in Figure 1, Bussing et al. (2005) studied parent-reported help-seeking steps for ADHD and identified notable differences in illness careers by child gender and racial background. African American females most commonly had “lay care” careers, in which behavioral problems were handled without professional assistance, whereas Caucasian males were most likely to have “patient” careers, receiving treatment from their pediatricians. Insights gained by the study stimulated further refinement of a help-seeking model for ADHD that distinguished between the occurrence of problem behaviors (e.g., impulsivity, inattention, hyperactivity), problem recognition (not necessarily shared by parents, children and network members), consultation about the problem with relevant network members, interpretation of the problem (e.g., misbehavior; social deviance; normal variation; learning problem), intervention selection consistent with the interpretation (e.g., discipline if considered a misbehavior; no intervention if considered a normal variation; medical care if considered an illness etc.), and outcomes.
Figure 1.
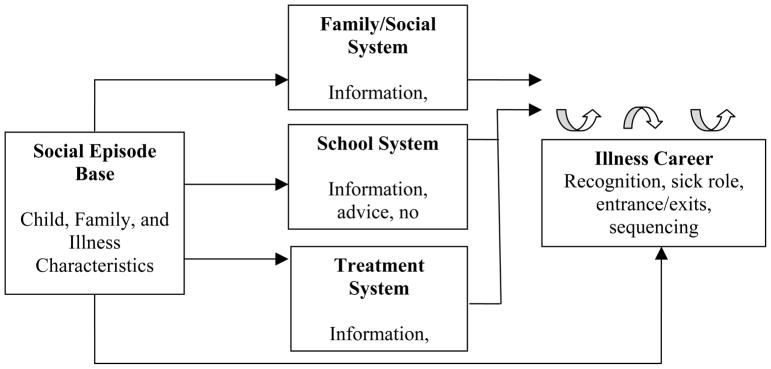
Adapted family network-based access model.
Note. Our model was adapted from Costello, Pescosolido, Angold, and Burns (1998).
The current study was designed to examine the interpersonal experiences, potential consultations, wellness and illness perspectives and stimuli for perspective shifts in a prospective qualitative data collection approach. We sought to maximize opportunities to learn about adolescents’ lived experiences through a qualitative design using multiple informants, reflecting the perspectives of adolescents, their mothers and teachers, in order to understand how their perceptions translate into healthcare-use decisions. In this study, we pursue the following research question: How do daily life events reported by adolescents, their mothers and teachers, and constructed perspectives of these events, shape the illness career transitions of adolescents affected by ADHD?
Methods
This study was embedded in a longitudinal cohort study that has followed public school students at risk for and with ADHD since 1998 (Bussing et al., 2005). We employed a qualitative adaptation of the experience sampling method (QESM) to gather accounts of help-seeking experiences related to ADHD in real time from eight triads of teens with ADHD, their mothers, and one teen-selected teacher (Koro-Ljungberg, Bussing, Williamson, & M’Cormack, in press). QESM enabled immediate, self-reports of events as they occurred in natural settings (Csikszentmihalyi, Rathunde & Whalen, 1993; Kubey, Larson, & Csikszentmihalyi, 1996; Larson & Csikszentmihalyi, 1983). In particular, this participant driven method allowed greater influence of when and what information to report in comparison to traditional, quantitative applications of experience sampling methods where researchers determine reporting intervals using beepers or other devices to request data from participants (Koro-Ljungberg et al.). Informed consent was obtained from all participating adults, as well as assent from the teens, as prescribed by our institutional review board.
We purposefully selected four teens with and four teens without previous ADHD treatment during elementary school years to explore experiences that helped or hindered help-seeking. This selection was based on the assumption that previously treated teens and their parents would have a different type of knowledge and access to care for ADHD that would inform their perspectives and experiences. Four of the teens were girls and four of the teens were boys; four teens were African American and four were Caucasian. After selecting participants based on the criteria as described above, we found that three teens from the untreated group had been identified, since our earlier study phase, as being gifted or high achieving, and all other teens were receiving special education services for learning disabilities. Furthermore, once data collection began, we learned that only one of the four “treated” participants continued to receive ADHD treatment, and during the QESM data collection period, additional transitions occurred.
Our QESM application consisted of a three-month data collection period during which teens and parents were asked to report all important interactive, critical incidents associated with teens’ help-seeking using study-provided cell phones. We defined critical incidents as interactive events (between the teen, parents, teachers, peers, and community members) that occurred related to help-seeking for any problem. Teens and parents were instructed to contact the study team’s answering machine as close as possible to the occurrence of each event. Study team members checked messages daily to ensure the protection of teen participants from possible harm. Participating teachers, in turn, produced secure online reports about critical events that took place at school related to their student’s help-seeking. In order to ensure teen privacy, teachers’ reports consisted of naturally occurring information about teen help-seeking including firsthand accounts as well as interactions teachers had with others related to the teens. Phone calls were transcribed verbatim and teachers’ reports were collected from online. Transcriptions were checked for accuracy by a member of the research team other than the person who originally transcribed the data. A consistent member of the research team followed up with participants once (i.e., teachers and parents) or twice weekly (i.e., teens) with phone calls to confirm the content of their reports, thereby incorporating an on-going member check of data collected in the study design. In addition, feedback forums were conducted with groups of participants (parents and teachers mixed together, teens separately) to ensure findings were representative of their experiences. Participants provided us with direct feedback, shared additional examples, and generated conversations with each other about our major findings and themes. Overall participants agreed with our interpretations of the findings and were very supportive of our preliminary conclusions.
Data from participant self reports (including teens’ and parents’ phone messages and teachers’ online reports) served as primary data and thus were open coded and organized using NVivo (QSR International, 2006). However, data from feedback forums were considered as secondary source and thus were only used to support and clarify our primary findings, not to generate an additional data set to be coded and further analyzed. During open coding of our primary data, all data were coded inductively without any a priori commitments to particular theories. Later critical incident analysis was conducted (Angelides, 2001; Flanagan, 1953; Hektner & Csikszentmihalyi, 2002; Tirri & Koro-Ljungberg, 2002). The critical event analysis, or critical incident method, has been used as a tool for qualitative analysis and aims to identify events that have specific significance or that make a considerable contribution to the lives of the participants.
In this study, critical events served as meaning-making tools for many of our study participants, who naturally constructed their stories around the critical events of their lives. Therefore, we identified the critical events that were significant for our participants, as well as for our study aims and research purposes. Furthermore, we defined critical incidents as events that occurred related to help-seeking for any problem; we distinguished and coded separately the components of the help-seeking model including occurrences of problem behavior, problem recognition, consultation, interpretation of problem, intervention, and outcome. Data reported by participants occasionally included multiple iterations of the same event, when the event was significant enough to have implications for subsequent reporting times. For analysis purposes, incidents were included only one time per participant per incident. Next, incidents reported by each member of the triad were assembled in tables in chronological order within weeks. This enabled the identification of shared events across all participants, meaning events that had been reported by all triad members. This analysis showed that relatively few shared critical events occurred and that each teen was characterized by one commonly perceived problem area. The representativeness of each commonly perceived problem area was checked at the individual level by examining all critical events produced by study participants. With the confirming evidence of a critical event cluster, shared events were established as the focus of attention for that teen, or as events in the foreground. Other events reported by only one or two members of the triad were conceptualized as events in the background. Furthermore, events were interpreted as symbols the triads’ perceptions of teen wellness or illness. We present these conceptions in Figure 2. Next, individual and social elements that influenced the triad-constructed foci were identified.
Figure 2.

Shifting perspectives of illness and wellness among teens with ADHD, their families, and teachers.
Results
Critical events reported by all three members of each triad were remarkably few in number. The maximum number of such shared events in a triad was four and the minimum number was one. These events were important, however, in that they represented a shared focus of the problem the teen was having. Furthermore, shared events among each of our triads served to foreground shared problem events over other problem events reported individually by triad members. Additionally, remarkable transitions became evident. Only one teen continued receiving treatment, three teens had stopped treatment, two teens transitioned from being untreated to being treated and two teens remained untreated. These illness career transitions serve to frame our findings.
Continuing Treatment
Physical aggression foregrounded
In the current sample only one teen girl, referred to as Wendy, who started ADHD treatment during elementary school was still receiving treatment at the beginning of our QESM data collection. In addition to special education services for learning disabilities, she received medication and counseling. However, there was no apparent coordination of treatment planning or communication between different types of treatment providers even though Wendy’s behavior fluctuated notably, and her mother did not consult with treatment providers outside of scheduled sessions. This lack of consultation could be interpreted to mean that by Wendy taking her medication, her mother felt the condition was under control and that fluctuations in Wendy’s behavior were to be expected. Even though Wendy, her mother, and teacher reported events related to physical aggression and resulting suspensions throughout the data collection, it took an extreme event for her mother to seek a change in treatment. Alternatively, mother and Wendy’s desire for living an ordinary life were not seriously challenged until Wendy ran away for three days (see also Kralik, 2002). This shift resulted in a need for changes that enabled better control of ADHD symptoms and the minimalization of long-term social and academic consequences.
More specifically, Wendy herself minimized her role as the aggressor in order to maintain her positive sense of self (see e.g., Telford et al., 2006) and perceived herself as non-deviant and normal whereas Wendy’s mother perceived Wendy as a child with anger issues and “temper tantrums”. Wendy’s teacher, in turn, reported multiple and reoccurring events related to fights, physical aggression such as “punching another student in the face.” In the literature, high rates of verbal and relational aggression among girls with ADHD have been reported (Abikoff et al., 2002; Blachman & Hinshaw, 2002; Ohan & Johnston, 2007). Hay (2000) argued that girls’ antisocial behaviors are associated with increased social marginalization among same sex peers. Additionally, girls’ antisocial behaviors might be one way to become more attractive to certain boys even though that might simultaneously reduce the number of female peers and jeopardize relationships with parents and authorities.
The constructed focus on aggression problems was also influenced by (a) insufficient supervision at school and (b) school discipline policies. Many events reported regarding Wendy’s aggression occurred at school during times when there was less adult supervision (e.g., during class change and at lunch). Wendy’s difficulty controlling her behavior warranted more supervision than would be expected for a typical teen, yet the school was unable to accommodate for this. In addition, the school’s discipline policies highlighted Wendy’s anger issues. As the number of infractions increased, the school followed a progressive discipline policy that featured escalating consequences, regardless of the severity of the infraction. For example, after Wendy had a number of minor offenses (e.g., late for class), she was placed on the “no more timeout list” and less than a week later, Wendy’s teacher reported that Wendy was in in-school suspension as a result of “her no more time-outs. She was tardy to one of her classes.” Thus school intervention and discipline policies were punitive rather than assisting Wendy in determining how to behave appropriately (see e.g., DuPaul & Stoner, 2003). Furthermore, it could be argued that from the deviant teen’s perspective, suspension could be seen as a form of peer reputation enhancement; therefore suspension can become a form of compensation or a motivational goal for antisocial behaviors (Hay, 2000).
Emerging sexuality, being argumentative and disobedient backgrounded
Many critical events that could have been influenced by ADHD symptoms were reported individually by each triad member, and we labeled those events as events in the background. For example, the mother’s perspective on Wendy’s health care needs and her interpretations of Wendy’s life events were partly constructed in the context of adolescent sexuality, culturally and age-inappropriate sexual behavior, a turning point that ultimately moved Wendy toward additional treatment (i.e., counseling at community mental health center). Additionally, Wendy was constructed as argumentative, talking back, and as a child who had difficulty following the rules. Events when Wendy broke the rules at school often resulted in some form of school discipline. For her part, Wendy did not report any events related to problems following the rules, which suggested that Wendy understood that breaking rules was problematic and made her appear deviant. For example, a typical report from Wendy included such things as “I’ve been good today” and “I’m about to do my homework.”
Transition from Treated to Untreated
School attendance and learning problems foregrounded
Three of our teens transitioned from being treated with medication and counseling in elementary school to being untreated in secondary school prior to QESM data collection. All three teens entered treatment, in part, due to what Loe and Feldman (2007) termed academic underachievement or “difficulties learning and applying knowledge” (p. 644), and difficulties with academic performance or “completing classwork or homework” (p. 644). Initially, ADHD diagnoses may have functioned to protect these teens from other stigmatizing events (see Telford et al., 2006), such as leaving general education classrooms for special education classrooms. However, at some point prior to QESM data collection, families discontinued ADHD treatment. Discontinued treatment can be interpreted as a shifting of wellness to the foreground (Telford et al., 2006). Telford and her colleagues (2006) suggested that shifts from focusing on illness to wellness might occur when there is a threat to control, which can be triggered by negative interactions that reinforce feelings of powerlessness or helplessness. The identification of a child as having learning disabilities might trigger such an interaction, especially when parents notice that treatment for ADHD does not cure learning problems (Purdie et al., 2002). Trimble (2001) noted when families are troubled by their children’s difficulties with learning disabilities they may make sense of these problems using explanations, beliefs, and interpretations that exacerbate feelings of distress and helplessness. Thus, having a child with learning disabilities alone can promote perceived threats to parental control. Furthermore, discontinuing treatment for ADHD might reflect a decision to shift the condition of ADHD to the background, allowing the teens to experience a degree of wellness, and leaving them with only one label (e.g., learning disabled) thereby appearing more “normal” (Paterson, 2001, 2003; Telford et al., 2006). Eschewing treatment for ADHD enabled families and teens to gain some measure of control and feelings of wellness, in spite of continued ADHD symptoms. For example, according to one mother their pediatrician concluded that there was a “personality conflict” between his son and one of his teachers and decided not to put his son back on medication for ADHD, an outcome that mother clearly favored. This enabled her son to privilege the social aspects of his life over his patient role, or what Telford and her colleagues (2006) characterized as “asserting self-agency through realizing personal needs and wishes in the life context” (p. 461).
School attendance and learning problems event clusters
All three teens experienced critical event clusters that foregrounded problems related to school. Families and teens who transitioned from treated to untreated perceived that school attendance and learning problems had external explanations and causes. For example, Wes explained that he missed school to stay home and do his “make-up work for those days like two or three weeks ago” when he was absent. Sometimes teenagers’ problems with school attendance were directly related to the school’s discipline policies including speaking with the dean, in-school suspensions, and out-of-school suspensions. For example, Janice, one of the boy’s teachers reported that her student “received a pass to the Dean’s office…When he came back, he told me that he was suspended for three days.” Thus, staying out of trouble so that the teens could be in school and operating within unjust and inflexible institutional policies represented important challenges for teenagers.
Many times teenagers’ critical events were also clustered around learning problems. Some teenagers frequently struggled with assignments, failing to ask for help from their teachers. In addition, other events suggested that even when students put forth effort, they were not academically successful (e.g., receiving poor grades after working hard). One teacher reported that her student “had studied a lot and then when she took the test in class she felt like she knew all the answers…[her] score was a 68 [due to spelling errors]”. External focus of control associated with teenagers’ learning and lack of positive self-image were demonstrated by participants’ reports that they were “bad at reading or math,” which further decreased motivation. Additionally, some parents believed that low grades could be improved through behavioral modification and thus they reported various discipline-related events when teenagers were punished for getting bad grades (e.g., missed a school dance, removal of privileges).
The foregrounding of school absences and learning problems was influenced by complex dynamics among (a) home/school communication, (b) family beliefs about education, and (c) school discipline policies. The influence of home/school communication was experienced by all three triads. Some mothers were very adept at communicating with schools and teachers and thus continuously monitored their teen’s school life and academic progress. For example, the teacher of one teen reported that “her mom wants to start using the daily agenda as a way to check her daughter’s homework assignments as well as her progress.” However, sometimes parent-school communication was one-sided and limited. For example, the school failed to contact one mother directly about her son’s suspensions and assignments to Saturday school and when mother contacted the school to request a change in date for a Saturday school detention no one from the school returned her call. Instead, when her son returned to school on Monday, he found out he was being suspended for missing Saturday school. It became evident that ineffective communication between home and school may have caused additional absences and limited parents’ ability to keep up with important school events and academic progress. Furthermore, Kalyanpur and Harry (2004) argued that the concept of professional hierarchy differentially influences the relationship between parents and schools. They contend that families from “devalued racial/ethnic groups” are “further disenfranchised because they are not participants in the critical discourse surrounding LD because of the persistent belief that their parenting skills are deficient” (Kalyanpur & Harry, 2004, p. 530).
Family beliefs about education also influenced the construction of focus on absences and learning problems. For some parents it was important that teenagers received a regular diploma instead of a special diploma whereas some other parents expressed that they only wanted their teens to be happy at school and they would be comfortable with a special diploma. Thus, family constructions about the value of a regular diploma influenced the foregrounding of the problem focus.
Sleeping problems, disorganization, inattention, and peer problems backgrounded
Constructed foci on school absences and learning problems pushed other ADHD-related symptoms to the background such as (a) sleeping problems, (b) disorganization, (c) interpersonal problems, and (d) attention seeking. Sleeping problems included such things as going to bed too early, staying up too late, and over sleeping for fun activities (e.g., bowling), as well as school. Teens with ADHD may present with significant sleep disturbances, which is “complicated by the fact that adolescence is a developmental period that often includes sleep disturbances” (Wolraich et al., 2005, p. 1735).
Disorganization, in turn, was also frequently reported in data. Students’ ability to be organized fluctuated both at home and at school. In addition, many teens experienced problems with interpersonal relationships that were exemplified by frequent disagreements with family members, teasing peers, and distancing from friends. For example, Taylor noted that “me and my brother was running to shoot the ball, and he hit me in my face with his elbow, so then I pushed him. He pushed me back and I started hitting him in the face”. Finally, some teens were constructed as attention-seeking students by their teachers and parents. These teens requested immediate attention, expressed frustration if they did not get their way, and they often dominated conversations in order to gain attention.
Transitioning from Untreated to Treated
Two girls transitioned from being untreated for ADHD in elementary school to receiving treatment in secondary school, and although they differed in many ways (academic placement, mental disorders in addition to ADHD, socio-demographic characteristics), they had one thing in common – a crisis precipitated treatment. In one case, the event was self-cutting; in the other case, a potential charge for battery and expulsion from school. Prior to a crisis, both families practiced lay care, or self-care, which enabled them to normalize problematic behaviors (Bussing et al., 2006; Telford et al., 2006). Active self care (e.g. religiosity and activation strategies), visible in the critical events reported by these mothers, could be interpreted as adaptive decision-making (Telford et al., 2006). For example, one parent reported that she “prayed for new friends” and sent her teen to participate in Bible study. However, with the advent of violence (i.e., potential battery charge) and self-injurious behavior (i.e., cutting), self-care strategies no longer functioned protectively. Thus, crises that could not be self-managed moved both families toward professional care, perhaps representing a shift toward illness in the foreground. Telford and her colleagues (2006) noted that moving illness in the foreground suggests that families cannot “effectively attend to other aspects of their lives – they are so overwhelmed by illness” (p. 462).
Social, attitude, and aggression problem event cluster
The foregrounding of social problems and attitude/aggression problems was influenced by dynamics among (a) relationship concerns, (b) teachers’ response to students, and (c) caregiver burden. Parents were concerned about their daughter’s relationships and socially acceptable friends. In the case of both girls, teachers’ responses to students also became essential and influential. For example, teachers at times downplayed students’ problems at school or used class structures and teacher’s pedagogy to support learning (see Bost & Riccomini, 2006 for more information on best teaching practice). For example, when a teacher noticed that the student’s grades were slipping, she spoke directly with the student about it. In addition, teachers then coached students on ways to improve their grades, gave them opportunities to earn extra credit, and provided additional time for them to study for exams or complete late homework during class. Our sample also included teachers who continued to use the same methods, regardless of students’ responses to them. For example, a teacher used whiteboards during math lessons to gather responses simultaneously from the group, by asking students to record their answer on the board and hold it up so the teacher could see everyone’s answers. Since our study participant had difficulties with math, she was reluctant to display her incorrect answers, which the teacher interpreted as student having “a very negative attitude.”.
Additionally, the constructed focus on attitude and aggression problems was sometimes influenced by an over-burdened caregiver. Kendall (1998) found that parenting a child with ADHD often exceeds the abilities and coping capacity of parents. Over the course of the data collection period Elizabeth, a single parent, experienced the death of loved ones while taking care of elderly relatives, as well as her daughter, her siblings, and extended family. All of these things took Elizabeth’s focus away from her daughter’s problems. Thus, events reported by Elizabeth were mostly reactive instead of proactive.
Sexual abuse, substance use, self-destruction, and learning problems backgrounded
The focus on social problems pushed some very important concerns to the background including incidents of sexual abuse and experimentation with drugs and alcohol. Additionally, one mother’s awareness of her daughter’s self-injurious behaviors moved the mother to seek treatment unlike other deviant behaviors her daughter had previously exhibited (e.g., substance use, promiscuity). Learning problems were also reported throughout the course of data collection. Even though mothers and teenagers did not report many learning-related events, teachers’ critical event reports captured various learning problems associated with problems taking tests, doing math, or reading fluently.
Remaining Untreated
Two boys in our data set never received treatment for ADHD, and they were high achieving individuals taking advanced classes. Both of their mothers operated with wellness in the foreground, which afforded a focus on the boys’ gifted, high-achieving selves. However as their sons aged, both mothers had concerns about their sons’ behaviors and inquired about the possibility of treatment. One mother was repeatedly assured by her pediatrician that there was nothing to be concerned about, and when another mother had her son evaluated for ADHD at the end of QESM data collection, she was told that his condition was “not a serious problem.”
The literature on giftedness and ADHD treatment has been rife with controversy over the last decade (Goerss, Amend, Web, Web, & Beljan, 2006; Mika, 2006). Goerss et al.have argued that overexcitability, a concept described as being related to giftedness that intensifies and broadens experiences of gifted individuals, is misinterpreted as impulsivity and hyperactivity. These scholars and others have made the case that many gifted students have been inaccurately labeled with ADHD and that further research is needed to identify the extent to which “misdiagnosis” and “over medication” occurs (Gross et al., 2007; Nelson et al., 2006), whereas Mika (2006) contended that overexcitability was actually ADHD and that it was irresponsible not to treat affected students.
Importantly, the health care professionals’ recommendations for these untreated boys were made in light of apparently normal adaptive functioning because of extensive scaffolding by these teens’ families for academic success. Scaffolding, rooted in the work of Vygotsky, is the use of temporary supports to assist students as they work to achieve independent competence in a new or emerging skill (Jamarillo, 1996). For example, parents assisted their teens with breaking long-term assignments into manageable short-term chunks. Parental involvement in teens’ schoolwork was so natural that both mother and son frequently used the pronoun “we” (e.g., “we worked out a plan”). In order for a diagnosis of ADHD to be given, functioning in two areas of life must be impaired (American Psychiatric Association, 1994). In the cases of the two untreated boys, both families, especially the mothers, were proactive and provided scaffolding and support, which allowed for appropriate adaptive behavior and mitigated challenging behavior (Loe & Feldman, 2007). Furthermore, reports from both teachers contained ADHD-related events; however, teacher interpretations of these events did not reflect deviance. Rather, teacher reports illustrated a downplaying of problematic events alongside admiration for the abilities of these young men extolling such things as “he’s at the top of his class” and “he’s so smart.” Thus, potential problems for high-achieving teens with ADHD were accommodated for or minimized by the adults around them.
Homework and social problems foregrounded
One untreated boy constructed himself as an individual who had problems with homework – not the homework itself but the logistics involved in getting the homework done and turned in, or what Loe and Feldman (2007) refer to as academic performance. He reported events when he forgot to bring home the materials he needed, started homework late at night because he was busy with other things or simply procrastinated, and talked in class, which resulted in classwork turning into homework. Furthermore, he recognized when he had problems with homework completion and sometimes he thought of solutions for himself, a form of self-care (Bussing et al., 2006). For example, he alternated homework with other activities to alleviate his boredom with the work.
Various socio-political elements influenced the construction of homework problem focus and included (a) the value the family placed on school, (b) extensive scaffolding by family members, (c) teacher’s protection of gifted boy from stigma, and (d) the teen’s assumption of the “cool pose” (Majors & Billson, 1993). Similar to Reis and her colleagues (2005) who noted that academically talented teens from diverse backgrounds often have families who support and value education, Alexander’s family valued education, and he was expected to succeed in school. In order to meet these expectations Alexander’s mother and her daughters often rescued Alexander from his homework troubles so much that his teacher reported no problems with homework. Additionally, Alexander’s teacher was proactive and protective when it came to this student’s academic success. Her pro-activeness might be partially explained by her awareness of African American gifted students’ underrepresentation in schools, and by the fact that scholars have suggested that teachers play an important part in the identification process, and more importantly, the retention process of African American gifted students (Milner & Ford, 2007). For example, when teacher reported problematic school events, she interpreted those difficulties as a result of Alexander’s “cool pose” (Majors & Billson, 1993) in front of his peers.
In the case of another untreated gifted boy, all members of this triad reported events related to social problems throughout the twelve-week data collection period. The teenager himself described making fun of or teasing other students and being annoyed or unhappy with peers because they would not do what he wanted whereas his mother referred to events related to social difficulties with friends, other family members, and problems with the general public (e.g., making noises at a restaurant). Additionally, the teacher reported socially inappropriate behaviors during class including laughing at other students, as well as punishment the student received for tapping another student on the head after being told not to.
Sleeping and memory problems, impulsivity, hyperactivity, and inattention backgrounded
The concentrated focus on homework problems failed to account for other underlying ADHD-related problems teens were experiencing including (a) sleeping problems, (b) impulsivity, (c) hyperactivity, and (d) inattention. Sleeping problems were reported by both parents and teens including running late for school because of being up so late, staying up late because of taking a nap, and missing the bus due to oversleeping. Teenagers also experienced and described impulsive events such as running through the halls to sign up to be in the same group for a field trip and rushing into things without considering the consequences. Both parents and teachers reported numerous events related to hyperactivity including repetitive drumming, clicking one’s pen, and ball bouncing. In addition to breaking down long-term assignments, parents described events when they eliminated distractions (e.g., turned off the cable during the school week) and looked over teens’ homework to ensure that it was complete and correct. However, this parental assistance and scaffolding often went unseen by teachers who reported that teens’ backpacks and notebooks were organized and that they returned assignments in a timely fashion. Thus, these teens experienced many more ADHD-related symptoms than the focus of their critical event cluster suggested.
Discussion
The experiences of these teens with ADHD, their families, and their teachers offer important insights relevant to both access to care and illness adaptation. Not surprisingly, triad accounts offered different perspectives. During adolescence, greater independence naturally occurs in the home lives of teens. Thus, parents are less aware of all that is happening in the lives of their teens. In addition, during secondary school, teens have multiple teachers for shorter periods of time making secondary teachers less aware of all events in the lives of teens (Wolraich et al., 2005).
Four transition patterns (continuing treatment, stopping treatment, transitioning into treatment, and staying untreated) were evidenced in the shared foci of daily events reported by adolescents, mothers, and teachers. Ongoing illness adaptation also influenced individuals’ decisions to utilize health services. Therefore, careful examinations of structural (network ties), functional (advice, material aid, emotional support), and cultural characteristics (attitudes and beliefs toward illness and medical care) of network interactions was important in understanding health and illness behavior (see Pescosolido’s (1991) illness career model) and help-seeking. The patterns of illness transition evident among our participants supported a model of shifting perspectives of illness and wellness similar to Paterson’s description (2001, 2003).
Although some children may truly outgrow ADHD, this did not appear to explain the experiences of our teen participants, as they continued to exhibit various levels of ADHD symptoms and impairments in functioning. An ADHD diagnosis requires documented functional impairment in two or more settings, not just the appearance of symptoms, yet, the current literature defines successful treatment as a reduction in core symptoms (The MTA Cooperative Group, 1999). For our teens, their level of functioning, rather than ADHD symptoms displayed within school and social settings influenced their illness careers while simultaneously shaping their access to care. In our data it became evident that entering treatment in adolescence was precipitated by crisis, dropping out of ADHD treatment co-existed with learning disabilities, and giftedness predicted late entrance or no entrance into treatment. More specifically, crises experiences were large and influenced the behavioral/social functioning of the teens. These disruptions influenced both family and teen adaptive functioning, which shifted illness into the foreground. Prior to large crisis events, each of the three teens consistently experienced a multitude of ADHD-related symptoms. However, until the crisis arose, symptoms were tolerated and accepted as typical of each teen’s functioning and pushed to the background prompting no change in help-seeking. However, after the crisis, illness was once again shifted to the foreground and AHD symptoms were reinvestigated as possible causes of the crisis.
Treatment for ADHD itself does not cure learning disabilities. Of the five participants with learning disabilities, only one continued ADHD treatment through adolescence. We speculate that the persistence of learning disabilities despite ADHD treatment likely influenced participants’ decisions to stop the ADHD treatment, since it was not seen as helping the child do better in school. Notably though, learning difficulties were the identified problem focus for only one teenager with established LD, whereas for the other cases, the intervention efforts targeted “bad” behavior (i.e., aggression and school attendance problems). Thus, our findings suggested that for students with learning problems, school efforts were concentrated on student behavior rather than on their unique learning needs, something mirrored in the literature. In a recent meta-analysis of inventions for ADHD, Purdie et al. (2002) found few studies examined the effects of school-based interventions on academic achievement and learning. Instead, many studies focused on the behavioral affects of the intervention with the logic being that more time-on-task translates into better educational outcomes; however, evidence suggested that improved behavior did not always lead to improved academic outcomes (Purdie et al.). In addition, events reported in this study suggested that strategies many teachers used did not follow principles of effective instruction (see e.g., Bost & Riccomini, 2006 for exemplary strategies) for children and teenagers with special needs. We can speculate how much more teens with learning difficulties, might benefit if, in addition to a mental health referral for behavior problems, they also had receive more individualized instruction aimed at addressing learning problems.
Our study findings also offered interesting insights about the role of giftedness and parental efforts in shaping illness careers. Three of the four teens who were not treated for ADHD when they were younger were in advanced classes in middle or high school. In all three cases, these teens’ mothers worked very hard to make sure their children succeeded academically. The examples from these mothers provided insights about the potential role of mothers’ laycare and even teen self-care in remediating functional impairment associated with ADHD, thus ameliorating the ADHD to a point that no need for further treatment was detectable. Gifted teen experiences were accompanied by several potential protective factors, namely high academic achievement, absence of conduct or aggression problems, two-parent family households and high SES.
Furthermore, our data suggested that the teachers who worked with these teens viewed their ADHD symptoms in light of their high achievement (Goerss et al., 2006; Mika, 2006; Nelson et al., 2006). Teachers tended to be forgiving of manifestations of what might have been considered deviant classroom behavior in other contexts. Teachers seemed to be unaware of the high level of parental involvement in ensuring academic task completion and often assumed an almost protective role in making sure teens were not labeled (Milner & Ford, 2007). Thus, families and teachers of high-achieving teens with wellness in the foreground focused on the talented and gifted self of the teen. Only a large crisis in the experience of one high-achieving teen caused a shift to illness in the foreground. Taken together, this suggests absent a large crisis, many high achieving or gifted teens and their families have adaptive functioning that facilitates well being.
Study Limitations and Implications for Future Research
An important limitation of this study was that our teen participants represented two extremes – they were all either high achieving or were in special education classes. None of these teens had been classified as such in elementary school. The fact that so many students were now receiving special education services was not surprising especially when academic problems are one of the hallmarks of ADHD. The high concentration of gifted teenagers in our sample may be an artifact of our sampling procedure, or an artifact of the geographical location of our study participants, as the area is known to have a high concentration of gifted students. Furthermore, study findings have to be considered in light of the fact that we required shared events to include teacher perspectives – by necessity, this limited such events to topics a teacher would reasonably be expected to have experiences with. However, teachers’ perspective was essential considering the number of hours teenagers spend in school every weekday. In addition, teachers play an important role in identifying children who need evaluations for ADHD related difficulties.
This qualitative study presented some interesting and consistent patterns related to the illness career of teenagers with ADHD; a study that investigates whether or not these patterns hold true for a larger population of teens seems warranted. Loe and Feldman (2007) have called for extensive research on the kinds of educational interventions that are effective for students with ADHD, a call that we echo. In particular, we suggest that the efficacy of academic interventions for students with learning disabilities and ADHD be explored. Our findings also indicated that families can and do play an important role in school success, particularly when it comes to high-achieving students. An exploratory study of parents who are skilled at improving the adaptive academic functioning of their children might provide insight for other families who are less successful. This might result in a form of families helping other similarly situated families. Finally, our data suggested that ADHD care in elementary school years did not necessarily improve teen’s and parents’ understanding of the developmental course of ADHD and its likely presentation in adolescence, which raises questions about how to improve the ADHD education that is supposed to be provided as part of routine care (American Academy of Pediatrics, 2007). Furthermore, our findings clearly documented that “continuing ADHD treatment” into adolescence did not necessarily imply “met treatment need” and thus emphasized the need to utilize more complex approaches for studies addressing access to care or quality standards (Rutter, 1987; Zima et al., 2005).
Acknowledgments
This research was supported by a grant from the National Institute of Mental Health to Regina Bussing and Mirka Koro-Ljungberg (R01 MH57399). The authors wish to thank Dana Mason, B.A., and Fredline M’Cormack, Ph.D., for help with the data collection, and families and teachers whose participation made the study possible.
Biographies
Pamela Williamson, Ph.D., is an assistant professor of Special Education at the University of Cincinnati in Cincinnati, Ohio, USA.
Mirka Koro-Ljungberg, Ph.D., is an associate professor of Educational Psychology at the University of Florida in Gainesville, Florida, USA.
Regina Bussing, M.D., M.S.H.S., is a professor of Child and Adolescent Psychiatry at the University of Florida in Gainesville, Florida, USA.
Contributor Information
Pamela Williamson, Email: Pamela.Williamson@uc.edu, University of Cincinnati, Cincinnati, Ohio, USA, Edwards Center (One), 45-51 Corry Boulevard, Room 4150H, Cincinnati, OH 45221, 513.556.9137, 513.556.1581 fax, ML-0022.
Mirka Koro-Ljungberg, University of Florida, Gainesville, Florida, USA, 1414 Norman Hall PO BOX 117047, Gainesville, FL 32611.
Regina Bussing, University of Florida, Gainesville, Florida, USA, 1600 SW Archer Rd, Rm HD-G-003, PO BOX 100157, Gainesville, FL 32610-0157
References
- Abikoff HB, Jensen PS, Arnold LLE, Hoza B, Hechtman L, Pollack S, et al. Observed classroom behavior of children with ADHD: Relationship to gender and comorbidity. Journal of Abnormal Child Psychology. 2002;30(4):349–359. doi: 10.1023/a:1015713807297. [DOI] [PubMed] [Google Scholar]
- American Academy of Pediatrics. Practice parameters for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry. 2007;46:894–921. doi: 10.1097/chi.0b013e318054e724. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4. Washington, DC: American Psychiatric Association; 1994. edition (DSM-IV) [Google Scholar]
- Andersen RM. Revisiting the behavioral model and access to medical care: Does it matter? Journal of Health and Social Behavior. 1995;36(1):1–10. [PubMed] [Google Scholar]
- Antshel KM, Faraone SV, Stallone K, Nave A, Kaufmann FA, Doyle A, et al. Is attention deficit hyperactivity disorder a valid diagnosis in the presence of high IQ? Results from the MGH Longitudinal Family Studies of ADHD. Journal Child Psychology Psychiatry. 2007;48(7):687–694. doi: 10.1111/j.1469-7610.2007.01735.x. [DOI] [PubMed] [Google Scholar]
- Angelides P. The development of an efficient technique for collecting and analyzing qualitative data: The analysis of critical incidents. International Journal of Qualitative Studies in Education. 2001;14(3):429–442. [Google Scholar]
- Biederman J, Faraone S, Milberger S, Guite J, Mick E, Chen L, et al. A prospective 4-year follow-up study of attention-deficit hyperactivity and related disorders. Archives of General Psychiatry. 1996;53(5):437–446. doi: 10.1001/archpsyc.1996.01830050073012. [DOI] [PubMed] [Google Scholar]
- Blachman DR, Hinshaw SP. Patterns of friendship among girls with and without attention-deficit/hyperactivity disorder. Journal of Abnormal Child Psychology. 2002;30(6):625–640. doi: 10.1023/a:1020815814973. [DOI] [PubMed] [Google Scholar]
- Bost LW, Riccomini PJ. Effective instruction: An inconspicuous strategy for dropout prevention. Remedial and Special Education. 2006;27:301–311. [Google Scholar]
- Bury MR. The sociology of chronic illness: A review of research and prospects. Sociology of Health and Illness. 1991;13(4):451–468. [Google Scholar]
- Bussing R, Gary FA, Mills TL, Garvan CW. Cultural variations in parental health beliefs, knowledge, and information sources related to attention-deficit/hyperactivity disorder. Journal of Family Issues. 2007;28(3):291–318. [Google Scholar]
- Bussing R, Koro-Ljungberg M, Gary F, Mason D, Garvan CW. Exploring help-seeking for ADHD symptoms: A mixed-methods approach. (2005) Harvard Review of Psychiatry. 2005;13(2):85–101. doi: 10.1080/10673220590956465. [DOI] [PubMed] [Google Scholar]
- Bussing R, Koro-Ljungberg ME, Williamson P, Gary FA, Garvan CW. What “Dr. Mom” ordered: A community-based exploratory study of parental selfcare responses to children’s ADHD symptoms. Social Science and Medicine. 2006;63:871–882. doi: 10.1016/j.socscimed.2006.03.014. [DOI] [PubMed] [Google Scholar]
- Bussing R, Zima BT, Mason D, Hou W, Garvan CW, Forness S. Use and persistence of pharmacotherapy for elementary school students with attention-deficit/hyperactivity disorder. Journal of Child and Adolescent Psychopharmacology. 2005;15(1):78–87. doi: 10.1089/cap.2005.15.78. [DOI] [PubMed] [Google Scholar]
- Charney R. Teaching children to care: Classroom management for ethical and academic growth, K-8. Turner Falls, MA: Northeast Foundation for Children; 2002. [Google Scholar]
- Costello EJ, Pescosolido BA, Angold A, Burns BJ. A family network-based model of access to child mental health services. Research in Community and Mental Health. 1998;9:165–190. [Google Scholar]
- Csikszentmihalyi M, Rathunde K, Whalen S. Talented teenagers. New York: Cambridge University Press; 1993. [Google Scholar]
- DuPaul GJ, Stoner GD. ADHD in the schools: Assessment and intervention strategies. 2. New York: Guilford Press; 2003. [Google Scholar]
- Eiraldi RB, Mazzuca LB, Clarke AT, Power TJ. Service utilization among ethnic minority children with ADHD: A model of help-seeking behavior. Administration and Policy in Mental Health. 2006;33(5):607–622. doi: 10.1007/s10488-006-0063-1. [DOI] [PubMed] [Google Scholar]
- Flanagan J. The critical incident method. Pittsburgh, PA: American Institute for Research and University of Pittsburgh; 1953. [Google Scholar]
- Fletcher JM, Shaywitz SE, Shaywitz BA. Comorbidity of learning and attention disorders: Separate but equal. Pediatric Clinics of North America. 1999;46(5):885–897. doi: 10.1016/s0031-3955(05)70161-9. [DOI] [PubMed] [Google Scholar]
- Frazier TW, Demaree HA, Youngstrom EA. Meta-analysis of intellectual and neuropsychological test performance in attention-deficit/hyperactivity disorder. Neuropsychology. 2004;18(3):543–555. doi: 10.1037/0894-4105.18.3.543. [DOI] [PubMed] [Google Scholar]
- Goerss J, Amend ER, Webb JT, Webb N, Beljan P. Comments on Mika’s critique of Hartnett, Nelson, and Rinn’s Article, “Gifted or ADHD? The Possibilities of Misdiagnosis. Roeper Review. 2006;28:249–251. [Google Scholar]
- Gross CM, Rinn AN, Jamieson KM. Gifted adolescents’ overexcitabilities and self-concepts: An analysis of gender and grade level. Roeper Review. 2007;29:240–248. [Google Scholar]
- Hansen DL, Hansen EH. Caught in a balancing act: Parents’ dilemmas regarding their ADHD child’s treatment with stimulant medication. Qualitative Health Research. 2006;16(9):1267–1285. doi: 10.1177/1049732306292543. [DOI] [PubMed] [Google Scholar]
- Hay I. Gender self-concept profiles of adolescents suspended from high school. Journal of Child Psychology & Psychiatry & Allied Disciplines. 2000;41(3):345. [PubMed] [Google Scholar]
- Hektner J, Csikszentmihalyi M. The experience sampling method: Measuring the context and content of lives. In: Bechtel R, Churchman A, editors. Handbook of Environmental Psychology. New York: John Wiley & Sons; 2002. pp. 233–243. [Google Scholar]
- Jaramillo J. Vygotsky’s sociocultural theory and contributions to the development of constructivist curricula. Education. 1996;117(1):133–140. [Google Scholar]
- Jensen PS, Arnold LE, Swanson JM, Vitiello B, Abikoff HB, Greenhill LL, et al. 3-Year Follow-up of the NIMH MTA Study. Journal for the American Academy of Child and Adolescent Psychiatry. 2007;46(8):989–1002. doi: 10.1097/CHI.0b013e3180686d48. [DOI] [PubMed] [Google Scholar]
- Kalyanpur M, Harry B. Impact of the social construction of LD of culturally diverse families: A response to Reid and Valle. Journal of Learning Disabilities. 2004;37:530–533. doi: 10.1177/00222194040370060801. [DOI] [PubMed] [Google Scholar]
- Kendall J. Outlasting disruption: The process of reinvestment in families with ADHD children. Qualitative Health Research. 1998;8:839–857. doi: 10.1177/104973239800800609. [DOI] [PubMed] [Google Scholar]
- Koro-Ljungberg M, Bussing R, Williamson P, M’Cormack F. Reflecting on the experience sampling method in the qualitative research context: Focus on knowledge production and power during the data collection process. Field Methods in press. [Google Scholar]
- Kralik D. The quest for ordinariness: Transition experienced by midlife women living with chronic illness. Journal of Advanced Nursing. 2002;39(2):146–154. doi: 10.1046/j.1365-2648.2000.02254.x. [DOI] [PubMed] [Google Scholar]
- Kubey R, Larson R, Csikszentmihalyi M. Experience sampling method applications to communication research questions. Journal of Communication. 1996;46(2):99–120. [Google Scholar]
- Larson R, Csikszentmihalyi M. The experience sampling method. In: Reis H, editor. Naturalistic approaches to studying social interaction. San Francisco: Jossey-Bass; 1983. pp. 41–56. [Google Scholar]
- LeFever GB, Villers MS, Morrow AL, Vaughn ES., III Parental perceptions of adverse educational outcomes among children diagnosed and treated for ADHD: A call for improved school/provider collaboration. Psychology in the Schools. 2005;39(1):63–71. [Google Scholar]
- Loe IM, Feldman HM. Academic and educational outcomes of children with ADHD. Journal of Pediatric Psychology. 2007;32:643–654. doi: 10.1093/jpepsy/jsl054. [DOI] [PubMed] [Google Scholar]
- Majors RG, Billson JM. Cool pose: The dilemma of black manhood in America. New York: Simon and Shuster Adult Publishing Group; 1993. [Google Scholar]
- Meaux JB, Hester C, Smith B, Shoptaw A. Stimulant medications: A trade-off? The lived experience of adolescents with ADHD. Journal for Specialists in Pediatric Nursing. 2006;11(4):214–226. doi: 10.1111/j.1744-6155.2006.00063.x. [DOI] [PubMed] [Google Scholar]
- Mick E, Faraone SV, Biederman J. Age-dependent expression of attention-deficit/hyperactivity disorder symptoms. Psychiatric Clinics of North America. 2004;27(2):215–224. doi: 10.1016/j.psc.2004.01.003. [DOI] [PubMed] [Google Scholar]
- Mika E. Research commentary point-counterpoint: Diagnosis of giftedness and ADHD. Roeper Review. 2006;28(4):237–242. [Google Scholar]
- Milner HR, Ford DY. Cultural considerations in the underrepresentation of culturally diverse elementary students in gifted education. Roeper Review. 2007;29(3):166–173. [Google Scholar]
- The MTA Cooperative Group. Multimodal treatment study of children with ADHD: A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry. 1999;(56):1073–1086. doi: 10.1001/archpsyc.56.12.1073. [DOI] [PubMed] [Google Scholar]
- Nelson JM, Rinn AN, Hartnett DN. The possibility of misdiagnosis of giftedness and ADHD still exists: A response to Mika. Roeper Review. 2006;28(4):243–248. [Google Scholar]
- Office of Special Education. A clarification of state and local responsibilities under federal law to address the needs of children with attention deficit disorders. OSERS News in Print. 1992;4(3):27–29. [Google Scholar]
- Ohan JL, Johnston C. What is the social impact of ADHD in girls? A multi-method assessment. Journal of Abnormal Child Psychology. 2007;35(2):239–250. doi: 10.1007/s10802-006-9076-1. [DOI] [PubMed] [Google Scholar]
- Paterson BL. The shifting perspectives model of chronic illness. Journal of Nursing Scholarship. 2001;33(1):21–26. doi: 10.1111/j.1547-5069.2001.00021.x. [DOI] [PubMed] [Google Scholar]
- Paterson BL. The koala has claws: Applications of the shifting perspectives model in research of chronic illness. Qualitative Health Research. 2003;13(7):987–994. doi: 10.1177/1049732303251193. [DOI] [PubMed] [Google Scholar]
- Pescosolido BA. Illness careers and network ties: A conceptual model of utilization and compliance. Advances in Medical Sociology. 1991;2:161–184. [Google Scholar]
- Purdie N, Hattie J, Carroll A. A review of the research on interventions for attention deficit hyperactivity disorder: What works best? Review of Educational Research. 2002;72(1):61–99. [Google Scholar]
- QSR International. NVivo (Version 7) [Computer software] Cambridge, MA: QSR International; 2006. [Google Scholar]
- Rasmussen P, Gillberg C. Natural outcome of ADHD with developmental coordination disorder at age 22 years: a controlled, longitudinal, community-based study. Journal for the American Academy of Child and Adolescent Psychiatry. 2000;39:1424–1431. doi: 10.1097/00004583-200011000-00017. [DOI] [PubMed] [Google Scholar]
- Reis SM, Colbert RD, Hebert TP. Understanding resilience in diverse, talented students in an urban high school. Roeper Review. 2005;27(2):110–120. [Google Scholar]
- Rutter M. Psychosocial resilience and protective mechanisms. American Journal of Orthopsychiatry. 1987;57(3):316–331. doi: 10.1111/j.1939-0025.1987.tb03541.x. [DOI] [PubMed] [Google Scholar]
- Shaywitz BA, Fletcher JM, Shaywitz SE. Defining and classifying learning disabilities and attention-deficit/hyperactivity disorder. Journal of Child Neurology. 1995;10(Supplemental):S50–57. doi: 10.1177/08830738950100S111. [DOI] [PubMed] [Google Scholar]
- Snowden LR. Bias in mental health assessment and intervention: Theory and evidence. American Journal of Public Health. 2003;93(2):239–243. doi: 10.2105/ajph.93.2.239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sonuga-Barke EJ. Causal models of attention-deficit/hyperactivity disorder: From common simple deficits to multiple developmental pathways. Biological Psychiatry. 2005;57(11):1231–1238. doi: 10.1016/j.biopsych.2004.09.008. [DOI] [PubMed] [Google Scholar]
- Telford K, Kralik D, Koch T. Acceptance and denial: Implications for people adapting to chronic illness: Literature review. Journal of Advanced in Nursing. 2006;55:457–464. doi: 10.1111/j.1365-2648.2006.03942.x. [DOI] [PubMed] [Google Scholar]
- Tirri K, Koro-Ljungberg M. Critical incidents in the lives of gifted female Finnish scientists. The Journal of Secondary Gifted Education. 2002;13(4):151–163. [Google Scholar]
- Trimble S. Making sense in conversations about learning disabilities. Journal of Marital and Family Therapy. 2001;27:473–486. doi: 10.1111/j.1752-0606.2001.tb00341.x. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Education. IDEA proposed regulations, 42 fed. Reg. 55026, 55115, to be codified at 34 c.F.R. §§ 300.660–662 2004 [Google Scholar]
- Williams SJ. Chronic illness as biographical disruption or biographical disruption as chronic illness? Reflections on a core concept. Sociology of Health and Wellness. 2000;22(1):40–67. [Google Scholar]
- Wolraich ML, Wibbelsman CJ, Brown TE, Evans SW, Gotlieb EM, Knight JR, et al. Attention-deficit/hyperactivity disorder among adolescents: A review of the diagnosis, treatment, and clinical implications. Pediatrics. 2005;115(6):1734–1746. doi: 10.1542/peds.2004-1959. [DOI] [PubMed] [Google Scholar]
- Zima BT, Hurlburt MS, Knapp P, Ladd H, Tang L, Duan N, et al. Quality of publicly-funded outpatient specialty mental health care for common childhood psychiatric disorders in California. Journal for the American Academy of Child and Adolescent Psychiatry. 2005;44(2):130–144. doi: 10.1097/00004583-200502000-00005. [DOI] [PubMed] [Google Scholar]