

Abstract
Background:
Cysts of the skin are one of the commonly excised specimens in the surgical outpatient department. A majority of them being clinically diagnosed as sebaceous cysts, their true nature is only discernible on histopathological examination. Closer examination of the type of keratinization involved will throw light into the exact nature of the cyst. Trichilemmal or Pilar cyst is one such entity, which presents in both a non-neoplastic and neoplastic form.
Aims:
The present retrospective observational study was undertaken to find out the incidence of these cysts in surgical pathology practice in a rural hospital and to enlist the various morphological forms that these cysts may take.
Materials and Methods:
The histopathology files were reviewed for a period of 6 years for cases coded as pilar cyst.
Results:
A total of eight cases (5.75%) were identified, which showed features of trichilemmal differentiation. A single case each of proliferating trichilemmal cyst and malignant proliferating trichilemmal tumors were noted. Most of the cases were seen among females on the scalp.
Conclusions:
Trichilemmal tumor is an uncommon histopathological entity. Many of these lesions may be mistakenly diagnosed due to lack of recognition of the unique type of keratinization.
Keywords: Malignant pilar tumor, Pilarcyst, Proliferating pilar tumor, Proliferating trichilemmal cyst
Introduction
Cystic lesions of the skin are commonly encountered in surgical practice with sebaceous cyst being the most common clinical diagnosis. Much confusion and misconception exist among surgeons regarding the exact nature and origin of these lesions, with the cyst contents on casual observation appearing to be sebaceous in nature. McGavran and Binnington made a detailed study of all the characteristics of “sebaceous cysts” under the electron microscope. They concluded that those cysts wherein keratinization occurred without keratohyaline granules, as in the cases of the cortex of hair and nail, were derived from the piliary apparatus, particularly the external root sheath and hence should be called as pilar cysts. Pinkus, while accepting the pilar theory, identified the follicular isthmus of the external root sheath of the hair follicle as the exact origin of these pilar cysts and suggested the name “trichilemmal cyst.”[1,2]
Pilar cysts are common, occurring in 5-10% of the population. They occur preferentially in areas with dense hair follicle concentrations; therefore, 90% occur in the scalp. They are the most common cutaneous cyst in the scalp and the second most common cyst in the head and neck region. Pilar cysts are almost always benign, with malignant transformation occurring rarely. In 2% of cases, single or multiple foci of proliferating cells lead to proliferating tumors, often called proliferating trichilemmal cysts or tumors. Proliferating trichilemmal cysts grow rapidly and may arise de novo also. Although biologically benign, they may be locally aggressive, becoming large and ulcerated. Rarely, malignant transformation leads to distant metastasis. No absolute clinical criteria can distinguish a benign proliferating trichilemmal cyst from a malignant proliferating trichilemmal cyst. Hence the entire lesion must undergo histopathological examination. A variety of diagnostic terms for proliferating trichilemmal tumor have been appended in the literature during the past four decades reflecting dissimilar interpretations of the biologic nature of the lesion.[3–9]
The present study was undertaken to study the various morphological forms of pilar cysts encountered in surgical pathology practice at a rural hospital over a period of 6 years.
Materials and Methods
The histopathology consultation files of the Department of Pathology were reviewed for a period of 6 years between January 2005 and December 2010. Cases coded as pilar cyst, trichilemmal cyst, proliferating pilar or trichilemmal cyst and malignant proliferating pilar or trichilemmaltumor and accessioned in the aforementioned period were retrieved from our aggregated institutional files. The paraffin embedded and H and E, stained histopathology slides were reviewed and the relevant histomorphological were noted. The relevant clinical details available from the histopathological examination request forms were also noted.
Results
During the period January 2005 to December 2010, a total of 139 cysts in relation to the skin were excised. Upon review of the cases, a total of eight cases (5.75%) were identified during the above period showing features of trichilemmal differentiation. Six cases were trichilemmal cysts; one was a proliferating trichilemmal cyst and the last was a malignant proliferating trichilemmal tumor. Most of the cases were seen among females. Except for a single case of trichilemmal cyst which occurred on the face of a 12-year-old female, rest of the cases were noted on the scalp of middle aged to elderly individuals. The smallest lesion was a trichilemmal cyst of 0.3cm diameter and the largest lesion was a proliferating trichilemmal cyst of 5 × 3cm dimension. In two cases, the trichilemmal cysts were multiple with as many as four cysts in a case [Table 1]. A history of removal of similar cysts 3 years back with reappearance of multiple trichilemmal cysts on the scalp was obtained in a middle-aged female. All the cases were clinically diagnosed as sebaceous cysts with the exception of the malignant proliferating trichilemmal tumor, which was clinically suspected to be a squamous cell carcinoma because of its large size, exophytic nature of the growth and the ulceration of the overlying skin. Incidentally one case of trichilemmal cyst was associated with scleroderma.
Table 1.
Spectrum of pilar cysts

Discussion
An enclosed space lined by epithelium containing fluid or other material within a tissue is called a cyst. Cysts in relation to skin are classified on the basis of their pathogenesis. Those related to or derived from the dermal appendages are common compared to developmental cysts which result from persistence of vestigial remnants. Trichilemmal cyst is one such appendageal cyst.[3,5,8,9]
Appendageal tumors are neoplasms whose differentiation is towards one or more of the adnexal structures of the skin. Proliferating trichilemmal tumor is a solid cystic neoplasm that shows differentiation similar to that of the isthmus of the hair follicle.[6,7] Even though both trichilemmal cyst and proliferating trichilemmal cyst show trichilemmal type of keratinization and can occur together, one is essentially a cyst and other a neoplastic proliferation. Trichilemmal cyst is usually a solitary intradermal or sub cutaneous lesion. They are clinically indistinguishable from epidermal cysts though being less common than them. It is commonly found on the scalps of females. They are easily enucleable with no punctum in contrast to epidermal cysts.[3,5,8,10,11] Most of the cases in our study were noted on the scalp of middle aged females. Two cases of multiple trichilemmal cysts were also noted.
Grossly, they are firm smooth walled, cream white cysts with sectioned surface showing cream white semi solid cheesy contents.
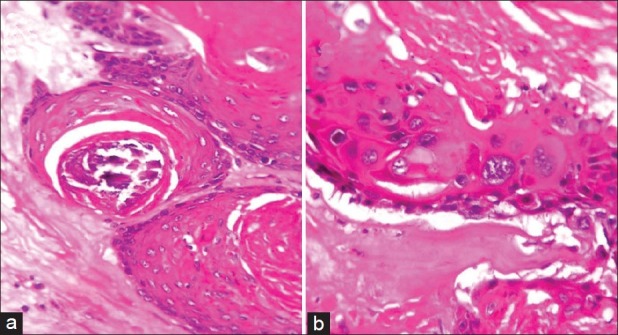
Microscopically these cysts are lined by stratified squamous epithelium. There are no distinct intercellular bridges visible among the epithelial cells and they show a distinct peripheral palisading. Individual cells increase in bulk and vertical diameter towards the lumen. Cells close to the cystic cavity are swollen and filled with pale cytoplasm. The keratinization is abrupt with no intervening granular layer [Figure 1a]. The cyst contains homogeneous eosinophilic material unlike the lamellated keratin flakes in an epidermal cyst[Figure 1b]. Cholesterol clefts are common in the keratinous material with the cyst content being calcified in 1/4th of cases. Cyst ruptures with considerable foreign body giant cell reaction. Immunohistochemistry is positive for keratin K10 and K17.[5] All the cases in our study fulfilled the classical histomorphological features as described above.
Figure 1.

(a) Trichilemmal cyst showing abrupt trichilemmal type of keratinisation.(b) Epidermal cyst with granular layer. H and E, ×10
Polarized microscopy reveals perpendicularly oriented bundles of tonofibrils in the lining epithelial cells. There is an abrupt loss of cytoplasmic organelles in the anucleate cells.[3,5] The keratinization in these cysts is analogous to that which takes place in the outer root sheath of the hair or trichilemmal.[3] Proliferating trichilemmal tumor is a solid cystic neoplasm that shows trichilemmal differentiation similar to that of the isthmus of hair follicle. This tumor has been called by various names in literature like epidermoid carcinoma in sebaceous cyst, sub epidermal acanthoma, proliferating epidermoid cyst, invasive hair matrix tumor of the scalp, trichochlamydocarcinoma, giant hair matrix tumor, proliferating trichilemmal cyst, proliferating pilar cyst, proliferating follicular cystic neoplasm, proliferating trichilemmal cystic squamous cell carcinoma and proliferating isthmica cystic carcinoma.[4–8]
The lesion was first described by Wilson Jones as a proliferating epidermoid cyst. Similar to trichilemmal cyst, proliferating trichilemmal tumor has a predilection for the scalp in elderly females. Face, trunk, back and forehead are the other common sites in that order.[5,7] These tumors present as solitary, multilobular, large, exophytic masses. Multiple lesions are rare and they can arise within a naevus sebaceous. Lesions can range in size from 2 cm to 10 cm on an average with exotic case of a large 25 cm tumor also on record.[7]
The histopathology of these tumors extends along a spectrum with trichilemmal cyst having minimal epithelial proliferation at one end and gross epithelial hyperplasia with minimally cystic areas mimicking a squamous cell carcinoma at other end.[7,12–16] One end of the spectrum shows on histopathological examination a well circumscribed solid and cystic neoplasm involving dermis and sometimes subcutaneous tissue. There is lobular proliferation of squamous cells with prominent epithelial infoldings into the cyst lumen. Peripheral palisading of small basaloid cells arranged along thick vitreous membrane formation is noted focally. These cells differentiate towards larger keratinocytes with abundant eosinophilic cytoplasm. There is abrupt trichilemmal keratinization. The compact eosinophilic keratin thus formed can show areas of dystrophic calcification and cholesterol cleft formation. The neoplastic cells are monomorphic with insignificant cytologic atypia and rare mitoses. The nests of the squamous cells can be seen extending into the adjacent connective tissue, but the proliferation of cells occurs mostly inwards into the cyst. Remnants of trichilemmal cysts can be seen at one end.[5,7,12]
One such tumor was seen in our consultation. This was a skin covered large multiloculated cyst of 5 × 3cm dimension excised from the scalp of a 60-year-old male. The cysts were filled with viscous material with the septae between adjacent lobules showing grey white nodular areas with yellowish white specks. Cyst lining was predominantly smooth with focal trabeculations and focal nodular grey white areas [Figure 2a]. Histopathological sections from the above mass showed a well circumscribed dermal lesion composed of variably sized lobules of squamous epithelium exhibiting abrupt trichilemmal keratinization. Foci of calcification and giant cell reaction to the keratin were also noted [Figure 2b].
Figure 2.

(a) Skin covered large multiloculated cyst filled with viscous material with intervening grey white nodular areas. (b) Lobules of squamous epithelium showing trichilemmal keratinisation. H and E, ×10
At the other end of the spectrum is an invasive growth which is seen extending beyond the confines of the cyst wall. There is an extensive cellular atypia with appreciable nuclear pleomorphism. There is high mitotic activity with focal areas showing necrosis. There is an invasion into the adjacent structures with stromal desmoplasia. Sometimes a spindle cell carcinomatous area can also be seen. This end of the spectrum has been called the malignant proliferating trichilemmal tumor.[5,7,17–21]
The case diagnosed histopathologically as a malignant proliferating trichilemmal tumor was a nodular grey white exophytic growth excised from the scalp of a 45-year-old female. Clinical examination showed no regional lymphadenopathy. The growth was partly covered with skin and showed central ulcerated area and sectioned surface was predominantly solid, vaguely lobulated and focally displaying calcified spots [Figure 3]. Sections from the above lesion showed a mostly well circumscribed lobular proliferation of squamous epithelial cells showing abrupt trichilemmal type of keratinization with focal areas showing epidermoid type keratinization. Dystrophic calcification and giant cell reaction to the keratin were also evident [Figure 4a]. The epithelial cells in most areas showed moderate to severe nuclear atypia with some nuclei appearing to be giant sized and irregularly contoured with prominent nucleoli. Atypical mitotic figures were also noted in these proliferating islands as also individual cell keratinization [Figure 4b]. Few areas showed epithelial cells with clear cytoplasm. The stroma adjacent to these lobules showed extensive desmoplasia, focal invasion and chronic inflammatory reaction. Small foci of benign appearing typical pilar cysts were also seen in the tumor. The overlying skin showed no morphological abnormalities.
Figure 3.

Exophytic skin covered growth with central ulceration
Figure 4.
(a) Lobules of proliferating squamous epithelium with abrupt trichilemmal keratinisation and dystrophic calcification of keratin. H and E, ×10. (b) Moderate to severe nuclear atypia in the squamous epithelial cells lining the cyst. H and E, ×40
Seventy six cases of proliferating trichilemmal tumors were reviewed by Jay Ye and his co-workers and they proposed that these tumors can be stratified into three groups based on tumor silhouette, degree of nuclear atypia, mitotic activity, necrosis and perineural or angiolymphatic invasion. Group 1 tumors are considered benign. Group 2 tumors have a potential for locally aggressive growth and Group 3 tumors having metastatic potential. Groups 2 and 3 were considered to be low and high grades of malignancy among proliferating trichilemmal tumors of the skin.[17] Most cases of proliferating trichilemmal tumors pursue a favorable clinical course and surgical excision is curative. Malignant transformation is indicated by high proliferative activity and DNA aneuploidy. Lymph node metastasis at the time of presentation of malignant proliferating trichilemmaltumor has been reported in literature.[7,20,21]
The important differential diagnoses for a proliferating trichilemmal tumor are trichilemmal cyst, proliferating epidermoid or infundibular cyst and trichilemmal carcinoma. Although a trichilemmal cyst can be seen sometimes in association with a proliferating trichilemmal tumor, the lesion by itself is not a neoplasm. Also it lacks the multilobular architecture of its neoplastic counterpart. Proliferating epidermoid cyst is most common in the anogenital region in male patients. Morphologically they show a cystic cavity lined by stratified squamous epithelium with infundibular keratinization. Trichilemmal carcinoma is a lesion commonly presenting as a slow growing epidermal papule, indurated plaque, or nodule that may ulcerate on the face or ears. Histologically these tumors are composed predominantly of cytologically atypical clear cells resembling outer root sheath. These cells have prominent cytologicatypia with foci of pilar type keratinization.[3,5,7]
Malignant transformation of an epidermal inclusion cyst is uncommon and few such cases have been reported in literature which may be confused for a proliferating trichilemmal tumor. This highlights the importance of examining all cysts of the skin however benign they may appear clinically to avoid any misdiagnosis.[22] At times, clinically these cysts may become tender and inflamed. When these cysts rupture, they evoke inflammation in the surrounding tissue. Only few reports in literature have addressed the immunologic nature of this reaction. The pathologic changes observed in these cysts could be triggered by (1) cyst rupture with its accompanying inflammation; or (2) by the balance between matrix metalloproteinases and their inhibitors. Furthermore, the adjacent adipocytes may be releasing adiponectin which may regulate the inflammatory responses in the area.[23]
In summary, it is seen that trichilemmal tumor is an uncommon histopathological entity. Without paying closer attention to the trichilemmal type of keratinization, many of these lesions may be mistakenly diagnosed as squamous-cell carcinomas. It is imperative that every cyst excised from the skin should be closely studied, especially the larger lobulated masses, although the clinical diagnosis may be an innocuous sounding “sebaceous cyst!!!”
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Chandrasekaran V, Parkash S, Raghuveer CV. Epidermal cysts: A- clinicopathological and biochemical study. Postgrad Med J. 1980;56:823–7. doi: 10.1136/pgmj.56.662.823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Warvi WN, Gates O. Epithelial cysts and cystic tumors of the skin. Am J Pathol. 1943;19:765–83. [PMC free article] [PubMed] [Google Scholar]
- 3.Kirkham N. Tumors and cysts of the epidermis. In: Elder DE, Elenitsas R, Johnson BL, Murphy GF, editors. Lever's Histopathology of the skin. 9th ed. Philadelphia: Lippincott Williams and Wilkins; 2005. pp. 814–6. [Google Scholar]
- 4.Rosai J. Rosai and Ackerman's surgical pathology. 9th ed. Vol. 1. St Louis: Mosby; 2004. pp. 151–3. [Google Scholar]
- 5.Weedon D. Skin pathology. 2nd ed. Edinburgh: Churchill Livingstone; 2002. pp. 504–7. [Google Scholar]
- 6.Klein W, Chan E, Seykora JT. Tumors of the epidermal appendages. In: Elder DE, Elenitsas R, Johnson BL, editors. Lever's Histopathology of the Skin. 9th ed. Philadelphia: Lippincott Williams and Wilkins; 2005. pp. 882–6. [Google Scholar]
- 7.Kaddu S, Requena L. Malignant tumors with follicular differentiation. In: Le Boit PE, Burg G, Weedon D, Sarasin A, editors. Pathology and Genetics of Skin Tumors. Lyon: IARC press; 2006. pp. 149–51. [Google Scholar]
- 8.Hurt MA, SantaCruz DJ. Tumors of the skin. In: Fletcher CD, editor. Diagnostic Histopathology of Tumors. 2nd ed. Vol. 2. London: Churchill Livingstone; 2000. pp. 1400–4. [Google Scholar]
- 9.Mc Nutt NS, Smoller BR, Contreras F. Skin. In: Damjanov I, Linder J, editors. Anderson's Pathology. 10th ed. Vol. 2. St Louis: Mosby; 1996. pp. 2445–6. [Google Scholar]
- 10.Nair PS. A clinicopathologic study of skin appendageal tumors. Indian J Dermatol Venereol Leprol. 2008;74:550. doi: 10.4103/0378-6323.44339. [DOI] [PubMed] [Google Scholar]
- 11.Buis PA, Verweij W, van Diest PJ. Value of histopathologic analysis of subcutis excisions by general practitioners. BMC Fam Pract. 2007;8:5. doi: 10.1186/1471-2296-8-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kumar P, Chatura KR, Haravi RM, Chandrasekhar HR. Proliferating trichilemmal cyst mimicking squamous cell carcinoma. Indian J Dermatol Venereol Leprol. 2000;66:149–50. [PubMed] [Google Scholar]
- 13.Sengul I, Sengul D. Posttraumatic proliferating trichilemmal tumour on the frontal region of the scalp: A case report. Cases J. 2010;3:80. doi: 10.1186/1757-1626-3-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sethi S, Singh UR. Proliferating trichilemmal cyst: Report of two cases, one benign and the other malignant. J Dermatol. 2002;29:214–20. doi: 10.1111/j.1346-8138.2002.tb00252.x. [DOI] [PubMed] [Google Scholar]
- 15.Aydin M, Aslaner A. Proliferating trichilemmal tumors on breast and scalp: Report of a case. Internet J Surg. 2006;7:2. [Google Scholar]
- 16.Kim HJ, Kim TS, Lee KH, Kim YM, Suh CH. Proliferating trichilemmal tumors: CT and MR imaging findings in two cases, one with malignant transformation. AJNR Am J Neuroradiol. 2001;22:180–3. [PMC free article] [PubMed] [Google Scholar]
- 17.Ye J, Nappi O, Swanson PE, Patterson JW, Wick MR. Proliferating pilar tumors: A clinicopathologic study of 76 cases with a proposal for definition of benign and malignant variants. Am J Clin Pathol. 2004;122:566–74. doi: 10.1309/0XLEGFQ64XYJU4G6. [DOI] [PubMed] [Google Scholar]
- 18.Trabelsi A, Stita W, Gharbi O, Kanani N, Sriha B, Korbi S. Malignant proliferating trichilemmal tumor of the scalp: A case report. Dermatol Online J. 2008;14:11. [PubMed] [Google Scholar]
- 19.Oh JE, Ahn C, Yang JS, Min KW, Song KY, Kim SJ, et al. Malignant proliferating trichilemmal tumour in renal transplantation. Nephrol Dial Transplant. 1997;12:2768–71. doi: 10.1093/ndt/12.12.2768. [DOI] [PubMed] [Google Scholar]
- 20.Siddha M, Budrukkar A, Shet T, Deshpande M, Basu A, Patil N, et al. Malignant pilar tumor of the scalp: A case report and review of literature. J Cancer Res Ther. 2007;3:240–3. doi: 10.4103/0973-1482.39001. [DOI] [PubMed] [Google Scholar]
- 21.Bae SB, Lee KK, Kim JS, Lee JH, Lee NS, Lee GT, et al. A case of malignant proliferating trichilemmoma of the scalp with multiple metastases. Korean J Intern Med. 2001;16:40–3. doi: 10.3904/kjim.2001.16.1.40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ziadi S, Trimeche M, Hammedi F, Sriha B, Jomaa W, Mokni M, et al. Squamous cell carcinoma arising from an epidermal inclusion cyst: A case report. N Am J Med Sci. 2010;2:46–7. [PMC free article] [PubMed] [Google Scholar]
- 23.Abreu Velez AM, Brown VM, Howard MS. An inflamed trichilemmal (pilar) cyst: Not so simple? N Am J Med Sci. 2011;3:431–4. doi: 10.4297/najms.2011.3431. [DOI] [PMC free article] [PubMed] [Google Scholar]