

Abstract
Background:
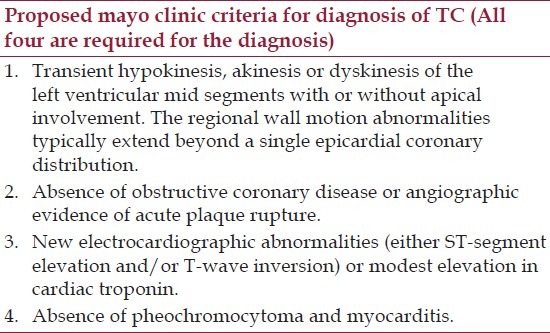
Takotsubo cardiomyopathy (TC) or transient left ventricular apical ballooning syndrome is an acute cardiac syndrome characterized by transient wall motion abnormalities extending beyond a single epicardial vessel in the absence of significant obstructive coronary artery disease.
Aim:
This study was to describe the clinical characteristics of TC in North America.
Materials and Methods:
We identified 10 patients who met the Mayo Clinic criteria for TC using our Electronic Medical Records. We also conducted a systematic review of case series of TC that were done in North America by searching the MEDLINE database. We identified 11 case series that met our eligibility criteria.
Results:
Our systematic review included 620 patients. Chest pain and ST segment elevation were the cardinal features of this syndrome, but the prevalence was lower than in the European and Asian cohort (50% and 39% as compared with 80% and 70%, respectively). Classic precipitating emotional or physical stress was described in > 80% of patients. Cardiac biomarkers were found to be elevated in >90% of our patients.
Conclusions:
TC is a worldwide problem and clinical presentation appears to be similar in North American, European, and Asian countries. However, fewer patients in our cohort presented with typical chest pain and electrocardiography (ECG) changes, which might suggest ethnic variations in the syndrome or perhaps a more aggressive diagnostic approach in North American countries.
Keywords: Broken heart syndrome, Left ventricular apical ballooning syndrome, Stress induced cardiomyopathy, Takotsubo cardiomyopathy, Transient left ventricular dysfunction
Introduction
Takotsubo Cardiomyopathy (TC) or transient left ventricular (LV) apical ballooning syndrome is a relatively new diagnosis. The first reported case was in 1991.[1] Since then it has been increasingly documented with a prevalence of 1–2% of patients with acute coronary syndrome.[2,3] It is characterized by transient LV dysfunction either with apical (“typical”) or midventricular (“atypical”) akinesia.[3,4]
Available data on demographic and clinical characteristic is based mainly on relatively small case series and most of the data comes from Asian and European country.[5,6] This study aims to report a case series and present a systematic review of reported case series conducted exclusively in North America in order to summarize the demographic and clinical data of patients with TC in this region.
Materials and Methods
From January 2009 to December 2011, clinical records of consecutive 1187 patients admitted with a diagnosis of acute coronary syndrome who underwent cardiac catheterization at Bassett medical center (Cooperstown, NY) were retrospectively reviewed. Ten patients were found to meet the proposed Mayo Clinic criteria for TC [Table 1].[7] Demographic, clinical, and laboratory data were recorded for each patient. Statistics were conducted to determine the frequency of each feature compared to previous reports.
Table 1.
Proposed mayo clinic criteria for diagnosis of TC
Results
Collected data is summarized in Table 2. All patients were female aged 49–72 years (mean age = 61.3 years). The most common presenting complaint was chest pain with only 1 patient presenting with shortness of breath. Of the 9 chest pain patients, 3 had associated shortness of breath. Emotional or physical stressors were identified in 7 patients. ST segment elevation was the most common electrocardiography (ECG) change, followed by T wave inversion. However, 4 patients did not have any abnormal ECG.
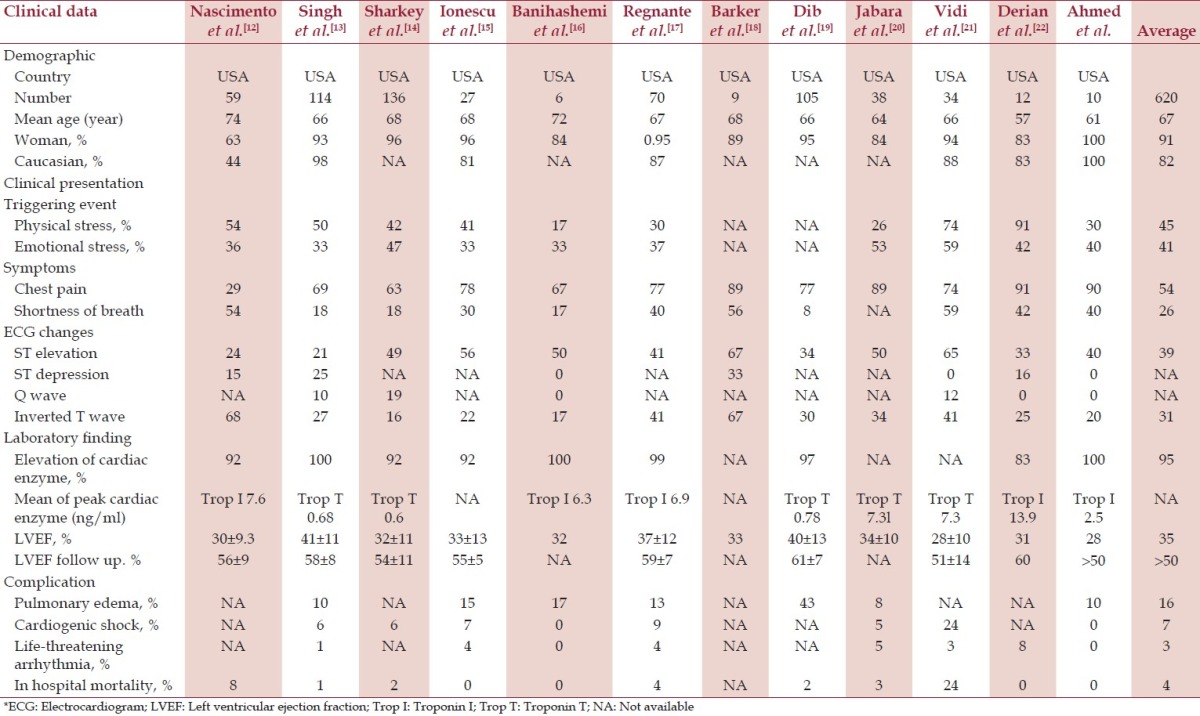
Table 2.
Demographic and clinical characteristics of consecutive patients in North America with the diagnosis of TC
All patients in our study had elevated Troponin I with an average of 2.5 ng/ml. All, but one patient, showed reduced LV ejection fraction that had been normalized within 1 month. One patient had documented pulmonary edema, while none of them experienced significant arrhythmias. There were no in-hospital deaths in this cohort.
Systematic review
We identified published case series by searching the PubMed database (through May 2012) that met proposed Mayo Clinic criteria for TC [Table 1].[7] The following search terms were used, LV apical ballooning syndrome, TC, stress induced cardiomyopathy, broken heart syndrome, ampulla cardiomyopathy, and transient LV dysfunction. We also manually searched the references from review articles. We included only studies that were performed in North America in an attempt to characterize clinical and demographic data of TC in this region. When more than one case series were reported from the same medical center or hospital, we included only the case series with largest number of patient to avoid duplication. We excluded case series that reported on <5 patients to minimize potential bias of reporting non-representative cases.
Data assessment
Using previously described search term in PubMed database, we identified 19 potentially relevant articles. After full length article review, 4 of them were excluded since they reported <5 patients, 3 of them were excluded due to potential patient duplication,[8–10] and a study was excluded since it included only patients with prior emotional stress.[11] Eleven case series met our inclusion criteria and were included for data analysis.[12–22] Figure 1 outlines our search methodology and selection process.
Figure 1.
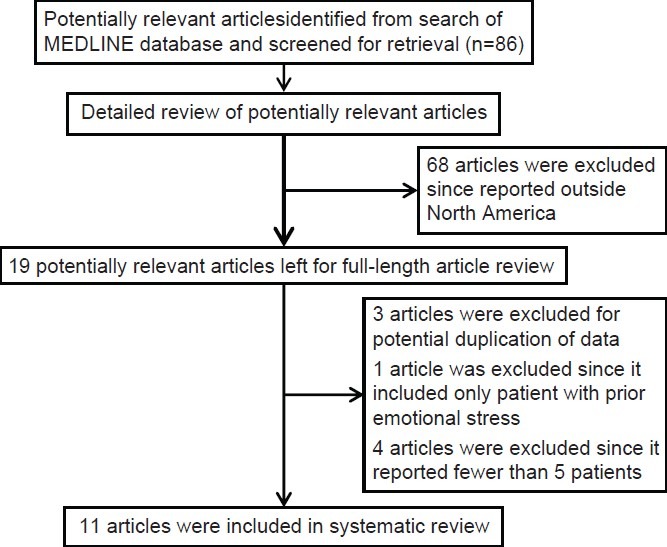
Case series identification
Table 2 summarizes demographic, clinical, and laboratory data of 11 case series that met this systematic review and our case series. The 12 case series comprised a total of 620 patients. Four largest studies contributed 425 patients (68.5%).[13,14,17,19] All studies were done in United State with the majority of patient being Caucasian except a study conducted in Florida that had Hispanic patient as the majority.[12]
Demographic and clinical features
Female predominance was seen in all series, ranging from 63–100%. The patients tended to present in their 60-80s with the mean age 67 years. Chest pain and shortness of breath are the most common presenting symptoms though a small number of cases with initial presentations of syncope, cardiac arrest, or diaphoresis were reported in some series.[12–14,17] Preceding stress, either physical or emotional, were identified in most of the patient (45% and 41%, respectively).
Electrocardiographic and laboratory data
ST segment elevation was the most common ECG changes found in TC (21–65%, mean 39%), followed by T wave inversion (17–68%, mean 31%). Other ECG abnormalities reported in these series include new pathologic Q wave, prolong QTc, new onset left and right bundle branch block, atrial fibrillation, ventricular tachycardia, and ventricular fibrillation. However, normal ECG does not exclude TC since the number of patients had normal ECG at presentation (as high as 33% in one series,[16] and 40% in our cohort).
Most of the patients had elevated cardiac enzyme, consistently reported to be >90% in every studies. Mean peak of Troponin ranged from 0.6–13.9 ng/ml.
LV function was assessed by transthoracic echocardiography or left venticulography in all studies. Almost all patients with this cardiomyopathy had reduced ventricular systolic function with mean LV ejection fraction (LVEF) of 35%. Typical dyskinesia of the LV apical or mid-ventricular segment with hyperkinetic basal wall was demonstrated. The reduced LVEF and wall motion abnormalities completely resolved in most of patients within a month.
Complication and in-hospital mortality
Though generally considered as benign and reversible cardiac condition, TC confers certain amount of morbidity and mortality. Pulmonary edema was observed over 10% in some series,[13,15–17,19] and in-hospital death attributable to TC was seen in most of the series,[12–14,17,19–21] with overall mortality of 3%.
Discussion
TC is a newly recognized disease entity that was first described in 1991.[1] Following the original description, several case series from Eastern countries, especially from Far East region, have been reported suggesting that this cardiomyopathy might affect mostly Asian population,[4,23–25] and most of our understanding and recognition of this syndrome is based largely on these studies.[5] More recent case series from other ethnic groups, including Caucasian,[11,26,27] and Black,[28,29] have been described as well suggesting that this syndrome is a worldwide problem that might affect patient in any ethnic group.
Although consistently described in Caucasian population, most of the studies were conducted in European countries,[6] leaving the clinical characteristic of patients with TC in North America unclear. Here, we report the first systematic review of TC in this region, emphasizing the clinical and laboratory presentation.
Consistent with the Asian and European cohort, there is a striking female population in their 60–80s. Chest pain remained the most common initial presentation but, interestingly, it was found in only half of the patient of our North American cohort as compared with >80% in Asian and European cohort.[6] This might reflect a more aggressive approach toward coronary angiography in this region. Triggering emotional or physical stress was found in the majority of patients, as previously described in Asian and European cohort.
ECG changes are less striking in our cohort. ST segment elevation and T wave inversion were found in only 39% and 31% of patients, respectively, in contrast to >90% in Japanese cohort and >60% in European cohort.[5,6] This might suggest the ethnic variation of the disease or, again, might just reflect more aggressive diagnostic approach in North American countries; thus, detecting more subtle cases without ECG changes. High percentage of patients with elevated cardiac biomarker was reported in our cohort. Impaired LV systolic function with rapid recovery was persistently described in our study as well.
Though generally regarded as reversible condition, TC contributes to significant morbidity and mortality. Flash pulmonary edema was observed in one out of five of our cohort, comparable to the number seen in the previous report.[6] Cardiogenic shock and life-threatening arrhythmia were also seen in a significant portion of patients in our study. Total 3% of in-hospital mortality was, again, noted in our review, consistent with other reports.
Conclusion
In conclusion, we report a case series and conducted a systematic review of TC in North American countries in an attempt to better characterize the clinical and demographic characteristics of patients with TC in this region. Interestingly, the number of patients with chest pain and ECG changes was significantly lower in our study as compared to previous reports from Europe and Asia.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. Myocardial stunning due to simultaneous multivessel coronary spasms: A review of 5 cases. J Cardiol. 1991;21:203–14. [PubMed] [Google Scholar]
- 2.Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: A systematic review. Eur Heart J. 2006;27:1523–9. doi: 10.1093/eurheartj/ehl032. [DOI] [PubMed] [Google Scholar]
- 3.Kurowski V, Kaiser A, von Hof K, Killermann DP, Mayer B, Hartmann F, et al. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): Frequency, mechanisms, and prognosis. Chest. 2007;132:809–16. doi: 10.1378/chest.07-0608. [DOI] [PubMed] [Google Scholar]
- 4.Tsuchihashi K, Ueshima K, Uchida T, Oh-mura N, Kimura K, Owa M, et al. Transient left ventricular apical ballooning without coronary artery stenosis: A novel heart syndrome mimicking acute myocardial infarction. Angina Pectoris-Myocardial Infarction Investigations in Japan. J Am Coll Cardiol. 2001;38:11–8. doi: 10.1016/s0735-1097(01)01316-x. [DOI] [PubMed] [Google Scholar]
- 5.Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, et al. Systematic review: Transient left ventricular apical ballooning: A syndrome that mimics ST-Segment elevation myocardial infarction. Ann Intern Med. 2004;141:858–65. doi: 10.7326/0003-4819-141-11-200412070-00010. [DOI] [PubMed] [Google Scholar]
- 6.Pilgrim TM, Wyss TR. Takotsubo cardiomyopathy or transient left ventricular apical ballooning syndrome: A systematic review. Int J Cardiol. 2008;124:283–92. doi: 10.1016/j.ijcard.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 7.Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): A mimic of acute myocardial infarction. Am Heart J. 2008;155:408–17. doi: 10.1016/j.ahj.2007.11.008. [DOI] [PubMed] [Google Scholar]
- 8.Sharkey SW, Lesser JR, Zenovich AG, Maron MS, Lindberg J, Longe TF, et al. Acute and reversible cardiomyopathy provoked by stress in women from the United states. Circulation. 2005;111:472–9. doi: 10.1161/01.CIR.0000153801.51470.EB. [DOI] [PubMed] [Google Scholar]
- 9.Elesber A, Lerman A, Bybee KA, Murphy JG, Barsness G, Singh M, et al. Myocardial perfusion in apical ballooning syndrome correlate of myocardial injury. Am Heart J. 2006;152:469.e9–13. doi: 10.1016/j.ahj.2006.06.007. [DOI] [PubMed] [Google Scholar]
- 10.Bybee KA, Prasad A, Barsness GW, Lerman A, Jaffe AS, Murphy JG, et al. Clinical characteristics and thrombolysis in myocardial infarction frame counts in women with transient left ventricular apical ballooning syndrome. Am J Cardiol. 2004;94:343–6. doi: 10.1016/j.amjcard.2004.04.030. [DOI] [PubMed] [Google Scholar]
- 11.Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, et al. Neurohumonal features of myocardial stunning due to sudden emotional stress. New Engl J Med. 2005;352:539–48. doi: 10.1056/NEJMoa043046. [DOI] [PubMed] [Google Scholar]
- 12.Nascimento FO, Santana O, Perez-Caminero M, Benjo AM. The characteristics of stress cardiomyopathy in an ethnically heterogenous population. Clinics (Sao Paulo) 2011;66:1895–9. doi: 10.1590/S1807-59322011001100008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Singh NK, Rumman S, Mikell FL, Nallamothu N, Rangaswamy C. Stress cardiomyopathy: Clinical and ventriculographic characteristics in 107 north American subjects. Int J Cardiol. 2010;141:297–303. doi: 10.1016/j.ijcard.2008.12.043. [DOI] [PubMed] [Google Scholar]
- 14.Sharkey SW, Windenburg DC, Lesser JR, Maron MS, Hauser RG, Lesser JN, et al. Natural history and expansive clinical profile of stress (Tako-Tsubo) cardiomyopathy. J Am Coll Cardiol. 2010;55:333–41. doi: 10.1016/j.jacc.2009.08.057. [DOI] [PubMed] [Google Scholar]
- 15.Ionescu CN, Aguilar-Lopez CA, Sakr AE, Ghantous AE, Donohue TJ. Long-term outcome of Tako-Tsubo cardiomyopathy. Heart Lung Circ. 2010;19:601–5. doi: 10.1016/j.hlc.2010.06.667. [DOI] [PubMed] [Google Scholar]
- 16.Banihashemi MR, Khan IA. Acute stress-induce cardiomyopathy: A brief observation. In J Card. 2009;134:273–7. doi: 10.1016/j.ijcard.2007.12.105. [DOI] [PubMed] [Google Scholar]
- 17.Regnante RA, Zuzek RW, Weinsier SB, Latif SR, Linsky RA, Ahmed HN, et al. Clinical characteristics and four-year outcomes of patients in the Rhode Island Takotsubo cardiomyopathy registry. Am J Cardiol. 2009;103:1015–9. doi: 10.1016/j.amjcard.2008.12.020. [DOI] [PubMed] [Google Scholar]
- 18.Barker S, Solomon H, Bergin JD, Huff JS, Brady WJ. Electrocardiographic ST-segment elevation: Takotsubo cardiomyopathy versus ST-segment elevation myocardial infarction-- A case series. Am J Emerg Med. 2009;27:220–6. doi: 10.1016/j.ajem.2008.02.016. [DOI] [PubMed] [Google Scholar]
- 19.Dib C, Asivatham S, Elesber A, Rihal C, Friedman P, Prasad A. Clinical correlates and prognostic significance of electrocardiographic abnormalities in apical ballooning syndrome (Takotsubo/stress-induced cardiomyopathy) Am Heart J. 2009;157:933–8. doi: 10.1016/j.ahj.2008.12.023. [DOI] [PubMed] [Google Scholar]
- 20.Jabara R, Gadesam R, Pendyala L, Chronos N, King SB, Chen JP. Comparison of the clinical characteristics of apical and non-apical variants of “broken heart” (takotsubo) syndrome in the United States. J Invasive Cardiol. 2009;21:216–22. [PubMed] [Google Scholar]
- 21.Vidi V, Rajesh V, Singh PP, Mukherjee JT, Lago RM, Venesy DM, et al. Clinical characteristics of Tako-Tsubo cardiomyopathy. Am J Cardiol. 2009;104:578–82. doi: 10.1016/j.amjcard.2009.04.028. [DOI] [PubMed] [Google Scholar]
- 22.Derian W, Soundarraj D, Rosenberg MJ. Stress induced cardiomyopathy: Not always apical ballooning. Rev Cardiovasc Med. 2007;8:228–33. [PubMed] [Google Scholar]
- 23.Kawai S, Suzuki H, Yamaguchi H, Tanaka K, Sawada H, Aizawa T, et al. Ampulla cardiomyopathy (‘Takotusbo’ cardiomyopathy)--reversible left ventricular dysfunction: With ST segment elevation. Jpn Circ J. 2000;64:156–9. doi: 10.1253/jcj.64.156. [DOI] [PubMed] [Google Scholar]
- 24.Kurisu S, Sato H, Kawagoe T, Ishihara M, Shimatani Y, Nishioka K, et al. Tako-tsubo-like left ventricular dysfunction with ST-segment elevation: A novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J. 2002;143:448–55. doi: 10.1067/mhj.2002.120403. [DOI] [PubMed] [Google Scholar]
- 25.Abe Y, Kondo M, Matsuoka R, Araki M, Dohyama K, Tanio H. Assessment of clinical features in transient left ventricular apical ballooning. J Am Coll Cardiol. 2003;41:737–42. doi: 10.1016/s0735-1097(02)02925-x. [DOI] [PubMed] [Google Scholar]
- 26.Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left ventricle: First series in white patients. Heart. 2003;89:1027–31. doi: 10.1136/heart.89.9.1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Schneider B, Stein J. Tako-tsubo-like transient left ventricular dysfunction: Prevalence and clinical findings in a western population. Circulation. 2004;110:697. [Google Scholar]
- 28.Pezzo SP, Hartlage G, Edwards CM. Takotsubo cardiomyopathy presenting with dyspnea. J Hosp Med. 2009;4:200–2. doi: 10.1002/jhm.402. [DOI] [PubMed] [Google Scholar]
- 29.Patel HM, Kantharia BK, Morris DL, Yazdanfar S. Takotsubo syndrome in African-American women with atypical presentations: A single-center experience. Clin Cardiol. 2007;30:14–8. doi: 10.1002/clc.21. [DOI] [PMC free article] [PubMed] [Google Scholar]