

Abstract
Study Objectives:
To examine whether the initial benefit of weight loss on obstructive sleep apnea (OSA) severity at 1 year is maintained at 4 years.
Design:
Randomized controlled trial with follow-up at 1, 2, and 4 years.
Setting:
4 Look AHEAD clinical centers.
Participants:
Two hundred sixty-four obese adults with type 2 diabetes and OSA.
Interventions:
Intensive lifestyle intervention with a behavioral weight loss program or diabetes support and education.
Measurements:
Change in apnea-hypopnea index on polysomnogram.
Results:
The intensive lifestyle intervention group's mean weight loss was 10.7 ± 0.7 (standard error), 7.4 ± 0.7, and 5.2 ± 0.7 kg at 1, 2, and 4 years respectively, compared to a less than 1-kg weight loss for the control group at each time (P < 0.001). Apnea-hypopnea index difference between groups was 9.7 ± 2.0, 8.0 ± 2.0, and 7.7 ± 2.3 events/h at 1, 2 and 4 years respectively (P < 0.001). Change in apnea-hypopnea index over time was related to the amount of weight loss (P < 0.0001) and intervention, independent of weight loss (P = 0.001). Remission of OSA at 4 years was 5 times more common with intensive lifestyle intervention (20.7%) than diabetes support and education (3.6%).
Conclusions:
Among obese adults with type 2 diabetes and OSA, intensive lifestyle intervention produced greater reductions in weight and apnea-hypopnea index over a 4 year period than did diabetes support and education. Beneficial effects of intensive lifestyle intervention on apneahypopnea index at 1 year persisted at 4 years, despite an almost 50% weight regain. Effect of intensive lifestyle intervention on apnea-hypopnea index was largely, but not entirely, due to weight loss.
Citation:
Kuna ST; Reboussin DM; Borradaile KE; Sanders MH; Millman RP; Zammit G; Newman AB; Wadden TA; Jakicic JM; Wing RR; Pi-Sunyer FX; Foster GD; Sleep AHEAD Research Group. Long-term effect of weight loss on obstructive sleep apnea severity in obese patients with type 2 diabetes. SLEEP 2013;36(5):641-649.
Keywords: Apnea-hypopnea index, polysomnogram
INTRODUCTION
Obesity is the strongest predictor of obstructive sleep apnea (OSA), a prevalent breathing disorder during sleep associated with increased risk of motor vehicle accidents, hypertension, cardiovascular disease, and metabolic disorders.1,2 Weight loss is frequently recommended to improve OSA among obese patients. Previously, we reported baseline and 1-y follow-up results of the Sleep AHEAD (Action for Health in Diabetes) study examining the effect of weight loss on OSA severity in obese adults with type 2 diabetes. Sleep AHEAD is a four-center ancillary investigation of the Look AHEAD study, a 16-center prospective, randomized, controlled clinical trial in overweight and obese adults with type 2 diabetes investigating the long-term health effect of an intensive lifestyle intervention (ILI) consisting of dietary modification, exercise, and education versus diabetes support and education (DSE).3,4 The Sleep AHEAD study took advantage of the anticipated differences in weight change between groups over time to assess the effect of weight loss on OSA. The Look AHEAD study recently reported changes in weight, glycemic control, and cardiovascular disease risk factors over 4 y.5
Of the 306 individuals who enrolled in the Sleep AHEAD study, central sleep apnea was diagnosed in one participant on the unattended polysomnography (PSG); this individual was excluded from the study. Of the remaining 305 participants, 87% had OSA (apnea-hypopnea index [AHI] ≥ 5 events/h).3 The ILI group had significantly greater reductions in weight and AHI than did the DSE group after 1 y.4 Two small (n ≤ 72) randomized trials, recruiting from different patient populations, have recently reported similar reductions in OSA severity following 12 mo of weight loss.6–9 In the longest study to date, Tuomilehto and colleagues reported that, among 71 patients with mild OSA, improvement in AHI after weight loss at 1 y was sustained at 2 y despite weight regain.10
The current study examined whether the initial benefit of weight loss on the severity of OSA at 1 y was maintained at 4 y.4 To our knowledge, it is the largest and longest study of its kind. We hypothesized that obese patients with type 2 diabetes and OSA receiving ILI would experience greater reduction in AHI over 4 y compared to those receiving DSE.
METHODS
Subjects
Look AHEAD's primary inclusion criteria were age 45-76 y, body mass index (BMI) ≥ 25 kg/m2 (or ≥ 27 kg/m2 if taking insulin), physician-verified type 2 diabetes, hemoglobin A1C < 11%, and blood pressure < 160 mm Hg systolic and < 100 mm Hg diastolic. Look AHEAD subjects with a previous surgical or current medical treatment for OSA were excluded from participation in the Sleep AHEAD study. Individuals with previously diagnosed but untreated OSA were eligible to participate. The protocol was approved by each site's Institutional Review Board and participants provided written informed consent. The study was registered at www.clinicaltrials.gov (registration, NCT00194259).
When comparing those participants who were enrolled in the Sleep AHEAD study to those enrolled in the Look AHEAD but not the Sleep AHEAD study at the four Look AHEAD sites (n = 1,012), there were no differences between the groups in weight, BMI, sex, race/ethnicity, or waist circumference. There were also no differences between the two groups in the response to the question: How often do you feel excessively (overly) sleepy during the day? (1 = 1 day/mo or less, 2 = 2-4 days/mo, 3 = 5-15 days/mo, 4 = 16-30 days/mo). Sleep AHEAD study participants were slightly older (61.3 ± 6.5 y versus 58.7 ± 6.9 y, P = 0.001) and had slightly lower hemoglobin A1C values (7.2 ± 1.1% versus 7.4 ± 1.2%, P = 0.03) than those Look AHEAD study participants who were not enrolled in the Sleep AHEAD study.3
As part of the Look AHEAD study, participants were randomly assigned to ILI or DSE using a web-based data management system that verified eligibility. Randomization was stratified by clinical center and blocked with random block sizes. The following individuals were blinded to participant assignment: the Look AHEAD personnel collecting outcome measures, the technologists performing and/or scoring the home unattended sleep studies, and the biostatistician during data collection. The details of the Look AHEAD and Sleep AHEAD study designs, participant characteristics at baseline, intervention, and outcomes are detailed elsewhere.3–5,11–14
Intensive Lifestyle Intervention
ILI participants received a group behavioral weight loss program developed for obese patients with type 2 diabetes.13 They were prescribed portion-controlled diets with liquid meal replacements, and snack bars for the first 4 mo (with reduced use from mo 5 through 12). The physical activity prescription was 175 min per week of moderate-intensity activity such as brisk walking. In years 2 through 4, intervention was provided mainly on an individual basis and included at least one on-site visit per mo and a second contact by telephone, mail, or e-mail. At each session, participants were weighed, self-monitoring records reviewed, and a new lesson presented.
Diabetes Support and Education
DSE consisted of three group sessions annually.14 These sessions focused on diet, physical activity, and social support. Information on behavioral strategies was not presented, and participants were not weighed at the sessions.
Polysomnography and Morphometrics
PSGs at baseline and 1 and 2 y were performed with the Compumedics PS2 monitor (Compumedics Sleep, Abbots-ville, Australia). The PSGs at 4 y were performed with the Compumedics Safiro monitor. The change in recording device was necessitated by the obsolescence and discontinuation of the PS2 monitor by the manufacturer. The monitors used the same oximeter to record the oxygen saturation signal and the same computer software program was used to assist in the manual scoring of all PSG recordings. Prior to using the Safiro monitor in Sleep AHEAD study participants, simultaneous overnight PSGs were performed with the PS2 and Safiro monitors in 15 adult males with suspected OSA who were not participating in the Sleep AHEAD study. No differences in sleep stage and respiratory outcome measures were found between the two sets of recordings. The AHI on the Safiro recordings (mean [± standard deviation], 60.9 ± 29.7 events/h) and on the PS2 recordings (63.6 ± 32.1 events/h) were not significantly different (P = 0.21) and were highly correlated (P < 0.0001; R = 0.97; see supplemental material for additional details).
The sleep technicians and PSG scorer were blinded to participant randomization. All PSGs were scored at a centralized reading laboratory.15–17 Apnea was defined as the cessation of airflow for at least 10 sec with (obstructive apnea) or without (central apnea) respiratory efforts. Hypopnea was defined as a 30% or greater reduction in airflow or thoracoabdominal movement lasting at least 10 sec with at least a 4% oxygen desaturation. AHI was the average number of apneas and hypopneas per h of sleep and used to classify OSA severity as mild (5 ≤ AHI < 15 events/h), moderate (15 ≤ AHI < 30 events/h), and severe (AHI ≥ 30 events/h).
Intrascorer reliability and the possibility of scoring drift over time was determined by having the masked scorer rescore 92 randomly chosen Sleep AHEAD PSGs over the course of the study. The sample included 47 PSGs from baseline, 20 from the 1-y follow-up, 8 from the 2-y follow-up, and 17 from 4-y follow-up. Of these studies, 28% were rescored within 1 y of their original score, 27% between 1 and 2 y, 12% between 2 and 3 y, and 23% between 3 and 4 y. The remaining 10% of the studies were rescored at least 4 y following their original score. The median number of days between the date of the original score and that of the rescore was 581, with a range of 38 days to 5.6 y. The original and rescored AHI measurements were highly correlated (r = 0.97; 95% confidence interval: 0.95 to 0.98). The median difference between scores is -0.15 events/h and the median absolute difference was 2.1 events/h. There was some indication that the difference between scores decreased as the time between original and rescoring increased, but the effect was small, i.e., 2 units over the entire range time between scorings (see supplemental material).
Participants and their primary care providers were informed in writing about the results of each sleep study and, if OSA was present (AHI ≥ 5 events/h), the severity of the disease. Prior to each visit, participants were asked if they had received any treatment for OSA. None received surgical treatment over the 4-y period. Those who were on positive airway pressure treatment were asked not to use the treatment for 3 nights prior to the polysomnogram and cautioned not to drive if sleepy during that period. A recent report indicates that 3 nights is a sufficient interval to reverse any treatment-related effect on AHI.18 Weight, height, and waist and neck circumference were assessed within 1 week of each PSG.11,19
Statistical Analysis
The means reported at baseline are unadjusted averages. All tests of group differences were based on the intent-to-treat principle; however, 41 participants with follow-up were excluded because they did not have OSA on baseline PSG (AHI < 5 events/h). The primary analysis was a mixed-effects model to estimate change in AHI over time using all available data and adjusting for clinical site, baseline AHI, and visit year. A first-order autoregressive structure was used to model correlations over time. An interaction term was used to test for possible changes in the intervention effect over time. In secondary analyses, change in weight and change in AHI, adjusting for changes in weight, neck circumference, and waist circumference, were analyzed using the same model. Estimates of the change in AHI within each intervention arm and change in weight also used the mixed-effects model.
Two analyses were performed to assess the possibility that missing AHI data at follow-up (17.0% at 1 y, 20.5% at 2 y, and 37.5% at 4 y) might bias the results: one testing whether the probability of a missing PSG was related to our covariates, and another determining whether the patterns of missing PSGs were related to change in AHI. In the first model, because weight measurements from the main Look AHEAD trial were rarely missing (3% at year 1, 5% at year 2, and 7% at year 4), we could assess the relationship between missing PSG data and clinical site, year of follow-up, baseline AHI, intervention arm, and follow-up weight measurements using generalized estimating equation models. Baseline AHI, intervention group, and follow-up weight measurements were not predictive of a missing PSG, though, as expected study site and follow-up year were. Participant retention was lower at one of the study sites due to a frequent change in study personnel at that site. In addition, pattern-mixture models were used to further assess missing data.20 In these analyses, participants were placed into groups depending on their missing data pattern. These missing data patterns were then included in analyses to examine the effect of missing data patterns on changes in AHI. Interaction terms were included to determine whether any effect of missing data patterns was moderated by intervention arm or year of follow-up. There were no statistically significant main or interaction effects for pattern, indicating that patterns of missing data were not related to observed changes in AHI. These analyses support our decision to treat the AHI measurements as missing-at-random, so that the mixed-effects analysis of covariance models used to obtain adjusted mean changes for AHI and weight were not biased by the missing PSG data.
The mixed-effects maximum likelihood and generalized estimating equation analysis of repeated outcomes were performed in Proc Mixed software (SAS, version 9; SAS Institute Inc, Cary, North Carolina) using an alpha level of 0.05.
RESULTS
Participants
Baseline participant characteristics are reported in Table 1.4 No differences were noted between the ILI and DSE groups for these measures. In particular, there were no differences between the groups in age (P = 0.79) and menopausal status in women (P = 0.64). There were 89.6% of the women who reported that they were postmenopausal. The number of Sleep AHEAD study participants in the ILI and DSE groups who completed assessments over time is shown in Figure 1. At their 1-y visit, 5.9% of participants with OSA at baseline had obtained treatment for their OSA, and 9.0% and 11.5% reported obtaining treatment at the 2- and 4-y visits, respectively. All of these participants were on positive airway pressure treatment and none had obtained surgical treatment. Of the 29 participants on treatment at the 4-y follow-up, 4 had mild OSA on baseline testing, 12 had moderate OSA, and 13 had severe OSA.
Table 1.
Baseline characteristics of the study participants

Figure 1.
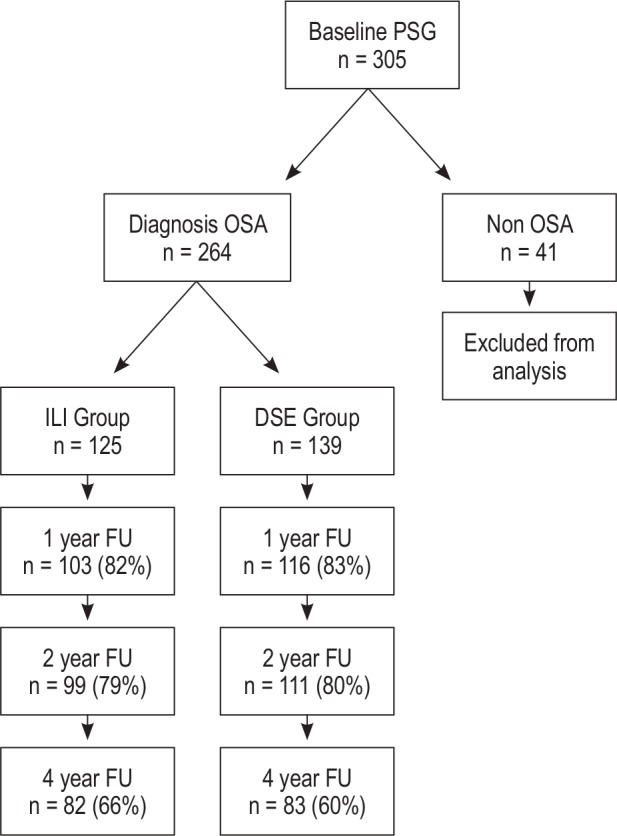
Diagram showing the number of Sleep AHEAD participants in the intensive lifestyle intervention and diabetes support and education groups who completed assessments over time. DSE, Diabetes Support and Education; FU, follow-up; ILI, intensive lifestyle intervention; OSA, obstructive sleep apnea; PSG, polysomnogram.
Weight and AHI
Figure 2 shows the change in AHI and weight from baseline. The ILI group had a significantly greater weight loss than the DSE group at 1, 2, and 4 y (Table 2, P < 0.001). Difference in body weight between the two groups was 10.8 ± 1.0, 6.7 ± 1.0, and 4.4 ± 1.0 kg at 1, 2, and 4 y, respectively (P < 0.001; Figure 2). Changes in waist and neck circumferences showed a similar between-group pattern (Table 2). The ILI group had significantly lower AHIs than the DSE group at 1, 2, and 4 y (Table 2, P < 0.009). The difference in AHI between the groups was 9.7 ± 2.0, 8.0 ± 2.0, and 7.7 ± 2.3 events/h at 1, 2, and 4 y, respectively (P ≤ 0.001; Figure 2).
Figure 2.

Estimated mean (standard error) changes in body weight and AHI from baseline at year 1, 2, and 4. AHI, apnea-hypopnea index (the number of apneahypopnea events/h). The dashed line indicates the Diabetes Support and Education group; the solid line indicates the Intensive Lifestyle Intervention group.
Table 2.
Estimated mean (standard error) changes in body weight, apnea-hypopnea index, and neck and waist circumference at 1, 2, and 4 years

The estimated effect of weight change on change in AHI was 0.43 in both the DSE (P = 0.0009) and ILI (P < 0.0001) groups, i.e., a 0.43 improvement in AHI for every kg of weight loss. We also performed a regression of change in AHI from baseline to year 4 with categories of weight change as a predictor: ≥ 5 kg gain, ± 5 kg change, 5-9 kg loss, and ≥ 10 kg loss. Weight category was not a significant predictor in the model. It is expected that the continuous change in weight would be more sensitive to associations than the categories.
At 4 y, more than twice as many ILI participants (43.9%) compared with DSE participants (18.1%) demonstrated improvement in their OSA category (e.g., severe to moderate, moderate to mild, and mild to none; Figure 3). Remission of OSA (AHI < 5 events/h) at 4 y was 5 times more common in ILI participants (20.7%) than in DSE participants (3.6%). The percentage of participants who had severe OSA at 4 y was 35% in the DSE group compared to 14.6% in the ILI group.
Figure 3.
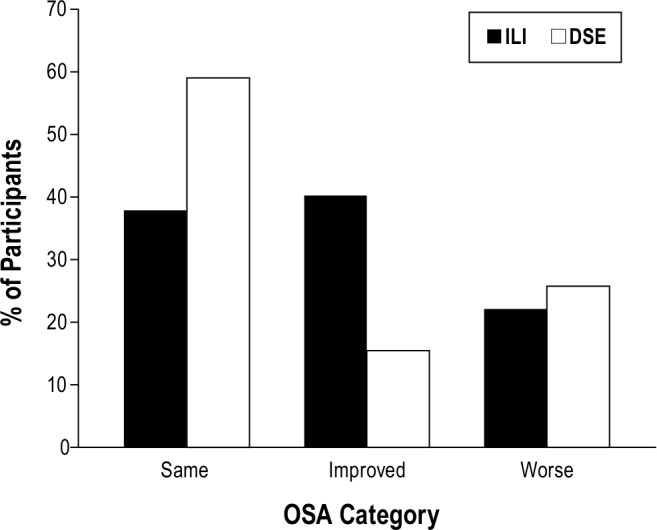
Percentage of participants in intensive lifestyle intervention (black bars, n = 90) and diabetes support and education (white bars, n = 97) whose obstructive sleep apnea (OSA) category improved (≥ 1 category change), worsened (≥ 1 category change), or was unchanged from baseline to year 4. Data are from the participants who had baseline and year 4 data.
Figure 4 shows the percentage of ILI and DSE participants without OSA and with mild, moderate, and severe OSA at 4 y compared to their OSA severity at baseline. Participants in the DSE group were less likely than ILI participants to experience a change in OSA severity category at year 4. Most of the participants who had OSA (AHI ≥ 5) at baseline but not at year 4 were ILI participants with mild OSA at baseline. ILI participants with moderate and severe OSA at baseline showed similar shifts to less severe OSA at year 4.
Figure 4.
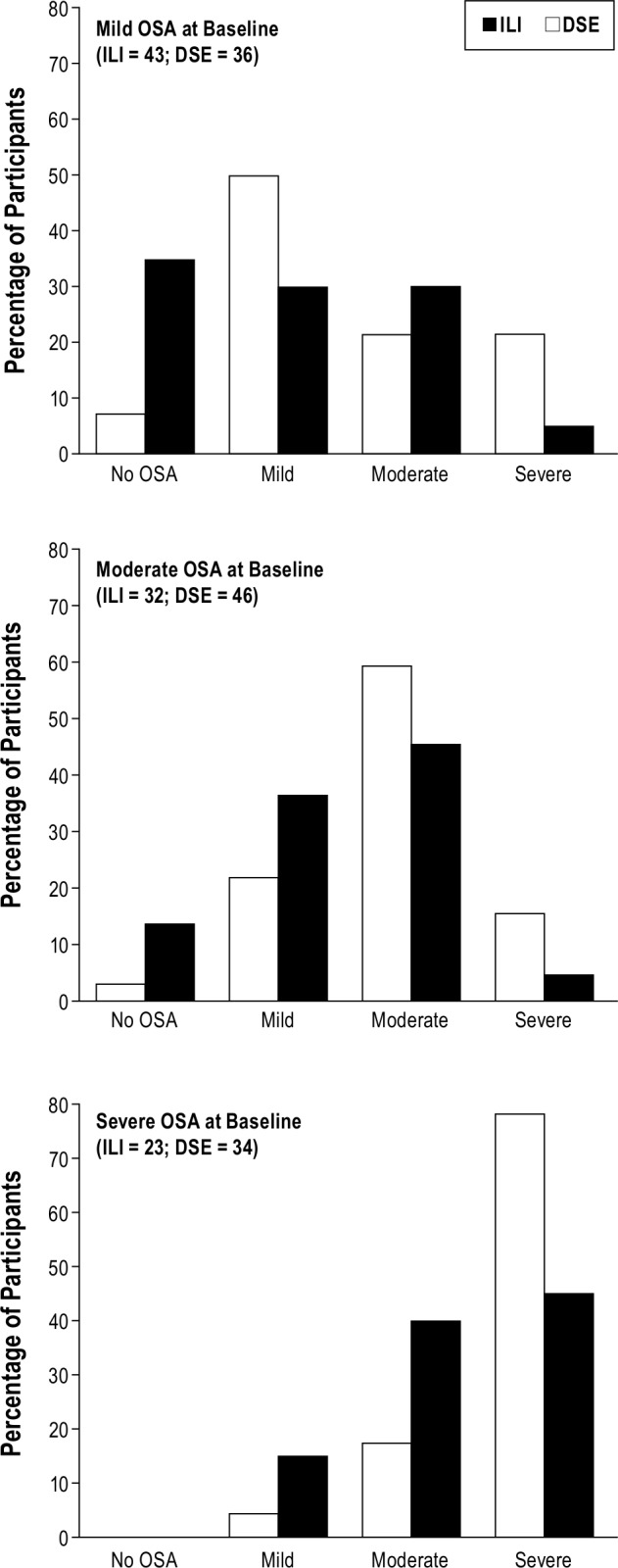
Percentage of ILI (black bars) and DSE (white bars) participants without OSA and with mild, moderate, and severe OSA at 4 years compared to their OSA severity at baseline. DSE, Diabetes Support and Education; ILI, intensive lifestyle intervention.
Treatment Interaction Effects
The change in AHI from baseline over time was independently related to intervention arm and change in body weight (Table 3; P < 0.0001). When change in weight was added to the model, follow-up year had no effect on the change in AHI over time (P = 0.58), indicating that the change in AHI at 1 y remained relatively constant at 2 y and 4 y (Table 3). Furthermore, when change in weight was added to the model, intervention arm remained significant (P = 0.001) indicating an effect of ILI on AHI over time independent of weight change. Change in AHI over time was strongly related to baseline AHI (P < 0.001) with greater changes in AHI occurring in individuals with higher AHI at baseline. When changes in waist and neck circumference were added to the model, no relationship was present between these measures and change in AHI over time and the previously noted relationships with other covariates remained significant (Table 3). Unlike our 1-y results, the 4-y results did not show that the intervention was more effective for men.
Table 3.
Mixed-effects models estimating change in AHI over time

DISCUSSION
This is the first randomized controlled trial demonstrating the effect of an ILI on the severity of OSA over a 4-y period. Extending the results of our previously reported findings of the Sleep AHEAD cohort,3,4 the current results indicate that, among obese patients with type 2 diabetes and OSA, the improvement in AHI that was associated with ILI with weight loss at 1 y persisted at 4 y despite a 50% weight regain. The change in AHI over the 4-y period was greater in participants who had higher baseline AHI and who experienced greater decreases in weight. However, even when weight change was included in the model, the intervention group had an independent effect on the change in AHI over time (P = 0.001).
The current results show that changes in category of OSA severity at 1 y persisted at 4 y.4 At 4 y, more than five times as many participants in the ILI group than in the DSE group had total remission of their OSA, and the prevalence of severe OSA among ILI participants was half that of the DSE group. This benefit is of particular significance because aging in adults is an independent risk factor for OSA.21–23 Remission of OSA occurred in those individuals with mild to moderate OSA at baseline. Among those participants with severe OSA, none had remission of OSA and few changed to a mild severity. It is of note that the improvement in AHI by 0.43 events/h/kg of weight loss in the ILI group, in which the mean baseline AHI baseline was 22.9 ± 18.0 events/h and BMI 36.8 ± 5.8 kg/m2, was similar to the reduction of 0.4 events/h/kg weight loss reported by Tuomilhelto et al.7 in a cohort with mild OSA (mean baseline AHI 10 ± 3 events/h and BMI 33.4 ± 2.8 kg/m2). The similarity in results suggests a linear relationship between weight loss and change in AHI across the spectrum of OSA severity and may explain why none of the participants with severe OSA in the current study experienced a remission of their OSA with weight loss. In both the ILI and DSE groups, a similar proportion of participants had a worsening of OSA severity category over time. Indeed, some study participants with mild OSA at baseline had severe OSA at the 4-y follow-up. This was even observed in the ILI group, suggesting the effect of factors other than body weight on OSA. It is unknown if these participants were less adherent to the ILI regimen, and the number of participants was too small to perform subanalyses of other possible contributing factors. Although most individuals in the ILI group continued to have OSA following weight loss, the decrease in the presence and/or severity of OSA among obese patients who have type 2 diabetes is likely to be associated with significant clinical benefit.1 Emerging evidence suggests that a reduction in AHI is associated with a decrease in cardiovascular risk.24–26 These data suggest that the reduction of OSA severity associated with the weight reduction achieved by participants in our study will decrease exposure to the risks of OSA as well as reduce health care use and economic costs.27,28
The results of our 4-y follow-up study extend to recently published randomized controlled trials.6–9,29 Tuomeileto and colleagues randomized 81 participants (BMI 28-40 kg/m2) with mild OSA to a very low calorie diet for 12 w with supervised lifestyle counseling for 1 y versus a single general dietary and exercise counseling session.7 At 1 y, weight had decreased (mean [ ± SD]) 10.7 ± 6.5 kg in the lifestyle intervention group and 2.4 ± 5.6 kg in the control group (P < 0.001). The change in AHI was (mean [ ± SD]) -4.0 ± 5.6 events/h in the lifestyle intervention group and 0.3 ± 8.0 events/h in the control group (P = 0.017). This study was limited by the relatively small sample size and the significant between group differences in body weight at baseline (P = 0.002). More recently, these investigators reported their 2-y follow-up results.10 No lifestyle counseling was offered during the second year. The favorable changes achieved by the lifestyle intervention in the first year were sustained at the 2-y follow-up despite a weight regain of about 50%. Interpretation of these data must be done in the context that the analysis was performed on a per protocol rather than an intent-to-treat basis.30
Johansson and colleagues performed a randomized, parallel arm study in 63 obese men with moderate to severe OSA.6 The intervention group received a very-low-energy liquid diet for 7 weeks followed by 2 weeks of gradual introduction of normal food. The control group adhered to their usual diet. At 9 weeks, the intervention group's mean body weight was 20 kg (95% confidence interval 18-21) lower than that of the control group, whereas its mean AHI was 23 events/h (range 15-30) lower. In the intervention group, 5 of 30 (17%) were disease free after the energy restricted diet (AHI < 5), with 15 of 30 (50%) having mild disease (AHI 5-14.9). Like the current study, greater improvement in AHI was observed in patients with more severe OSA at baseline. Similar results were obtained from participants initially randomized to usual diet who were subsequently crossed over to the very-low-energy liquid diet intervention.8 Combining both groups into an observational study, these investigators recently reported that the initial improvement in AHI at 9 weeks was sustained at 1 y despite an approximate increase in weight of 25%.8
Our finding that the change in AHI over time was associated not only with weight loss but with intervention group independent of weight change is of particular interest. It is possible that residual confounders other than factors directly associated with the ILI intervention may have accounted for these results. Among a multicomponent lifestyle intervention, it is difficult to ascertain whether changes in diet, physical activity, fitness, or some other nonspecific treatment effects (e.g, improved adherence to health recommendations) may have accounted for the weight-independent effects on AHI. Previous studies suggest that diet and physical activity may affect the symptoms and perhaps severity of sleep apnea.31–36 A recent randomized controlled trial in sedentary overweight/obese adults found that exercise training improved AHI independent of weight loss.37 It is possible that exercise independent of weight loss may have resulted in changes in central adiposity.38,39 Although changes in waist and neck circumference were examined and were not found to be independent predictors after change in weight was included in models, these measurements may be crude and quantitative analysis of fat such as by abdominal CT scan may be needed to examine this more closely.
A troubling finding was that so few study participants received treatment for OSA at the follow-up visits even though they and their primary care providers were informed in writing about the results of each sleep study. Similar findings were reported by investigators of the Sleep Heart Health Study who used the same disclosure strategy.40 In addition, a recent study found that primary care patients in a public health hospital were less likely to be referred for PSG compared with mammogram and endoscopy.41 Greater education of patients and their healthcare providers is needed to heighten awareness of the prevalence and potential clinical consequences of OSA in obese patients with type 2 diabetes.
Our prospective, randomized controlled trial on the effects of weight loss on sleep apnea has several strengths compared with prior studies. In addition to our larger sample of both men and women, to our knowledge, the study participants were followed longer than for any previous study. Our study has several important limitations. The exclusion from the analysis of the 41 participants who did not have sleep apnea (AHI ≥ 5 events/h) at baseline might have influenced the findings. Participants with mild disease in particular are more likely to change disease categories. Therefore, it is possible that those individuals who were not identified as having OSA at baseline may have had OSA at the 1-, 2-, and 4-y follow-up. If changes in AHI in this group were correlated with changes in weight, exclusion of those participants from the analysis might have contributed to misclassification of disease and disease severity. Misclassification might also explain why approximately 18% and 25% of the participants in the DSE group had improvements or worsening, respectively, in OSA severity category at year 4. Given the known night-to-night variability in AHI and the arbitrary cut point for diagnosing OSA, these findings may also have been due to misclassification. However, changes in weight and an aging effect might also help explain these findings. Given the relatively small number of participants without OSA at baseline and the missing data in many of those participants on follow-up due to different participants being studied in different year, it was not possible to assess the relationship between the changes in AHI and weight in this subgroup. Although we do not know the extent of misclassification, it is unlikely that it affected the results of this randomized controlled trial because it would have existed in both groups between which the comparisons were made. Regression analysis showed that weight change had a significant relationship with change in AHI.
Another significant limitation of our study is the presence of 37.5% dropout for the sleep studies at 4 y. This attrition was primarily due to Look AHEAD study participants declining to perform follow-up PSGs due to the burden of this repeated testing. To address the relatively high attrition, we examined whether the probability of a missing PSG was related to available covariates and whether the patterns of missing PSG were related to the change in AHI. No such associations were seen. Nevertheless, one cannot be completely sure that the results are not related to the dropout, because these were post hoc analyses. It is also important to note that the results of this study should not be generalized to younger patients, to patients without type 2 diabetes, or to patients with milder degrees of OSA.
CONCLUSION
In conclusion, the significant improvement in OSA severity among obese patients with type 2 diabetes and OSA achieved following 1 y of an ILI was maintained at 4 y despite a 50% weight regain over that period. The association of change in AHI with ILI independent of weight change suggests the importance of a structured, comprehensive treatment approach beyond just weight reduction in management of patients with OSA.
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Foster serves on the Scientific Advisory Board of Con Agra Foods, Nutri-system, Tate, Lyle and United Health Group. He has received grants from NIH, CDC, USDA, Robert Wood Johnson Foundation, Nutrisystem American Beverage Association and Novo-Nordisk. Dr. Jakicic is a member of Free & Clear Scientific Advisory Board, has grants or grants pending from BodyMedia, Inc., and receives payment for lectures by JennyCraig. Dr. Kuna receives grant support from Philips Respironics. Dr. Sanders is Editor-in-Chief and Editor for UpToDate®; Field Editor for Sleep Medicine and Deputy Editor for the journal SLEEP. He serves as a consultant to Philips Respironics. Dr. Zammit is a consultant for Actelion, Alexza, Arena, Aventis, Biovail, Boehringer-Ingelheim, Cephalon, Elan, Eli Lilly, Evotec, Forest, Glaxo Smith Kline, Jazz Pharmaceuticals, King Pharmaceuticals, Ligand, McNeil, Merck, Neurocrine Biosciences, Organon, Pfizer, Renovis, Sanofi-Aventis, Select Comfort, Sepracor, Shire, Somnus, Takeda Pharmaceuticals, Vela, and Wyeth-Ayerst Research. He also provides expert testimony for Acorda and has received grants or has grants pending from Abbott, Actelion, Ancile, Apnex, Arena, Aventis, Cephalon Inc, CHDI, Elan, Epic, Evotec, Forest, Galderma, Glaxo Smith Kline, H. Lundbeck A/S, King, Merck and Co., National Institute of Health (NIH), Neurim, Neurocrine Biosciences, Neurogen, Organon, Orphan Medical, Otsuka, Pfizer, Predix, Respironics, Sanofi-Aventis, Sanofi-Synthelabo, Schering-Plough, Sepracor, Shire, Somaxon, Takeda Pharmaceuticals North America, Targacept, Thymon, Transcept, UCB Pharma, Predix, Vanda, and Wyeth-Ayerst Research. Dr. Zammit has received payment for lectures from Neurocrine Biosciences, King Pharmaceuticals, McNeil, Sanofi-Aventis, Sanofi-Synthelabo, Sepracor, Takeda Pharmaceuticals, Vela Pharmaceuticals, and Wyeth-Ayerst Research. Dr. Wadden has received grant support from NutriSystem and serves on the advisory boards of Novo Nordisk, Orexigen and Vivus. Dr. Millman has served as a consultant for Johnson and Johnson Business Development. The other authors have indicated no financial conflicts of interest.
ACKNOWLEDGMENTS
Members of the Sleep AHEAD research group at each site consisted of the following individuals:
St.Luke's-Roosevelt Hospital/Clinilabs: Jon Freeman, PPSGT, PhD, Jennifer Patricio
University of Pennsylvania: Brian McGuckin, Stephanie Krauthamer-Ewing, Allan Pack, MB, ChB, PhD, Richard Schwab, MD, Mary Jones-Parker, RPSGT, Matthew Anastasi, RPSGT, Beth Staley, RPSGT, Liz Roben
Brown University: Marie Kearns, Caitlin Egan
Temple University: Nida Cassim, Valerie Darcey, Sakhena Hin, Stephanie Vander Veur
A detailed list of the Look AHEAD Research Group is provided in reference 11.
Members of the Observational Safety and Management Board were:
Kingman P. Strohl, MD (chair)
Donald L. Bliwise, PhD
Helaine E. Resnick, PhD
This study was supported by the National Institutes of Health NHLBI grant HL070301 and NIDDK grants DK60426, DK56992, and DK057135
Footnotes
A commentary on this article appears in this issue on page 627.
SUPPLEMENTAL MATERIAL
Polysomnography and Morphometrics
Figure S1 shows the Bland-Altman plot of agreement of apnea-hypopnea index (AHI) on simultaneous overnight polysomnograms (PSG) performed with the PS2 and Safiro monitors in 15 adult males with suspected OSA who were not participating in Sleep AHEAD. No differences in sleep stage and respiratory outcome measures were found between the two sets of recordings. The AHI on the Safiro recordings (mean [± SD], 60.9 ± 29.7 events per hour) and on the PS2 recordings (63.6 ± 32.1 events per hour) were not significantly different (P = 0.21) and were highly correlated (P < 0.0001; R = 0.97).
Intra-scorer reliability and the possibility of scoring drift over time was determined by having the masked scorer rescore 92 randomly chosen Sleep AHEAD PSGs over the course of the study. The original and rescored AHI measurements were highly correlated (r = 0.97; 95 percent confidence interval: 0.95 to 0.98). The median difference between scores is -0.15 events/h and the median absolute difference was 2.1 events/h. Figure S2 shows the Bland-Altman plot of agreement of AHI on rescoring.
There is some indication that the difference between scores decreased as the time between original and rescoring increased, but the effect was small, i.e., 2 units over the entire range time between scorings (Figure S3) and was attenuated when two cases with absolute differences greater than 10 are omitted.
Bland-Altman plot comparing agreement of apnea-hypopnea index (AHI) on simultaneous overnight PSGs performed with the PS2 and Safiro monitors in 15 adult males.
Bland-Altman plot of agreement of AHI on rescoring 92 randomly chosen Sleep AHEAD PSGs over the course of the study.
Difference between the initial and rescored AHI relative to the time between the two scorings.
REFERENCES
- 1.Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea; a population health perspective. Am J Respir Crit Care Med. 2002;165:1217–39. doi: 10.1164/rccm.2109080. [DOI] [PubMed] [Google Scholar]
- 2.Chan AS, Phillips CL, Cistulli PA. Obstructive sleep apnoea--an update. Intern Med J. 2010;40:102–6. doi: 10.1111/j.1445-5994.2009.02069.x. [DOI] [PubMed] [Google Scholar]
- 3.Foster GD, Sanders MH, Millman R, et al. Obstructive sleep apnea among obese patients with type 2 diabetes. Diabetes Care. 2009;32:1017–9. doi: 10.2337/dc08-1776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Foster GD, Borradaile KE, Sanders MH, et al. A randomized study on the effect of weight loss on obstructive sleep apnea among obese patients with type 2 diabetes: the Sleep AHEAD study. Arch Intern Med. 2009;169:1619–26. doi: 10.1001/archinternmed.2009.266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Look AHEAD Research Group. Wing RR. Long-term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes mellitus: four-year results of the Look AHEAD trial. Arch Intern Med. 2010;170:1566–75. doi: 10.1001/archinternmed.2010.334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Johansson K, Neovius M, Lagerros YT, et al. Effect of a very low energy diet on moderate and severe obstructive sleep apnoea in obese men: a randomised controlled trial. BMJ. 2009;339:b4609. doi: 10.1136/bmj.b4609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tuomilehto HP, Seppa JM, Partinen MM, et al. Lifestyle intervention with weight reduction: first-line treatment in mild obstructive sleep apnea. Am J Respir Crit Care Med. 2009;179:320–7. doi: 10.1164/rccm.200805-669OC. [DOI] [PubMed] [Google Scholar]
- 8.Johansson K, Hemmingsson E, Harlid R, et al. Longer term effects of very low energy diet on obstructive sleep apnoea in cohort derived from randomised controlled trial: prospective observational follow-up study. BMJ. 2011;342:d3017. doi: 10.1136/bmj.d3017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tuomilehto HP. Initial improvements in apnoea-hypopnoea index after very low calorie diet maintained for 1 year with weight loss maintenance program. Evid Based Med. 2012;17:32–33. doi: 10.1136/ebm.2011.100169. [DOI] [PubMed] [Google Scholar]
- 10.Tuomilehto H, Gylling H, Peltonen M, et al. Sustained improvement in mild obstructive sleep apnea after a diet- and physical activity-based lifestyle intervention: postinterventional follow-up. Am J Clin Nutr. 2010;92:688–96. doi: 10.3945/ajcn.2010.29485. [DOI] [PubMed] [Google Scholar]
- 11.Look AHEAD Research G. Bray G, Gregg E, et al. Baseline characteristics of the randomised cohort from the Look AHEAD (Action for Health in Diabetes) study. Diab Vasc Dis Res. 2006;3:202–15. doi: 10.3132/dvdr.2006.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Look AHEAD Research Group. Pi-Sunyer X, Blackburn G, et al. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the Look AHEAD trial. Diabetes Care. 2007;30:1374–83. doi: 10.2337/dc07-0048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Look AHEAD Research Group. Wadden TA, West DS, et al. The Look AHEAD study: a description of the lifestyle intervention and the evidence supporting it. Obesity (Silver Spring) 2006;14:737–52. doi: 10.1038/oby.2006.84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ryan DH, Espeland MA, Foster GD, et al. Look AHEAD (Action for Health in Diabetes): design and methods for a clinical trial of weight loss for the prevention of cardiovascular disease in type 2 diabetes. Control Clin Trials. 2003;24:610–28. doi: 10.1016/s0197-2456(03)00064-3. [DOI] [PubMed] [Google Scholar]
- 15.Iber C, Ancoli-Israel S, Chesson AL, Quan SF for the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events. Westchester, IL: American Academy of Sleep Medicine; 2007. [Google Scholar]
- 16.Kushida CA, Littner MR, Morgenthaler T, et al. Practice parameters for indications for polysomnography and related procedures: an update for 2005. Sleep. 2005;28:499–521. doi: 10.1093/sleep/28.4.499. [DOI] [PubMed] [Google Scholar]
- 17.American Academy of Sleep Medicine Task Force. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. Sleep. 1999;22:667–89. [PubMed] [Google Scholar]
- 18.Kohler M, Stoewhas AC, Ayers L, et al. Effects of continuous positive airway pressure therapy withdrawal in patients with obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2011;184:1192–9. doi: 10.1164/rccm.201106-0964OC. [DOI] [PubMed] [Google Scholar]
- 19.Calloway C, Chumlea W, Bouchard C. Circumferences. In: Lohmann TG, Roche AF, Martorell R, editors. Anthropometric standardization manual. Champaign, IL: Human Kinetics; 1988. pp. 39–64. [Google Scholar]
- 20.Hedeker D, Gibbons RD. Application of random-effects pattern-mixture models for missing data in longitudinal studies. Psychol Methods. 1997;2:64–78. [Google Scholar]
- 21.Bixler EO, Vgontzas AN, Lin HM, et al. Prevalence of sleep-disordered breathing in women: effects of gender. Am J Respir Crit Care Med. 2001;163:608–13. doi: 10.1164/ajrccm.163.3.9911064. [DOI] [PubMed] [Google Scholar]
- 22.Bixler EO, Vgontzas AN, Ten Have T, Tyson K, Kales A. Effects of age on sleep apnea in men: I, prevalence and severity. Am J Respir Crit Care Med. 1998;157:144–8. doi: 10.1164/ajrccm.157.1.9706079. [DOI] [PubMed] [Google Scholar]
- 23.Young T, Shahar E, Nieto FJ, et al. Predictors of sleep-disordered breathing in community-dwelling adults: the Sleep Heart Health Study. Arch Intern Med. 2002;162:893–900. doi: 10.1001/archinte.162.8.893. [DOI] [PubMed] [Google Scholar]
- 24.Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. doi: 10.1016/S0140-6736(05)71141-7. [DOI] [PubMed] [Google Scholar]
- 25.Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342:1378–84. doi: 10.1056/NEJM200005113421901. [DOI] [PubMed] [Google Scholar]
- 26.Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034–41. doi: 10.1056/NEJMoa043104. [DOI] [PubMed] [Google Scholar]
- 27.Bahammam A, Delaive K, Ronald J, Manfreda J, Roos L, Kryger MH. Health care utilization in males with obstructive sleep apnea syndrome two years after diagnosis and treatment. Sleep. 1999;22:740–7. doi: 10.1093/sleep/22.6.740. [DOI] [PubMed] [Google Scholar]
- 28.Kapur V, Blough DK, Sandblom RE, et al. The medical cost of undiag-nosed sleep apnea. Sleep. 1999;22:749–55. doi: 10.1093/sleep/22.6.749. [DOI] [PubMed] [Google Scholar]
- 29.Hemmingsson E. Does medically induced weight loss improve obstructive sleep apnea in the obese: review of randomized trials. Clinical Obesity. 2011;1:26–30. doi: 10.1111/j.1758-8111.2010.00004.x. [DOI] [PubMed] [Google Scholar]
- 30.Hemmingsson E, Johansson K, Neovius M. Randomized controlled trial on weight loss in obstructive sleep apnea: inappropriate analysis limits main conclusion. Am J Clin Nutr. 2011;93:474. doi: 10.3945/ajcn.110.006130. [DOI] [PubMed] [Google Scholar]
- 31.Hong S, Dimsdale JE. Physical activity and perception of energy and fatigue in obstructive sleep apnea. Med Sci Sports Exerc. 2003;35:1088–92. doi: 10.1249/01.MSS.0000074566.94791.24. [DOI] [PubMed] [Google Scholar]
- 32.Norman JF, Von Essen SG, Fuchs RH, McElligott M. Exercise training effect on obstructive sleep apnea syndrome. Sleep Res Online. 2000;3:121–9. [PubMed] [Google Scholar]
- 33.Barnes M, Goldsworthy UR, Cary BA, Hill CJ. A diet and exercise program to improve clinical outcomes in patients with obstructive sleep apnea--a feasibility study. J Clin Sleep Med. 2009;5:409–15. [PMC free article] [PubMed] [Google Scholar]
- 34.Peppard PE, Young T. Exercise and sleep-disordered breathing: an association independent of body habitus. Sleep. 2004;27:480–4. doi: 10.1093/sleep/27.3.480. [DOI] [PubMed] [Google Scholar]
- 35.Quan SF, O'Connor GT, Quan JS, et al. Association of physical activity with sleep-disordered breathing. Sleep Breath. 2007;11:149–57. doi: 10.1007/s11325-006-0095-5. [DOI] [PubMed] [Google Scholar]
- 36.Vasquez MM, Goodwin JL, Drescher AA, Smith TW, Quan SF. Associations of dietary intake and physical activity with sleep disordered breathing in the Apnea Positive Pressure Long-Term Efficacy Study (APPLES) J Clin Sleep Med. 2008;4:411–8. [PMC free article] [PubMed] [Google Scholar]
- 37.Kline CE, Crowley EP, Ewing GB, et al. The effect of exercise training on obstructive sleep apnea and sleep quality: a randomized controlled trial. Sleep. 2011;34:1631–40. doi: 10.5665/sleep.1422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Irwin ML, Yasui Y, Ulrich CM, et al. Effect of exercise on total and intra-abdominal body fat in postmenopausal women: a randomized controlled trial. JAMA. 2003;289:323–30. doi: 10.1001/jama.289.3.323. [DOI] [PubMed] [Google Scholar]
- 39.Stewart KJ, Bacher AC, Turner KL, et al. Effect of exercise on blood pressure in older persons: a randomized controlled trial. Arch Intern Med. 2005;165:756–62. doi: 10.1001/archinte.165.7.756. [DOI] [PubMed] [Google Scholar]
- 40.Gottlieb DJ, Yenokyan G, Newman AB, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the Sleep Heart Health Study. Circulation. 2010;122:352–60. doi: 10.1161/CIRCULATIONAHA.109.901801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Thornton JD, Chandriani K, Thornton JG, et al. Assessing the prioritization of primary care referrals for polysomnograms. Sleep. 2010;33:1255–60. doi: 10.1093/sleep/33.9.1255. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Bland-Altman plot comparing agreement of apnea-hypopnea index (AHI) on simultaneous overnight PSGs performed with the PS2 and Safiro monitors in 15 adult males.
Bland-Altman plot of agreement of AHI on rescoring 92 randomly chosen Sleep AHEAD PSGs over the course of the study.
Difference between the initial and rescored AHI relative to the time between the two scorings.