

Abstract
Hypercalciuria is the most common metabolic abnormality found in patients with calcium-containing kidney stones. Patients with hypercalciuria often excrete more calcium than they absorb, indicating a net loss of total body calcium. The source of this additional urine calcium is almost certainly the skeleton, the largest repository of calcium in the body. Hypercalciuric stone formers exhibit decreased bone mineral density (BMD) which is correlated with the increase in urine calcium excretion. The decreased BMD also correlates with an increase in markers of bone turnover, as well as increased fractures. In humans, it is difficult to determine the cause of the decreased BMD in hypercalciuric stone formers. To study the effect of hypercalciuria on bone we utilized our genetic hypercalciuric stone-forming (GHS) rats which were developed through successive inbreeding of the most hypercalciuric Sprague-Dawley rats. GHS rats excrete significantly more urinary calcium than similarly fed controls and all the GHS rats form kidney stones while control rats do not. The hypercalciuria is due to a systemic dysregulation of calcium homeostasis, with increased intestinal calcium absorption, enhanced bone mineral resorption and decreased renal tubule calcium reabsorption associated with an increase in vitamin D receptors in all these target tissues. We recently found that GHS rats fed an ample calcium diet have reduced BMD and their bones are more fracture prone, indicating an intrinsic disorder of bone not secondary to diet. Using this model, we should better understand the pathogenesis of hypercalciuria and stone formation in humans to ultimately improve bone health of patients with kidney stones.
Keywords: nephrolithiasis, hypercalciuria, bone density
Bone Resorption in Hypercalciuric Stone Formers
The majority of humans with calcium (Ca) -containing kidney stones are hypercalciuric compared to those who do not form stones [1–3]. Hypercalciuria increases urine supersaturation with respect to the solid phases of Ca hydrogen phosphate and Ca oxalate, enhancing the probability of nucleation and growth of crystals into clinically significant kidney stones [4]. Patients with hypercalciuria often excrete more calcium than they absorb reflecting a net loss of total body Ca [2, 5, 6]. A low calcium diet often leads to greater net Ca excretion than any increase in Ca absorption in hypercalciuric patients and renal stone formers, suggesting that the source of this additional urine (U) Ca is almost certainly the skeleton, the largest repository of body Ca [7]. Patients with fasting hypercalciuria have a marked reduction in spinal bone density [8] and Pietschmann et al. found lower spinal BMD in hypercalciuric compared to normocalciuric patients [9]. However, the bone pathology observed in patients with idiopathic hypercalciuria is not well defined.
Bone mineral density (BMD) is correlated inversely with UCa excretion in both men [10] and women [11] stone formers but not in non-stone formers [7]. A number of studies using a variety of methods including radiologic densitometry, quantitative computed tomography (CT), dual-energy x-ray absorptiometry and single-photon absorptiometry, confirm that patients with nephrolithiasis have a reduction, generally mild, in BMD compared to matched controls [5, 9, 12–16].
Jaeger et al. found that stone formers were slightly shorter and had a significantly lower BMD at the tibial diaphysis and the tibial epiphysis compared to controls [12]. Giannini found that 49 recurrent stone formers with idiopathic hypercalciuria had a lower lumbar spine Z-score than normal controls [13]. Misael da Silva et al. examined bone formation and resorption parameters in 40 stone formers and classified 10 as osteopenic [14]. Tasca et al. found a more negative Z-score in L1–L2 vertebrae in hypercalciuric patients than in controls [15]. After adjusting for a large number of variables, an analysis of the 3rd National Health and Nutrition Examination Survey (NHANES III) demonstrated that men with a history of kidney stones have a lower femoral neck BMD than those without a history of stone formation [17]. Analysis of a large cohort of older men again demonstrated an association between kidney stones and decreased BMD of the femoral neck [18]. Thus decreased bone density has been found both in vertebrae and long bones of hypercalciuric stone formers compared to normal patients; however, it is not clear whether either of these bone types is more predominantly affected than the other.
Idiopathic hypercalciuria has been associated with markers of increased bone turnover which may provide a possible explanation for the decreased BMD [16, 19]. Urinary hydroxyproline is increased in unselected patients with idiopathic hypercalciuria [16] and serum osteocalcin levels are elevated in stone formers who have a defect in renal tubule Ca reabsorption, but not in those with only excessive intestinal Ca absorption [19]. Bone turnover studies with 47Ca demonstrated increased bone formation and resorption with the latter predominating [20]. Cytokines known to increase bone resorption have also been shown to be elevated in patients with idiopathic hypercalciuria [8, 14, 21, 22]. Pacifici has shown that the cytokine interleukin 1 (IL-1) is elevated in the monocytes of patients with fasting hypercalciuria but not in those with excessive intestinal Ca absorption [8]. Weisinger confirmed the elevation in IL-1 and also demonstrated that IL-6 and tumor necrosis factorα (TNF-α) were elevated [21]. Similar observations have been made by others [14, 22]. In a few studies where bone biopsies were examined, a picture compatible with low bone formation and turnover has been most consistently observed [16, 23]. A retrospective study of idiopathic hypercalciuric male stone formers found the only biologic factor associated with the low BMD in these patients was a fasting hypercalciuria on a 2 day Ca-restricted diet [24]. This suggested a parathyroid-independent pathologic process resulting in bone Ca efflux that might be exploited as a tool to identify hypercalciuric patients at risk for decreased BMD.
Based on the observed changes in BMD and bone turnover in patients with nephrolithiasis, it is perhaps not surprising that they have a fracture rate that is higher than that of subjects without nephrolithiasis [16]. In NHANES III there was an increased risk of wrist and spine fractures in stone formers [17] and, in a retrospective analysis, stone formers had an increased incidence of vertebral fractures, but not fractures at other sites [16]. The change in fracture rate occurs over a much longer time frame than changes in BMD. As the decreased BMD manifests itself much sooner than increased fracture rate, there has been more focus on the decreased BMD associated with hypercalciuria and nephrolithiasis to try to understand the underlying mechanisms of the changes in bone that occur as a result of the hypercalciuria. The reduction in BMD associated with idiopathic hypercalciuria in humans could be caused by a primary disorder of bone formation and/or resorption. Alternatively, the decrease in BMD could be due to differences between stone formers and normal controls in renal handling of dietary constitutents such as Ca, sodium and/or protein, perhaps over a lifetime. Each of these substances influences urine Ca excretion [25] and potentially, BMD or bone structure. In humans it is virtually impossible to experimentally determine the primary causative factors leading to the observed decline in BMD.
Hypercalciuric Rats as a Model for Human Idiopathic Hypercalciuria
To help understand the mechanism of idiopathic hypercalciuria in humans, we developed an animal model of this disorder in which dietary and environmental factors can be readily controlled over a lifetime [26]. Through over 90 generations of successive inbreeding of the most hypercalciuric progeny of the most hypercalciuric male and female of an initial large group of Sprague-Dawley (SD) rats, we established a strain of rats that now consistently excretes ~8–10 times as much urinary Ca as comparably fed SD controls (Table 1, Fig. 1). As these hypercalciuric rats form kidney stones on a normal rat diet [26] they have been termed genetic hypercalciuric stone-forming (GHS) rats. Compared to SD, the GHS rats have a normal serum Ca but absorb far more dietary Ca [26], similar to observations in man [1]. The increase in intestinal Ca absorption is due to a significant increase in the mucosal to serosal (absorptive) Ca flux with no change in the serosal to mucosal (secretory) flux [27]. When the hypercalciuric rats are fed a diet essentially devoid of Ca, UCa excretion remains significantly elevated compared with that of similarly fed SD rats [28], indicating there is also a defect in renal tubule Ca reabsorption or an increase in bone resorption, or both, again similar to observations in humans [29, 30].
Table 1.
Comparison of characteristics of kidney stone-forming hypercalciuric humans with GHS rats
| Hypercalciuric Stone-Forming (IH) Humans | Genetic Hypercalciuric Stone-Forming (GHS) rats | |
|---|---|---|
| Urine Ca Excretion | Increased (by definition) | Increased [26–28, 31, 33, 37, 41, 42, 45, 70–72] |
| Intestinal Ca Absorption | Increased in most patients [1, 5, 20, 73] | Increased [26, 27, 37, 40, 74] |
| Renal Tubular Ca Reabsorption | Decreased in many patients [30, 75, 76] | Decreased[33] |
| Bone Resorption | Increased in most patients – as evidenced by markers of bone resorption [8, 14, 16, 19, 21, 22] | Increased[31, 32] |
| Bone Mineral Density | Decreased in most patients [1, 5, 9, 12–14, 29, 77] | Decreased[46] |
| Serum PTH | Normal to reduced [77–80] or elevated [78] | Reduced [72] |
| Serum 1,25(OH)2D3 | Normal to elevated [29, 73, 77, 78, 81, 82]] | Normal to elevated [28, 34, 35, 37, 74] |
| Vitamin D Receptor | Increased number [39] or no increase [83] Gene polymorphisms [84–88] |
Increased number [37, 74, 89] |
| Ca Receptor | Changes in number not reported. Activating and inactivating mutations associated with hyper- and hypo-calciuria, respectively [90, 91]; gene polymorphisms[92, 93] | Increased number [34] Treatment with cinacalcet activates the receptor – associated with increased UCa in SD but not GHS rats [72] |
| Stone formation | Consequence of hypercalciuria [1, 6, 73, 94] | Present [26, 40, 41, 45] |
Fig. 1. Progression of hypercalciuria in GHS rats.
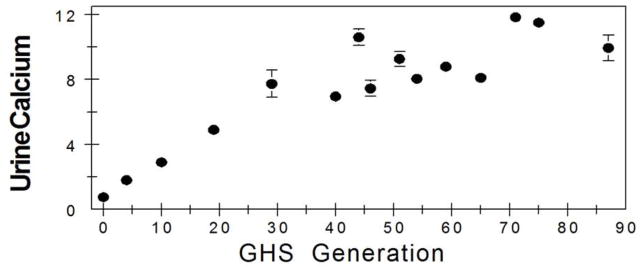
Through successive inbreeding of the most hypercalciuric progeny of SD rats we have established a strain of genetic hypercalciuric stone-forming (GHS) rats that all excrete ~8–10 times as much urinary Ca as the parental strain. All data are from published studies [26, 36, 46, 57, 69].
To determine whether there is a primary defect in bone homeostasis we fed adult GHS rats a low Ca diet and found that they were in negative Ca balance. The concomitant administration of a bisphosphonate, which significantly inhibits bone resorption, significantly reduces urinary Ca excretion indicating that bone is the source of this additional urinary Ca (Fig. 2) [31]. We then cultured bone from neonatal GHS rats and SD neonates. In vitro there is no difference in baseline or PTH-stimulated bone resorption between neonatal rat calvariae from the GHS rats compared to the parental SD rats [32]. However, there is enhanced net Ca efflux from cultured GHS rat calvariae in response to increasing amounts of 1,25(OH)2D3 in comparison to calvariae from SD rats. The increased Ca efflux in response to 1,25(OH)2D3 in the GHS rat bones could reflect a decrease in osteoblastic bone formation, an increase in osteoclastic bone resorption, or a combination of the two. These findings indicate a defect in bone mineral Ca efflux in addition to the increase in intestinal absorption of Ca.
Fig. 2. Effect of the bisphosphonate, alendronate, on urine Ca excretion.
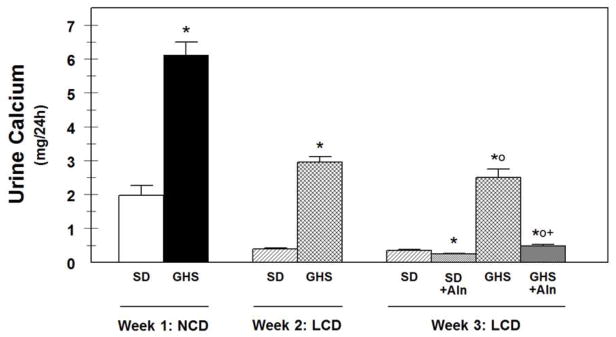
Urine Ca was measured from SD and GHS rats initially on a normal Ca diet (NCD) for 1 week. These rats were then switched to a low Ca diet (LCD). After an additional week on LCD, half of each group was also given alendronate (Aln) and UCa measured. * p < 0.05 vs SD; op<0.05 vs SD on LCD; +p<0.05 vs GHS on LCD [31].
To determine if the hypercalciuria was also secondary to an inherent defect in renal tubular Ca reabsorption we performed clearance studies. We found that the fractional excretion of Ca is significantly higher in parathyroidectomized GHS rats compared to SD rats [33]. The increased excretion is not diminished on a low Ca diet. The effect of the diuretic chlorothiazide is greater, and that of furosemide is smaller, in the GHS compared with SD rats, suggesting that the defect in renal Ca handling might be at the level of the thick ascending limb. These results indicate an additional primary defect in renal Ca reabsorption.
Thus, the hypercalciuric rats have a systemic dysregulation in Ca homeostasis: they absorb more intestinal Ca, they resorb more bone, and they do not adequately reabsorb filtered Ca (Fig. 3). We have found that in the principal Ca transporting tissues, bone, kidney and intestine, these hypercalciuric rats have an increased number of vitamin D receptors (VDR) and Ca sensing receptors (CaR) [34–37]. This can account for the increased responsiveness we found for neonatal GHS calvariae to 1,25(OH)2D3 [32]. The transcription factor Snail decreases VDR [38] and importantly we have recently reported that levels of Snail are lower in GHS rats [36], suggesting potential underlying mechanism(s) for the hypercalciuria. In at least one human study, circulating monocytes from patients with idiopathic hypercalciuria were shown to have an increased number of VDR [39]; however, we do not know if hypercalciuric humans have altered levels of Snail.
Fig. 3. Systemic abnormality in Ca homeostasis in GHS rats.
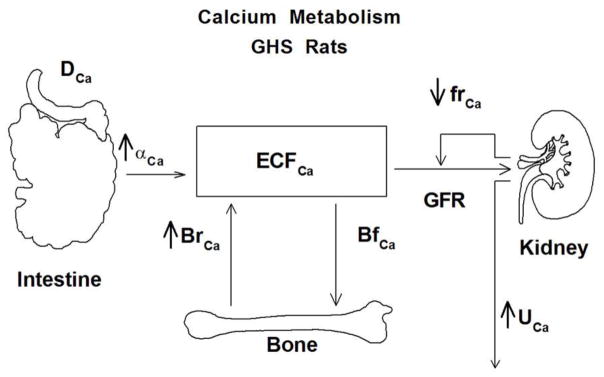
When compared to control rats fed a comparable dietary Ca (DCa) the GHS rats exhibit increased intestinal Ca absorption (αCa), increased bone resorption (BrCa) and decreased renal Ca reabsorption (frCa) [26].
After eating standard rat chow (1.2% Ca) for 18 wks virtually all of the GHS rats form kidney stones while there is no evidence for stone formation in comparably fed SD rats [26, 40]. The stones contain only Ca and phosphate (P), without oxalate (Ox), and by X-ray diffraction the stones are exclusively poorly crystalline apatite [40–42]. Calcium phosphate is the initial solid phase found in patients with calcium oxalate stone disease [43, 44]. When fed additional hydroxyproline, an amino acid which is metabolized to Ox, these rats form CaOx kidney stones [45], the most common kidney stones formed by man [45]. The pathophysiology responsible for the hypercalciuria parallels that found in hypercalciuric humans and is thus an excellent model for understanding the mechanism of the hypercalciuria (Table 1).
GHS Rat Bone
As observed in human hypercalciuric patients, the BMD and bone strength in GHS rats is reduced even when fed a diet with ample Ca (Fig. 4) [46]. The GHS rats have a reduction in cortical (humerus) and trabecular (L(1)–L(5) vertebrae BMD and a decrease in trabecular volume and thickness. GHS rats do not have a change in vertebral strength (failure stress), ductibility (failure strain), stiffness (modulus), or toughness, whereas in the humerus, there is reduced ductibility and toughness and an increase in modulus, indicating that the defect in mechanical properties is mainly manifested in cortical, rather than trabecular, bone. In the GHS rat the cortical bone is more mineralized than the trabecular bone. Thus, the GHS rats, fed an ample Ca diet, have reduced BMD with reduced trabecular volume, mineralized volume, and thickness, and their bones are more brittle and fracture prone, indicating that GHS rats have an underlying defect of bone not related to a deficiency in dietary Ca.
Fig. 4. GHS rats have a reduction in bone mineral density (BMD).
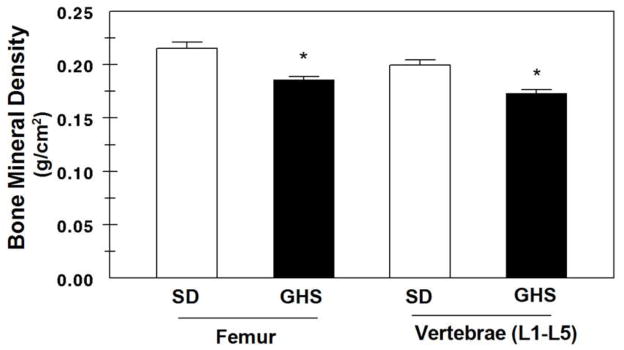
Comparison of BMD from SD (open bars) and GHS (solid bars) rat femur and vertebrae fed a normal 1.2 % Ca diet. Groups of 8 female rats, initially weighing 140 gm, were kept on the diet for 6 weeks. Results are mean ± SE. * p<0.05 vs SD [46].
Thiazide diuretic agents such as chlorthalidone (CTD) reduce urine Ca excretion in normals [47], patients with hypercalciuria [48] and rats [49]. These drugs act by stimulating Ca reabsorption in the distal convoluted tubule [47] and by producing extracellular fluid volume depletion [50]. Thiazide diuretics are used to treat CaOx stone formers [1, 2]; a meta-analysis revealed that in studies of more than two years duration, there was a significant reduction in stone recurrence rate [51]. A number of studies have shown that when thiazides are used to treat hypertension [52] there is also a reduction of osteoporotic fractures [53, 54] and often an increase in BMD [55]. There are very few studies of the effect of other agents used to treat hypercalciuria or stone formation on BMD, although one long-term study of potassium citrate therapy in idiopathic calcium stone formers did find a longitudinal increase in forearm BMD after two years of therapy [56].
We used GHS rats to test the hypothesis that CTD would have a favorable effect on BMD and bone quality. GHS rats were fed an ample Ca diet and half were also fed CTD [57]. As expected CTD reduces UCa in GHS rats [49, 58]. In the axial and appendicular skeleton an increase in trabecular mineralization is observed with CTD compared to controls [57]. CTD also improved the architecture of trabecular bone. By μCT analysis, trabecular bone volume (BV/TV), trabecular thickness and trabecular number are increased with CTD. A significant increase in trabecular thickness with CTD was confirmed by static histomorphometry. CTD also improves the connectivity of trabecular bone. Significant improvements in vertebral strength and stiffness were measured by vertebral compression. Conversely, a slight loss of bending strength is detected in the femoral diaphysis with CTD. These results obtained in hypercalciuric rats suggest that CTD can favorably influence vertebral fracture risk. Further studies will be necessary to more precisely define the mechanism of the decrease in BMD associated with the hypercalciuria in the GHS rat.
Several studies have examined the effect of thiazides on bone cells in vitro. Hydrochlorothiazide was found to inhibit bone resorption by isolated rat osteoclasts at relatively high concentrations [59]. Thiazides were also shown to decrease bone resorption in organ cultures, possibly by inhibition of osteoclast differentiation of hematopoietic precursors[60]. Alternatively, thiazides may directly act on osteoblasts to inhibit the sodium-chloride cotransporter [61], although these drugs continued to inhibit pit formation in cocultures of osteoblasts and marrow cells from mice lacking this cotransporter [60]. Thiazides have also been found to selectively inhibit osteocalcin and M-CSF from human osteoblastic cells [62, 63] and may stimulate osteoblast differentiation [64], effects which could directly promote bone formation while blocking bone resorption. The mechanism by which CTD increases BMD in the GHS rat has not yet been studied.
Future challenges
The prevalence of kidney stone disease has increased in the past few decades [65]. Hypercalciuria leading to nephrolithiasis is a systemic disorder of calcium homeostasis and is associated with bone disease leading to fractures, as well as chronic kidney disease, increased risk of coronary artery disease, hypertension and other metabolic disorders [66].
A primary end point for successful metabolic treatment of patients with Ca-containing kidney stones is a decrease in the rate of stone recurrence [1–3]. As discussed above, stone formers have both a reduction in BMD [5, 9, 12–17, 67] and an increase in fracture rate compared to non-stone formers [16, 17]. While decreasing recurrent stone formation is an important goal, what should concern clinicians equally is maintaining and improving the patient’s BMD and bone quality [67]. While acute stone episodes often are resolved quickly, patients may live the remainder of their lives in pain and with reduced function due to the osseous complications related to fractures [68]. We are utilizing the GHS rats, not only to better understand the pathogenesis of hypercalciuria and stone formation, but to study their bones as well. With the knowledge gained from this important model, which closely mirrors the physiology of hypercalciuria and stone formation in man, we will be better able to understand and treat the bone disorders in hypercalciuric stone formers and ultimately reduce fractures.
Acknowledgments
This work was supported by grants RO1 DK 75462 and AR 46289 from the National Institutes of Health.
Footnotes
Disclosures:
None
Reference List
- 1.Monk RD, Bushinsky DA. Kidney stones. In: Kronenberg HM, Melmed S, Polonsky KS, Larsen PR, editors. Williams Textbook of Endocrinology. W.B. Saunders; Philadelphia: 2011. pp. 1350–1367. [Google Scholar]
- 2.Bushinsky DA, Coe FL, Moe OW. Nephrolithiasis. In: Brenner BM, editor. The Kidney. W.B. Saunders; Philadelphia: 2012. pp. 1455–1507. [Google Scholar]
- 3.Worcester EM, Coe FL. Calcium Kidney Stones. New England Journal of Medicine. 2010;363:954–963. doi: 10.1056/NEJMcp1001011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bushinsky DA, Moe OW. Calcium Stones. In: De Broe ME, editor. Oxford Textbook of Clinical Nephrology. Oxford: 2012. [Google Scholar]
- 5.Bushinsky DA. Recurrent hypercalciuric nephrolithiasis - does diet help? N Eng J Med. 2002;346:124–125. doi: 10.1056/NEJM200201103460210. [DOI] [PubMed] [Google Scholar]
- 6.Pak CYC. Pathophysiology of calcium nephrolithiasis. In: Seldin DW, Giebisch G, editors. The Kidney: Physiology and Pathophysiology. Raven Press, Ltd; New York: 1992. pp. 2461–2480. [Google Scholar]
- 7.Asplin JR, Bauer KA, Kinder J, Muller G, Coe BJ, Parks JH, Coe FL. Bone mineral density and urine calcium excretion among subjects with and without nephrolithiasis. Kidney Int. 2003;63:662–669. doi: 10.1046/j.1523-1755.2003.00763.x. [DOI] [PubMed] [Google Scholar]
- 8.Pacifici R, Rothstein M, Rifas L, et al. Increased monocyte interleukin-1 activity and decreased vertebral bone density in patients with fasting idiopathic and hypercalciuria. J Clin Endocrinol Metab. 1990;71:138–145. doi: 10.1210/jcem-71-1-138. [DOI] [PubMed] [Google Scholar]
- 9.Pietschmann F, Breslau NA, Pak CYC. Reduced vertebral bone density in hypercalciuric nephrolithiasis. J Bone Miner Res. 1992;7:1383–1388. doi: 10.1002/jbmr.5650071205. [DOI] [PubMed] [Google Scholar]
- 10.Vezzoli G, Soldati L, Ardila M, et al. Urinary calcium is a determinant of bone mineral density in elderly men participating in the InCHIANTI study. Kid Int. 2005;67:2006–2014. doi: 10.1111/j.1523-1755.2005.00302.x. [DOI] [PubMed] [Google Scholar]
- 11.Giannini S, Nobile M, Dalle Carbonare L, et al. Hypercalciuria is a common and important finding in postmenopausal women with osteoporosis. Eur J Endocrinol. 2003;149:209–213. doi: 10.1530/eje.0.1490209. [DOI] [PubMed] [Google Scholar]
- 12.Jaeger P, Lippuner K, Casez JP, Hess B, Ackerman D, Hug C. Low bone mass in idiopathic renal stone formers: magnitude and significance. Journal of Bone and Mineral Research. 1994;9:1525–1532. doi: 10.1002/jbmr.5650091004. [DOI] [PubMed] [Google Scholar]
- 13.Giannini S, Nobile M, Sartori L, Calo L, Tasca A, Dalle Carbonare L, Ciuffreda M, D’Angelo A, Pagano F, Crepaldi G. Bone density and skeletal metabolism are altered in idiopathic hypercalciuria. Clin Nephrol. 1998;50:94–100. [PubMed] [Google Scholar]
- 14.Misael da Silva AM, dos Reis LM, Pereira RC, Futata E, Branco-Martins CT, Noronha IL, Wajchemberg BL, Jorgetti V. Bone involvement in idiopathic hypercalciuria. Clin Nephrol. 2002;57:183–191. doi: 10.5414/cnp57183. [DOI] [PubMed] [Google Scholar]
- 15.Tasca A, Cacciola A, Ferrarese P, Ioverno E, Visona E, Bernardi C, Nobile M, Giannini S. Bone alterations in patients with idiopathic hypercalciuria and calcium nephrolithiasis. Urology. 2002;59:865–869. doi: 10.1016/s0090-4295(02)01626-6. [DOI] [PubMed] [Google Scholar]
- 16.Heilberg IP, Weisinger JR. Bone disease in idiopathic hypercalciuria. Curr Opin Nephrol Hypertens. 2006;15:394–402. doi: 10.1097/01.mnh.0000232880.58340.0c. [DOI] [PubMed] [Google Scholar]
- 17.Lauderdale DS, Thisted RA, Wen M, Favus M. Bone mineral density and fracture among prevalent kidney stone cases in the Third National Health and Nutrition Examination Survey. J Bone Miner. 2001;16:1893–1898. doi: 10.1359/jbmr.2001.16.10.1893. [DOI] [PubMed] [Google Scholar]
- 18.Cauley JA, Blackwell T, Zmuda JM, Fullman RL, Ensrud KE, Stone KL, Barrett-Connor E, Orwoll ES. Correlates of trabecular and cortical volumetric bone mineral density at the femoral neck and lumbar spine: the osteoporotic fractures in men study (MrOS) J Bone Miner Res. 2010;25:1958–1971. doi: 10.1002/jbmr.86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Urivetzky M, Anna PS, Smith AD. Plasma osteocalcin levels in stone disease: A potential aid in the differential diagnosis of calcium nephrolithiasis. J Urol. 1988;139:12–14. doi: 10.1016/s0022-5347(17)42273-7. [DOI] [PubMed] [Google Scholar]
- 20.Liberman UA, Sperling O, Atsmon A, Frank M, Modan M, deVries A. Metabolic and calcium kinetic studies in idiopathic hypercalciuria. J Clin Invest. 1968;47:2580–2590. doi: 10.1172/JCI105940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Weisinger JR, Alonzo E, Bellorin-Font E, et al. Possible role of cytokines on the bone mineral loss in idiopathic hypercalciuria. Kid Int. 1996;49:244–250. doi: 10.1038/ki.1996.34. [DOI] [PubMed] [Google Scholar]
- 22.Ghazali A, Fuentes V, Desaint C, et al. Low bone mineral density and peripheral blood monocyte activation profile in calcium stone formers with idiopathic hypercalciuria. J Clin Endocrinol Metab. 1997;82:32–38. doi: 10.1210/jcem.82.1.3649. [DOI] [PubMed] [Google Scholar]
- 23.Steiniche T, Mosekilde L, Christensen MS, Melsen F. Histomorphometric analysis of bone in idiopathic hypercalciuria before and after treatment with thiazide. APMIS. 1989;97:302–308. doi: 10.1111/j.1699-0463.1989.tb00792.x. [DOI] [PubMed] [Google Scholar]
- 24.Letavernier E, Traxer O, Daudon M, Tligui M, Hubert-Brierre J, Guerrot D, Sebag A, Baud L, Haymann JP. Determinants of osteopenia in male renal-stone-disease patients with idiopathic hypercalciuria. Clinical journal of the American Society of Nephrology: CJASN. 2011;6:1149–1154. doi: 10.2215/CJN.10191110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lemann J, Jr, Bushinsky DA, Hamm LL. Bone buffering of acid and base in humans. Am J Physiol Renal Physiol. 2003;285:F811–F832. doi: 10.1152/ajprenal.00115.2003. [DOI] [PubMed] [Google Scholar]
- 26.Bushinsky DA, Frick KK, Nehrke K. Genetic hypercalciuric stone-forming rats. Curr Opinion Nephrol Hyperten. 2006;15:403–418. doi: 10.1097/01.mnh.0000232881.35469.a9. [DOI] [PubMed] [Google Scholar]
- 27.Bushinsky DA, Favus MJ. Mechanism of hypercalciuria in genetic hypercalciuric rats: inherited defect in intestinal calcium transport. J Clin Invest. 1988;82:1585–1591. doi: 10.1172/JCI113770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kim M, Sessler NE, Tembe V, Favus MJ, Bushinsky DA. Response of genetic hypercalciuric rats to a low calcium diet. Kidney Int. 1993;43:189–196. doi: 10.1038/ki.1993.31. [DOI] [PubMed] [Google Scholar]
- 29.Coe FL, Favus MJ, Crockett T, Strauss AL, Parks JH, Porat A, Gantt C, Sherwood LM. Effects of low-calcium diet on urine calcium excretion, parathyroid function and serum 1,25(OH)2D3 levels in patients with idiopathic hypercalciuria and in normal subjects. Am J Med. 1982;72:25–32. doi: 10.1016/0002-9343(82)90567-8. [DOI] [PubMed] [Google Scholar]
- 30.Pak CY. Kidney stones. Lancet. 1998;351:1797–1801. doi: 10.1016/S0140-6736(98)01295-1. [DOI] [PubMed] [Google Scholar]
- 31.Bushinsky DA, Neumann KJ, Asplin J, Krieger NS. Alendronate decreases urine calcium and supersaturation in genetic hypercalciuric rats. Kidney Int. 1999;55:234–243. doi: 10.1046/j.1523-1755.1999.00247.x. [DOI] [PubMed] [Google Scholar]
- 32.Krieger NS, Stathopoulos VM, Bushinsky DA. Increased sensitivity to 1,25(OH)2D3 in bone from genetic hypercalciuric rats. Am J Physiol (Cell Physiol) 1996;271:C130–C135. doi: 10.1152/ajpcell.1996.271.1.C130. [DOI] [PubMed] [Google Scholar]
- 33.Tsuruoka S, Bushinsky DA, Schwartz GJ. Defective renal calcium reabsorption in genetic hypercalciuric rats. Kidney Int. 1997;51:1540–1547. doi: 10.1038/ki.1997.212. [DOI] [PubMed] [Google Scholar]
- 34.Yao J, Karnauskas AJ, Bushinsky DA, Favus MJ. Regulation of renal calcium-sensing receptor gene expression in response to 1,25(OH)2D3 in genetic hypercalciuric stone forming rats. Journal of the American Society of Nephrology. 2005;16:1300–1308. doi: 10.1681/ASN.2004110991. [DOI] [PubMed] [Google Scholar]
- 35.Karnauskas AJ, van Leeuwen JP, van den Bemd GJ, Kathpalia PP, DeLuca HF, Bushinsky DA, Favus MJ. Mechanism and function of high vitamin D receptor levels in genetic hypercalciuric stone-forming rats. Journal of Bone and Mineral Research. 2005;20:447–454. doi: 10.1359/JBMR.041120. [DOI] [PubMed] [Google Scholar]
- 36.Bai S, Wang H, Shen J, Zhou R, Bushinsky DA, Favus MJ. Elevated vitamin D receptor levels in genetic hypercalciuric stone-forming rats are associated with downregulation of Snail. Journal of Bone and Mineral Research. 2010;25:830–840. doi: 10.1359/jbmr.091010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Li XQ, Tembe V, Horwitz GM, Bushinsky DA, Favus MJ. Increased intestinal vitamin D receptor in genetic hypercalciuric rats: a cause of intestinal calcium hyperabsorption. J Clin Invest. 1993;91:661–667. doi: 10.1172/JCI116246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Larriba MaJs, Bonilla F, Mu¤oz A. The transcription factors Snail1 and Snail2 repress vitamin D receptor during colon cancer progression. The Journal of Steroid Biochemistry and Molecular Biology. 2010;121:106–109. doi: 10.1016/j.jsbmb.2010.01.014. [DOI] [PubMed] [Google Scholar]
- 39.Favus MJ, Karnauskas AJ, Parks JH, Coe FL. Peripheral blood monocyte vitamin D receptor levels are elevated in patients with idiopathic hypercalciuria. J Clin Endocrinol Metab. 2004;89:4937–4943. doi: 10.1210/jc.2004-0412. [DOI] [PubMed] [Google Scholar]
- 40.Bushinsky DA, Grynpas MD, Nilsson EL, Nakagawa Y, Coe FL. Stone formation in genetic hypercalciuric rats. Kidney Int. 1995;48:1705–1713. doi: 10.1038/ki.1995.468. [DOI] [PubMed] [Google Scholar]
- 41.Asplin JR, Bushinsky DA, Singharetnam W, Riordon D, Parks JH, Coe FL. Relationship between supersaturation and crystal inhibition in hypercalciuric rats. Kidney Int. 1997;51:640–645. doi: 10.1038/ki.1997.93. [DOI] [PubMed] [Google Scholar]
- 42.Bushinsky DA, Parker WR, Asplin JR. Calcium phosphate supersaturation regulates stone formation in genetic hypercalciuric stone-forming rats. Kidney Int. 2000;57:550–560. doi: 10.1046/j.1523-1755.2000.00875.x. [DOI] [PubMed] [Google Scholar]
- 43.Evan AP, Lingeman JE, Coe FL, Parks JH, Bledsoe SB, Shao Y, Sommer AJ, Paterson RF, Kuo RL, Grynpas M. Randall’s plaque of patients with nephrolithiasis begins in basement membranes of thin loops of Henle. The Journal of clinical investigation. 2003;111:607–616. doi: 10.1172/JCI17038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Bushinsky DA. Nephrolithiasis: site of the initial solid phase. The Journal of clinical investigation. 2003;111:602–605. doi: 10.1172/JCI18016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bushinsky DA, Asplin JR, Grynpas MD, Evan AP, Parker WR, Alexander KM, Coe FL. Calcium oxalate stone formation in genetic hypercalciuric stone-forming rats. Kidney Int. 2002;61:975–987. doi: 10.1046/j.1523-1755.2002.00190.x. [DOI] [PubMed] [Google Scholar]
- 46.Grynpas M, Waldman S, Holmyard D, Bushinsky DA. Genetic hypercalciuric stone-forming rats have a primary decrease in bone mineral density and strength. Journal of Bone and Mineral Research. 2009;24:1420–1426. doi: 10.1359/JBMR.090223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Friedman PA, Bushinsky DA. Diuretic effects on calcium metabolism. Seminars in Nephrology. 1999;19:551–556. [PubMed] [Google Scholar]
- 48.Coe FL, Parks JH, Bushinsky DA, Langman CB, Favus MJ. Chlorthalidone promotes mineral retention in patients with idiopathic hypercalciuria. Kidney International. 1988;33:1140–1146. doi: 10.1038/ki.1988.122. [DOI] [PubMed] [Google Scholar]
- 49.Bushinsky DA, Asplin JR. Thiazides reduce brushite, but not calcium oxalate, supersaturation and stone formation in genetic hypercalciuric stone-forming rats. Journal of the American Society of Nephrology. 2005;16:417–424. doi: 10.1681/ASN.2004070543. [DOI] [PubMed] [Google Scholar]
- 50.Breslau NA, Moses AM, Weiner IM. The role of volume contraction in the hypocalciuric action of chlorothiazide. Kid Int. 1976;10:164–170. doi: 10.1038/ki.1976.91. [DOI] [PubMed] [Google Scholar]
- 51.Pearle MS, Roehrborn CG, Pak CYC. Meta-analysis of randomized trials for medical prevention of calcium oxalate nephrolithiasis. Journal of Endurology. 1999;13:679–685. doi: 10.1089/end.1999.13.679. [DOI] [PubMed] [Google Scholar]
- 52.Ernst ME, Carter BL, Zheng S, Grimm RH. Meta-analysis of dose-response characteristics of hydrochlorothiazide and chlorthalidone: effects on systolic blood pressure and potassium. Am J Hypertens. 2010;23:440–446. doi: 10.1038/ajh.2010.1. [DOI] [PubMed] [Google Scholar]
- 53.Renjmark L, Vestergaard P, Mosekilde L. Reduced fracture risk in users of thiazide diuretics. Calc Tiss Int. 2005;76:167–175. doi: 10.1007/s00223-004-0084-2. [DOI] [PubMed] [Google Scholar]
- 54.Feskanisch D, Willett WC, Stampfer Jm, Golditz GA. A prospective study of thiazide use and fractures in women. Osteoporos Int. 1997;7:79–84. doi: 10.1007/BF01623465. [DOI] [PubMed] [Google Scholar]
- 55.Sigurdsson G, Franzson L. Increased bone mineral density in a population-based group of 70-year-old women on thiazide diuretics, independent of parathyroid hormone levels. J Int Med. 2001;250:51–56. doi: 10.1046/j.1365-2796.2001.00850.x. [DOI] [PubMed] [Google Scholar]
- 56.Vescini F, Buffa A, La Manna G, Ciavatti A, Rizzoli E, Bottura A, Stefoni S, Caudarella R. Long-term potassium citrate therapy and bone mineral density in idiopathic calcium stone formers. Journal of endocrinological investigation. 2005;28:218–222. doi: 10.1007/BF03345376. [DOI] [PubMed] [Google Scholar]
- 57.Bushinsky DA, Willett T, Asplin JR, Culbertson C, Che SPY, Grynpas M. Chlorthalidone improves vertebral bone quality in genetic hypercalciuric stone-forming rats. Journal of Bone and Mineral Research. 2011 doi: 10.1002/jbmr.374. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Bushinsky DA, Favus MJ, Coe FL. Mechanism of chronic hypocalciuria with chlorthalidone: reduced calcium absorption. Am J Physiol(Renal Fluid Electrolyte Physiol.l6) 1984;247:F746–F752. doi: 10.1152/ajprenal.1984.247.5.F746. [DOI] [PubMed] [Google Scholar]
- 59.Hall TJ, Schaueblin M. Hydrochlorothiazide inhibits osteoclastic bone resorption in vitro. Calcified tissue international. 1994;55:266–268. doi: 10.1007/BF00310404. [DOI] [PubMed] [Google Scholar]
- 60.Lalande A, Roux S, Denne MA, Stanley ER, Schiavi P, Guez D, De Vernejoul MC. Indapamide, a thiazide-like diuretic, decreases bone resorption in vitro. Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research. 2001;16:361–370. doi: 10.1359/jbmr.2001.16.2.361. [DOI] [PubMed] [Google Scholar]
- 61.Barry EL, Gesek FA, Kaplan MR, Hebert SC, Friedman PA. Expression of the sodium-chloride cotransporter in osteoblast-like cells: effect of thiazide diuretics. The American journal of physiology. 1997;272:C109–116. doi: 10.1152/ajpcell.1997.272.1.C109. [DOI] [PubMed] [Google Scholar]
- 62.Aubin R, Menard P, Lajeunesse D. Selective effect of thiazides on the human osteoblast-like cell line MG-63. Kidney international. 1996;50:1476–1482. doi: 10.1038/ki.1996.461. [DOI] [PubMed] [Google Scholar]
- 63.Lajeunesse D, Delalandre A, Guggino SE. Thiazide diuretics affect osteocalcin production in human osteoblasts at the transcription level without affecting vitamin D3 receptors. Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research. 2000;15:894–901. doi: 10.1359/jbmr.2000.15.5.894. [DOI] [PubMed] [Google Scholar]
- 64.Dvorak MM, De Joussineau C, Carter DH, Pisitkun T, Knepper MA, Gamba G, Kemp PJ, Riccardi D. Thiazide diuretics directly induce osteoblast differentiation and mineralized nodule formation by interacting with a sodium chloride co-transporter in bone. Journal of the American Society of Nephrology: JASN. 2007;18:2509–2516. doi: 10.1681/ASN.2007030348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Stamatelou KK, Francis ME, Jones CA, Nyberg LM, Curhan GC. Time trends in reported prevalence of kidney stones in the United States: 1976–1994. Kidney international. 2003;63:1817–1823. doi: 10.1046/j.1523-1755.2003.00917.x. [DOI] [PubMed] [Google Scholar]
- 66.Sakhaee K, Maalouf NM, Sinnott B. Clinical review. Kidney stones 2012: pathogenesis, diagnosis, and management. J Clin Endocrinol Metab. 2012;97:1847–1860. doi: 10.1210/jc.2011-3492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Sakhaee K, Maalouf NM, Kumar R, Pasch A, Moe OW. Nephrolithiasis-associated bone disease: pathogenesis and treatment options. Kidney Int. 2011;79:393–403. doi: 10.1038/ki.2010.473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Trombetti A, Herrmann F, Hoffmeyer P, Schurch MA, Bonjour JP, Rizzoli R. Survival and potential years of life lost after hip fracture in men and age-matched women. Osteoporosis International. 2002;13:731–737. doi: 10.1007/s001980200100. [DOI] [PubMed] [Google Scholar]
- 69.Asplin JR, Donahue SE, Lindeman C, Michalenka A, Strutz KL, Bushinsky DA. Thiosulfate reduces calcium phosphate nephrolithiasis. Journal of the American Society of Nephrology. 2009;20:1246–1253. doi: 10.1681/ASN.2008070754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Hoopes RR, Reid R, Sen S, Szpirer C, Dixon P, Pannet A, Thakker RV, Bushinsky DA, Scheinman SJ. Quantitative trait loci for hypercalciuria in a rat model of kidney stone disease. Journal of the American Society of Nephrology. 2003;14:1844–1850. doi: 10.1097/01.asn.0000073920.43848.a3. [DOI] [PubMed] [Google Scholar]
- 71.Bushinsky DA, Kim M, Sessler NE, Nakagawa Y, Coe FL. Increased urinary saturation and kidney calcium content in genetic hypercalciuric rats. Kidney Int. 1994;45:58–65. doi: 10.1038/ki.1994.7. [DOI] [PubMed] [Google Scholar]
- 72.Bushinsky DA, LaPlante K, Asplin JR. Effect of cinacalcet on urine calcium excretion and supersaturation in genetic hypercalciuric stone-forming rats. Kidney Int. 2006;69:1586–1592. doi: 10.1038/sj.ki.5000324. [DOI] [PubMed] [Google Scholar]
- 73.Coe FL, Favus MJ, Asplin JR. Nephrolithiasis. In: Brenner BM, Rector FC Jr, editors. The Kidney. W.B. Saunders Company; Philadelphia: 2004. pp. 1819–1866. [Google Scholar]
- 74.Yao J, Kathpalia P, Bushinsky DA, Favus MJ. Hyperresponsiveness of vitamin D receptor gene expression to 1,25-dihydroxyvitamin D3: A new characteristic of genetic hypercalciuric stone-forming rats. J Clin Invest. 1998;101:2223–2232. doi: 10.1172/JCI1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Pak CYC, Kaplan R, Bone H. A simple test for the diagnosis of absorptive, resorptive and renal hypercalciurias. N Eng J Med. 1975;292:497. doi: 10.1056/NEJM197503062921002. [DOI] [PubMed] [Google Scholar]
- 76.Pak CYC, Britton F, Peterson R, Ward D, Northcutt C, Breslau NA, McGuire J, Sakhaee K, Bush S, Nicar M, Norman D, Peters P. Ambulatory evaluation of nephrolithiasis: classification, clinical presentation and diagnostic criteria. Am J Med. 1980;69:19–30. doi: 10.1016/0002-9343(80)90495-7. [DOI] [PubMed] [Google Scholar]
- 77.Bataille P, Achard JM, Fournier A, Boudailliez B, Westell PF, Esper NE, Bergot C, Jans I, Lalau JD, Petit J, Henon G, Jeantet MAL, Bouillon R, Sebert JL. Diet, vitamin D and vertebral mineral density in hypercalciuric calcium stone formers. Kidney International. 1991;39:1193–1205. doi: 10.1038/ki.1991.151. [DOI] [PubMed] [Google Scholar]
- 78.Shen FH, Baylink DJ, Nielsen RL, Sherrard DJ, Ivey JL, Haussler MR. Increased serum 1,25-dihydroxyvitamin D in idiopathic hypercalciuria. J Lab Clin Med. 1977;90:955–962. [PubMed] [Google Scholar]
- 79.Coe FL, Canterbury JM, Firpo JJ, Reiss E. Evidence for secondary hyperparathyroidism in idiopathic hypercalciuria. J Clin Invest. 1973;52:134–142. doi: 10.1172/JCI107156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Burckhardt P, Jaeger P. Secondary hyperparathyroidism in idiopathic renal hypercalciuria: fact or theory? J Clin Endocrinol Metab. 1981;55:550. doi: 10.1210/jcem-53-3-550. [DOI] [PubMed] [Google Scholar]
- 81.Kaplan RA, Haussler MR, Deftos LJ, Bone H, Pak CYC. The role of 1,25 dihydroxyvitamin D in the mediation of intestinal hyperabsorption of calcium in primary hyperparathyroidism and absorptive hypercalciuria. J Clin Invest. 1977;59:756–760. doi: 10.1172/JCI108696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Insogna KL, Broadus AE, Dryer BE, Ellison AF, Gertner JM. Elevated production rate of 1,25-dihydroxyvitamin D in patients with absorptive hypercalciuria. J Clin Endocrinol Metab. 1985;61:490–495. doi: 10.1210/jcem-61-3-490. [DOI] [PubMed] [Google Scholar]
- 83.Zerwekh JE, Reed BY, Heller HJ, Gonzalez GB, Haussler MR, Pak CY. Normal vitamin D receptor concentration and responsiveness to 1,25-dihydroxyvitamin D3 in skin fibroblasts from patients with absorptive hypercalciuria. Miner Electrolyte Metab. 1998;24:307–313. doi: 10.1159/000057388. [DOI] [PubMed] [Google Scholar]
- 84.Rendina D, Mossetti G, Viceconti R, Sorrentino M, Castaldo R, Manno G, Guadagno V, Strazzullo P, Nunziata V. Association between vitamin D receptor gene polymorphisms and fasting idiopathic hypercalciuria in recurrent stone-forming patients. Urology. 2004;64:833–838. doi: 10.1016/j.urology.2004.05.013. [DOI] [PubMed] [Google Scholar]
- 85.Bid HK, Kumar A, Kapoor R, Mittal RD. Association of vitamin D receptor gene (Fokl) polymorphism with calcium oxalate nephrolithiasis. J Endourol. 2005;19:111–115. doi: 10.1089/end.2005.19.111. [DOI] [PubMed] [Google Scholar]
- 86.Chen WC, Chen HY, Lu HF, Hsu CD, Tsai FJ. Association of the vitamin D receptor gene start codon Fok I polymorphism with calcium oxalate stone disease. BJU International. 2001;87:168–171. doi: 10.1046/j.1464-410x.2001.02074.x. [DOI] [PubMed] [Google Scholar]
- 87.Valdivielso JM, Fernandez E. Vitamin D receptor polymorphisms and diseases. Clin Chim Acta. 2006;371:1–12. doi: 10.1016/j.cca.2006.02.016. [DOI] [PubMed] [Google Scholar]
- 88.Jackman SV, Kibel AS, Ovuworie CA, Moore RG, Kavoussi LR, Jarrett TW. Familial calcium stone disease: Taql polymorphism and the vitamin D receptor. J Endourol. 1999;13:313–316. doi: 10.1089/end.1999.13.313. [DOI] [PubMed] [Google Scholar]
- 89.Favus MJ. Hypercalciuria: Lessons from studies of genetic hypercalciuric rats. Journal of the American Society of Nephrology. 1994;5:S54–S58. doi: 10.1681/ASN.V55s54. [DOI] [PubMed] [Google Scholar]
- 90.Gambaro G, Vezzoli G, Casari G, Rampoldi L, D’Angelo A, Borghi L. Genetics of hypercalciuria and calcium nephrolithiasis: from the rare monogenic to the common polygenic forms. Am J Kid Dis. 2004;44:963–986. doi: 10.1053/j.ajkd.2004.06.030. [DOI] [PubMed] [Google Scholar]
- 91.Chattopadhyay N, Brown EM. Role of calcium-sensing receptor in mineral ion metabolism and inherited disorders of calcium-sensing. Molecular Genetics and Metabolism. 2006;89:189–202. doi: 10.1016/j.ymgme.2006.07.003. [DOI] [PubMed] [Google Scholar]
- 92.Vezzoli G, Tanini A, Ferrucci L, Soldati L, Bianchin C, Franceschelli F, Malentacchi C, Porfirio B, Adamo D, Terranegra A, Falchetti A, Cusi D, Bianchi G, Brandi ML. Influence of calcium-sensing receptor gene on urinary calcium excretion in stone-forming patients. J Am Soc Neph. 2002;13:2517–2523. doi: 10.1097/01.asn.0000030077.72157.d2. [DOI] [PubMed] [Google Scholar]
- 93.Scillitani A, Guarnieri V, De Geronimo S, Muscarella LA, Battista C, D’Agruma L, Bertoldo F, Florio C, Minisola S, Hendy GN, Cole DEC. Blood ionized calcium is associated with clustered polymorphisms in the carboxyl-terminal tail of the calcium-sensing receptor. Journal of Clinical Endocrinology Metabolism. 2004;89:5634–5638. doi: 10.1210/jc.2004-0129. [DOI] [PubMed] [Google Scholar]
- 94.Parks JH, Coe FL. Pathogenesis and treatment of calcium stones. Seminars in Nephrology. 1996;16:398–411. [PubMed] [Google Scholar]