

Abstract
Objective
To understand the effect of current and future long-term care (LTC) policies on family eldercare hours for older adults (60 years of age and older) in Singapore.
Data Sources
The Social Isolation Health and Lifestyles Survey, the Survey on Informal Caregiving, and the Singapore Government's Ministry of Health and Department of Statistics.
Study Design
An LTC Model was created using system dynamics methodology and parameterized using available reports and data as well as informal consultation with LTC experts.
Principal Findings
In the absence of policy change, among the elderly living at home with limitations in their activities of daily living (ADLs), the proportion of those with greater ADL limitations will increase. In addition, by 2030, average family eldercare hours per week are projected to increase by 41 percent from 29 to 41 hours. All policy levers considered would moderate or significantly reduce family eldercare hours.
Conclusion
System dynamics modeling was useful in providing policy makers with an overview of the levers available to them and in demonstrating the interdependence of policies and system components.
Keywords: Aging/elderly/geriatrics, disability, health policy/politics/law/regulation, long-term care: home care/nursing homes, geriatrics, medical decision making, modeling: multilevel
Driven by age dynamics, fertility rate declines, and increases in longevity, the share of the global population 60 years of age and older is expected to double from about 11 to 22 percent by 2050 (World Health Organization 2012). A potential consequence of this demographic shift is an increase in the prevalence of health conditions, such as chronic disease and disability, including underlying physical, cognitive, and sensory limitations. As the number of elderly individuals living with health conditions rises, the impact of caregiving, herein measured as eldercare hours, for their informal family caregivers is likely to increase. Evidence suggests that excess caregiver burden is associated with depression (Covinsky et al. 2003; van Wijingaarden, Schene, and Koeter 2004; Malhotra et al. 2012), reduced labor force participation (Heitmueller and Inglis 2007; Arksey and Glendinning 2008; Bolin, Lindgren, and Lundborg 2008), and increased health care utilization (Schulz and Beach 1999) among caregivers. These potential negative outcomes of caregiving demonstrate the need for an effective long-term care (LTC) policy.
Similar to other developed countries in Asia, including Japan, South Korea, and Taiwan, the city-state of Singapore is predicted to undergo a significant increase in older adults between now and 2050 (Bloom, Canning, and Fink 2010). This demographic dynamic provides an excellent case study of population aging and the potential impact of LTC policy interventions on eldercare hours. As a result of more effective medical care, improved living standards, and decades of subreplacement level fertility rates, the population of Singapore has transitioned from one with high mortality, high fertility, and a median age of 20 years in 1970 (Teo et al. 2006) to an aging one with low mortality, low fertility, and a median age of 38 (Singapore Department of Statistics 2012). These shifts are expected to raise the old-age dependency ratio from 12 percent in 2007 to 56 percent in 2050 (Ducanes and Abella 2008). Today, one of the central concerns for Singapore is how the country will care for greater numbers of older people with fewer potential caregivers.
Although many older Singaporeans are expected to live healthy, independent lives, some will develop disabilities that require significant contributions of care hours from skilled (e.g., nurses and physical therapists) and unskilled (e.g., family members and foreign domestic workers, similar to personal and home care aides in the United States and Europe) caregivers. A study by Ng et al. (2006) revealed that the prevalence of dependency in at least one activity of daily living (ADL) in Singaporeans aged 60 and older was 10.8 percent. Government efforts to encourage self-care and active aging (Ministry of Community Development, Youth and Sports [MCYS] (2008/2009), and cohort effects related to improved living environment may modulate the need for caregiving but may not substantially reduce the need for people and services to care for dependent elders.
In Singapore, the average household size is 3.5 persons (Singapore Department of Statistics 2010), and about 85 percent of households earn less than $6,000 SGD per month (Ministry of Manpower 2009). To help Singaporeans finance their health care, the government has established four programs: Medisave, Medifund, Medishield, and Eldershield. Medisave is a medical savings account system that covers approximately 85 percent of Singapore's population; it is a subset of the Central Provident Fund, a mandatory government pension scheme to which employees contribute a portion of their wages to fund retirement and their personal health care needs (Metodiev 2007). When an individual or family does not have sufficient Medisave funds to afford care, they may become eligible for Medifund, a means-tested safety net for those in financial hardship. Although Medisave and Medifund are the primary means through which Singaporeans pay for their medical care, Medishield as well as private insurance schemes are available to cover a significant portion of expenses from catastrophic or prolonged illnesses (Chia and Tsui 2005). Similar to Medishield but tailored to the needs of the older population, Eldershield helps fund expenses incurred as a result of severe disability. For Singaporean households earning less than $1,439 SGD per month, 75 percent of LTC costs are subsidized by the government. For those households earning between $1,440 and $3,800 SGD per month, 50 percent of LTC costs are subsidized, and for those earning between $3,801 and $5,600 SGD, 25 percent of LTC costs are subsidized.
In contrast with the United Kingdom and the United States, Singapore has sought to minimize LTC costs by adopting an LTC policy that promotes “the family as the first line of care and support for persons with disabilities” (Teo, Chan, and Straughan 2003; Ministry of Social and Family Development 2007), a position in accord with the widely accepted Confucian tradition of filial piety (Liu 2000). Only in instances when family support is insufficient may qualifying, means-tested elders receive subsidies from the government either to employ a foreign domestic worker (FDW) (equivalent to a live-in maid in the United States and Europe) or pay for the use of home- and community-based services (HCBS) or a nursing home (Teo 1994; Mehta 2004; Teo et al. 2006).
Correspondingly, there are 59 nursing homes and a total of just 9,300 nursing home beds in Singapore, all of which are occupied (Ministry of Health 2007). Of the 59 nursing homes in Singapore, 30 are private and 29 are run by voluntary welfare organizations (VWOs; that is, charities providing welfare services); eight of the private nursing homes and 23 of those run by VWOs receive subsidies from the Ministry of Health (Ministry of Health 2007). Consequently, just 2 percent of the elderly population in Singapore live in a nursing home (Singapore Department of Statistics 2012), and the Singapore Government has proposed only limited increases in the number of nursing home beds (MCYS 1999) despite expectations that demand will increase significantly. Instead, the vast majority of older Singaporeans are expected to age in place, in effect maintaining the proportion of older Singaporeans coresiding with family (Mehta 2005). In contrast with its plans for nursing home capacity, Singapore is promoting the expansion and enhancement of HCBS to better enable older disabled individuals to remain at home.
In Singapore, HCBS consists of a continuum of integrated care for senior citizens, including day rehabilitation centers, day care centers for dementia patients, home medical and nursing care, and home help. Other community support services are also available, such as meal delivery, laundry service, and accompaniment to the clinic or hospital. Although a wide range of services are offered, affordability and accessibility remain critical issues. Families using HCBS report difficulty transporting care recipients to and from community centers, high service cost, and location of facilities as some of the problems encountered with HCBS (Mehta 2005). According to contact with service providers, HCBS is about 50 percent more expensive compared with the cost of hiring an FDW and thus may be a considerably less attractive option for many Singaporeans, especially considering that an FDW is able to help not only with eldercare but also with cleaning, cooking, and other domestic tasks. Indeed, 17 percent of households in Singapore employ an FDW to help with a dependent elder, and 49 percent of those with an ADL-limited elder in need of human assistance employ an FDW (MCYS SIHLS 2009).
Owing to the trends outlined above, developing a viable LTC infrastructure for the disabled elderly is a high priority. As a first step, it is important to understand the dynamics of LTC needs and the potential impact of policy options to address those needs. Projections of future eldercare hours for the disabled elderly in Singapore were not available, as was evidence of the effect of LTC policies on such eldercare hours. In this study, a system dynamics (SD) model was used to simulate the following LTC policy scenarios: no policy changes, an increase the number of nursing home beds, an increase in the proportion of families with an FDW helping to assist in eldercare, and an increase in the attractiveness of HCBS. This exercise is intended to promote informed decision making and provide insight into the scope of potential LTC problems and their solutions. The modeling process led to and was able to inform an ongoing data collection survey seeking to better understand family- and care-recipient preferences for LTC going forward.
Methods
SD modeling is a process of problem identification, causal hypothesis generation, diagramming the proposed causal relationships, translation of qualitative hypotheses into a quantitative simulation, reliability testing, and policy analysis (Forrester 1961; Richardson and Pugh 1981; Meadows and Robinson 1985; Sterman 2000). SD models consist of an interconnecting set of differential and algebraic equations developed from a broad range of relevant empirical data (Homer and Hirsch 2006). The model is refined until it is able to satisfy requirements concerning its realism and clarity, its ability to reproduce historical patterns, and its potential to generate useful insights (Forrester and Senge 1980; Sterman 1984; Barlas 1996).
Compared with other simulation models (e.g., lumped population contagion models, Markov models, and microsimulation models), SD models admit more variables on the basis of logic or expert opinion for which solid statistical estimates may not be available (Homer and Hirsch 2006). SD modelers find that a broad boundary that includes a variety of realistic causal factors, policy levers, and feedback loops is often what is needed for finding effective solutions to persistent, dynamically complex problems. The SD modeling approach captures complexity by focusing on the causal relationships and dynamic feedback mechanisms between actors and systems of interest. By capturing nonlinear phenomena and taking into account the interdependence of competing sectors, SD models provide a more manageable and comprehensive way to project demand and examine the future impact of policies on a system than do demand estimation models.
SD is a relatively underutilized methodology in the field of health services research; however, the academic literature supports SD models as valuable in assisting policy formation in health care and addressing the dynamic complexity that characterizes many public health issues (Taylor and Lane 1998; Dangerfield 1999; Coyle 2000; Brailsford and Hilton 2001; Homer and Hirsch 2006). SD modeling has been applied to issues of population health since the 1970s (Homer and Hirsch 2006). Luginbuhl et al. (1981) used an SD methodology and model to investigate myocardial infarction prevention and rehabilitation as a means of cost containment. Lane, Monefeldt, and Rosenhead (2000) applied an SD model of the interaction of demand patterns and resource deployment to examine admission delays in an accident and emergency department in the United Kingdom. Roberts et al. (1982) used an SD computer simulation model to study the complex interaction between health policies designed to curb smoking and attempts on behalf of the tobacco industry to counter these restrictions. Levin, Roberts, and Hirsch (1975) used a mathematical SD model to analyze the social, economic, and psychological causes of addiction and critically evaluate an array of collective strategies and the trade-offs among them.
The LTC Model presented in this study was created using SD methodology (Randers 1980; Sterman 2000). First, a conceptual computer model was developed that simulated the reference modes (i.e., the current behavior pattern of key variables). Next, this conceptual model was presented to a total of 10 LTC experts, including nursing home managers, HCBS coordinators, patient placement agency representatives, and health care planners from the Ministry of Health to verify its structure and assumptions regarding causal relationships. Following verification, the model was parameterized using publically available reports and data. When data were unavailable, estimates from LTC experts were used. Finally, the model was simulated, base-case projections were made, potential policy interventions were tested, and the insights gained were shared with LTC experts.
Simulation Model
The LTC Model simulates population aging and living arrangements for elderly living with one or more ADL limitations needing human assistance. The purpose of the model is to project the demand and supply of LTC in Singapore and to understand the effect of current and future policies on family eldercare hours. The model has two submodels that are structurally linked: a population submodel (Figure 1) and a living arrangement submodel (Figure 2). The structure of the model is hierarchical, which permits the validation of its internal structure.
Figure 1.
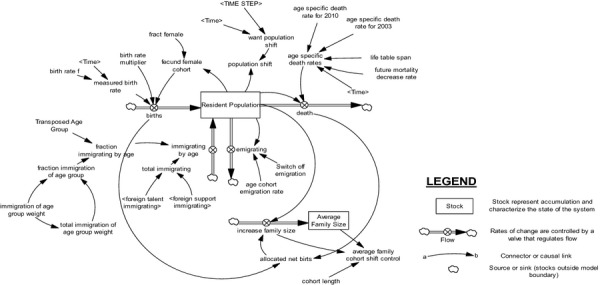
Population Submodel
Figure 2.
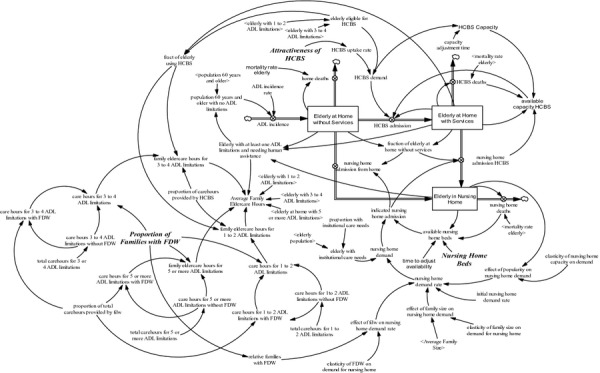
Elderly with Activity of Daily Living Limitations Living Arrangement Submodel
Population Submodel
Based on a published model (Thompson et al. 2012), the population submodel (Figure 1) illustrates an aging chain of the Singaporean population. The model represents the resident population (citizens and permanent residents) and the age distribution of the population disaggregated by 1-year age cohorts. The population aging chain shows births, deaths, immigration, and emigration as the four determinants of population change over time. Births are a function of the current birth rate and the fecund population, whereas deaths are a function of cohort population and the current mortality rate, which is held constant over time. Immigration is the transition from foreign labor to permanent resident status and is determined by a constant fraction of eligible foreigners immigrating. Emigration is defined as the estimated resident population migrating from Singapore to other countries, and the emigration rate is determined through calibration. The aging process is conceptually straightforward: births flow into the first age cohort; the surviving population in each age cohort flows into the subsequent cohort with the exception of the final age cohort; the nonsurviving contingent in each age cohort is removed via an outflow that reflects the mortality for that age cohort. The population submodel was calibrated using publicly available national statistical data from the Singapore Department of Statistics.
Living Arrangement Submodel
The living arrangement submodel (Figure 2) estimates the size and likely living arrangement (i.e., nursing home, at home with HCBS, and at home without HCBS) of the elderly population 60 years of age and older with at least one ADL limitation needing human assistance. The living arrangement submodel integrates demand and supply of LTC to understand the effect of a demand-supply gap on family caregiver burden as measured by family eldercare hours. In the model, family eldercare hours are hours of eldercare (care for ADLs and instrumental ADLs) directly provided by family member(s), excluding hours provided by an FDW, whereas total eldercare hours include family eldercare hours and hours provided by HCBS and an FDW. The number of eldercare hours a family provides depends on the number of ADL limitations the care recipient has, where the care recipient lives (i.e., either at home with their family or in a nursing home), the presence of an FDW helping with eldercare, and HCBS utilization.
The number of ADL-limited elderly living at home is a function of the incidence of at least one ADL limitation needing human assistance in the population, the admission rates of elders residing at home to HCBS and nursing homes, and the mortality rate. The incidence of having at least one ADL limitation needing human assistance is determined by the estimated annual incidence rate for at least one ADL limitation needing human assistance and the size of the elderly population at risk for developing ADL limitations, defined as the difference between the elderly population and the elderly population with at least one ADL limitation needing human assistance. HCBS and nursing home admissions are determined by availability, which is based on capacity. In the LTC model, it is assumed that available nursing home beds will go to elderly persons with the greatest perceived care needs. The number of elders receiving HCBS is a net accumulation determined by the rate of HCBS admission, the rate of nursing home admission of those already receiving HCBS, and the mortality rate of those receiving HCBS. The number of elderly persons residing in nursing homes is a function of nursing home admissions and the mortality rate of institutionalized elderly.
Nursing home demand is modeled as a function of the elderly persons with institutional care needs in the elderly population aged 60 years and older. The population of elderly persons—an output from the population submodel—is multiplied by the proportion of elderly Singaporeans with institutional care needs (UN Economic and Social Commission for Asia and the Pacific 2002) to obtain the number of elderly persons with institutional care needs. In the model, the initial nursing home demand rate is adjusted by changes in family size, the proportion of families with an FDW, and the number of institutionalized elderly. As average family size decreases, nursing home demand is expected to increase. While increasing the number of families with an FDW is likely to decrease nursing home demand, an increase in the number of elderly residing in nursing homes is anticipated to increase nursing home demand given that it may become more socially acceptable in Singapore for families to institutionalize their elders.
Demand for HCBS is a function of the elderly population with one to four ADL limitations and the HCBS uptake rate. The HCBS uptake rate is a function of the attractiveness of HCBS. HCBS attractiveness is a subjective measure of caregivers' and care recipients' perception of HCBS relative to other LTC options and is based on estimates by LTC experts. These perceptions may be affected by changes in apparent quality, accessibility, or out-of-pocket costs. A direct, causal relationship is assumed between the attractiveness of HCBS and the uptake rate. As the attractiveness of HCBS increases, the relative attractiveness of other care options will decrease, assuming that such options are substitutes for HCBS (e.g., hiring an FDW to assist with eldercare).
The supply of HCBS is modeled as a delayed response to demand for HCBS. As demand for HCBS increases, the supply of HCBS increases with a delay of 1.5 years. Meanwhile, the supply of nursing home beds is modeled as a policy variable in the living arrangements submodel. The decision to add nursing home beds is decided by government policy preferences.
Policy Scenarios
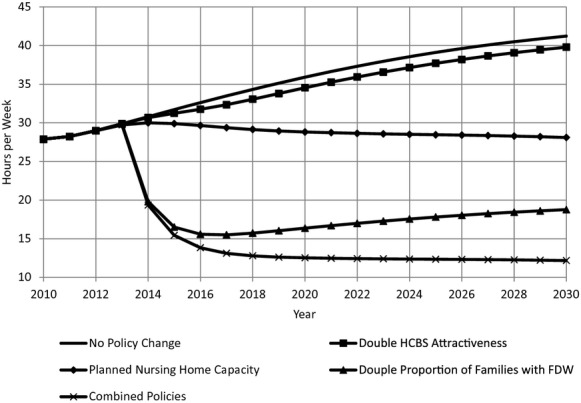
In addition to a base-case scenario in which no new options are developed (no policy change), the following policy scenarios were simulated: (1) an instantaneous increase in the attractiveness of HCBS from 20 to 40 percent (double HCBS attractiveness) in 2013, (2) an increase the number of nursing home beds from 9,300 at present to 14,700 by the year 2020 and to 22,400 by 2030 (planned nursing home capacity) as suggested by the Inter-Ministerial Committee on Health-care for the Elderly (MCYS 1999), (3) an instantaneous increase in the proportion of families with an FDW assisting with eldercare from 49 to 98 percent in 2013 (double proportion of families with FDWs), and (4) a simultaneous implementation of policies 1, 2, and 3 (combined policies).
Data Sources
The Social Isolation, Health and Lifestyles Survey (SIHLS), a nationally representative survey of 5,000 community-dwelling elderly Singaporeans aged 60 years and older, was conducted in 2009 by the MCYS. Details about the survey and its sampling methodology can be found elsewhere (Malhotra et al. 2010). Data from the SIHLS were utilized to assess the prevalence of one or more ADL limitations needing human assistance among resident Singaporeans 60 years of age and older, and the proportion of those with one to two, three to four, and five or more ADL limitations.
The Singapore Survey on Informal Caregiving (SSIC), conducted between 2010 and 2011 by the MCYS, is a national survey of 1,190 community-dwelling care recipients (Singaporeans aged 75 years or older receiving human assistance for at least one ADL limitation), and their primary informal caregiver (a family member or friend but not an FDW) most involved in providing care or ensuring the provision of care to the care recipient. Primary informal caregivers interviewed in the SSIC reported on the number of hours per week they, and/or their family members or FDWs, helped the care recipients with one or more ADL limitations (i.e., bathing, dressing and undressing, eating, toileting, getting in and out of bed, walking and taking care of appearance) or instrumental ADL limitations (i.e., using the telephone, getting to places out of walking distance, shopping, preparing meals, doing housework, taking medication, and handling money). The total reported care hours per week, irrespective of source of care, was then stratified by the number of ADL limitations of the care recipient, ranging from one to seven. Furthermore, the proportion of total reported care hours per week provided by an FDW or by family members (including the caregiver) was determined overall, as well as by number of ADL limitations of the care recipient. The proportion of care recipients receiving eldercare from an FDW was also determined.
Other demographic and population data used in the model were obtained from The Singapore Department of Statistics (http://www.singstat.gov.sg). Nursing home and HCBS capacity data were obtained from other publically available sources (MCYS 1999). For a list of selected model inputs, see Table 1.
Table 1.
Model Inputs
| Parameter | Value | Unit | Source |
|---|---|---|---|
| Average total care hours for elderly with 1 to 2 ADL limitations* | 70 | Hours/week | MCYS SSIC (2010/2011) |
| Average total care hours for elderly with 3 to 4 ADL limitations* | 75 | Hours/week | MCYS SSIC (2010/2011) |
| Average total care hours for elderly with 5 or more ADL limitations* | 98 | Hours/week | MCYS SSIC (2010/2011) |
| Proportion of total eldercare hours provided by an FDW | 0.72 | Dimensionless | MCYS SSIC (2010/2011) |
| Proportion of families with an elderly with ≥1 ADL limitations needing human assistance with an FDW | 0.491 | Dimensionless | MCYS SSIC (2010/2011) |
| Proportion of care hours provided by HCBS | 0.30 | Dimensionless | Estimate by LTC experts |
| Proportion of elderly (60+ years of age) with institutional care needs | 0.03 | Dimensionless | United Nations Social Policy Paper No. 10 |
| ADL incidence rate | 0.00768 | Dimensionless/Year | Model calibration |
| Attractiveness of HCBS | 0.20 | Dimensionless/Year | Estimate by LTC experts |
| Capacity adjustment time | 1.5 | Year | Estimate by LTC experts |
| Proportion of ADL-limited elderly with 1 to 2 ADL limitations* | 0.36 | Dimensionless | MCYS SIHLS (2009) |
| Proportion of ADL-limited elderly with 3 to 4 ADL limitations* | 0.24 | Dimensionless | MCYS SIHLS (2009) |
| Proportion of ADL-limited elderly with 5 or more ADL limitations* | 0.4 | Dimensionless | MCYS SIHLS (2009) |
| Prevalence of ≥1 ADL limitations in population 60+ years of age* | 0.0478 | Dimensionless | MCYS SIHLS (2009) |
| Elasticity of nursing home capacity on demand for nursing home | 0.1 | Dimensionless | Estimate by LTC experts |
| Elasticity of FDW on demand for nursing home | 0.1 | Dimensionless | Estimate by LTC experts |
| Elasticity of family size on demand for nursing home | 0.1 | Dimensionless | Estimate by LTC experts |
| Mortality rate for individuals 60 years of age and older | 0.1134 | Dimensionless/Year | Singapore Department of Statistics (2012) |
| Nursing home beds | Year | Number of beds | |
| 2012 | 9,300 | MOH (2012) | |
| 2020 | 14,900 | MCYS (1999) | |
| 2030 | 22,400 | MCYS (1999) |
Note. *Needing human assistance.
Results
From 2012 to 2030, the number of resident Singaporeans 60 years of age and older with at least one ADL limitation needing human assistance is projected to increase from 27,900 individuals to about 57,300 individuals. Of these 57,300 individuals, approximately 36 percent are expected to have one or two ADL limitation(s), 24 percent are expected to have three or four ADL limitations, and 40 percent are projected to have five or more ADL limitations.
By 2030, with no policy changes, the model projects 48,000 (83 percent) of those elderly with one or more ADL limitations needing human assistance will reside at home. Of these 48,000 individuals, only 12 percent (5,800 individuals) are projected to use HCBS. Among the ADL-limited elderly living at home, the proportion of those with a higher number of ADL limitations will increase. While, by 2030, the proportion with one to four ADL limitation(s) is projected to decrease from 92 to 72 percent, the proportion of elderly individuals with five or more ADL limitations is projected to increase from 8 to 28 percent.
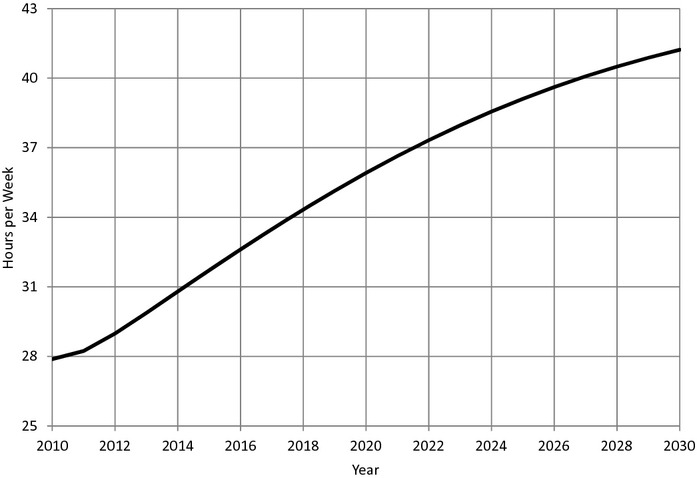
By 2030, in the absence of policy change and as a result of increases in the prevalence of ADL-limited elderly needing human assistance and the proportion of those with a higher number of limitations, average family eldercare hours are projected to increase by 41 percent—from 29 hours per week to 41 hours per week (Figure 3). Because more severely disabled elders require relatively more eldercare hours, the increase in care hours will be disproportionately borne by families with elders with five or more ADL limitations. Between now and 2030, the proportion of families providing at least 60 hours of eldercare per week is projected to increase from 8 to 28 percent, whereas the proportion of families providing less than 60 hours per week is projected to decline from 92 to 72 percent.
Figure 3.
Projected Family Eldercare Hours
Relative to no policy changes, all policy levers would either moderate the increase of or significantly decrease average family eldercare hours (Figure 4). By doubling the attractiveness of HCBS, average family eldercare hours increase from 29 hours per week at present to just 40 hours per week by 2030. Doubling the proportion of families using an FDW to assist in eldercare reduces average family eldercare hours from 29 hours per week at present to 19 hours per week by 2030. By providing the planned increase in nursing home beds, average family eldercare hours are projected to decrease from 29 hours per week at present to 28 hours per week by 2030. By implementing all policies simultaneously, average family eldercare hours decrease from 29 hours per week at present to 12 hours per week by 2030.
Figure 4.
Impact of Policy on Family Eldercare Hours
Discussion
The model presented in this study is the first SD model that integrates population aging and the demand and supply of LTC arrangements to evaluate the effect of current and future policies on family eldercare hours. The study projected that the prevalence of resident Singaporeans 60 years of age and older with at least one ADL limitation needing human assistance will more than double as an increasing number of people grow old and inevitably develop aging-related health problems and limitations. In the absence of change, by 2030, average family eldercare hours are projected to increase by 41 percent while the distribution of disability among the elderly will shift toward those with more severe ADL limitations.
Doubling the proportion of families with an FDW helping with eldercare would have the strongest impact on reducing average family eldercare hours in Singapore. Similar to other Asian countries, this is because FDWs care for elderly with any level of disability and, when present, contribute about 72 percent of total eldercare hours for an ADL-limited elder (MCYS 2009). In the long run, however, issues such as the availability and cost of FDWs may make other LTC policy options more viable. Increasing the number of nursing home beds is the next strongest policy lever. By providing more nursing home beds, the number of community-dwelling elderly with five or more ADL limitations is projected to decrease. Consequently, and assuming families of an institutionalized elder provide no care hours, the number of family caregivers is reduced, which leads to a decrease in average family eldercare hours by 2030. Although doubling the attractiveness of HCBS reduces average family eldercare hours compared with no policy changes, this policy has the least impact because the proportion of elderly with one to four ADL limitations (i.e., the group that qualifies for HCBS) is decreasing and HCBS reduces family eldercare hours by a smaller proportion compared with other LTC policy options.
One limitation of this study is that, because the model is an aggregate model that seeks to analyze the impact of various policies, the use of mean values to represent the population may under or overestimate certain values or increase the uncertainty surrounding the projected outcomes. In addition, the outcome values rely largely on the projected population trend in Singapore. Any change observed in the population trend is likely to change the numerical values observed from the simulation. A final limitation includes the possibility that some ADL-limited elderly needing human assistance may have dementia, which could have affected the total number of eldercare hours reported in the SSIC. This may have led to a slight overestimation in the number of eldercare hours that ADL-limited elderly needing human assistance actually require.
Conclusion
SD modeling was useful in demonstrating the interdependence of the policies and system components and in providing policy makers with an overview of the levers available to them. The LTC Model also provided numerical estimates of future ADL-limited elderly in need of LTC and to quantify the impact of policy interventions on family caregivers. At the same time, this model was designed to be sufficiently generic so that it could be applied to other countries that are facing similar eldercare challenges as a result of population aging.
This work provides the foundation for ongoing and future investigation into the cost and workforce needs associated with the policy levers discussed herein. The analysis reinforces the need for additional data, such as the factors that influence the uptake of services. Indeed, the model led to and informed such a data collection effort on behalf of the Agency for Integrated Care, a quasi-governmental entity that plans and facilitates LTC placement in Singapore.
This work has several limitations. The LTC Model does not reveal how service uptake occurs or assess the adequacy of care hours provided to disabled elderly. In addition, the LTC Model is unable to be used to learn about individual care needs because it is highly aggregated and was designed to be used for policy making. The model also does not provide information on the cost of LTC policies nor their labor requirements—subjects of ongoing research.
The LTC Model shows that there is likely to be a demand-supply gap in the provision of institutional care. Whether this gap is to be filled by the private sector alone or would benefit from public involvement is an issue that policy makers should consider in planning long-term care in Singapore. If more private LTC providers enter the market, more nursing home beds will be available for families who can afford such services. Consequently, this would reduce family eldercare hours, providing some social benefit. Meanwhile, greater privatization of LTC services in Singapore may increase competition and reduce service costs, and if more private LTC providers enter the market, the involvement of government in the provision of LTC services may decline.
Acknowledgments
Joint Acknowledgment and Disclosure Statement: This research is supported by the Singapore Ministry of Health's National Medical Research Council under its STaR Award Grant as part of the project “Establishing a Practical and Theoretical Foundation for Comprehensive and Integrated Community, Policy and Academic Efforts to Improve Dementia Care in Singapore.” The authors have no conflict of interest.
Disclosures: None.
Disclaimers: None.
SUPPORTING INFORMATION
Additional supporting information may be found in the online version of this article:
Appendix SA1: Author Matrix.
References
- Arksey H, Glendinning C. “Combining Work and Care: Carers' Decision-making in the Context of Competing Policy Pressures”. Social Policy and Administration. 2008;42:1–18. [Google Scholar]
- Barlas Y. “Formal Aspects of Model Validity and Validation in System Dynamics”. System Dynamics Review. 1996;12:183–210. [Google Scholar]
- Bloom DE, Canning D, Fink G. “Population Aging and Economic Growth”. In: Spence M, Leipziger D, editors. Globalization and Growth: Implications in a Post Crisis World. Washington, DC: Commision on Growth and Development; 2010. pp. 297–328. [Google Scholar]
- Bolin K, Lindgren B, Lundborg P. “Your Next of Kin or Your Own Career? Caring and Working among the 50+ of Europe”. Journal of Health Economics. 2008;27:718–38. doi: 10.1016/j.jhealeco.2007.10.004. [DOI] [PubMed] [Google Scholar]
- Brailsford S, Hilton N. 2001. “A Comparison of Discrete Event Simulation and System Dynamics for Modeling Health Care Systems” [accessed December 20, 2012]. Available at http://eprints.soton.ac.uk/35689/1/glasgow_paper.pdf.
- Chia NC, Tsui AKC. “Medical Savings Accounts in Singapore: How Much is Adequate?”. Journal of Health Economics. 2005;24(5):855–75. doi: 10.1016/j.jhealeco.2005.01.005. [DOI] [PubMed] [Google Scholar]
- Covinsky KE, Newcomer R, Fox P, Wood J, Sands L, Dane K, Yaffe K. “Patient and Caregiver Characteristics Associated with Depression in Caregivers of Patients with Dementia”. Journal of General Internal Medicine. 2003;18(2):1006–14. doi: 10.1111/j.1525-1497.2003.30103.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coyle G. “Qualitative and Quantitative Modelling in System Dynamics: Some Research Questions”. Systems Dynamics Review. 2000;16(3):225–44. [Google Scholar]
- Dangerfield BC. “System Dynamics Applications to European Health Care Issues”. Journal of the Operational Research Society. 1999;50(4):345–53. [Google Scholar]
- Ducanes G, Abella M. Labour Shortage Responses in Japan, Korea, Singapore, Hong Kong, and Malaysia: A Review and Evaluation. Bangkok: International Labour Organization Regional Office for Asia and the Pacific; 2008. [Google Scholar]
- Forrester JW. Industrial Dynamics. Cambridge, MA: Productivity Press; 1961. [Google Scholar]
- Forrester JW, Senge P. “Test for Building Confidence in System Dynamics Models”. TIMS Studies in the Management Sciences. 1980;14:209–28. [Google Scholar]
- Heitmueller A, Inglis K. “The Earnings of Informal Carers: Wage Differentials and Opportunity Costs”. Journal of Health Economics. 2007;26:821–41. doi: 10.1016/j.jhealeco.2006.12.009. [DOI] [PubMed] [Google Scholar]
- Homer JB, Hirsch GB. “System Dynamics Modeling for Public Health: Background and Opportunities”. American Journal of Public Health. 2006;96(3):452–8. doi: 10.2105/AJPH.2005.062059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lane DC, Monefeldt C, Rosenhead JV. “Looking in the Wrong Place for Healthcare Improvements: A System Dynamics Study of an Accident and Emergency Department”. Journal of Operational Research Society. 2000;51(5):518–31. [Google Scholar]
- Levin G, Roberts EB, Hirsch GB. Persistent Poppy: A Computer-Aided Search for Heroin Policy. Cambridge, MA: Ballinger Publishing Company; 1975. [Google Scholar]
- Liu WT. “Values and Caregiving: The Significance of Filial Piety in Elder Care”. In: Liu WT, Kendig H, editors. Who Should Care for the Elderly? An East-West Value Divide. Singapore: Singapore University Press; 2000. pp. 183–99. [Google Scholar]
- Luginbuhl WH, Forsyth BR, Hirsch GB, Goodman MR. “Prevention and Rehabilitation as a Means of Cost Containment: The Example of Myocardial Infarction”. Journal of Public Health Policy. 1981;2(2):103–15. [PubMed] [Google Scholar]
- Malhotra R, Chan A, Malhotra C, Østbye T. “Prevalence, Awareness, Treatment and Control of Hypertension in the Elderly Population of Singapore”. Hypertension Research. 2010;33(12):1223–31. doi: 10.1038/hr.2010.177. [DOI] [PubMed] [Google Scholar]
- Malhotra C, Malhotra R, Østbye T, Matchar D, Chan A. “Depressive Symptoms among Informal Caregivers of Older Adults: Insights from the Singapore Survey on Informal Caregiving”. International Psychogeriatrics. 2012;24(8):1335–46. doi: 10.1017/S1041610212000324. (In Press) [DOI] [PubMed] [Google Scholar]
- Meadows DL, Robinson J. The Electronic Oracle: Computer Models and Social Decisions. Chichester, England: John Wiley and Sons; 1985. [Google Scholar]
- Mehta KK. “Social Work and Social Development”. In: Mehta KK, Wee A, editors. Social Work in Context: A Reader. Singapore: Marshall Cavendish Academic; 2004. [Google Scholar]
- Mehta KK. “Stress among Family Caregivers of Older Persons in Singapore”. Journal of Cross- Cultural Gerontology. 2005;20:319–34. doi: 10.1007/s10823-006-9009-z. [DOI] [PubMed] [Google Scholar]
- Metodiev MV. “Health Care System in Singapore”. Economic Policy Review. 2007;54:8. [Google Scholar]
- Ministry of Community Development, Youth and Sports. 1999. “Report of the Inter-Ministerial Committee on Health-Care for Elderly” [accessed December 20, 2011]. Available at http://www.sma.org.sg/sma_news/3105/news/3105n1.html.
- Ministry of Community Development, Youth and Sports (MCYS) 2008. /2009. “State of the Elderly in Singapore” [accessed December 20, 2012] Available at http://app1.mcys.gov.sg/Portals/0/Summary/research/State%20of%20the%20Elderly_Release%203.pdf.
- Ministry of Health. 2007. “Bed Statistics in Nursing Homes” [accessed December 20, 2012]. Available at http://www.aic.sg/uploadedFiles/Silver_Pages/About_Long-Term_Care/Understanding/Care_Services_Available/Nursing_Homes/MOH%20Supplement%20%20on%20Bed%20Statistics%20in%20Nursing%20Homes%20.pdf.
- Ministry of Health. 2012. “More Facilities to Help Seniors Age-in-Place” [accessed 20 December 2012] Available at: http://www.moh.gov.sg/content/moh_web/home/pressRoom/pressRoomItemRelease/2012/more-facilities-to-help-seniors-age-in-Place.html.
- Ministry of Manpower. 2009. “Report on Labour Force in Singapore” [accessed December 20, 2012]. Available at http://www.mom.gov.sg/Documents/statistics-publications/manpower-supply/report-labour-2009/mrsd_2009LabourForce.pdf.
- Ministry of Social and Family Development. 2007. “Enabling Masterplan” [accessed December 20, 2012]. Available at: http://app.msf.gov.sg/ResearchRoom/ResearchStatistics/EnablingMasterplan.aspx.
- Ng TP, Niti M, Chiam PK, Kua EH. “Prevalence and Correlates of Functional Disability in Multiethnic Elderly Singaporeans”. Journal of the American Geriatrics Society. 2006;54(1):21–9. doi: 10.1111/j.1532-5415.2005.00533.x. [DOI] [PubMed] [Google Scholar]
- Randers J, editor. Elements of the System Dynamics Method. Cambridge, MA: Productivity Press; 1980. [Google Scholar]
- Richardson GP, Pugh ALI. Introduction to System Dynamics Modelling with Dynamo. Cambridge, MA: Productivity Press; 1981. [Google Scholar]
- Roberts EB, Homer J, Kasabian A, Varrell M. “A Systems View of the Smoking Problem: Perspective and Limitations of the Role of Science in Decision-Making”. International Journal of Bio-Medical Computing. 1982;13(1):69–86. doi: 10.1016/0020-7101(82)90051-4. [DOI] [PubMed] [Google Scholar]
- Schulz R, Beach SR. “Caregiving as a Risk Factor for Mortality”. Journal of the American Medical Association. 1999;282(23):2215–9. doi: 10.1001/jama.282.23.2215. [DOI] [PubMed] [Google Scholar]
- Singapore Department of Statistics. 2010. “Key Indicators of Resident Households” [accessed December 20, 2012]. Available at http://www.singstat.gov.sg/stats/themes/people/hhldindicators.pdf.
- Singapore Department of Statistics. 2012. “Key Annual Indicators” [accessed December 20, 2012]. Available at http://www.singstat.gov.sg/stats/keyind.html.
- Sterman JD. “Appropriate Summary Statistics for Evaluating the Historical Fits of System Dynamics Models”. Dynamica. 1984;10:51–66. [Google Scholar]
- Sterman JD. Business Dynamics: Systems Thinking and Modeling for a Complex World. Boston: McGraw-Hill Higher Education; 2000. [Google Scholar]
- Taylor K, Lane D. “Simulation Applied to Health Services: Opportunities for Applying the System Dynamics Approach”. Journal of Health Services Research and Policy. 1998;3(4):226–32. doi: 10.1177/135581969800300409. [DOI] [PubMed] [Google Scholar]
- Teo P. “The National Policy on Elderly People in Singapore”. Ageing and Society. 1994;14(3):405–27. [Google Scholar]
- Teo P, Chan A, Straughan P. “Providing Health Care for Older Persons in Singapore”. Health Policy. 2003;64(3):399–413. doi: 10.1016/s0168-8510(02)00201-4. [DOI] [PubMed] [Google Scholar]
- Teo PA, Mehta K, Leng LT, Chan A. Ageing in Singapore: Service Needs and the State. New York: Routledge; 2006. [Google Scholar]
- Thompson JP, Riley CM, Eberlein RL, Matchar DB. “Future Living Arrangements of Singpaoreans with Age-related Dementia”. International Journal of Psychogeriatrics. 2012;24(10):1592–9. doi: 10.1017/S1041610212000282. [DOI] [PubMed] [Google Scholar]
- UN Economic and Social Commission for Asia and the Pacific. New York: United Nations; 2002. “Ageing in Asia and the Pacific: Emerging Issues and Successful Practices.” United Nations Social Policy Paper No. 10. [Google Scholar]
- van Wijingaarden B, Schene A, Koeter M. “Family Caregiving in Depression: Impact of Caregivers' Daily Life, Distress, and Help Seeking”. Journal of Affective Disorders. 2004;81(3):211–22. doi: 10.1016/S0165-0327(03)00168-X. [DOI] [PubMed] [Google Scholar]
- World Health Organization. 2012. “World Health Day: Are You Ready? What You Need to Know about Aging” [accessed December 20, 2012]. Available at http://www.who.int/world-health-day/2012/toolkit/background/en/index.html.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.