

Abstract
Objective
A meta-analysis was conducted to test theoretical hypotheses about the predictors of enrollment and completion of condom-use-promotion interventions among men and women.
Design
A meta-analysis summarized research reports of the efficacy of experimental interventions on human immunodeficiency virus (HIV) prevention.
Main Outcome Measures
The outcome measure consisted of (a) a measure of participation, obtained by subtracting the actual number of participants from the number of the invited people, and (b) a measure of retention was obtained by subtracting the number of participants who completed the intervention from the number of commencers.
Results
Experimental interventions providing instrumental and financial resources (e.g., payments) increased initiation and retention more among predominantly male samples, whereas experimental interventions using group formats increased initiation and retention more among predominantly female samples. These patterns remained while controlling for past condom use, other HIV-risk behaviors, and demographics associated with gender composition.
Conclusion
People seek out HIV-prevention interventions to fulfill gender-specific needs, and these differences must be taken into account in the design of HIV-prevention interventions.
Keywords: gender, HIV prevention interventions, participation
Recent U.S. health statistics have revealed that, within a given year, women are more likely to become infected with human immunodeficiency virus (HIV) than are men (Centers for Disease Control and Prevention, 2006). Although the differences are in part attributable to women being more easily infected through vaginal intercourse than men (Hader, Smith, Moore, & Holmberg, 2001; National Institutes of Health, 2007), there may also be disparities in the efficacy and effectiveness of HIV-prevention interventions for men and women (HRSA Care ACTION, 1999). For example, according to a previous meta-analysis, overall change in behavior following HIV-prevention interventions is greater for men than for women (Albarracín et al., 2005). Furthermore, this problem may be compounded by differential enrollment in interventions, which in turn may be related to different determinants of participation across gender groups. After all, a significant number of people at risk for HIV infection never enroll in relevant programs, and others enroll but drop out before completion (Rutledge, Roffman, Picciano, Kalichman, & Berghius, 2002).
The theoretical analysis that guided the present meta-analysis focused on human needs (see, e.g., Maslow, 1943). Although participation and retention in health-prevention interventions may serve the need of reducing risk (e.g., Barragán et al., 2005; Noguchi, Albarracín, Durantini, & Glasman, 2007), instrumental and social needs are also likely to be important. Interventions accompanied by tangible incentives (general health care, money, or social welfare benefits) may satisfy financial or instrumental needs, whereas interventions that are socially supportive to audiences may meet social needs. Importantly, financial and instrumental incentives may attract the more independent- and outcome-oriented men, whereas group (vs. individual) interventions may attract the more community-oriented women.
In the present meta-analysis, intervention participation was studied by analyzing enrollment and attrition in experimental programs. Some studies reported the number of target participants and the number of people who actually enrolled in a study group (e.g., Weinhardt, Carey, Carey, & Verdecias, 1998; Wenger, Linn, Epstein, & Shapiro, 1991). Thus, these reports were used to calculate the odds of accepting to partake in the intervention (and the study). Other studies reported the number of participants who began and finished the study (Rutledge et al., 2002; Sayre et al., 2002; Spicer, 2003; Toft, 1995; Veach, Ramley, Kippers, & Sorg, 2000). These samples sizes were used to calculate the odds of staying in the intervention. Later, the odds of acceptance and retention were studied as a function of the percentage of women in a sample and the characteristics of the intervention associated with instrumental and financial incentives, as well as group formats. Gender could then be analyzed in combination with instrumental/financial incentives and group formats as a test of the impact of these resources across gender groups.
Participation in HIV-Prevention Interventions as a Function of the Audience’s Gender
Despite the widespread importance of estimating attrition in health-promotion interventions, the literature predicting attrition is inconclusive about differences across men and women. A growing amount of research indicates that women are more likely than men to use health services for a range of problems from depression to physical disabilities (Albizu García, Alegría, Freeman, & Vera, 2001; Galdas, Cheater & Marshall, 2005; Hussaini, Moore, & Cain, 1994; Lee, 2002; Leong, & Zachar, 1999; Ross, Essien, Williams, & Fernández, 2003; Stolley, 1997; Thom, 1986; Weissman & Kleiman, 1977). Compared with men, women appear to have greater tolerance for the social stigma associated with seeking psychotherapy than men (Johnson, 1988). Women were also more likely to seek counseling and other services and were more receptive to admitting a need for help and to sharing their concerns with others (Johnson, 1988). In the area of HIV prevention, however, men have been reported to enroll less but complete intervention-research studies more than women. In particular, a meta-analysis by Noguchi et al. (2007) revealed an association of β = 0.36 and − 0.11 (p < .05) between the percentage of women in a sample and acceptance and retention in HIV-prevention studies (i.e., both treatment and control conditions). Although this finding is important, estimating correlations of gender composition with acceptance and completion of interventions, not studies, would provide more precise estimates. The present meta-analysis provided these estimates.
More than estimating the relation between female gender and acceptance or completion of condom-use-promotion interventions, we were interested in examining external incentives to participation across men and women. Specifically, different external factors may serve as incentives to participation by women and men (a resource-differential model). For example, men may be better recruited by financial and instrumental factors, whereas women may be more attracted to interventions that offer social rewards. On this vein, whereas the past literature on gender and attrition has been invaluable in describing the problem (see Brannen & Rubin, 1996; Carrington, 2004; Condelli, Koch, & Fletcher, 2000; Rabinowitz, 2002; Schilling & Sachs, 1993; Schweitzer, 1997), our interest was to test social-psychological hypotheses in this area.
The model we tested states that men and women require specific external incentives. Social psychological research has found different psychological orientations men and women with regard to the dimensions of agency (i.e., focus on the self and autonomy) and communion (i.e., focus on other people and relationships; Bakan, 1966; Carlson, 1971; Hegelson, 1994). Because of a combination of biological and social factors, men are more likely to develop personality traits related to agency (Hegelson, 1994), whereas women are more likely to develop personality traits related to communion. From this perspective, men may be more attracted to participate in interventions with financial/instrumental compensations (see, e.g., Pearson, 2003; Rosener, 1995), whereas women may be more attracted by the social exchange provided by group interventions (Durantini et al., 2006).
Method
Overview
The present meta-analysis included research reports of condom-use-promoting interventions that detailed sample sizes for either or both the target group and the enrolled group, as well as the group of commencers and the group of completers. These data were used to calculate the odds of accepting and staying in an intervention. In turn, these odds were analyzed as a function of instrumental/financial resources and group (vs. individual) formats. Also, these analyses were performed as a function of the gender of the sample to determine the relative weight of these external factors across different gender groups. Supplementary analyses controlled for the associations of these demographics with education, behavioral risk, and intervention features were conducted for all interventions as well as only multiple-session interventions. Adding seven predictors together was not possible because of multicollinearity problems and the number of cases. Hence, these predictors were added one at a time to the other equations in Table 2. These results are available from the authors.
Table 2.
Regressions for the Effects of Gender and External Resources
| All interventions
|
Only multisession interventions
|
|||||
|---|---|---|---|---|---|---|
| Acceptance | Retention | Retentiona | Acceptance | Retention | Retentiona | |
| % Women | 0.58* | −0.19*** | 0.51 | −0.07* | ||
| Instrumental/financial incentives | −0.03 | 0.38*** | −0.04 | 0.26*** | ||
| % Women × instrumental/financial incentives | −0.67* | −0.22*** | −0.50 | −0.43*** | ||
| Past condom use (linear) | 0.15 | −0.16*** | 0.54 | 0.05 | ||
| Past condom use (quadratic) | 0.54* | 0 | 0.11 | −0.09+ | ||
| k | 17 | 78 | 11 | 47 | ||
| QR | 17.67*** | 837.96 | 21.28*** | 605.55*** | ||
| QE | 15.89*** | 979.89 | 1.04 | 553.42*** | ||
| R2 | .53 | .46 | .95 | .52 | ||
| % Women | −1.36*** | −0.50*** | — | −0.28*** | ||
| Group interventiona | 0.52* | −0.26*** | — | −0.49*** | ||
| % Women × group intervention | 1.99*** | 0.48*** | — | 0.30*** | ||
| Past condom use (linear) | −0.08 | 0.05 | — | 0.15** | ||
| Past condom use (quadratic) | 0.31+ | −0.25*** | — | −0.22*** | ||
| k | 16 | 70 | — | 43 | ||
| QR | 30.50*** | 649.16*** | — | 543.19*** | ||
| QE | 3.04* | 843.81*** | — | 518.87*** | ||
| R2 | .91 | .44 | — | .51 | ||
| % Women | −0.40*** | −0.29*** | ||||
| Instrumental/financial incentives | 0.33*** | 0.18* | ||||
| % Women × instrumental/financial incentives | −0.14** | −0.26*** | ||||
| Group interventiona | −0.04 | −0.21*** | ||||
| % Women × group intervention | 0.34*** | 0.28*** | ||||
| Past condom use (linear) | 0.21 | 0.12 | ||||
| Past condom use (quadratic) | −0.30* | −0.14 | ||||
| k | 71 | 43 | ||||
| QR | 756.81*** | 603.17*** | ||||
| QE | 740.56*** | 458.90*** | ||||
| R2 | .51 | .57 | ||||
Note. k = number of conditions in analysis; QR = coefficient of homogeneity for regression; QE = coefficient of homogeneity for error; R2 = squared multiple regression coefficient. Unless otherwise indicated, entries are standardized beta weights. Only treatment samples were used in this analysis. Within each panel, all variables were entered simultaneously.
Factor represented dichotomous choices (1 = yes; 0 = no). This analysis was conducting with all predictors in the equation. The same omnibus regression could not be performed for acceptance because of insufficient number of conditions.
p < .08.
p < .05.
p < .01.
p < .001.
Restrictions in space prevent us from displaying all these results. Importantly, although the analyses reported here are new, the data used in this study were largely overlapping with the data used by Noguchi et al. (2007). Based on Noguchi et al.’s conclusion that past condom use was a significant determinant of participation in condom-use-promoting interventions, the current meta-analysis included studies for which this factor would be controlled. In addition, the present database has been updated to include more recent studies.
Literature Search
As part of a computerized search, we combined the key words condom use, AIDS, STD/STI, and HIV with intervention, behavior, knowledge, education, prevention, intervention, condoms, communication, attitudes, and message. The search comprised the period between 1988 and 2006 (for more details, see Noguchi et al., 2007).
Eligibility Criteria
The following eligibility criteria were used to select target reports from more than 700 articles located through the bibliographic search:
Presence of a condom-use-promotion intervention.
Presence of either or both the number of enrolled participants and targets and the number of commencers and completers of the intervention.
For completion rates, the N of completers had to be reported for the intervention itself or an immediate posttest on the day of the last session.
For completion rates, only within-subjects designs were used.
Presence of baseline behavior measures.
Presence of a description of the gender of the population.
Presence of data on incentives and group/individual format. Partitioning of studies.
For each paper (for a list of references go to http://www.psych.uiuc.edu/~dalbarra), we retrieved each available intervention and control condition. In addition, whenever the report separated different samples, we attempted to treat each independent sample separately. Five papers, however, did not report Ns for each intervention condition in a separate fashion, leading to collapsing the groups of these interventions into a single group. No control group was merged, because this situation only applied to the intervention groups within the five aforementioned reports.
Effects Sizes for Acceptance and Retention
To obtain measures of initial acceptance, we retrieved the number of target participants, and also the number of participants who accepted to take part, and, if any, the number of participants excluded by the experimenter. To measure retention, we recorded the number of commencers and completers of the intervention. When available, these data allowed us to compute the odds of acceptance (invited/commencers and excluded) and retention (completers/commencers) in a sample. Odds of 1 correspond to equal probability of acceptances and declinations or retention and drop out. Odds greater than 1 correspond to more likely acceptance than declination or retention than drop out. Odds smaller than 1 correspond to more likely declination than acceptance or dropout than retention. As mentioned, whenever possible, acceptance and retention rates were calculated for each independent condition. Also, rates for control groups were always calculated separately.
We also recorded the mean number of completed sessions when this information was available. However, the number of sessions (M = 3.71, k = 87) was highly correlated with the estimated retention rates (r = −.37, p < .01). Also, whenever the number of completed sessions was reported, retention was also reported. As a result, only the odds of completion were used in our analyses of retention.
Coding of Moderators
Independent raters coded relevant characteristics of the reports and methods used in the study. After the initial training, the overall intercoder agreement was 95%. Intercoder-reliability coefficients (kappas for categorical variables and simple correlations for continuous variables) were greater than .90 in all cases. Occasional disagreements were resolved by discussion with a third coder and further examination of the studies.
When attrition data were provided for several conditions at the same time (the five reports with more than one collapsed treatment group), the coded moderators were averaged across conditions. In those cases, the descriptors for gender and past condom use were averaged across groups. Also, in these situations, we averaged moderators pertaining to external incentives, as well as group formats. For example, if one condition used attitudinal arguments (i.e., a value of 1) and the other none (i.e., a value of 0), we averaged both with a resulting value of .50 on presence of attitudinal arguments.
Audience’s Demographics
To record the gender composition of each group, we recorded the percentage of women in each sample. Also we recorded mean age, years of education, ethnicity, annual income, and marital status.
Instrumental/Financial Resources
Individual and group formats
Furthermore, we coded for whether incentives were offered to participants. The specific forms were payments, transportation, child care, reminders, HIV test (when it was only offered, but was not a required part of the program), other health care, and other incentives. Each incentive received a 1 (vs. 0 for its absence), and all incentives were averaged as an overall index of instrumental/financial resources. Analyses were replicated with each specific incentive as well as the overall index. Because the patterns were the same regardless of the specific index, we only report the results for the overall index. Finally, we registered whether the interventions were delivered to groups (i.e., a score of 1) or individuals (i.e., a score of 0).
Other descriptors
To further describe the sample demographically, we recorded included risk groups, sexual transmitted infections (STI) and HIV rates, number of sexual partners, and number of pregnant participants.
Regarding the intervention strategies, we recorded presence (i.e., a score of 1) or absence (i.e., a score of 0) of (a) information on HIV; (b) specific information on condom use; (c) threat arguments (e.g., discussions about the recipient’s personal risk of contracting HIV or other STIs); (d) attitudinal arguments (e.g., statements about the positive implications of using condoms for the health of the partners and for the romantic relationship); (e) normative arguments (e.g., asserting support for condom use on the part of friends, family members, or partners); and (f) control arguments. In addition, we registered whether the program entailed active training in (g) condom use behavioral skills (e.g., opening wrapper without tearing it, unrolling condom in proper direction); (h) negotiation skills (e.g., role-playing condom use negotiation); (i) whether HIV counseling and testing was performed; and (j) whether condoms were provided. The impact of these strategies on change has been established elsewhere (see also Albarracín et al., 2005; Durantini et al., 2006) and may correlate with the gender of a sample, the use of incentives, and group delivery formats.
We also coded for other methodological characteristics that are relevant to the setup of the interventions. We recorded (a) the setting of the intervention; (b) the number of sessions and session duration; (c) the percentage of completed sessions; (d) the number of days between the baseline measures and the last session; and (e) the recruitment method. Finally, we recoded (f) the publication year; (g) the country of intervention (i.e., United States vs. other countries); and (h) the city of intervention for studies in the United States.
Analytic Strategy
Average estimates of acceptance and retention were calculated by using Hedges and Olkin’s (1985) procedures. To perform moderator analyses, the continuous moderators of gender and financial/instrumental incentives, as well as an indicator for group formats, were included in weighted regression equations, along with control variables including past condom use (see Noguchi et al., 2007). Interaction terms were used to model differences depending on gender composition of the groups. To decompose interactions, beta weights were obtained for groups that were predominantly male or predominantly female. The error of the beta weights was corrected based on Hedges and Olkin’s (1985) recommendations. Analyses were repeated after controlling for potential confounds of gender, financial/instrumental resources, and group formats. Analyses were also done for all interventions and for multisession interventions. Some supplementary analyses were performed using weighted analyses of variance to examine the effects of various methodological moderators.
Average estimates of effect sizes were performed using fixed-and random-effects procedures. Moderator analyses were also performed with both methods. However, many of the random-effect analyses were non significant even when the patterns and effect sizes were the same as that for fixed-effects analyses. This result is expected given our sample size and does not deter from the value of our results.
Results
Following some descriptive analyses, continuous variables were included in regression analyses and dichotomous variables in analyses of variance (ANOVAs) to analyze moderating effects. Although odd ratios were used throughout, means were back-transformed to proportions for interpretational purposes. A first set of analyses was performed with our full sample of 103 conditions included in 50 reports. However, when considering the effects of the incentives, only intervention groups (k = 83) were analyzed.
Description of Reports
The 76 studies were produced between 1987 and 2005, and yielded 83 experimental conditions and 20 control conditions. Most of the conditions belonged to reports published in journals (k = 70), although some were unpublished theses (k = 6). In average, each report had at least two conditions, such as two interventions or one intervention and one control group. Most the studies were conducted in the United States (68%). The other represented countries were Australia (6%), Thailand (6%), Namibia (6%), Canada (3%); Rwanda (2%), South Africa (2%), Vietnam (2%), Israel (2%), Singapore (2%); Kenya (1%), and Mozambique (1%). The average size of each condition at the beginning of the studies was 197 (SD = 312).
In the overall sample, audiences were predominantly female (mean percent = 64, SD = 40). Forty-seven percent of the samples included a paid fee in exchange for participation. Other frequent incentives were free heath care (19%), a free HIV or STI test (7%), child care (25%), transportation (11%), and other incentives such as food (20%). With respect to delivery formats, around half of the synthesized interventions were delivered to groups.
The average age of our samples was 25 years (SD = 7.5), the average education was 12 years (SD = 1.24), and the average income US$11,400 ((SD = 8,075). The most frequently represented ethnic background was African (M = 48%, SD = 39), followed by European (M = 20%, SD = 27.50), Latin American (M = 12%, SD = 22), Asian (M = 11%, SD = 31), and Native American (M = 0.14%, SD = 0.70). Researchers often targeted teenagers (18%), disadvantaged women (17%), and female sex workers (8%). Other reports were targeted to men who have sex with men (8%), clients of STI clinics (11%), multiple-partner heterosexuals (1%), mentally ill patients (2%), drug users (9%), female partners of intravenous drug users (2%), military personnel (4%), and juvenile delinquents or prisoners (3%). The mean HIV rate was 9% (SD = 48) and, in average, 49% of the participants reported a recent STI infection (SD = 33). An average of two percent of the sample (SD = 6) was pregnant and the mean number of sexual partners was one (SD = 1). In average, participants reported using condoms less than half of the time in the past. A similar proportion declared using condoms “the last time” they had had sex. Only one in four participants reported “always” using condoms, whereas almost a half reported never using condoms. Our overall measure of condom use was 53% past condom use (SD = 29).
Of the articles reporting where the study took place, most of the interventions were conducted in medical settings (50%), followed by schools 16%), community centers (12%), the street (1%), and other places (13%). The average intervention duration was 4 sessions (SD = 4) of 75 minutes each (SD = 69). The average number of days between the baseline measures and the last session was 31. The intervention generally included information on HIV (77%) and condom use (60%), arguments intended to increase perceived HIV threat (43%), arguments to increase control perception (47%), and behavioral-skills training (negotiation skills: 36%, condom use skills: 22%).
Analyses of Representativeness of the Sample of Studies
Many studies in the literature do not describe either exact attrition for the intervention groups or the baseline condom use of the sample. As a result, one could speculate that the selection criteria might generate a nonrepresentative sample of studies. However, our effect sizes did not deviate from normality, suggesting absence of biases (Wang & Bushman, 1999). These data imply that inclusion of more studies would be unlikely to alter the conclusions of this meta-analysis. Other analyses of demographics and change data in this meta-analysis compared with Albarracín et al.’s (2005) one also indicated that the sample of studies was representative of the overall universe of studies (for similar conclusions and a more detailed report of these procedures, see Noguchi et al., 2007).
Average Participation
We first estimated the weighted mean odds of acceptance and retention in our sample of conditions.
Average Odds of Acceptance and Retention
Of the 19 conditions with reported target Ns, a total of 5,137 people were offered participation and 3,601 accepted. Of the total number of units in the meta-analysis (k = 103), 20,341 participants started the intervention, and 15,931 completed it. These Ns resulted in average odds of acceptance of 0.82 (proportion = .45) (fixed effects confidence interval [CI] for odds = 0.76 to 0.87; fixed-effects CI for proportions = .43 to .47). Moreover, the average odds of retention were 2.46 using fixed-effects analyses (proportion = .71; fixed-effects CI for odds = 2.36 to 2.53; fixed-effects CI for proportions = .70 to .72) and 5.10 using fixed-effects analyses (proportion = .84; fixed-effects CI for odds = 4.14 to 6.23; fixed-effects CI for proportions = .81 to .86).
Results in Treatment and Control Groups
Analyses of participation and retention as a function of intervention and control groups indicated differences in retention. Specifically, the odds of acceptance were similar (0.77 vs. 0.82; proportions = .44 vs. .45) for intervention and control conditions, respectively, QB (1) = 0.14, ns. However, the odds of retention were significantly higher in intervention than control conditions (3.97 vs. 2.39; proportions = .80 vs. .71), QB (1) = 41.46, p < .001. Most of these analyses we present hereafter are based on the sample of intervention groups.
Gender, Financial/Instrumental Resources, and Group Formats
We first examined the simple associations of gender, financial/instrumental resources, and group formats with acceptance and retention controlling for past condom use. Based on Noguchi et al.’s (2007) findings, controls for condom use (linear and quadratic) were introduced in the equations. A summary of these analyses appears in Table 1, for all interventions and multisession interventions. To maximize the number of effects, gender, financial/instrumental resources, and an indicator variable for group formats were entered in separate regressions. As shown, female gender had positive associations with acceptance but negative associations with retention. Across the board, financial/instrumental resources had no association with acceptance, but had a positive correlation with retention. Also, group (vs. individual) formats were negatively correlated with retention.
Table 1.
Acceptance and Retention as a Function of Gender and External Resources
| All interventions
|
Only multisession interventions
|
|||
|---|---|---|---|---|
| Acceptance | Retention | Acceptance | Retention | |
| % Women | 0.09 | −0.23** | 0.02 | −0.16*** |
| Past condom use (linear) | 0.47** | −0.02 | 0.94*** | 0.27*** |
| Past condom use (quadratic) | 0.33+ | −0.35*** | −0.02 | −0.52*** |
| Kk | 17 | 80 | 11 | 48 |
| QR | 11.73*** | 406.33*** | 19.81*** | 253.68*** |
| QE | 21.84*** | 1461.23*** | 2.51 | 930.68*** |
| R2 | .35 | .22 | .89 | .21 |
| Instrumental/financial incentives | 0.10 | 0.52*** | −0.10 | 0.54*** |
| Past condom use (linear) | 0.49** | −0.05+ | 0.98*** | 0.16*** |
| Past condom use (quadratic) | 0.37+ | −0.14*** | −0.06 | −0.28*** |
| k | 17 | 78 | 11 | 47 |
| QR | 11.75*** | 720.10*** | 20.09*** | 512.36*** |
| QE | 21.81*** | 1097.75*** | 2.31 | 646.61*** |
| R2 | .35 | .40 | .90 | .44 |
| Group interventiona | 0.12 | −0.16*** | −0.07 | −0.57*** |
| Past condom use (linear) | 0.50*** | −0.36** | 0.92*** | 0.31*** |
| Past condom use (quadratic) | 0.32+ | 0.38* | 0 | −0.34*** |
| k | 16 | 72 | 11 | 43 |
| QR | 11.97*** | 458.32*** | 19.88*** | 513.30*** |
| QE | 21.57*** | 1056.70*** | 2.43 | 548.77*** |
| R2 | .36 | .30 | .89 | .48 |
Note. k = number of conditions in analysis; QR = coefficient of homogeneity for regression; QE = coefficient of homogeneity for error; R2 = squared multiple regression coefficient. Unless otherwise indicated, entries are standardized beta weights. Only treatment samples were used in this analysis. All variables in each panel were entered simultaneously.
Factor represented dichotomous choices (1 = yes; 0 = no).
p < .08.
p < .05.
p < .01.
p < .001.
Moderators of Participation as a Function of Gender External Resources
We then examined the key hypothesis in this study: whether the influence of external resources differs as a function of gender and the nature of the differences if any are found. For this purpose, we analyzed the log odds for either acceptance or retention as a function of (a) percentage of women in a sample, (b) external resources (either financial/instrumental resources or group formats), and (c) the interaction between the two included variables. Regression analyses were weighted by the inverse of variance of the log odds and controlled for past condom use (linear and quadratic trends). Table 2 presents a summary of these weighted regression analyses, which replicated after including potential confounds and when all three equations were entered simultaneously. However, Table 2 presents the results from separate regressions for instrumental/financial resources and group formats because these results maximize power. To interpret the interactions, Figure 1 presents correlations across groups with more and less than 50% women.
Figure 1.
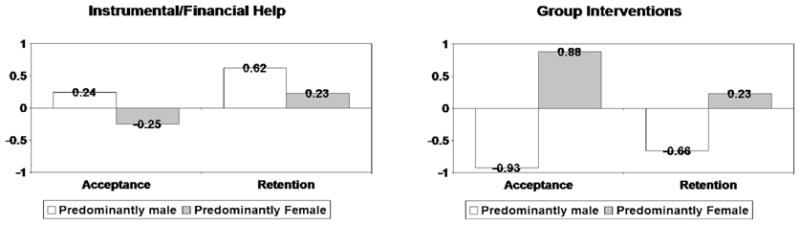
Left: Weighted simple regression coefficients with acceptance and retention as the dependent measures and the continuous index of instrumental/financial incentives as the predictor. Right: Weighted simple regression coefficients with acceptance and retention as the dependent measures and the group format indicator variable as the predictor. All coefficients are statistically significant.
Regressing acceptance rates on the presence of group interventions revealed a positive association for predominantly female samples, but a negative association for predominantly male samples. Thus, these results suggest that group interventions attracted women but not men. Likewise, as shown in Figure 1, predominantly female samples stayed more when the intervention was delivered to groups, whereas predominantly male samples stayed less when the intervention was delivered to groups and more when instrumental/financial help was provided. Thus, these findings strongly support the predicted gender-specific pattern of incentives.
We hypothesized that associations of instrumental/financial resources and the use of group formats with acceptance and retention would be different across men and women. However, because many factors influenced acceptance and retention, it was important to identify potential confounds with gender, instrumental/financial resources, and group formats. Analyses revealed that gender and group formats had significant correlations with other coded characteristics, whereas instrumental/financial resources did not. Specifically, percentage of women correlated negatively with the age of the participants (r = −.37, p = .05), the presence of drug using participants (r = −.22, p = .05), and the presence of military personnel (r = −.33, p = .01), but positively with the inclusion of college students (r = .21, p = .05). Interventions run in groups correlated negatively with inclusion of multiple-partner heterosexuals (r = −.24, p = .05), military personnel (r = −.24, p = .05), and STI-clinic patients (r = −.26, p = .02). Moreover, group formats correlated positively with the inclusion of disadvantaged women (r = .30, p = .01). Thus, these factors were controlled for in supplementary analyses of gender differences. The additional analyses replicated the findings in Tables 1 and 2.
Supplementary Exploratory Analyses of Participation Determinants Among Men and Women
Supplementary analyses were conducted to see if the setting or certain intervention characteristics influenced acceptance and retention in combination with gender (see Table 3). These analyses comprised weighted ANOVAs with an indicator variable or a dichotomized predictor related to the recruitment or intervention and a dichotomized variable for percentage of women. Given the small number of papers reporting size of the targeted audience, the results for acceptance revealed only one interesting interaction between gender and recruitment. This interaction suggested that women were more attracted than men by personal contact at the time of enrollment.
Table 3.
Supplementary Exploratory Moderators of Acceptance and Retention Across Gender Groups
| Predominantly female audiences
|
Predominantly male audiences
|
||||||
|---|---|---|---|---|---|---|---|
| Setting used | Setting not used | Simple effect Qs(1) | Setting used | Setting not used | Simple effect Qs(1) | Interaction Qs(1) | |
| Acceptance | |||||||
| Setting | |||||||
| Hospital setting (k = 19) | −.30 | .17 | 9.90** | −.28 | −.03 | 8.39** | 1.49 |
| Community setting (k = 19) | — | −.15 | — | — | −.23 | — | 0 |
| School setting (k = 19) | .04 | −.16 | .07 | — | −.23 | — | 0 |
| Work setting (k = 19) | .18 | −.29 | 9.50** | −.02 | −.28 | 6.00* | 1.45 |
| Recruited by fliers (k = 19) | — | −.15 | — | — | −.23 | — | 0 |
| Recruited by personal contact (k = 19) | .15 | 0.31 | 6.04* | −.23 | −.25 | .03 | 5.45* |
| Recruited by nurse (k = 13) | — | −.29 | — | −.03 | −.28 | 3.07 | 0 |
| Recruited by peer (k = 13) | — | −.29 | — | — | −.23 | — | 0 |
| Recruited by outreach worker (k = 13) | — | −.29 | — | −.03 | −.28 | 3.07 | 0 |
| Recruited by doctors (k = 13) | — | −.29 | — | −.03 | −.28 | 3.07 | 0 |
| Recruited by research team (k = 13) | −.15 | −.59 | 3.24* | — | −.23 | — | 0 |
|
| |||||||
| Retention | |||||||
| Setting | |||||||
| Hospital setting (k = 77) | −.04 | .58 | 2.80 | 1.05 | .98 | .05 | 44.55*** |
| Community setting (k = 77) | .58 | .12 | 1.59 | −.08 | 1.13 | 8.97** | 182.50*** |
| Work setting (k = 77) | −.27 | .71 | 8.23** | 2.02 | .97 | 6.36** | 253.17*** |
| School setting (k = 77) | 2.21 | .21 | 4.66* | 2.04 | 1.01 | 2.14 | 14.06*** |
| Recruited by fliers (k = 85) | 4.42 | .28 | .38 | .59 | 1.04 | .51 | 10.32*** |
| Recruited by personal contact (k = 85) | .19 | 1.18 | 2.46 | 1.02 | 1.03 | 0 | 22.49*** |
| Recruited by nurse (k = 54) | — | 1.26 | — | 2.20 | 1.17 | 4.56 | 0 |
| Recruited by peer (k = 54) | — | 1.26 | — | .61 | 1.24 | .78 | 0 |
| Recruited by outreach worker (k = 54) | .84 | 1.52 | .61 | .99 | 1.29 | 1.09 | 3.27* |
| Recruited by doctors (k = 54) | — | 1.26 | — | 2.20 | 1.17 | 4.56* | 0 |
| Recruited by research team (k = 54) | 1.47 | .94 | .51 | −.16 | 1.34 | 10.50*** | 80.71*** |
|
| |||||||
| Intervention features | |||||||
| Duration of the intervention | High | Low | High | Low | |||
| Number of sessions (k = 75) | .51 | .90 | .65 | .60 | 1.26 | 10.41*** | 4.65* |
| Number of minutes per session (k = 60) | .88 | .55 | .53 | .14 | 1.11 | 8.68** | 97.23*** |
| Days between baseline and last session (k = 62) | .65 | .69 | 3.38* | .65 | .75 | 40.43*** | 5.45* |
| Intervention strategies | Present | Absent | Present | Absent | |||
| Information on HIV (k = 75) | .33 | .12 | .22 | 1.05 | .99 | 0.05 | 1.82 |
| Information on condoms (k = 75) | .23 | .33 | .07 | .88 | 1.18 | 1.92 | 4.70* |
| Threat/risk arguments (k = 75) | .28 | .29 | 0 | 1.08 | 1.00 | .13 | .67 |
| Attitudinal arguments (k = 75) | .47 | .23 | .30 | .88 | 1.07 | .50 | 15.50*** |
| Normative arguments (k = 75) | −.25 | .60 | 1.87 | .62 | 1.14 | 4.04* | 1.17 |
| Control arguments (k = 75) | .88 | .12 | 3.47* | .72 | 1.36 | 10.32*** | 173.90*** |
| Condom use skills (k = 75) | 1.44 | .22 | 2.19 | .89 | 1.10 | .81 | 58.78*** |
| Negotiation skills (k = 75) | 1.38 | .09 | 7.70** | .64 | 1.23 | 8.20** | 244.90*** |
| HIV testing (k = 75) | −.49 | .59 | 8.07** | 1.16 | .54 | 6.36* | 257.35*** |
| Condoms provided (k = 75) | .16 | .48 | .85 | 1.26 | .50 | 12.31*** | 129.00*** |
Note. Table entries are weighted mean proportions transformed from log odds. All discrete predictors were dummy coded, and continuous variables were dichotomized and dummy-coded. QB for simple and main effect = homogeneity coefficient for the difference across levels of a factor, distributed as a χ2 with number of factor levels −1 degrees of freedom. QB for interaction = homogeneity coefficient for the interaction between factors, distributed as a χ2 with (number of levels of factor A − 1) × (number of levels of factor B − 1) degrees of freedom. Significant QBs indicate significant effects of the involved factors. k = number of conditions in analysis.
Only treatment samples were used in this analysis.
p < .05.
p < .01.
p < .001.
Several interesting interactions emerged for retention across predominantly male and female samples. First, hospital and school settings correlated with more retention for men, whereas hospital and work settings correlated with more retention for men but less for women. Second, recruitment by fliers and longer sessions were associated with better retention for women than men, whereas smaller numbers of sessions and shorter sessions were associated with better retention for men than women. Third, attitudinal arguments, control-enhancing arguments, condom-use-skills training, and negotiation-skills training were associated with better retention for women but worse for men. Fourth, including normative arguments was associated with worse retention than not including them, and this effect was stronger in men than women. Finally, interventions that included HIV testing and condom provision were associated with more retention for men but worse for women.
Discussion
Despite prior valuable contributions in the area of attrition (Oakley, Fullerton, & Holland, 1995; Pedlow and Carey (2003), there has not been a prior conceptual analysis of participation in behavioral-change programs by men and women. Our meta-analysis tested a model of gender differences related to the cultural preferences of men and women. We found support for the need for different external incentives that fit agency needs in men and communion needs in women. Consistent with the gender-specific-resource model, men were better retained by intervention associated to instrumental/financial resources than were women, whereas women mostly enrolled and completed interventions that provided social and emotional incentives, such group designs.
Other interesting findings emerged from more exploratory moderator analyses. First, the intervention setting had a differential effect across genders: school and community intervention settings were linked to better retention in predominantly female samples but worse retention in predominantly male samples. In contrast, work and hospital settings were associated with better retention in predominantly male samples but worse retention in predominantly female samples. Second, recruitment by personal contact attracted women but made no difference for men. Third, both predominantly female and male samples showed more completion in short interventions (i.e., with fewer sessions), but this effect was stronger in the predominantly male samples. Fourth, with regards to session length, predominantly female samples showed more completion of longer sessions, but predominantly male samples showed more completion of shorter sessions. Last, when the intervention included attitudinal arguments, control arguments, condom-use-skills training, and negotiation-skills training, predominantly female samples showed more completion but predominantly male samples showed less completion. Contrarily, when the intervention included HIV testing and condom provision, predominantly male samples showed more completion but predominantly female samples showed less completion.
Implications for Behavioral Interventions
Several important recommendations follow from these findings. First, the implementation of various forms of financial and instrumental assistance seems key to attract men, In this sense, social services must increase efforts to offer support for men, given they often perceive that only women and children receive assistance (Albarracín, Durantini, & Earl, 2007). Second, with regard to the format, individual interventions and short sessions may be advantageous for men. However, if group interventions are the only option (due to budgetary restrictions or other reasons), and/or if monetary incentives are not possible, researchers may need to find ways of changing male norms about social support. Otherwise, the use of group interventions may be a deterrent for men, particularly those who adhere to traditional masculine roles. Finally, the content of the intervention itself is essential to ensure intervention completion by men, particularly the provision of HIV testing and condoms as part of the intervention.
With respect to women, long group sessions seem ideal to obtain enrollment and completion of HIV-prevention interventions. Women also benefit from a small number of sessions, and these formats may be combined with strategies able to raise emotional involvement and gratification: attitudinal and control arguments as well as training in negotiation skills and condom use. Delivery in community settings and schools should also maximize intervention completion in female populations. Hospitals and work places are ideal settings for men. In contrast, the use of financial and instrumental incentives for women deserves further work. In particular, it is presently unclear why predominantly female samples show lesser acceptance of and retention in interventions that offer instrumental/financial resources. On the one hand, women may experience social environmental difficulties attending sessions and thus researchers may unsuccessfully attempt to attract them by increasing the financial/instrumental incentives. On the other hand, female samples might experience greater psychological reactance (Brehm, 1972; Brehm & Cohen, 1962) to external incentives, perhaps because the incentives are perceived as coercive. These possibilities both seem plausible and deserve attention in future research. If the negative association is a result of unsuccessful attempts at increasing participation, more successful procedures should be used. However, if reactance is confirmed, practitioners interested in recruiting and retaining women should use more subtle recruitment tactics.
Implications for Clinical Trials
One interesting aspect is that men seem to enroll more with the use of incentives that could be considered somewhat coercive when one conducts a clinical trial. However, payments are considered coercive only when the amount of money is high. Moreover, IRBs (Institutional Review Boards) have procedures to prevent such coercion (Council for International Organizations of Medical Sciences, 2002; IRB, 2002), and many of the studies involved U.S. researchers who are mandated to have IRB approval. With respect to services, the studies that offered health care, for instance, did not make participation a prerequisite for the care. Quite often, the facility offered care that was available to both participants and nonparticipants. Perhaps more importantly, in real-world conditions, our results imply integrating HIV prevention with other services that are instrumental to men’s goals. Moreover, when countries are resource-deprived, perhaps women are more likely than men to enroll and stay in interventions and should be an important target of interventions.
Limitations and Need for Research on Enrollment and Retention as a Function of Sexual Orientation and Ethnicity
This study has several limitations. First, most meta-analytic findings are correlational. For example, the interactive effects of gender and external resources could potentially be explained by other characteristics of the studies, the populations, or the methods used. Fortunately, however, this limitation was mitigated by our controlling for identified correlates to rule out spurious findings. Second, reports vary in their completion and many important features of a study are not part of standard reports. In our work, whereas intervention characteristics were almost always described, much less information was given about how samples were recruited and what incentives were offered. Hopefully, as researchers and journal editors become aware of the implications of such limited reporting, future meta-analyses may replicate these conclusions with a larger sample of studies. Also, primary research may effectively address some of these questions, including the processes that mediate some of our findings.
Although men and women were shown to differ in patterns of enrollment and retention, only 8% of the synthesized samples included men who have sex with men. Clearly, the motivations underlying enrollment and attrition may also differ across gay and straight people. As more research accrues, these analyses will be essential to understand how to reach groups with varying sexual orientation. Similarly, women and men vary in ethnicity, age, and many other factors. Unfortunately, however, the data available to date does not permit analyses crossing gender with these factors and then with the incentives offered in experimental interventions. Future work should address this important problem.
Our findings should also be analyzed in relation to the nature of the behavior, as men and not women are the actual users of condoms. One may argue, for example, that women may enroll or stay for social reasons only because the behavior is not relevant to them. Although the enrollment and retention dynamics may differ in domains such as seeking a mammography, our past data do not imply lack of relevance for women. For example, Noguchi et al. (2007) reported that women have higher enrollment rates than men whereas men have higher retention rates than men. All in all then, these findings suggest that different aspects of condom-use interventions are of interest to each group, and that factors other than HIV prevention come to play.
Final Note
Our study represents a first step in understanding differences in participation across men and women. The findings revealed that the needs of a particular population hold the key to understanding and, hopefully, increasing participation in HIV-prevention programs. We hope that these findings, which were inspired by broad social psychological concepts, will reduce the spread of HIV among women and men all over the globe.
Acknowledgments
This research was funded by grants from the National Institutes of Health (K02-MH01861 and R01-NR08325). We thank Laura Glasman, Ece Kumkale, and Allison Earl, as well as the undergraduate research assistants working in the second author’s lab during the academic years 2002–2006, for their invaluable assistance with this project. We also thank the attitudes lab at the Department of Psychology at the University of Florida for a discussion of the ideas reported in this article.
Contributor Information
Marta R. Durantini, Department of Psychology, University of Florida, Gainesville, Florida
Dolores Albarracín, Department of Psychology, University of Florida, and Department of Psychology, University of Illinois at Urbana-Champaign.
References
- Albarracín D, Durantini MR, Earl A. Unpublished focus groups data. 2007 Unpublished raw data. [Google Scholar]
- Albarracín D, Gillette JC, Earl AN, Glasman LR, Durantini MR, Ho MH. A test of major assumptions about behavior change: A comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychological Bulletin. 2005;131:856–897. doi: 10.1037/0033-2909.131.6.856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Albizu-García CE, Alegría M, Freeman D, Vera M. Gender and health services use for a mental health problem. Social Science & Medicine. 2001;53:865–878. doi: 10.1016/s0277-9536(00)00380-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bakan D. The duality of human existence. Chicago: Rand McNally; 1966. [Google Scholar]
- Barragán M, Hicks G, Williams MV, Franco-Paredes C, Duffus W, del Río C. Low health literacy is associated with HIV test acceptance. Journal of General Medicine. 2005;20:422–425. doi: 10.1111/j.1525-1497.2005.40128.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brannen SJ, Rubin A. Comparing the effectiveness of gender-specific and couple groups in a court-mandated spouse abuse treatment program. Research on Social Work Practice. 1996;6:405–424. [Google Scholar]
- Brehm JW. Responses to loss of freedom: A theory of psychological reactance. Washington, D. C: General Learning Corporation, National Bureau of Education, Department of the Interior; 1972. [Google Scholar]
- Brehm JW, Cohen AR. Explorations in cognitive dissonance. New York: Wiley; 1962. [Google Scholar]
- Carlson R. Sex differences in ego functioning: Exploratory studies of agency and communion. Journal of Consulting and Clinical Psychology. 1971;37:267–277. doi: 10.1037/h0031947. [DOI] [PubMed] [Google Scholar]
- Carrington GE. Predictors of African American male utilization of individual counseling services. Dissertation Abstracts International Section A: Humanities & Social Sciences. 2004;65:1675. [Google Scholar]
- Centers for Disease Control and Prevention. Data and statistics. 2006 Retrieved March 20, 2006, from http://www.cdc.gov/scientific.htm.
- Condelli WS, Koch MA, Fletcher B. Treatment refusal/attrition among adults randomly assigned to programs at a drug. Journal of Substance Abuse Treatment. 2000;18:395–407. doi: 10.1016/s0740-5472(99)00086-0. [DOI] [PubMed] [Google Scholar]
- Council for International Organizations of Medical Sciences . International ethical guidelines for biomedical research involving human subjects. Geneva, Swiss: 2002. [PubMed] [Google Scholar]
- Durantini MR, Albarracín D, Mitchell AL, Earl AN, Gillette JC. Influential agents of behavior change for different genders, ethnicities, ages, and behaviorally-defined groups: A meta-analysis of HIV-prevention interventions. Psychological Bulletin. 2006;132:212–248. doi: 10.1037/0033-2909.132.2.212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galdas PM, Cheater F, Marshall P. Men and heath help-seeking behavior: Literature review. Journal of Advanced Nursing. 2005;49:616–623. doi: 10.1111/j.1365-2648.2004.03331.x. [DOI] [PubMed] [Google Scholar]
- Hader SL, Smith DK, Moore JS, Holmberg SD. HIV infection in women in the United States. Journal of the America Medical Association. 2001;285:1186–1192. doi: 10.1001/jama.285.9.1186. [DOI] [PubMed] [Google Scholar]
- Hedges LV, Olkin I. Statistical methods for meta-analysis. San Diego, CA: Academic Press; 1985. [Google Scholar]
- Hegelson VS. Relation of agency and communion to well-being: Evidence and potential explanation. Psychological Bulletin. 1994;116:412–428. [Google Scholar]
- HRSA Care ACTION. HIV/AIDS in racial and ethnic minorities. 1999 Retrieved on March 20, 2006, from http://hab.hrsa.gov/publications/hrsa299.htm.
- Hussaini BA, Moore ST, Cain VA. Psychiatric symptoms and help seeking behavior among the elderly: And analysis of racial and gender differences. Journal of Gerontological Social Work. 1994;21:177–193. [Google Scholar]
- Institutional Review Board. Guidebook. 2002;3 Retrieved August 18, 2008, from http://www.hhs.gov/ohrp/irb/irb_guidebook.htm. [Google Scholar]
- Johnson ME. Influences of gender and sex role orientation on help-seeking attitudes. Journal of Psychology. 1988;122:237–241. [Google Scholar]
- Lee F. The social costs of seeking help. The Journal of Applied Behavioral Sciences. 2002;38:17–35. [Google Scholar]
- Leong FT, Zachar P. Gender and opinions about mental illness as predictors of attitudes toward seeking professional psychological help. Journal of Guidance & Counseling. 1999;27:123–132. [Google Scholar]
- Maslow AH. A theory of human motivation. Psychological Review. 1943;50:370–396. [Google Scholar]
- National Institutes of Health. Women and girls and HIV/AIDS. 2007 Retrieved January 10, 2007, from http://www.oar.nih.gov/about/research/women.
- Noguchi K, Albarracín D, Durantini MR, Glasman LR. Who is exposed to which health promotion programs? A meta-analysis of motivations underlying enrollment and retention in HIV prevention interventions. Psychological Bulletin. 2007;133:955–975. doi: 10.1037/0033-2909.133.6.955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oakley A, Fullerton D, Holland J. Behavioural interventions for HIV/AIDS prevention. AIDS. 1995;9:479–486. [PubMed] [Google Scholar]
- Pearson S. Men’s use of sexual health services. Family Planning and Reproductive Health Care. 2003;29:190–194. doi: 10.1783/147118903101198060. [DOI] [PubMed] [Google Scholar]
- Pedlow CT, Carey MP. HIV sexual risk reduction interventions for youth. Behavior Modification. 2003;27:135–190. doi: 10.1177/0145445503251562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rabinowitz DC. Predictors of attrition in a predominantly Caucasian middle-class clinic-based weight loss program. Dissertation Abstracts International, Section B. 2002;62:5796. [Google Scholar]
- Rosener J. America’s competitive secret: Women managers. New York: Oxford University Press; 1995. [Google Scholar]
- Ross MW, Essien EJ, Williams ML, Fernandez ME. Concordance between sexual behavior and sexual identity in street outreach samples of four racial/ethnic groups. Sexually Transmitted Diseases. 2003;30:110–113. doi: 10.1097/00007435-200302000-00003. [DOI] [PubMed] [Google Scholar]
- Rutledge SE, Roffman RA, Picciano JF, Kalichman SC, Berghius JP. HIV prevention and attrition: Challenges and opportunities. AIDS and Behavior. 2002;6:69–82. [Google Scholar]
- Sayre SL, Schmitz JM, Stotts AL, Averill PM, Rhades HM, Grabowski JJ. Determining predictors of attrition in an out-patient substance abuse program. American Journal of Drug and Alcohol Abuse. 2002;28:55–72. doi: 10.1081/ada-120001281. [DOI] [PubMed] [Google Scholar]
- Schilling RF, Sachs C. Attrition from an evening alcohol rehabilitation program. American Journal of Drug and Alcohol Abuse. 1993;19:239–248. doi: 10.3109/00952999309002683. [DOI] [PubMed] [Google Scholar]
- Schweitzer CN. A study of the relationship between psychosocial factors and attrition, compliance, and gains in Phase II cardiac rehabilitation. Dissertation Abstracts International, A. 1997;58:0392. [Google Scholar]
- Spicer J. Minnesota model: Evolution of multidisciplinary approach to addiction recovery. Center City, MN: Hazelden; 1993. [Google Scholar]
- Stolley KS. Male versus female sterilization: A social power model. Dissertation Abstracts International, Section A. 1997;57:3699. [Google Scholar]
- Thom B. Sex differences in help-seeking for alcohol problems: Barriers to help-seeking. British Journal of Addiction. 1986;81:777–788. doi: 10.1111/j.1360-0443.1986.tb00405.x. [DOI] [PubMed] [Google Scholar]
- Toft D. The Minnesota Model: Humane, holistic, flexible. Hazelden News Professional Update I. 1995;2:16. [Google Scholar]
- Veach LJ, Ramley TP, Kippers SM, Sorg JD. Retention predictors related to intensive outpatients programs for substance use disorders. American Journal of Drug and Alcohol Abuse. 2000;26:417–428. doi: 10.1081/ada-100100253. [DOI] [PubMed] [Google Scholar]
- Wang MC, Bushman BJ. Integrating results through meta-analytical review using SAS software. Cary, NC: SAS Institute; 1999. [Google Scholar]
- Weinhardt LS, Carey MP, Carey KB, Verdecias RN. Increasing assertiveness skills to reduce HIV risk among women living with a severe and persistent mental illness. Journal of Consulting and Clinical Psychology. 1998;66:680–684. doi: 10.1037//0022-006x.66.4.680. [DOI] [PubMed] [Google Scholar]
- Weissman MM, Kleiman GL. Sex differences and the epidemiology of depression. Archives of General Psychiatry. 1977;34:98–111. doi: 10.1001/archpsyc.1977.01770130100011. [DOI] [PubMed] [Google Scholar]
- Wenger N, Linn LS, Epstein M, Shapiro MF. Reduction of high-risk sexual behavior among heterosexual undergoing HIV antibody testing: A randomized clinical trial. American Journal of Public Health. 1991;91:1580–1585. doi: 10.2105/ajph.81.12.1580. [DOI] [PMC free article] [PubMed] [Google Scholar]