

Abstract
Objectives. The aim was (1) to investigate the association between education and smoking status (current, former and never-smoking) among non-western immigrants in Norway and (2) examine if these associations fit the pattern predicted by the model of the cigarette epidemic.
Design. Data came from the Oslo Health Study and the Oslo Immigrant Health study (2000–2002). The first included all Oslo citizens from seven selected birth cohorts. The second included all Oslo citizens born in Turkey, Iran, Pakistan, Vietnam and Sri Lanka. 14,768 respondents answered questions on smoking, education and relevant background variables (over-all response rate 43.3%). Two gender specific multinomial logistic regression models with smoking status [current, former or never-smoker (reference)] as dependent variable were computed and predicted probabilities of smoking status among groups with different levels of education were calculated.
Results. Smoking prevalence among men ranged from 19% among Sri Lankans to 56% among Turks. Compared to the smoking prevalence among Norwegian men (27%), smoking was widespread among Iranians (42%) and Vietnamese (36%). Higher education was associated with lower probability of current smoking among all male immigrant groups except Sri Lankans. Never having smoked was positively associated with education among Pakistani and Norwegian men. Among women, < 5% smoked among Pakistanis, Vietnamese and Sri Lankans. Smoking prevalence among Turkish (28%) and Iranian (23%) women were comparable to Norwegian women (30%). The probability of smoking among Turkish and Iranian women with secondary education was higher than for other levels of education. The probability of being a never-smoker was high among Turkish and Iranian women with primary education.
Conclusions. High smoking prevalence among Turkish and Iranian men highlights the importance of addressing smoking behaviour in subgroups of the general population. Smoking was almost non-existent among Pakistani, Vietnamese and Sri Lankan women and indicates strong persistent social norms against smoking.
Keywords: smoking, education, immigrants, diffusion, epidemic
Introduction
During the last decades, cigarette smoking has changed from being a widespread and accepted practice to being a marker of social inequality. Today, there is a strong negative association between socioeconomic position (SEP) and smoking in most developed countries, including Norway (Giskes et al. 2005, Lund and Lindbak 2007).
The last decades have also been a period of ethnic diversification. In most European countries, immigrants from non-western countries have become increasingly common. With them, immigrants bring culturally specific health behaviours related to diet, alcohol consumption and smoking, among others. Regarding tobacco, studies from European countries report large differences in tobacco use between different ethnic groups (Bhopal et al. 2004, Gadd et al. 2005).
Few studies have addressed the role of SEP for smoking among immigrants. A Swedish study found higher odds of smoking for Arabic speaking men compared to Swedish men and lower odds for Arabic speaking women compared to Swedish women. These differences remained after controlling for education (Lindström and Sundquist 2002). Two Dutch studies found strong associations between smoking and education among immigrant groups (Nierkens et al. 2006, van Oort et al. 2006). In the former study, a negative socioeconomic gradient in smoking was observed for Turkish and Moroccan men. For Turkish and Moroccan women, however, the gradient was positive. The authors argued that this pattern fitted the pattern of the cigarette epidemic, in which people with higher education were the first to adopt and later stop smoking, followed by less educated groups.
The immigrant population in the Oslo, the capital city, defined as people born outside Norway with non-Norwegian parents, accounted for 22.3% of the total population in 2010. About 38.9% came from Europe, 38.7% from Asia including Turkey and 14.9% from Africa (Statistics Norway 2010a). More than 30% of all non-western immigrants in Norway live in Oslo (Henriksen 2007).
Given the relatively large and increasing number of citizens with immigrant background, knowledge of smoking patterns in these groups is increasingly important when assessing smoking behaviour in the general population. In addition, as smoking is the largest single cause of premature death in the developed world (Peto et al. 1996), knowledge about how smoking varies with SEP is crucial in identifying at-risk groups and implementing preventive measures against social inequalities in health.
For these reasons, this study will examine associations between education and smoking status (current, former and never-smokers) among five large non-western immigrant groups in Norway: Turks, Iranians, Pakistanis, Vietnamese and Sri Lankans. Furthermore, the study will examine whether cigarette use among immigrants fits the pattern suggested by the cigarette epidemic model and discuss some social mechanisms that can explain variations in smoking status between immigrant groups and the majority Norwegian population.
Theory and hypothesis
There are numerous factors that link smoking with socioeconomic status, including social norms, symbolic content of smoking, peer behaviour, perception of the health risks involved and perceived benefits resulting from smoking such as weight control and stress reduction. While all these factors are most likely associated with differences in smoking between SEP groups, they shed little light on why smoking has changed dramatically for men and women with different SEP during the last century.
In developed countries, studies have shown that smoking diffused through society in a uniform pattern that resembled an epidemic in which those with higher SEP were the first to adopt and later quit smoking (Ferrence 1989). The rise and fall of cigarette smoking can be divided into four stages. In the first stage (1900–1920), smoking was introduced among men with higher SEP while remaining marginal among women. In the second stage (1920–1950), smoking increased sharply, and reached more than half of the male population in most societies, while smoking among women increased to around 20% and became a widespread middle class and later working class habit. In the third stage (1950–1980), smoking began to decline, especially among those with higher SEP. Smoking among women reached a maximum of approximately 40%. In the last stage (1980–2000), smoking prevalence decreased among both men and women to around 20% (Ferrence 1989, Lopez et al. 1994).
Although, the model of cigarette diffusion accurately predicts the spread of smoking in most European countries (Pampel 2002), several factors suggest different smoking patterns among non-western immigrants. Studies have shown that most people start to smoke in late adolescence and that smoking habits acquired in adolescence shape later smoking behaviour (Jackson and Dickinson 2004). It is therefore likely that immigrants will maintain smoking habits from their countries of birth. However, several factors may influence smoking patterns after immigration, such as new information on the health consequences of smoking, increased income, different social norms, increasingly negative symbolic content and stricter legislation with regard to where smoking is allowed.
Among those who have not started to smoke before emigrating, there may still be cultural norms that hinder or promote smoking initiation. In most European countries, smoking is as prevalent today among men as among women. If immigrants adopt the smoking patterns of the majority, one would expect an increase in smoking prevalence for women who have emigrated from countries with a low female smoking prevalence. However, this would mainly concern those who grew up in the host country. In contrast, if norms restricting smoking among women are sufficiently strong, they might counter such processes.
The development of cigarette use over time suggests a specific relationship between education and smoking status at different stages of the epidemic. The first stage is characterised by few current smokers, a positive association between education and current smoking, few former smokers and a high percentage of never-smokers. In the second stage, the percentage of current smokers is higher, the association between education and current smoking is weaker and the percentage of never-smokers is lower compared to stage 1. In the two subsequent stages, the fraction of current smokers peaks and starts to decrease, the number of former smokers increases and the association between education and current smoking is increasingly negative.
To determine the extent and stage of smoking among immigrants, this study will examine (1) the percentage of current, former and never-smokers among men and women with non-western immigrant backgrounds and (2) the association between education and current, former and never-smoking within each immigrant group. Results will be compared to results from the majority Norwegian population.
Method
Sample
The data in this study came from two linked and pooled cross-sectional population surveys conducted in Oslo in 2000–2002: the Oslo Health Study (HUBRO) and the Oslo Immigrant Health Study (Immigrant-HUBRO), conducted by the Norwegian Institute of Public Health and the University of Oslo. HUBRO was carried out in May 2000 to September 2001 and included all registered citizens in Oslo born in 1924, 1925, 1940, 1941, 1955, 1960 and 1970.
The information brochure and the main and supplementary questionnaires (filled out after a clinical examination) were available in 11 different languages. 40,888 persons were invited to participate. Of these, 18,770 (45.9%) attended a clinical examination and/or submitted at least one questionnaire (Søgaard et al. 2004).
Due to the limited number of immigrants in the HUBRO study, a follow up study (Immigrant-HUBRO) was conducted in 2002 and included adults from the five biggest immigrant groups in Oslo at that time: Pakistanis, Iranians, Vietnamese, Sri Lankans and Turks. Those who had been invited to participate in the HUBRO study were not invited, to avoid participation in both studies. With the exception of Pakistanis,1 all first generation immigrants living in Oslo and born between 1942 and 1971 with the above-mentioned immigrant backgrounds were invited to participate (N = 7890). Three thousand and nineteen attended a clinical examination and/or submitted at least one questionnaire. The participation rate ranged from 31.7% (Pakistanis) to 50.9% (Sri Lankans) (Kumar et al. 2008). The average response rate was 38.3%.
As there were almost no immigrants among respondents born in 1924 and 1925, these cohort were left out.2 The overall response rate from both surveys excluding the 1924 and 1925 cohorts was 18,205/42,048 (43.3%).
Problems with self-selection in the HUBRO study have been addressed and people with lower secondary education or less and people born outside Norway were under-represented. However, for respondents under 45 years of age with primary or secondary education, attendance was higher for people born in non-western countries compared to Norwegians (Søgaard et al. 2004). There has not been carried out a similar evaluation for Immigrant-HUBRO, but a comparison of education among immigrant groups in the survey with official statistics did not show large discrepancies (Kumar et al. 2008).
Measures
Smoking status was determined by asking respondents if they smoked currently, had smoked before or had never smoked.
Information about country of birth, age, gender and marital status was collected from population registers.
Immigrant was defined as being born outside Norway with non-Norwegian parents. Respondents were also asked whether they had lived most of their time before the age of 16 years within or outside Norway.
Age was calculated as year of survey participation minus year of birth and varied from 20 to 61 years. Marital status was coded into two values, ever married and never married.
Number of years of education was recoded into three categories, primary (8 or 9 years or less), secondary (12 or 13 years) and tertiary (13 or more years), based on the education system in the country of birth.
The number of study participants with information on all variables was 14,768.
Analysis
Due to large gender differences in smoking observed in previous studies of non-western immigrants, men and women were examined separately. Using the mlogit command in STATA 11.2, two gender-specific multinomial logistic regression models were constructed with smoking status (never-smoker = reference) as dependent variables and country of birth (Norway = reference), age, education (tertiary = reference), marital status (ever married = reference) as independent variables.
As the primary interest was differences in smoking status among immigrants with different levels of education, an interaction between country of birth and education was included in the models. This increased model fit for both women and men.
Age squared was included as previous research has shown that the relationship between age and smoking may be curvilinear (Rogers et al. 1995). Although small, the coefficients were with one exception significant and likelihood-ratio tests indicated better model fit when age squared was included.
Likelihood-ratio tests showed that inclusion of a variable indicating if the respondent had grown up in Norway (grew up outside Norway = reference) improved model fit for women. For men, the variable was not significantly associated with smoking status nor increased model fit and was therefore not included. Norwegian born men and women who had grown up outside Norway were not included in the study.3 The full models are shown in Appendix 1.
From these two models, adjusted marginal mean probabilities of being a current, former and never-smoker within groups with different levels of education were computed for men and women. Differences between probabilities were tested with chi-square tests. All differences in probabilities described were significant at the 5% level unless stated otherwise.
Average marginal effects (AME) and adjusted marginal mean probabilities were computed to examine the association between the dependent variable and age, not having married and having grown up in Norway within each immigrant group.
Results
Descriptive statistics for the sample are shown in Table 1. Compared to the majority Norwegian population, smoking prevalence among men was high in all groups, except for Sri Lankans. Smoking among Turkish men was particularly high (56%). For women, there was a marked difference in smoking prevalence between Turks, Iranians and Norwegians on the one side and Sri Lankans, Pakistanis and Vietnamese on the other. Whereas 30% of Norwegian, 28% of Turkish and 23% of Iranian women smoked daily, this applied to less than 5% of Pakistani and Vietnamese women. The percentage of daily smokers among Norwegian women in Oslo was higher compared to the 25% reported by official statistics for this period (Statistics Norway 2010b).
Table 1.
Distribution of men and women by smoking status, education and demographic characteristics. Oslo 2000/2002. Percents and 95% confidence intervals (95% CI).
| Turkey |
Iran |
Pakistan |
Vietnam |
Sri Lanka |
Norway |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Percent | 95% CI | Percent | 95% CI | Percent | 95% CI | Percent | 95% CI | Percent | 95% CI | Percent | 95% CI | |
| Men | ||||||||||||
| Smoking status | ||||||||||||
| Current | 55.7 | 50.4–61.0 | 41.6 | 37.1–46.1 | 33.7 | 29.1–38.2 | 36.3 | 31.1–41.6 | 18.8 | 15.7–21.8 | 26.6 | 25.4–27.9 |
| Former | 21.6 | 17.1–26.0 | 23.6 | 19.7–27.5 | 18.5 | 14.8–22.3 | 33.5 | 28.4–38.7 | 14.9 | 12.1–17.6 | 28.3 | 27.0–29.6 |
| Never | 22.8 | 18.3–27.3 | 34.8 | 30.5–39.2 | 47.8 | 43.0–52.6 | 30.1 | 25.1–35.1 | 66.4 | 62.7–70.0 | 45.1 | 43.7–46.5 |
| Education | ||||||||||||
| Primary | 41.3 | 36.0–46.6 | 3.0 | 1.5–4.6 | 15.9 | 12.3–19.4 | 30.4 | 25.4–35.5 | 6.5 | 4.6–8.4 | 10.4 | 9.6–11.3 |
| Secondary | 33.2 | 28.2–38.3 | 32.3 | 28.0–36.5 | 48.0 | 43.2–52.9 | 33.5 | 28.4–38.7 | 58.4 | 54.6–62.3 | 22.5 | 21.3–23.7 |
| Tertiary | 25.4 | 20.8–30.1 | 64.7 | 60.4–69.1 | 36.1 | 31.4–40.8 | 36.0 | 30.8–41.3 | 35.0 | 31.4–38.7 | 67.1 | 65.8–68.4 |
| Grew up in Norway | 7.8 | 4.9–10.7 | 4.8 | 2.8–6.7 | 15.1 | 11.6–18.6 | 14.9 | 11.0–18.8 | 5.9 | 4.1–7.7 | 100.0 | - |
| Not married | 8.1 | 5.2–11.0 | 26.4 | 22.4–30.4 | 5.6 | 3.4–7.8 | 25.5 | 20.7–30.2 | 10.9 | 8.5–13.3 | 40.6 | 39.2–42.0 |
| Age (mean) | 39.4 | 38.4–40.5 | 40.3 | 39.6–41.0 | 42.2 | 41.2–43.3 | 41.3 | 40.3–42.3 | 39.0 | 38.5–39.6 | 44.5 | 44.2–44.9 |
| N | 334 | 462 | 410 | 322 | 645 | 4,861 | ||||||
| Women | ||||||||||||
| Smoking status | ||||||||||||
| Current | 27.6 | 22.6–32.7 | 23.3 | 18.8–27.8 | 3.7 | 1.7–5.7 | 4.9 | 2.8–7.1 | 0.2 | −0.2–0.6 | 30.1 | 28.9–31.3 |
| Former | 17.1 | 12.9–21.3 | 11.6 | 8.2–15.1 | 2.6 | 0.9–4.2 | 3.9 | 2.0–5.8 | 0.6 | −0.1–1.3 | 26.5 | 25.4–27.7 |
| Never | 55.3 | 49.7–60.9 | 65.1 | 60.0–70.2 | 93.8 | 91.2–96.3 | 91.2 | 88.3–94 | 99.2 | 98.5–100.0 | 43.4 | 42.1–44.7 |
| Education | ||||||||||||
| Primary | 59.5 | 54.0–65.1 | 14.3 | 10.6–18.1 | 33.5 | 28.6–38.5 | 42.9 | 37.9–47.8 | 8.8 | 6.3–11.3 | 9.6 | 8.8–10.3 |
| Secondary | 23.7 | 18.9–28.5 | 31.0 | 26.1–36.0 | 42.0 | 36.9–47.2 | 28.6 | 24.1–33.1 | 61.3 | 57.0–65.5 | 25.1 | 24.0–26.2 |
| Tertiary | 16.8 | 12.6–21.0 | 54.6 | 49.3–60.0 | 24.4 | 19.9–28.9 | 28.6 | 24.1–33.1 | 29.9 | 26.0–33.9 | 65.3 | 64.1–66.5 |
| Grew up in Norway | 10.5 | 7.1–14 | 5.7 | 3.2–8.2 | 13.4 | 9.8–16.9 | 17.1 | 13.4–20.9 | 8.6 | 6.2–11.0 | 100.0 | - |
| Not married | 5.3 | 2.7–7.8 | 9.9 | 6.7–13.0 | 4.8 | 2.6–7.1 | 26.0 | 21.6–30.4 | 6.8 | 4.7–9.0 | 37.4 | 36.1–38.6 |
| Age (mean) | 36.7 | 35.7–37.8 | 38.6 | 37.6–39.6 | 39.4 | 38.4–40.4 | 39.8 | 38.8–40.8 | 35.9 | 35.2–36.6 | 44.2 | 43.9–44.5 |
| N | 304 | 335 | 352 | 385 | 511 | 5,847 | ||||||
Norwegians was the only group in which daily smoking was as widespread among women as among men. Smoking among people from other countries could either be characterised as high for men and intermediate for women (Turkey and Iran) or intermediate for men and low for women (Sri Lanka, Pakistan and Vietnam).
For women born in Sri Lanka, only 1 out of 511 answered that she smoked daily, and only three answered that they had smoked previously. Due to the limited number of daily and former smokers, Sri Lankan women were eliminated from further analyses, reducing the effective sample size for the multivariate analysis to 14,257.
To examine the position of different immigrant groups within the framework of the cigarette epidemic, predicted probabilities of being a current, former and never-smoker among immigrant groups and the Norwegian majority was calculated (Appendix 2).
Education and current smoking among men
Among Turkish men the probability of being a current smoker was 0.18 points higher for men with secondary education compared to those with tertiary and 0.11 points higher than those with primary education4 (Figure 1). Similar to Turkish men, the probability of being a current smoker was 0.09 points higher among Iranian men with secondary education compared to tertiary.
Figure 1.
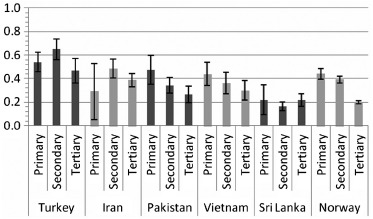
Marginal mean probabilities and 95% confidence intervals of current smoking at different levels of education. Men, Oslo 2000/2002.
Among Pakistani, Vietnamese and Norwegian men the probability of being a current smoker fell with increasing education. Differences between men with tertiary and primary education were 0.21 points for Pakistanis, 0.14 points among Vietnamese and 0.24 points for Norwegians.
In addition, for Pakistani and Norwegian men the probability of being a current smoker was 0.14 and 0.05 points lower for men with secondary compared to primary education.5 For Norwegians, a statistically significant difference was also found between those with secondary and tertiary education.
Education and former smoking among men
The probability of being a former smoker was 0.11 points lower for Turkish men with secondary education compared to men with tertiary6 and 0.09 points lower than those with primary education (Figure 2).
Figure 2.
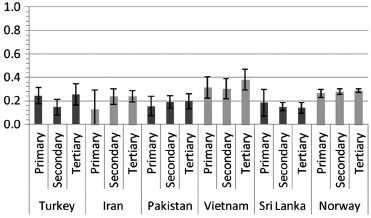
Marginal mean probabilities and 95% confidence intervals of former smoking at different levels of education. Men, Oslo 2000/2002.
The probability of being a former smoker was stable across education among men with other country backgrounds. However, the probability of being a former smoker was generally high for Vietnamese men compared to other immigrant groups.
Education and never-smoking among men
The probability of never having smoked was 0.18 points higher for Iranian men with tertiary education compared to secondary (Figure 3). Among Pakistanis and Norwegians, the probability of never having smoked rose with increasing education. In both groups, the probability of never-smoking was higher for men with tertiary education compared to primary (0.17 and 0.21 points, respectively).
Figure 3.
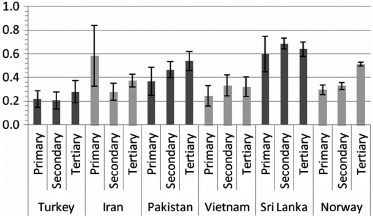
Marginal mean probabilities and 95% confidence intervals of never-smoking at different levels of education. Men, Oslo 2000/2002.
There was no relationship between education and being a current, former or never-smoker for Sri Lankan men. The probability of never having smoked was 0.6 or above for all levels of education.
The probability of being a current, former or never-smoker among Iranian men with primary education differed substantially from the two other levels of education. Wide confidence intervals indicated that the large differences were most likely the result of the low number of Iranian men with primary education in our data (N = 14).
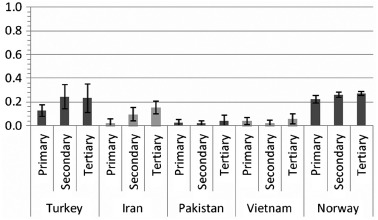
Education and current smoking among women
Turkish and Iranian women displayed similar tendencies as Turkish and Iranian men: The probability of being a current smoker was higher for those with secondary education compared to the two other levels of education, although statistically significant differences were only found for Iranian women (Figure 4).
Figure 4.
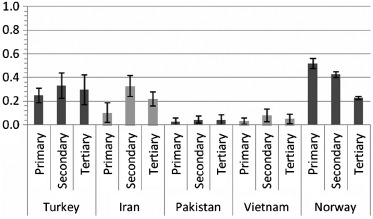
Marginal mean probabilities and 95% confidence intervals of current smoking at different levels of education. Women, Oslo 2000/2002.
For Pakistani and Vietnamese women the probability of current smoking was low at all levels of education (0.05 or below for Pakistanis and 0.08 or below for Vietnamese), although there was a tendency that Vietnamese women with secondary education had a higher probability of smoking than those with primary.
The probability of being a current smoker among Norwegian women was similar to Norwegian men both regarding size and direction: smoking decreased with increasing education.
Education and former smoking among women
The probability of being a former smoker was around 0.05 or below for Pakistani and Vietnamese women, regardless of education (Figure 5).
Figure 5.
Marginal mean probabilities and 95% confidence intervals of former smoking at different levels of education. Women, Oslo 2000/2002.
Among Turkish and Norwegian women the probability of being a former smoker was generally higher than for other groups (above 0.20 with the exception of Turkish women with primary education).
The probability of being a former smoker was 0.11 points higher for Turkish women with secondary compared to primary education and 0.05 points higher for Norwegian women with tertiary education compared to primary.
Similarly, among Iranians the probability of being a former smoker was higher among women with tertiary compared to primary education. However, for all levels of education the probabilities were low compared to Norwegian women, especially for those with primary education (0.02 for Iranian and 0.27 for Norwegian women).
Education and never-smoking among women
Regarding the probability for never having smoked, Turkish and Iranian women displayed similar profiles (Figure 6). Those with primary education had relatively high probability of never having smoked (0.62 for Turks and 0.88 among Iranians) and in both groups the probabilities were higher for those with primary education compared to any other level of education.
Figure 6.
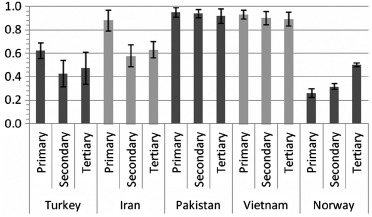
Marginal mean probabilities and 95% confidence intervals of never-smoking at different levels of education. Women, Oslo 2000/2002.
For Pakistani and Vietnamese women, the probability of never having smoked was around 0.9 or above for all groups regardless of education.
In contrast, the probability of never having smoked increased with education among Norwegian women. Norwegian women with tertiary education were twice as likely (0.50) to never having smoked compared to those with primary education (0.26).
Besides education, smoking status varied with other independent variables (see Appendix 1).7 For men, the relationships between predicted probabilities of being a current smoker and age were curvilinear.8 For Iranian, Pakistani and Vietnamese men the probability varied between around 0.20 at 18 years of age to around 0.40 among men in their mid-40s. At 60 years of age, the probability was around 0.30 for all three groups. For Norwegian men the pattern was similar but at all ages the probabilities were around 0.10 points lower. Among Turkish men, the probability of current smoking was greater at all ages, varying from 0.37 at 18 years to 0.59 at 45 years to 0.49 at 60 years. Compared to other groups, the probability of current smoking varied little with age among Sri Lankan men.
The association between age and being a current smoker among Turkish, Iranian and Norwegian women were similar in shape to Norwegian men. However, for Turkish and Iranian women the probabilities were generally lower. Among Pakistani and Vietnamese women, the probabilities of current smoking were low (below 0.10) for all ages.
For both men and women, those who had never been married had higher probability of being a current smoker compared to those having married. Among men the increase in probability of being a current smoker varied between 0.04 points (4%) for Sri Lankans and 0.06 points for Turks, Iranians and Vietnamese. Among women the increase in probability of being a current smoker varied from 0.01 points for Pakistanis and Vietnamese to 0.07 points for Turks and Norwegians.
The probability of being a current smoker was greater among women who had grown up in Norway compared to those who had not and varied with country background. The probability increased with around 0.20 points for Turks and Iranians and around 0.06 points for Pakistanis and Vietnamese.
Discussion
The main findings from this study are, first, that there are large differences in smoking prevalence between men and women with different non-western immigrant backgrounds, even for those who, from a European perspective, have emigrated from the same region. This highlights the importance of country specific analyses. Second, the study shows that education plays an important role for smoking status among men with non-western immigrant backgrounds in Norway, except for Sri Lankans. Education also played a role for smoking status among Turkish and Iranian women.
The initial rapid increase in cigarette smoking in most European countries fits the pattern described by the theory of diffusion of innovations (Ferrence 1989), developed by Rogers (2003). According to Rogers, diffusion consists of an innovation being communicated through a social structure over time. The innovation can be a product, norm, habit, belief and so on. The success of diffusion depends on the distance and quality of communication between those who first discover the innovation (innovators) and the rest of the social system. In the beginning only a few will adhere to the innovation (early adopters). However, if a sufficient number of people pick up the innovation (early majority) the phenomenon gains critical mass and spreads through the social structure. With time most of the group members will adhere to the innovation (late majority and laggards) (Rogers 2003).
New inventions or ideas may counteract or substitute older ones (Ferrence 2001). After widespread use, cigarette smoking has declined substantially in most countries with a long history of cigarette use. The diffusion of new information about the negative health effects of smoking, the implementation of smoke-free policies and changes in the symbolic content of smoking are likely to have made important contributions to the decline in smoking.
From a diffusion perspective, high smoking prevalence and low probability of never having smoked among Turkish and Iranian men indicate that in these groups, cigarette smoking has diffused throughout the social structure. The lower probability of smoking for men with tertiary education compared to secondary education suggests that smoking prevalence for men has reached its peak. However, the lack of a clear association between smoking cessation and education indicates that the decline in smoking, as predicted by the cigarette epidemic model, has not begun.
The relatively high smoking prevalence among Turkish and Iranian women with secondary education and the high probability of never having smoked among Turkish and Iranian woman with primary education suggests that uptake of smoking is limited to those with higher education. If those with primary education adopt the smoking pattern of higher educated women it is likely that the prevalence of smoking will remain high or even increase before decreasing.
Comparing these results with the cigarette epidemic model, Turks and Iranians would best be described as being late in stage two or early in stage three. The relatively high smoking prevalence among Pakistani and Vietnamese men and the very low smoking prevalence among Pakistani and Vietnamese women suggest that these groups are at the beginning of the cigarette epidemic. In comparison, the strong negative association between education and being a current smoker and the equally strong positive association between education and never having smoked among Norwegian men and women is in line with being in the fourth and last stage of the cigarette epidemic.
However, there are several findings that do not support a diffusion-based explanation. The high probability of being a never-smoker among Turkish and Iranian women with primary education suggests that women from these countries are at the beginning of the cigarette epidemic. Yet, the relatively high probability of being a former smoker among women with secondary or tertiary education from these two countries is a trait associated with being in a late stage of the epidemic.
Moreover, the smoking prevalence and the negative association between education and being a current smoker among Pakistani and Vietnamese men were similar to findings among Norwegian men. According to diffusion theory, smoking among Pakistani and Vietnamese women should be similar to Turkish, Iranian or Norwegian women. Yet, the low smoking prevalence, lack of association between education and cigarette smoking and high probability of never having smoked does not indicate that any diffusion of smoking habits has taken place.
Also, there does not seem to be any relationship between factors that are important for diffusion, in this case education, and current, former or never-smoking for Sri Lankan men, even though around 20% answered that they smoked daily. Finally, for Turks and Iranians of both genders, there was a general tendency that those with primary education had approximately the same probability of current smoking as those with tertiary education and, at the same time, lower probability than those with secondary education. This seems at odds with the diffusion process.
These discrepancies suggest the existence of strong cultural determinants of smoking, which limit or even block diffusion. From a social mechanism perspective, to understand peoples’ actions one should examine their desires, beliefs and opportunities (Hedström 2005) and successful diffusion will depend on all three.
Widespread adoption of cigarette smoking in the western world at the beginning of the twentieth century depended on both geographic and economic availability. A precondition for increased cigarette use among women in this period was the weakening of social norms restricting smoking. In comparison to cigars, pipe smoking or use of snuff, the cigarette was the first tobacco product that became acceptable among women. With the industrial revolution more spare time became available to a larger part of the population and cigarettes became an important component of new social rituals. Increased labour force participation among women increased both economic freedom and exposure to cigarette smoking (Collins 2004).
Besides opportunity, the cigarette has been an object of desire. To a large degree, this desire has been created by the tobacco industry (Brandt 2007), but is also likely to be the result of a ‘forbidden fruit’ type of social mechanism. In addition, the heavily debated role of smoking made cigarettes a forceful symbol of social and sexual liberation, especially for women, thereby giving young people motives to smoke (Brandt 2007).
The large differences in smoking prevalence between Turkish and Iranian women on the one hand and Pakistani, Vietnamese and Sri Lankan women on the other suggests that opportunity plays an important part in women's smoking. Studies have shown that there are strong social norms against women smoking in Pakistan (Bush et al. 2003), Sri Lanka (Seimon and Mehl 1998) and Vietnam (Morrow et al. 2002). The almost non-existent prevalence of smoking among Sri Lankan women in Norway mirrors findings from Sri Lanka (Chapman and Leng 1990).
It is likely that such norms could be linked to religion. Although smoking is not specifically prohibited in Islam (Ghouri et al. 2006), Nierkens et al. (2006) found that strong Muslim identification was associated with lower smoking prevalence for young Turkish adults in the Netherlands. However, the large differences in smoking prevalence for women from predominantly Muslim countries (Iran, Pakistan and Turkey) suggest that religion alone cannot account for these differences.
The low smoking prevalence among some women in our study suggests that gender-specific norms are at work among immigrant groups and maintained after emigration. Even though above 60% of Pakistanis and around 50% of Sri Lankans had lived in Norway for more than 15 years (Henriksen 2007), smoking prevalences were similar to prevalences in their countries of birth (Mackay and Eriksen 2002). The large differences between women from Pakistan, Vietnam and Sri Lanka on the one hand and Norwegian women on the other indicate a low degree of adoption of smoking habits from the Norwegian majority.
Like other immigrant groups, smoking among Turks resembles smoking in their country of birth. However, as noted by Dağli, although Turkey has a long history of tobacco use, American cigarettes were not introduced until the fall of the Turkish tobacco monopoly in the 1980s. This new form of tobacco circumvented older norms for tobacco use, especially for women. The open market also introduced cigarette advertising, which appealed to new consumer groups, such as groups with shorter education (Dağli 1999).
The changed market situation thus affected both opportunity and motives for smoking. Increased smoking among women after the introduction of foreign cigarettes could be a sign of opposition to traditional norms (Yuksel and Corbett 2005) in much the same way as European women used cigarettes at the beginning of the twentieth century.
The historical development of cigarette smoking in Turkey could help explain the observed smoking pattern among Turkish immigrants. While Turkish men have been smoking for decades and switched to cigarettes in the 1980s, social norms delayed the onset of smoking among women. The educational differences in smoking for Turkish men in our study could indicate that those with primary education are lagging behind in the diffusion process (or they could still use traditional forms of tobacco) while those with tertiary education have already begun adopting a new and healthier lifestyle. The relatively low smoking prevalence for women with primary education could reflect a more traditional view of smoking as not being acceptable among women.
In addition to opportunity and motivation, information about the negative health effects of smoking is likely to be of great importance for the diffusion process. Today, the amount of information available is much greater than at the beginning of the twentieth century and may disrupt diffusion. In a study of smoking in Malawi and Zambia, smoking was more prevalent among those with short education (Pampel 2005). The author argued that both increased knowledge of the adverse health effects of smoking among higher educated, and a relativisation of these effects by those less well off, resulted in a negative socioeconomic gradient in smoking, even though these countries could be characterised as early in the diffusion process. This could explain the negative educational gradient in smoking for Pakistani and Vietnamese men and also the positive association between smoking cessation and education among Turkish (and to some degree Iranian) women.
The findings in this article indicate that we can expect persistently high prevalences of smoking for Turkish and Iranian men with primary and secondary education and Pakistani men with primary education. In addition, the low smoking prevalence among some women indicates a strong potential for increased smoking, if these women adopt smoking habits from either men from their own country of birth or from the majority Norwegian population. This will depend on the persistence of smoking-related social norms and the spread of information about the negative health effects.
Strengths and limitations
There are several limitations of this study that must be addressed. Smoking among non-western immigrants in developed countries is a complex phenomenon involving several social factors such as social norms and the symbolic content of cigarette smoking. Moreover, the role of education in the rise and fall of cigarette smoking is difficult to determine on the basis of a cross-sectional study.
The cross-sectional data used in this study does not enable us to determine the causal effect of education on smoking or examine how smoking patterns change over time when moving to or growing up in a new smoking culture. However, when focusing on the associations between education and current, former and never-smoking, traits of the dynamic relationship between education and smoking can be examined.
One advantage of the data used in this study was that all citizens in Oslo from selected birth cohorts and country backgrounds were invited to participate. This ensured a relatively large number of respondents with immigrant backgrounds compared to studies based on randomly selected respondents from the general population.
All information material and survey questionnaires were distributed in the respondents’ national languages. However, even though several steps were taken to increase attendance the overall response rate was relatively low (43.3%). There may be several reasons for this. First, both surveys included a detailed questionnaire, a supplementary questionnaire and a clinical trial. For some, this may have been too time-consuming.
Second, some of the questions were of a personal and/or medical nature. If some of the questions were regarded as improper in some groups, members may have refrained from participating. This may account for the low response rates among immigrants from predominantly Muslim countries (32.7% among Turks, 31.7% among Pakistanis and 38.8% among Iranians) (Kumar et al. 2006).
Information about country of birth, age, marital status and gender came from official records. In contrast, data on smoking were self-reported. This is generally not a large problem, as research has show that self-reported smoking is normally an accurate measure for adults (Patrick et al. 1994). However and more important for this study, self-reported smoking behaviour might depend on how socially acceptable smoking is viewed in different cultures. This might partially account for the low smoking prevalence among women from Pakistan, Vietnam and Sri Lanka. It is also possible that the respondents smoked or used other tobacco products than cigarettes such as chewing tobacco or water pipes.
It is likely that differences between groups are influenced by selection caused by variations in immigration history. For example, smoking prevalence for Iranian women was relatively high compared to findings from Iran (Sarraf-Zadegan et al. 2004). Ninety percent of Iranians immigrating to Norway in the wake of the 1979 Iranian revolution were political refugees and had relatively long education (Henriksen 2007). It is therefore likely that those who emigrated were more liberal and/or had better social or economic opportunities to smoke compared to the majority Iranian population.
Yet, even though Iranian and Turkish immigrants have similar smoking patterns, their immigration history differs. Immigrants from Turkey arrived at the beginning of the 1970s and were predominantly young men with higher education than Turkish men generally and the main objective was work. Pakistanis share a similar history. Most Pakistanis who arrived were men from white-collar backgrounds and for many, manual work in Norway represented a reduction of social status (Tjelmeland and Brochmann 2003).
In contrast, most Vietnamese arrived as refugees in the aftermath of the Vietnamese war in 1975 and had generally little formal education. Sri Lankans arrived after the Sri Lankan civil war that ended in 1983 and almost all had primary education (Henriksen 2007).
Selection may also account for the variation in response rates. If acculturation or social integration was related to both participation and smoking, estimates may be biased. As noted above, respondents with short education were underrepresented among Norwegians. Given the social gradient in smoking in this group, this may have resulted in an under-representation of smokers. For all immigrant groups except Vietnamese, the response rates were generally lower for women than for men. If less integrated Turkish and Iranian women refrained from participating, this may have resulted in an overestimation of current smokers.
Although selection related to immigration histories or response rates may account for some of the variations in smoking patterns, finding in this paper suggests that cultural opportunities for smoking are particularly important, especially for women. The striking difference in smoking pattern between Turkish and Pakistani women, groups with similar immigration histories, is one example.
Key messages
-
(1)
This is the first study to examine the association between education and smoking among immigrants in Norway. Few European studies have addressed socioeconomic differences in smoking among immigrants.
-
(2)
Findings indicated large gender variations in smoking and very high smoking prevalence among Turkish and Iranian men with secondary education.
-
(3)
Higher education was associated with lower probability of smoking among all male immigrant groups except Sri Lankans.
-
(4)
Steps should be taken to prevent increased smoking prevalence among immigrant women.
Acknowledgements
Funding for this research was provided by the Norwegian Research Council (project no. 190443, ‘Tobacco and the social inequality gap’). I would like to thank Karl Erik Lund, Ellen J. Amundsen, Stale Østhus, Willy Pedersen and the Norwegian Institute of Public Health for comments.
Appendix
Appendix 1.
Multinomial logistic regression model of being a current, former or never-smoker (reference) controlling for education, country of birth, age, marital status and place of upbringing. Coefficients, standard errors (SE) and p-values. Oslo 2000/2002. Men and women separately.
| Men |
Women |
|||||
|---|---|---|---|---|---|---|
| Coefficient | SE | p-value | Coefficient | SE | p-value | |
| Current smoker | ||||||
| Education (tertiary = ref) | ||||||
| Primary | 1.34 | 0.12 | 0.00 | 1.51 | 0.12 | 0.00 |
| Secondary | 1.12 | 0.09 | 0.00 | 1.12 | 0.08 | 0.00 |
| Country of birth (Norway = ref) | ||||||
| Turkey | 1.61 | 0.27 | 0.00 | 1.53 | 0.40 | 0.00 |
| Iran | 1.00 | 0.14 | 0.00 | 0.88 | 0.31 | 0.01 |
| Pakistan | 0.31 | 0.21 | 0.13 | − 1.32 | 0.63 | 0.03 |
| Vietnam | 0.91 | 0.24 | 0.00 | − 1.18 | 0.45 | 0.01 |
| Sri Lanka | − 0.07 | 0.17 | 0.69 | – | – | – |
| Education * country of birth (Norwegians with tertiary education = ref) | ||||||
| Primary * Turkey | − 0.94 | 0.36 | 0.01 | − 1.99 | 0.40 | 0.00 |
| Primary * Iran | − 2.09 | 0.64 | 0.00 | − 2.65 | 0.53 | 0.00 |
| Primary * Pakistan | − 0.37 | 0.36 | 0.30 | − 1.98 | 0.84 | 0.02 |
| Primary * Vietnam | − 0.68 | 0.37 | 0.07 | − 2.09 | 0.64 | 0.00 |
| Primary * Sri Lanka | –1.27 | 0.44 | 0.00 | – | – | – |
| Secondary * Turkey | − 0.48 | 0.36 | 0.18 | − 0.89 | 0.44 | 0.05 |
| Secondary * Iran | − 0.60 | 0.25 | 0.02 | − 0.61 | 0.30 | 0.04 |
| Secondary * Pakistan | − 0.71 | 0.27 | 0.01 | − 1.08 | 0.71 | 0.13 |
| Secondary * Vietnam | − 0.97 | 0.34 | 0.01 | − 0.70 | 0.57 | 0.22 |
| Secondary * Sri Lanka | –1.47 | 0.23 | 0.00 | – | – | – |
| Age | 0.14 | 0.03 | 0.00 | 0.29 | 0.03 | 0.00 |
| Age squared | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Never married (ever married = ref) | 0.21 | 0.08 | 0.01 | 0.30 | 0.07 | 0.00 |
| Grew up in Norway (no = ref) | – | – | – | 1.18 | 0.26 | 0.00 |
| Constant | − 4.34 | 0.56 | 0.00 | − 8.06 | 0.67 | 0.00 |
| Former smoker | ||||||
| Education (tertiary = ref) | ||||||
| Primary | 0.47 | 0.13 | 0.00 | 0.47 | 0.13 | 0.00 |
| Secondary | 0.42 | 0.09 | 0.00 | 0.44 | 0.08 | 0.00 |
| Country of birth (Norway = ref) | ||||||
| Turkey | 0.72 | 0.31 | 0.02 | 0.78 | 0.46 | 0.09 |
| Iran | 0.32 | 0.16 | 0.05 | 0.03 | 0.37 | 0.94 |
| Pakistan | − 0.38 | 0.23 | 0.10 | − 1.78 | 0.65 | 0.01 |
| Vietnam | 0.91 | 0.23 | 0.00 | − 1.46 | 0.48 | 0.00 |
| Sri Lanka | − 0.73 | 0.20 | 0.00 | – | – | – |
| Education * country of birth (Norwegians with tertiary education = ref) | ||||||
| Primary * Turkey | − 0.26 | 0.42 | 0.53 | − 1.36 | 0.45 | 0.00 |
| Primary * Iran | –1.58 | 0.82 | 0.06 | − 2.87 | 1.04 | 0.01 |
| Primary * Pakistan | − 0.30 | 0.45 | 0.51 | − 1.03 | 0.84 | 0.22 |
| Primary * Vietnam | − 0.38 | 0.38 | 0.32 | − 0.85 | 0.59 | 0.15 |
| Primary * Sri Lanka | − 0.12 | 0.47 | 0.79 | – | – | – |
| Secondary * Turkey | − 0.67 | 0.46 | 0.14 | − 0.27 | 0.49 | 0.58 |
| Secondary * Iran | − 0.14 | 0.29 | 0.64 | − 0.81 | 0.41 | 0.05 |
| Secondary * Pakistan | − 0.29 | 0.31 | 0.36 | − 1.23 | 0.84 | 0.14 |
| Secondary * Vietnam | − 0.69 | 0.34 | 0.05 | − 1.54 | 0.84 | 0.07 |
| Secondary * Sri Lanka | − 0.42 | 0.26 | 0.11 | – | – | – |
| Age | 0.07 | 0.03 | 0.02 | 0.20 | 0.03 | 0.00 |
| Age squared | 0.00 | 0.00 | 0.36 | 0.00 | 0.00 | 0.00 |
| Never married (ever married = ref) | − 0.07 | 0.08 | 0.36 | − 0.12 | 0.08 | 0.14 |
| Grew up in Norway (no = ref) | - | - | - | 0.88 | 0.32 | 0.01 |
| Constant | − 2.96 | 0.61 | 0.00 | − 5.89 | 0.73 | 0.00 |
| Pseudo R2 | 0.06 | 0.09 | ||||
| N | 7034 | 7223 | ||||
Appendix 2.
Adjusted* marginal mean probabilities (p) and 95% confidence intervals (95% CI) of current, former and never-smoking at different levels of education among groups with different country backgrounds. Oslo 2000/2002. Men and women separately.
| Current smokers |
Former smokers |
Never-smokers |
||||
|---|---|---|---|---|---|---|
| p | 95% CI | p | 95% CI | p | 95% CI | |
| Men | ||||||
| Turkey | ||||||
| Primary | 0.54 | 0.46–0.62 | 0.24a | 0.17–0.31 | 0.22 | 0.15–0.29 |
| Secondary | 0.65c | 0.56–0.74 | 0.15 | 0.08–0.21 | 0.20 | 0.13–0.28 |
| Tertiary | 0.47 | 0.36–0.57 | 0.26 | 0.16–0.35 | 0.28 | 0.18–0.37 |
| Iran | ||||||
| Primary | 0.29 | 0.05–0.53 | 0.13 | − 0.04–0.29 | 0.58a | 0.33–0.84 |
| Secondary | 0.48c | 0.40–0.56 | 0.24 | 0.17–0.30 | 0.28c | 0.21–0.35 |
| Tertiary | 0.39 | 0.33–0.44 | 0.24 | 0.19–0.29 | 0.37 | 0.32–0.43 |
| Pakistan | ||||||
| Primary | 0.48b | 0.35–0.60 | 0.16 | 0.07–0.24 | 0.37b | 0.25–0.49 |
| Secondary | 0.34 | 0.28–0.41 | 0.19 | 0.14–0.24 | 0.47 | 0.40–0.54 |
| Tertiary | 0.27 | 0.19–0.34 | 0.19 | 0.13–0.26 | 0.54 | 0.46–0.62 |
| Vietnam | ||||||
| Primary | 0.44b | 0.34–0.54 | 0.32 | 0.23–0.41 | 0.24 | 0.16–0.33 |
| Secondary | 0.36 | 0.27–0.45 | 0.30 | 0.22–0.39 | 0.33 | 0.24–0.42 |
| Tertiary | 0.30 | 0.22–0.38 | 0.38 | 0.29–0.47 | 0.32 | 0.24–0.40 |
| Sri Lanka | ||||||
| Primary | 0.22 | 0.09–0.34 | 0.18 | 0.07–0.30 | 0.60 | 0.45–0.75 |
| Secondary | 0.17 | 0.13–0.20 | 0.15 | 0.11–0.19 | 0.69 | 0.64–0.73 |
| Tertiary | 0.22 | 0.17–0.27 | 0.14 | 0.10–0.19 | 0.64 | 0.58–0.70 |
| Norway | ||||||
| Primary | 0.44b | 0.40–0.49 | 0.26 | 0.23–0.30 | 0.30b | 0.25–0.34 |
| Secondary | 0.39c | 0.36–0.42 | 0.28 | 0.25–0.30 | 0.33c | 0.30–0.36 |
| Tertiary | 0.20 | 0.19–0.21 | 0.29 | 0.27–0.30 | 0.51 | 0.49–0.53 |
| Women | ||||||
| Turkey | ||||||
| Primary | 0.25 | 0.19–0.31 | 0.13a | 0.08–0.18 | 0.62ab | 0.55–0.69 |
| Secondary | 0.33 | 0.22–0.44 | 0.24 | 0.14–0.34 | 0.43 | 0.31–0.54 |
| Tertiary | 0.30 | 0.17–0.42 | 0.23 | 0.11–0.35 | 0.47 | 0.34–0.61 |
| Iran | ||||||
| Primary | 0.10ab | 0.02–0.18 | 0.02ab | − 0.02–0.06 | 0.88ab | 0.79–0.97 |
| Secondary | 0.33c | 0.24–0.42 | 0.10 | 0.04–0.15 | 0.58 | 0.48–0.67 |
| Tertiary | 0.22 | 0.16–0.27 | 0.15 | 0.10–0.21 | 0.63 | 0.56–0.70 |
| Pakistan | ||||||
| Primary | 0.03 | 0.00–0.06 | 0.02 | 0.00–0.05 | 0.95 | 0.91–0.99 |
| Secondary | 0.04 | 0.01–0.07 | 0.02 | 0.00–0.04 | 0.94 | 0.90–0.98 |
| Tertiary | 0.04 | 0.00–0.08 | 0.04 | 0.00–0.09 | 0.92 | 0.86–0.98 |
| Vietnam | ||||||
| Primary | 0.03 | 0.00–0.06 | 0.04 | 0.01–0.07 | 0.93 | 0.89–0.97 |
| Secondary | 0.08 | 0.03–0.13 | 0.02 | − 0.01–0.04 | 0.90 | 0.85–0.96 |
| Tertiary | 0.05 | 0.01–0.09 | 0.06 | 0.01–0.10 | 0.89 | 0.84–0.95 |
| Norway | ||||||
| Primary | 0.52ab | 0.47–0.56 | 0.22b | 0.19–0.26 | 0.26ab | 0.23–0.30 |
| Secondary | 0.42c | 0.40–0.45 | 0.26 | 0.24–0.28 | 0.32c | 0.29–0.34 |
| Tertiary | 0.23 | 0.21–0.24 | 0.27 | 0.26–0.28 | 0.50 | 0.49–0.52 |
Adjusted for age, marital status and whether the respondent had grown up in Norway (women only).
p < 0.05 for differences between primary and secondary education.
p < 0.05 for differences between primary and tertiary education.
p < 0.05 for differences between secondary and tertiary education.
Notes
Due to the large number of Pakistanis in Oslo a 30% random sample was invited.
3584 out of 6730 (53.3%) attended a clinical examination and/or submitted at least one questionnaire.
42 women (0.9%) and 56 men (1.0%).
X2 = 3.05, p = 0.08.
X2 = 3.53, p = 0.06 for Pakistanis and X2 = 3.07, p = 0.08 for Norwegians.
X2 = 3.51, p = 0.06.
Tables showing probabilities and average marginal effects for other independent variables than education are not included.
As the model did not include an interaction between country of birth and other variables except education, it is not possible to examine possible variations in the directions of the associations between age, marital status and place of upbringing between immigrant groups.
References
- Bhopal R., et al. Review of prevalence data in, and evaluation of methods for cross cultural adaptation of, UK surveys on tobacco and alcohol in ethnic minority groups. British medical journal. 2004;328(7431):76–78. doi: 10.1136/bmj.37963.426308.9A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brandt A.M. The cigarette century: the rise, fall, and deadly persistence of the product that defined America. New York: Basic Books; 2007. [Google Scholar]
- Bush J., et al. Understanding influences on smoking in Bangladeshi and Pakistani adults: community based, qualitative study. British medical journal. 2003;326(7396):962–965. doi: 10.1136/bmj.326.7396.962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chapman S., Leng W.W. Tobacco control in the third world, a resource atlas. Penang, Malaysia: International Organizatoin of Consumer Unions; 1990. [Google Scholar]
- Collins R. Interaction ritual chains. Princeton, NJ: Princeton University Press; 2004. [Google Scholar]
- Dağli E. Are low income countries targets of the tobacco industry? The international journal of tuberculosis and lung disease. 1999;3:113–118. [PubMed] [Google Scholar]
- Ferrence R.G. Deadly fashion: the rise and fall of cigarette smoking in North America. New York: Garland; 1989. [Google Scholar]
- Ferrence R.G. Diffusion theory and drug use. Addiction. 2001;96:165–173. doi: 10.1046/j.1360-0443.2001.96116512.x. [DOI] [PubMed] [Google Scholar]
- Gadd M., et al. Do immigrants have an increased prevalence of unhealthy behaviours and risk factors for coronary heart disease? European journal of cardiovascular prevention & rehabilitation. 2005;12:535–541. doi: 10.1097/01.hjr.0000174829.25388.ed. [DOI] [PubMed] [Google Scholar]
- Ghouri N., Atcha M., Sheikh A. Influence of Islam on smoking among Muslims. British medical journal. 2006;332(7536):291–294. doi: 10.1136/bmj.332.7536.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giskes K., et al. Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. Journal of epidemiology and community health. 2005;59:395–401. doi: 10.1136/jech.2004.025684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hedström P. Dissecting the social. On the principles of analytical sociology. Cambridge: Cambridge University Press; 2005. [Google Scholar]
- Henriksen K. Fakta om 18 innvandrergrupper i Norge. Oslo: Statistics Norway; 2007. [Google Scholar]
- Jackson C., Dickinson D. Cigarette consumption during childhood and persistence of smoking through adolescence. Archives of pediatrics & adolescent medicine. 2004;158:1050–1056. doi: 10.1001/archpedi.158.11.1050. [DOI] [PubMed] [Google Scholar]
- Kumar B.N., et al. Ethnic differences in obesity among immigrants from developing countries, in Oslo, Norway. International journal of obesity. 2006;30:684–690. doi: 10.1038/sj.ijo.0803051. [DOI] [PubMed] [Google Scholar]
- Kumar B.N., et al. The Oslo immigrant health profile. Oslo: Norwegian institute of public health; 2008. [Google Scholar]
- Lindström M., Sundquist J. Ethnic differences in daily smoking in Malmo, Sweden: Varying influence of psychosocial and economic factors. European journal of public health. 2002;12:287–294. doi: 10.1093/eurpub/12.4.287. [DOI] [PubMed] [Google Scholar]
- Lopez A.D., Collishaw N.E., Piha T. A descriptive model of the cigarette epidemic in developed countries. Tobacco control. 1994;3:242–247. [Google Scholar]
- Lund M., Lindbak R.L. Norwegian tobacco statistics 1973–2006. Oslo: Norwegian Institute for Alcohol and Drug Research; 2007. [Google Scholar]
- Mackay J., Eriksen M. The tobacco atlas. Geneva: World Health Organization; 2002. [Google Scholar]
- Morrow M., et al. Smoking and young women in Vietnam: the influence of normative gender roles. Social science & medicine. 2002;55:681–690. doi: 10.1016/s0277-9536(01)00310-0. [DOI] [PubMed] [Google Scholar]
- Nierkens V., De Vries H., Stronks K. Smoking in immigrants: do socioeconomic gradients follow the pattern expected from the tobacco epidemic? Tobacco control. 2006;15:385–391. doi: 10.1136/tc.2006.014902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pampel F.C. Inequality, diffusion, and the status gradient in smoking. Social problems. 2002;49:35–57. [Google Scholar]
- Pampel F.C. Patterns of tobacco use in the early epidemic stages: Malawi and Zambia, 2000–2002. American journal of public health. 2005;95:1009–1015. doi: 10.2105/AJPH.2004.056895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick D.L., et al. The validity of self-reported smoking: a review and meta-analysis. American journal of public health. 1994;84:1086–1093. doi: 10.2105/ajph.84.7.1086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peto R., et al. Mortality from smoking worldwide. British medical bulletin. 1996;52:12–21. doi: 10.1093/oxfordjournals.bmb.a011519. [DOI] [PubMed] [Google Scholar]
- Rogers E.M. Diffusion of innovations. New York: Free Press; 2003. [Google Scholar]
- Rogers R.G., Nam C.B., Hummer R.A. Demographic and socioeconomic links to cigarette smoking. Social biology. 1995;42:1–21. doi: 10.1080/19485565.1995.9988884. [DOI] [PubMed] [Google Scholar]
- Sarraf-Zadegan N., et al. Tobacco use among Iranian men, women and adolescents. European journal of public health. 2004;14:76–78. doi: 10.1093/eurpub/14.1.76. [DOI] [PubMed] [Google Scholar]
- Seimon T., Mehl G.L. Strategic marketing of cigarettes to young people in Sri Lanka: “go ahead – I want to see you smoke it now”. Tobacco control. 1998;7:429–433. doi: 10.1136/tc.7.4.429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Statistics Norway. Immigrants, by country background (table 07110) [online] 2010a. Available from: http://statbank.ssb.no [Accessed 30 October 2010]
- Statistics Norway. Daily smokers and occasional smokers, by region (table 07662) 2010b. [online]. Available from: http://statbank.ssb.no [Accessed 30 October 2010]
- Søgaard A.J., et al. The Oslo health study: the impact of self-selection in a large, population-based survey. International journal for equity in health. 2004;3:3–14. doi: 10.1186/1475-9276-3-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tjelmeland H., Brochmann G. I globaliseringens tid, 1940–2000. Oslo: Pax; 2003. [Google Scholar]
- Van Oort F., et al. Determinants of daily smoking in Turkish young adults in the Netherlands. Bmc public health. 2006;6:294–302. doi: 10.1186/1471-2458-6-294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yuksel H., Corbett K.K. Mixed messages: a qualitative study of the meanings and context of high school students’ tobacco use in Turkey. Health promotion international. 2005;20:360–366. doi: 10.1093/heapro/dai019. [DOI] [PubMed] [Google Scholar]