

Abstract
A 57-year-old woman with a history of hypertension, hyperlipidemia and stable angina is described. A coronary angiogram revealed the presence of a single coronary artery arising from the right sinus of Valsalva that was providing the left anterior descending (LAD), left circumflex and right coronary artery branches, with noncritical occlusive atherosclerotic plaques at the proximal circumflex artery. A small hypoplastic LAD tapering proximally was found, but no LAD and compensatory collateral circulatory vessels were observed distally. In the present report, the authors discuss this extremely rare combination of congenital coronary anomalies and their clinical implications.
Keywords: Coronary anomaly, Hypoplastic left anterior descending artery, Single coronary artery
Congenital coronary anomalies are found in approximately 1% of all patients undergoing coronary angiography (CAG) (1). Single coronary artery (SCA) is a rare congenital anomaly that is observed in approximately 0.02% of the population (2). In SCA, only one coronary artery arises from the aortic trunk from a single coronary ostium and supplies the entire heart. SCAs are usually asymptomatic and benign, but some SCA variants have been reported to carry a significant risk for severe cardiac events, including myocardial infarction and sudden cardiac death, especially during exercise (3). Based on the site of origin, the anatomical course and its clinical relevance, Yamanaka and Hobbs (1), and Lipton et al (4) have classified SCA anomalies into different groups (R, L, I to III). In contrast, hypoplastic coronary artery (HCA), a rare congenital abnormality, refers to congenital under-development of one or more major branches of the coronary arteries with the absence of compensatory collateral circulatory vessels (5).
In the current report, we present an extremely rare combination of congenital coronary artery anomalies formed with SCA and HCA detected incidentally during routine CAG in a female patient with stable angina pectoris.
CASE PRESENTATION
A 57-year-old woman was admitted to the cardiology department with stable angina pectoris. Her risk factors for coronary artery disease were hypertension and hyperlipidemia. The patient complained of exertional chest pain for the past five months, with evidence of inducible myocardial ischemia on exercise test. A stress test using thallium-201 imaging was performed and showed a perfusion defect involving the anteroseptal segment. On admission, the patient was asymptomatic. The physical examination was normal and the electrocardiogram showed atypical ST segment abnormalities in leads V4 to V6. An echocardiogram revealed normal left ventricular systolic function (ejection fraction 58%) and wall motions. CAG was performed. The left coronary artery ostium could not be cannulated selectively. The left coronary ostium was not observed by aortography or ventriculography (Figure 1A). Selective cannulation of the right sinus of Valsalva demonstrated an SCA originating from the right sinus of Valsalva. The left anterior descending (LAD) and circumflex (CX) arteries arose separately from a common trunk (Figures 1B and 1C). The LAD artery was very thin and hypoplastic and tapered proximally. No LAD artery and compensatory collateral circulatory vessels were observed distally (Figures 1B and 1C). The SCA was classified as type R-III. Furthermore, the angiogram revealed a noncritical atherosclerotic plaque at the proximal CX artery. A conservative treatment regimen with diltizem and nitrate was recommended in addition to avoidance of strenuous exercise.
Figure 1).
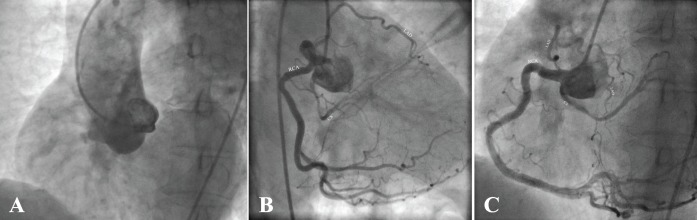
Single coronary artery arising from the right sinus of Valsalva and hypoplastic left anterior descending artery. A Left anterior oblique view of aortography demonstrating no left coroner ostium. B Right anterior oblique view 20°, caudal 30°. C Left anterior oblique view 25°, cranial 35°
DISCUSSION
SCA arising from the right sinus of Valsalva is a rare congenital coronary anomaly, particularly in the absence of other cardiac congenital diseases, and represents approximately 2% to 4% of all coronary anomalies (1,2,4). SCAs are usually associated with other congenital cardiac anomalies such as bicuspid aortic valve, mitral valve prolapse and ventricular septal defect (1,6). Lipton et al (4) were the first to classify SCA anomalies. Later, this classification was further modified by Yamanaka and Hobbs (1) based on their origin (right or left sinus of Valsalva) and the anatomical course (I, II or III) with regard to the ascending aorta and pulmonary trunk. Type L refers to a right coronary artery (RCA) arising from the left main coronary system, whereas type R refers to a coronary artery originating from the RCA. According to the subgroup designation, group I refers to an anomalous coronary artery with an anatomical course of either a solitary dominant normal RCA or left coronary artery (R-I or L-I). Group II refers to the relationship between the anomalous coronary artery and the aorta and pulmonary artery. Group III describes an anomaly in which the LAD and CX arteries arise separately from the proximal part of the normal RCA. The SCA in the patient described in the present report was classified as type R-III according to this classification.
The clinical significance of a SCA is primarily dependent on its course relative to the great arteries, being of potential risk for myocardial ischemia and sudden cardiac death. Extremely rare group I (R-I, L-I type) anomalies generally have a benign clinical course; however, the R II–III type and L II–III type anomalies, having a coronary artery branch following a dangerous course between the aorta and pulmonary trunk, may predispose to myocardial ischemia and arrhythmias during exercise (6,7).
HCA was first reported in 1970 and refers to congenital under-development of one or more major branches of the coronary arteries with significantly decreased luminal diameter or length. Its incidence is approximately 0.02% at autopsy (5). HCA is often revealed by sudden death, especially in young adults and athletes, but it can also cause myocardial ischemia and infarction (5). LAD artery agenesis and HCA have been reported as benign variants that can cause myocardial ischemia. There have been only two reports of an SCA associated with an absent or hypoplastic LAD artery in the literature (8,9). Prashanth and Mukhaini (9) reported a rare type of SCA originating from the right sinus of Valsalva, with the CX artery continuing from the RCA and hypoplastic LAD artery, which was incidentally found in a 63-year-old woman who presented with unstable angina. To the best of our knowledge, the present report is the first to describe an R-III type SCA associated with a hypoplastic LAD artery. In our patient, detailed investigation for ischemia was performed using the treadmill exercise test and stress test using thallium-201 imaging. Both techniques documented evidence of persistent myocardial ischemia. The anteroseptal defects during stress with incomplete redistribution at rest on thallium scintigraphy result from silent ischemia. In healthy individuals, compensatory collateral circulatory vessels originating from the RCA, CX or the distal LAD arteries supply this myocardial area. In our patient, the LAD artery was underdeveloped and collateral vessel flow to the left ventricle was insufficient, which led to inadequate stress perfusion. However, Shirani and Roberts (10) reported that 15% of SCA patients may expereince myocardial ischemia caused directly by abnormal anatomy of the arteries and not by coronary artery disease (10), which may be an alternative explanation for the compensatory collateral circulation observed in the present case.
REFERENCES
- 1.Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary angiography. Cathet Cardiovasc Diagn. 1990;21:28–40. doi: 10.1002/ccd.1810210110. [DOI] [PubMed] [Google Scholar]
- 2.Desmet W, Vanhaecke J, Vrolix M, et al. Isolated single coronary artery: A review of 50 000 consecutive coronary angiographies. Eur Heart J. 1992;13:1637–40. doi: 10.1093/oxfordjournals.eurheartj.a060117. [DOI] [PubMed] [Google Scholar]
- 3.Frescura C, Basso C, Thiene G, et al. Anomalous origin of coronary artery and risk of sudden death: A study based on an autopsy population of congential heart disease. Hum Pathol. 1998;29:689–95. doi: 10.1016/s0046-8177(98)90277-5. [DOI] [PubMed] [Google Scholar]
- 4.Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: Diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130:39–47. doi: 10.1148/130.1.39. [DOI] [PubMed] [Google Scholar]
- 5.Zugibe FT, Zugibe FT, Jr, Costello JT, Breithaupt MK. Hypoplastic coronary artery disease in the spectrum of sudden unexpected death in young and middle age adults. Am J Forensic Med Pathol. 1993;14:276–83. doi: 10.1097/00000433-199312000-00002. [DOI] [PubMed] [Google Scholar]
- 6.Angelini P. Coronary artery anomalies – current clinical issues: Definitions, classification, incidence, clinical relevance, and treatment guidelines. Texas Heart Inst J. 2002;29:271–8. [PMC free article] [PubMed] [Google Scholar]
- 7.Basso C, Corrado D, Thiene G. Congenital coronary artery anomalies as an important cause of sudden death in the young. Cardiol Rev. 2001;9:31–317. doi: 10.1097/00045415-200111000-00005. [DOI] [PubMed] [Google Scholar]
- 8.Antonellis J, Rabaouni A, Kostopoulos K, et al. Single coronary artery from the right sinus of Valsalva, associated with absence of left anterior descending and an ostium secundum type atrial septal defect: A rare combination. A case report. Angiology. 1996;6:621–5. doi: 10.1177/000331979604700612. [DOI] [PubMed] [Google Scholar]
- 9.Prashanth P, Mukhaini M. Single right coronary artery continuing as left circumflex artery and hypoplastic left anterior descending artery: A rare coronary anomaly. J Invasive Cardiol. 2008;20:192–4. [PubMed] [Google Scholar]
- 10.Shirani J, Roberts WC. Solitary coronary ostium in the aorta in the absence of other major congenital cardiovascular anomalies. J Am Coll Cardiol. 1993;21:137–43. doi: 10.1016/0735-1097(93)90728-j. [DOI] [PubMed] [Google Scholar]