

Abstract
Introduction
Psychiatric co-morbidity is common in Crohn’s disease (CD) and ulcerative colitis (UC). IBD-related surgery or hospitalizations represent major events in the natural history of disease. Whether there is a difference in risk of psychiatric co-morbidity following surgery in CD and UC has not been examined previously.
Methods
We used a multi-institution cohort of IBD patients without a diagnosis code for anxiety or depression preceding their IBD-related surgery or hospitalization. Demographic, disease, and treatment related variables were retrieved. Multivariate logistic regression analysis was performed to individually identify risk factors for depression and anxiety.
Results
Our study included a total of 707 CD and 530 UC patients who underwent bowel resection surgery and did not have depression prior to surgery. The risk of depression 5 years after surgery was 16% and 11% in CD and UC respectively. We found no difference in the risk of depression following surgery in CD and UC patients (adjusted OR 1.11, 95%CI 0.84 – 1.47). Female gender, co-morbidity, immunosuppressant use, perianal disease, stoma surgery, and early surgery within 3 years of care predicted depression after CD-surgery; only female gender and co-morbidity predicted depression in UC. Only 12% of the CD cohort had ≥ 4 risk factors for depression, but among them nearly 44% were subsequently received a diagnosis code for depression.
Conclusion
IBD-related surgery or hospitalization is associated with a significant risk for depression and anxiety with a similar magnitude of risk in both diseases.
Keywords: Crohn’s disease, depression, anxiety, surgery, hospitalization
INTRODUCTION
Crohn’s disease (CD) and ulcerative colitis (UC) are chronic inflammatory diseases of the gastrointestinal tract affecting over 1.4 million Americans and accounting for an estimated $6 billion in direct healthcare costs1–3. They are associated with considerable indirect costs in lost productivity and days absent from work. Nearly two-thirds of patients with CD require at least one surgery during the course of their disease4, 5 and a significant proportion require hospitalization4. Up to a third of patients with UC may require surgical treatment of their disease, either for refractoriness to medical therapy or cancer6–8. While recurrence of disease is common after surgery for CD, colectomy is considered curative for UC though subsequent ileo-anal pouch related issues including single or recurrent episodes of pouchitis, or other pouch-related complications occur frequently9.
Psychiatric co-morbidity, in particular depression and anxiety, are common in patients with inflammatory bowel disease (IBD). Lifetime prevalence of major depression may approach 30% and anxiety may occur even more commonly10–13. While many cross-sectional or prospective studies have examined the frequency of occurrence of such co-morbidity14–16, fewer have examined risk factors12. Intuitively, disease severity and activity are important determinants of psychological effects of underlying bowel disease11, 17–19. Nevertheless, no prior studies have specifically addressed the frequency of occurrence of or risk factors for depression or anxiety following an IBD -related surgery or hospitalization which represent major events in the natural history of disease. Identifying such subgroups may identify a high-risk cohort of patients who could be targeted for screening for such co-morbidity, and early interventions to improve outcomes. Furthermore, no studies have specifically compared the occurrence of such psychiatric co-morbidity following surgery or hospitalization between CD and UC.
We performed this study with the aims of (1) examining the risk of depression and anxiety following an IBD-related surgery or hospitalization in a large multi-institution cohort; and (2) identifying the risk factors for such psychiatric co-morbidity following surgery or hospitalization in IBD patients; and (3) to compare the occurrence of such psychiatric co-morbidity in those with CD to UC patients undergoing interventions.
METHODS
Study Cohort
This study included a cohort of patients with CD or UC seen at two large tertiary referral hospitals (Massachusetts General Hospital, and Brigham and Women’s Hospital) in Boston serving over 4 million people. Prior work has described the creation of this cohort in detail20. In brief, we first extracted all patients with ≥ 1 International Classification of Diseases, 9th edition (ICD-9) code for CD (555) (n = 14,288) or UC (556) (n=14,355). Subsequently, using an algorithm developed using clinical, laboratory, endoscopy, and pathology data, refined using ICD-9 codes and free text natural language processing concepts, we identified a cohort of 5,506 CD and 5,522 UC patients with a positive predictive value of 97%, with validation of the algorithm through additional chart review by a board certified gastroenterologist20.
Variables
Information was obtained on age, age at the time of the first diagnosis code of CD or UC, gender, and modified Charlson co-morbidity index21 (excluding variables related to anxiety, depression) using ICD-9 codes. We identified the cohort of patients who underwent a bowel resection through the use of ICD-9 codes for abdominal surgery (Supplementary Table 1), and extracted the date of the occurrence of such procedures. Information was also obtained on disease-related complications including fistulizing or stricturing disease, and perianal disease for CD patients using ICD-9 codes (Supplementary Table 1). Use of medications including immunomodulators (azathioprine, 6-mercaptopurine, methotrexate), anti-tumor necrosis factor α (anti-TNF) therapies (infliximab, adalimumab), and corticosteroids (prednisone, budesonide) was ascertained as codified data using the electronic prescription function of our electronic medical record (EMR). IBD-related hospitalizations were identified as those with a primary diagnosis of CD or UC upon discharge from the hospital. We also identified patients who had undergone at least one stoma surgery (ICD-9 46.1, 46.2), and those who had undergone more than 1 surgery. To adjust for intensity of healthcare utilization, we included a variable - ‘number of facts’ - which included total number of distinct medical encounters including office visits, laboratory tests, radiologic studies, and inpatient or outpatient procedures. This, divided by duration of follow-up, yielded ‘fact density’ which was a measure of healthcare utilization per unit time of follow-up.
Outcomes
Our primary outcome of the study was the development of anxiety and depression defined as in previous studies using ICD-9 codes for depressive disorders (296.2, 296.3, 298.0, 311) or generalized anxiety (293.84, 300.0, 313.0)13, 22. To validate the accuracy of the ICD-9 codes for depression and anxiety we selected a random subset of 100 patients from both hospitals with each of these codes, reviewed their medical records and found a positive predictive value for a diagnosis of depression or anxiety to be 92% and 90% respectively. The predictive value was similar from both major hospitals (MGH and BWH). Patients who had a diagnosis code for depression or anxiety prior to or on their first date of surgery, or within 30 days after the date of surgery were excluded from this study to reduce likelihood of identifying prevalent cases (Figure 1). Similarly, in the analysis of hospitalizations, those with psychiatric co-morbidity (major depression or anxiety) at the time of or prior to an IBD-related hospitalization, or within 30 days of such a hospitalization were excluded.
Figure 1.
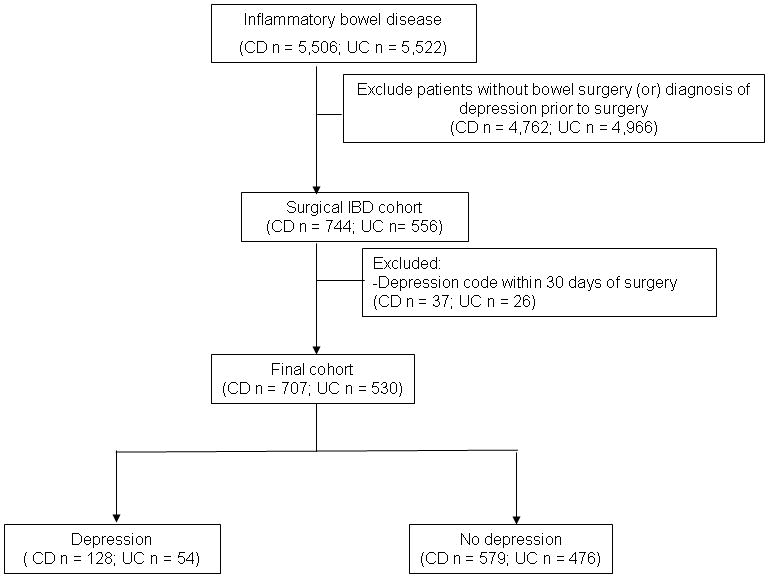
Flowchart demonstrating development of Crohn’s disease and ulcerative colitis cohorts
Statistical Analysis
All data was analyzed using Stata 11.0 (StataCorp, College Station, TX). Continuous variables were summarized using means and standard deviations and compared using t-tests. Categorical variables were expressed as proportions and compared using the chi-square test. Multivariate logistic regression analysis adjusting for potential confounders formed our main analysis examining predictors of depression or anxiety following surgery or hospitalization. Variables were selected for entry into the multivariate model based on significance at p < 0.1 on univariate analysis. The multivariate analysis was carried out using the forward stepwise procedure, retaining variables with p < 0.05. To account for secular trends in coding, year of surgery was included as a separate variable in all our multivariate models. We examined the occurrence of such psychiatric co-morbidity in the entire CD/UC cohort as well as each disease subgroup individually, comparing the rates across CD and UC. The predictors of depression and anxiety were also examined in the overall cohort as well as CD and UC separately. We performed sensitivity analyses to examine if having the diagnosis code for post-surgery depression or anxiety was a reflection of frequency of healthcare utilization by adjusting for fact density as described above, and for frequency of outpatient visits. The study was approved by the Institutional Review Board of Partners Healthcare.
RESULTS
Study Population
There were a total of 744 CD and 556 UC patients in our cohort who underwent ≥ 1 bowel resection surgery and did not have a diagnosis of depression prior to surgery. Among these, 63 had their first diagnosis code for depression within 30 days of the surgery (median 1 day) and were excluded resulting in 707 CD and 530 UC patients who were included in the analysis of post-surgery depression (Figure 1). The mean age of the cohort was 48 years with a mean age at surgery of 42 years. Just under half the cohort were women (47%). The cohort for analysis of anxiety following an IBD-related surgery comprised 1,183 patients.
Risk of Depression and Anxiety following IBD-related surgery or hospitalization
A total of 128 CD patients subsequently were given a diagnosis code for depression at a median of 2.2 years. Among those who required surgery, the risk of depression at 1, 2, and 5 years after surgery was 6, 8, and 16% (Figure 2). Similarly, 54 UC patients were given a diagnosis of depression at a median of 2.5 years. Interestingly, the risk of depression at 1, 2, and 5 years after surgery for UC was similar to the CD cohort at 5, 7 and 11% respectively (Figure 2). The crude overall frequency of depression was higher than we found for those undergoing surgery for diverticulitis (9%) or inguinal hernia (7%, p < 0.05). On multivariate logistic regression, adjusting for age, gender, co-morbidity, there was no difference in the risk of depression among post-surgery CD and UC patients (adjusted odds ratio (OR) 1.11, 95% confidence interval (CI) 0.84 – 1.47) suggesting a similar risk of post-surgery depression in both diseases. Among the entire CD cohort, 4,762 patients never required surgery. Compared to such patients, we observed a significantly elevated risk of depression in patients who required surgery (adjusted OR 1.34, 95% CI 1.01 – 1.77). Compared to UC patients who never required surgery (n = 4,928), those who did undergo surgery did not demonstrate this increase in risk for depression following surgery (OR 1.21, 95% CI 0.93 – 1.58).
Figure 2.
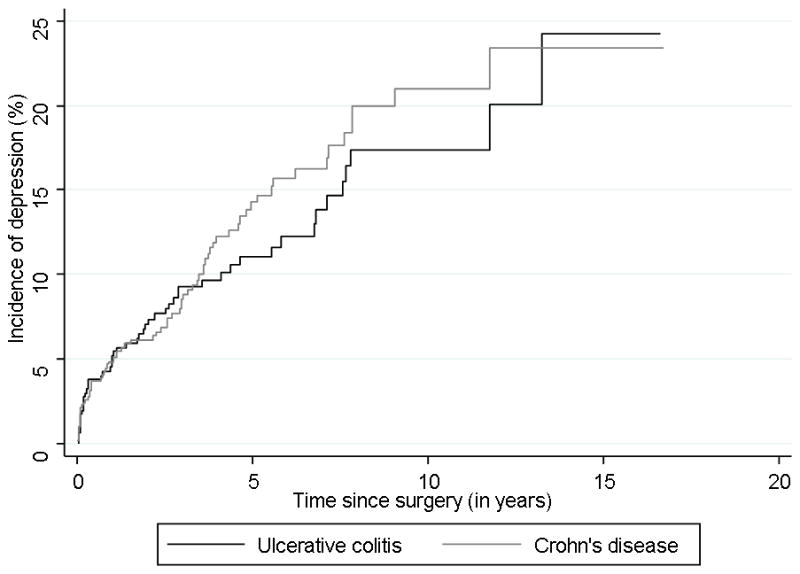
Risk of depression following IBD-related surgery in Crohn’s disease and ulcerative colitis
The risk of anxiety following IBD-related surgery at 1, 2, and 5 years was 7%, 9%, and 14% in CD patients and 7%, 10% and 12% in UC patients. There was no difference in the likelihood of anxiety based on IBD type (Odds ratio for CD vs. UC 1.09, 95% CI 0.82 – 1.44). Unlike what we identified for depression, the likelihood of anxiety following an IBD-related surgery was only mildly elevated compared to those who never underwent surgery for either CD (OR 1.20, 95% CI 0.93 – 1.55) or UC (OR 1.26, 95% CI 0.96 – 1.65).
A total of 2,062 CD patients and 1,345 UC patients required at least one IBD-related hospitalization, among who 33% and 41% subsequently required surgery. An IBD-related hospitalization itself was associated with a significant risk of depression. Even excluding those who subsequently underwent surgery, the risk of depression 5 years after a CD-related hospitalization was 17% with a corresponding risk of anxiety of 12%. This was nearly two-fold the risk of depression in those who never required hospitalization (OR 1.91, 95% CI 1.60 – 2.77). Similarly for UC, a disease related hospitalization was associated with an increase in risk for depression (OR 1.28, 95% CI 1.06 – 1.54) and anxiety (OR 1.32, 95% CI 1.09 – 1.59) compared to those who were never hospitalized.
Predictors of Depression and Anxiety following IBD-related surgery
Table 1 presents the characteristics of the patients, stratified by disease type and depression status. Both UC and CD patients who developed depression following surgery were more likely to be female and have greater co-morbidity. However, there were also differences between the two diseases. In CD, depressed patients were also more likely to be younger than 35 years at the time of surgery, or had surgery within 3 years of first diagnosis code for CD. The only disease phenotype associated with depression was the presence of perianal disease which was nearly twice as common in those with depression as those without. Those who developed depression were significant more likely to have required a stoma than those without (27% vs. 15%). The risk of depression 5 years after stoma surgery was 31% compared to 19% in those who never underwent stoma surgery (Figure 3). In UC, early surgery within 3 years was associated with an increased risk for depression similar to that seen for CD. However, there was no difference by age at surgery. Interestingly, there was also difference in risk of depression by requirement of a stoma in UC patients, likely due to the high frequency of requiring a stoma (temporary or permanent) as part of a two- or three-stage total colectomy with ileo-anal pouch reconstruction.
Table 1.
Characteristics of the Study Cohort of patients with Crohn’s disease and Ulcerative colitis undergoing surgery
| Crohn’s Disease | Ulcerative colitis | |||
|---|---|---|---|---|
| Characteristic | No Depression (n = 574) % | Depression (n=128) % | No Depression (n = 476) | Depression (n = 54) |
| Age in years [mean (SD)] | 48 (17) | 51 (17) * | 47 (19) | 49 (18) |
| Age at first diagnosis code for IBD [mean (SD)] | 39 (17) | 41 (19) | 39 (18) | 39 (17_ |
| Female | 49 | 63* | 41 | 68* |
| Charlson score ≥ 3 | 23 | 58* | 23 | 54* |
| Disease complications | ||||
| Fistulizing disease | 44 | 38 | ||
| Stricturing disease | 68 | 70 | ||
| Perianal involvement | 17 | 30* | ||
| Surgery characteristics | ||||
| Early Surgery (< 3 years) | 32 | 49* | 24 | 39* |
| Surgery at Age < 35 years | 59 | 67* | 58 | 58 |
| Stoma Surgery | 14 | 27* | 62 | 55 |
| ≥ 2 surgeries | 15 | 27* | 22 | 29 |
| Ever medication use | ||||
| Aminosalicylates | 44 | 51 | 42 | 54* |
| Steroids | 55 | 70* | 66 | 75 |
| Immunomodulators | 41 | 52* | 25 | 32 |
| Anti-TNF biologic use | 23 | 34* | 15 | 24* |
p < 0.05
SD – standard deviation, anti-TNF – anti tumor-necrosis factor α, IBD – inflammatory bowel diseases
Immunomodulators include azathioprine, 6-mercaptopurine, or methotrexate; Anti-TNF agents include infliximab or adalimumab
Figure 3.
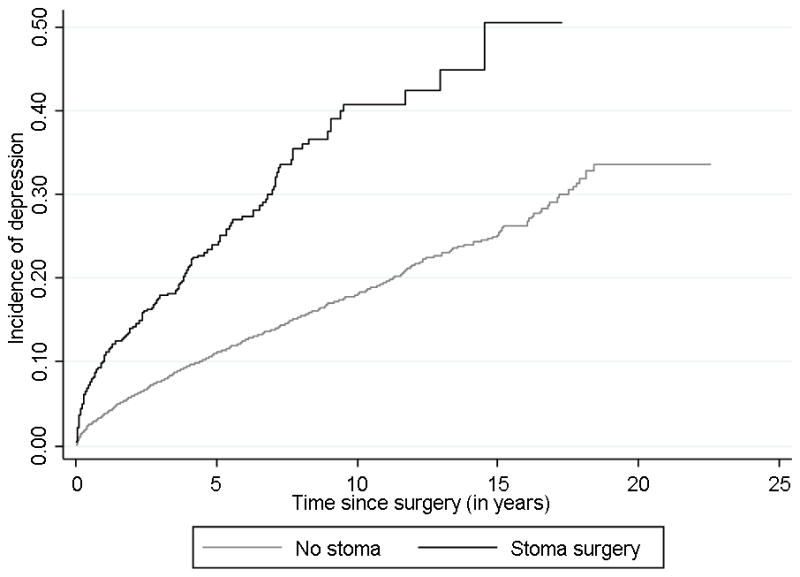
Risk of depression following surgery in Crohn’s disease, stratified by requirement for a stoma
Since there were differences in risk factors, we performed separate stepwise multivariate logistic regression analyses for both diseases. In CD, the strongest predictor was non-IBD medical co-morbidity (Table 2). Having a stoma was the next strongest predictor with an OR of 1.90 (95% CI 1.15 – 3.13). Female gender, perianal disease, need for immunomodulator therapy, and early surgery within 3 years also moderately increased risk of depression following surgery. The risk of depression increased with the number of risk factors; only 8% of those with 0 or 1 risk factor subsequently developed depression compared to 20% of those with 2 or 3 risk factors, and 44% of those with 4 or more risk factors (Figure 4). However, the distribution of risk factors was also not uniform between the risk strata; only 2% of those in the lowest risk category had a stoma surgery compared to 46% of the highest risk stratum. On the other hand, for UC, only female gender (OR 2.92) and Charlson score ≥ 3 (OR 3.73) were associated with increased risk of depression (Table 2). Multivariate analysis for predictors of anxiety revealed a significant overlap with the risk factors for depression with similar effect sizes for nearly all parameters for both CD and UC (Table 3).
Table 2.
Multivariate analysis of risk factors for depression following surgery in Crohn’s disease and ulcerative colitis
| Crohn’s disease | ||
|---|---|---|
| Characteristic | Adjusted Odds Ratio | 95% confidence interval |
| Female gender | 1.77 | 1.16 – 2.71 |
| Charlson score ≥ 3 | 4.31 | 2.82 – 6.57 |
| Surgery within 3 years | 1.54 | 1.01 – 2.37 |
| Immunomodulator use | 1.56 | 1.03 – 2.38 |
| Stoma surgery | 1.90 | 1.15 – 3.13 |
| Perianal disease | 1.64 | 1.01 – 2.69 |
| Ulcerative colitis | ||
| Female gender | 2.92 | 1.80 – 4.76 |
| Charlson score ≥ 3 | 3.73 | 2.33 – 5.97 |
All risk factors retained in the multivariate analysis by stepwise regression are described in the table.
Figure 4. Frequency of depression following surgery in Crohn’s disease, stratified by the number of risk factors.
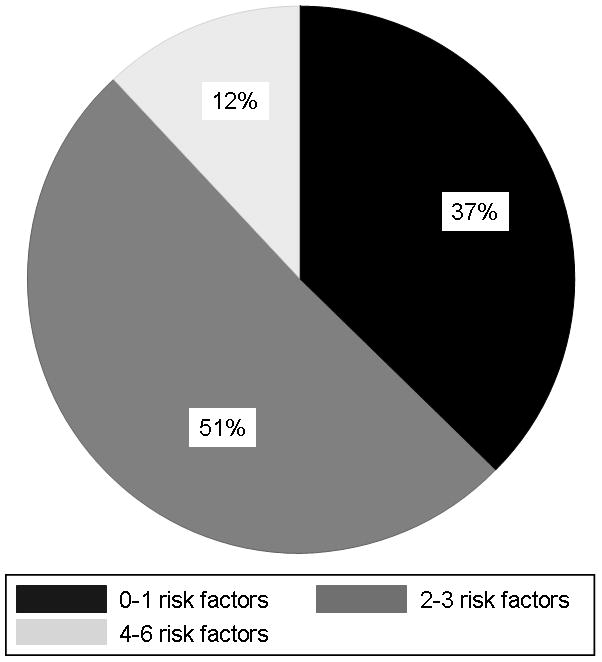
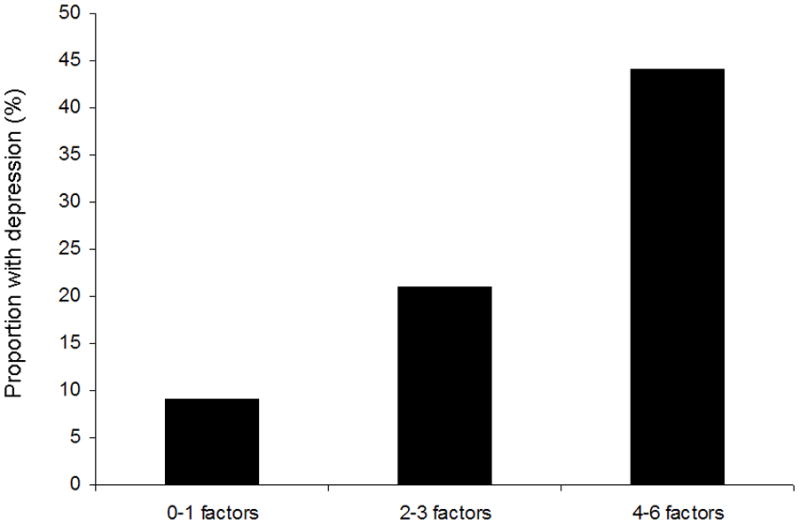
(a) Distribution of risk factors for depression following CD-related surgery
(b) Frequency of depression stratified by presence of risk factors
Table 3.
Multivariate analysis of risk factors for anxiety following surgery in Crohn’s disease and ulcerative colitis
| Crohn’s disease | ||
|---|---|---|
| Characteristic | Adjusted Odds Ratio | 95% confidence interval |
| Female gender | 2.07 | 1.35 – 3.19 |
| Charlson score ≥ 3 | 1.84 | 1.19 – 2.84 |
| Surgery within 3 years | 2.19 | 1.44 – 3.33 |
| Stoma surgery | 1.73 | 1.05 – 2.85 |
| ≥ 2 surgeries | 1.79 | 1.09 – 2.93 |
| Ulcerative colitis | ||
| Age (per 1 year) | 0.98 | 0.97 – 1.00 |
| Female gender | 1.84 | 1.18 – 2.87 |
| Charlson score ≥ 3 | 3.26 | 1.98 – 5.38 |
All risk factors retained in the multivariate analysis by stepwise regression are described in the table.
Sensitivity Analysis
We performed a variety of sensitivity analysis to examine the robustness of our findings. Primarily, to determine if the increased risk of anxiety or depression following surgery was solely a reflection of increased healthcare utilization (and consequently, increase in the number of diagnosis codes) in such patients, we adjusted for the number of outpatient gastroenterology office visit, all outpatient visits with a diagnosis of CD or UC, and number of inpatient hospitalizations, and found no attenuation of our effect sizes. Similarly, our OR estimates were rendered larger adjusting for density of healthcare utilization.
DISCUSSION
There is an increased risk of depression and anxiety in patients with CD or UC10–13. The extent to which this increased risk is determined by severity of disease is unclear. Furthermore, there have been no prior studies that have quantified the risk of such psychiatric co-morbidity after IBD-related surgery or hospitalization which represent major events in the natural history of IBD. Using a multi-institutional cohort, we demonstrate that even after excluding those who received a diagnosis of depression prior to surgery, CD and UC patients who underwent an IBD-related surgery had a 16% and 11% risk of receiving a diagnosis of depression at 5 years, with a similar substantial risk of anxiety. Furthermore, despite surgery for UC being considered curative, we observed a similar risk between both diseases. We also identified several sub-groups of patients at higher risk of such co-morbidity, which may facilitate targeted screening and early intervention.
Several studies have examined the co-occurrence of psychiatric co-morbidity in patients with IBD13–16, 23. However, there is limited literature examining risk factors for psychological distress in patients with IBD. Nahon et al. administered a questionnaire to 1,663 patients with IBD and identified 11% of patients to be depressed and 41% to be anxious12. On multivariate analysis, severity of disease defined as requiring two or more courses of steroids, hospitalization, need for immunosuppressive therapy or intestinal resection was an independent risk factor for anxiety but not depression. However, this broad definition of severe disease resulted in nearly 90% of their cohort irrespective of psychiatric co-morbidity being classified as having severe disease, limiting the utility of such composite definitions. Indeed when restricting their analysis to individual components of disease severity, they found that past history of surgery was associated with a lower risk of anxiety and had no effect on risk of depression. Our study differs from the prior studies in that we specifically focused on a relatively homogenous cohort of CD or UC patients who had all undergone surgery or required hospitalization. By specifically excluding those who received a diagnosis of depression or anxiety prior to surgery, we attempted to minimize the number of prevalent cases as well as the possibility of reverse causation or confounding where disease activity predicts both surgery as well as occurrence of psychiatric co-morbidity.
A key and interesting finding from our study is that the risk of depression or anxiety following IBD-related surgery or hospitalization was similar in CD and UC. While surgery for CD is usually not curative, is followed by nearly universal disease recurrence with only mild attenuation of this risk with existing medical therapies, a total colectomy for UC is considered curative. There are a few possible reasons for persistence of the risk for depression and anxiety in UC patients following surgery similar to that for CD. First, even after an ileal-pouch, patients can continue to be have frequency of bowel movements including need for nocturnal bowel movements which could affect health-related quality of life, which could in-turn lead to depressive symptoms24. Secondly, up to half of the patients may have at least one episode of pouchitis while one-quarter may have recurrent episodes9. Such fluctuations in disease activity could also influence risk of depression or anxiety. This is consistent with the findings from a small study by Hauser et al. that patients with an IPAA did not differ in their risk of depression compare to UC patients without IPAA but were more likely to be depressed than the general population25. Other studies have similarly shown that patients with an IPAA continue to have impairment in quality of life compared to the general population26, 27 though the literature in this area has yielded conflicting results28.
We also identified common and distinct risk factors for depression following-IBD related surgery. Female gender was common across both diseases, consistent with prior studies examining health-related quality of life and psychiatric co-morbidity in IBD29–32. In a prospective study, Beaugerie et al. demonstrated that perianal disease was associated with a disabling course of CD33. A high proportion of patients with perianal CD have depressive symptoms34, and demonstrate long-term impairment of quality of life35. In addition, early surgery defined as undergoing a resection within 3 years of first CD diagnosis code in our health system also increased risk of depression post-operatively, consistent with the hypothesis associating aggressive disease behavior with psychological co-morbidity.,
Requiring an ostomy bag is one of the highest rated concerns among CD and UC patients36–38. In the present study, among CD patients, the risk of depression or anxiety was influenced quite strongly by having an ostomy which was the strongest risk factor after non-IBD co-morbidity. However, we found no such effect on UC patients which could be due to the high frequency of stoma procedures (as part of two- or three-stage colectomy surgeries in UC). The literature on the effect of stoma on risk of subsequent psychological co-morbidity has been inconsistent. After surgery for colorectal cancer, having a stoma is associated with worse body image39 and increases risk for anxiety or depression. However, in CD, where surgery may not represent a permanent cure from disease, and patients may continue to experience symptoms related to ongoing bowel or perianal disease, having a stoma has not been consistently associated with worse quality of life when compared to other CD controls35, 40. However, no prior studies have specifically examined the effect of stoma or multiple surgeries on post-operative anxiety or depression in an IBD cohort. In addition, the association with non-IBD co-morbidity suggests that such patients may be more susceptible to functional impairment and consequences of IBD-related surgery or hospitalization. The association between co-morbidity and increased healthcare utilization post-operatively has also been demonstrated in other cohorts41, 42, suggesting management of IBD patients with such co-morbidity, particularly in the setting of severe disease requiring surgery remains challenging.
Finally, another important finding from out study was that an IBD-related hospitalization even in the absence of subsequent surgery was associated with a significant risk for depression and anxiety. This demonstrates that in addition to their effect on healthcare costs, hospitalizations remain an important event in disease course of both CD and UC. As demonstrated by prior studies, those requiring hospitalization form a high risk cohort for subsequent surgery4, 43, 44, but even in the absence of such an eventuality, remain at risk for psychological co-morbidity associated with their disease. Consideration must be given for routine screening for depression and anxiety in this cohort as well.
Our study has several implications. To our knowledge, ours is the first study specifically examining the overall occurrence of depression and anxiety following IBD-related surgery or hospitalization, as well the comparative incidence between both diseases. Our examination of predictors of depression or anxiety suggest that there are strong demographic, disease, or surgery related characteristics that place a patient at a substantially elevated risk of psychological co-morbidity even among a cohort with relative homogeneity in their disease severity. We suggest the need to routinely screen such patients for depression and anxiety as part of standard care in the immediate and late post-operative period, as well as after an IBD-related hospitalization. Given the significant morbidity and healthcare utilization associated with psychiatric co-morbidity, there is need for continued research into effective interventions to identify and treat such patients, and whether preventive interventions may be warranted in high-risk patients.
There are a few limitations to our study. First, we relied on administrative coding to identify the presence and date of diagnosis of depression or anxiety in the postoperative setting as well as predictors which may result in misclassification. However, misclassification is unlikely to be differential between the various risk factors, and we performed a validation of the ICD-9 codes used. Recognizing the increased risk for depression and anxiety, future prospective studies are necessary with structured evaluation of mood and other psychiatric co-morbidity following IBD-related surgery or hospitalization. Second, we did not have accurate and comprehensive information on the use of antidepressant or anti-anxiety medications in our cohort. Third, owing to the referral nature of our institutions, further studies examining our hypothesis in a population based cohort will help confirm the generalizability of our results. Given the linear increase in depression and anxiety diagnosis over time, it is unlikely that our findings are solely due to increased frequency of healthcare utilization and thus, the number of diagnosis codes, in the immediate perioperative period. We also did not have information on smoking status which could influence risk of surgery in CD.
In conclusion, we demonstrate that IBD-related surgery or hospitalization is associated with a significant risk for depression and anxiety in both CD and UC with similar magnitudes of risk across both diseases. Female gender and non-IBD co-morbidity were common risk factors for depression or anxiety in both CD and UC. Requirement for a stoma was a strong risk factor for depression following surgery in CD-but not UC patients. Continued screening for psychiatric co-morbidity following IBD-related surgery or hospitalization should be part of comprehensive IBD care, particularly for high-risk patients. There is need for ongoing research into effective modalities to improve health-related quality of life and other outcomes in such patients.
Supplementary Material
Supplementary Table 1: List of International Classification of Diseases, 9th Edition (ICD-9) codes used in defining variables of interest
What is known?
Anxiety and depression are common in patients with Crohn’s disease and ulcerative colitis
Severity of disease may be associated with risk of psychiatric co-morbidity
The incidence of depression or anxiety after an IBD-related surgery or hospitalization, or the risk factors for such psychiatric co-morbidity is unknown.
What is new here?
Approximately 16% of CD patients and 11% of UC patients develop depression at 5 years after undergoing IBD-related surgery with a similar risk between CD and UC.
Female gender, younger age at surgery, undergoing surgery soon after a diagnosis of CD, or requirement for a stoma were associated with increased risk of depression in CD while only female gender and co-morbidity predicted depression in UC.
Acknowledgments
Sources of Funding: The study was supported by NIH U54-LM008748. A.N.A is supported by funding from the American Gastroenterological Association and from the US National Institutes of Health (K23 DK097142). K.P.L. is supported by NIH K08 AR060257 and the Katherine Swan Ginsburg Fund. R.M.P. is supported by grants from the US National Institutes of Health (NIH) (R01-AR056768, U01-GM092691 and R01-AR059648) and holds a Career Award for Medical Scientists from the Burroughs Wellcome Fund. E.W.K is supported by grants from the NIH (K24 AR052403, P60 AR047782, R01 AR049880).
References
- 1.Kappelman MD, Rifas-Shiman SL, Porter CQ, Ollendorf DA, Sandler RS, Galanko JA, Finkelstein JA. Direct health care costs of Crohn’s disease and ulcerative colitis in US children and adults. Gastroenterology. 2008;135:1907–13. doi: 10.1053/j.gastro.2008.09.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Abraham C, Cho JH. Inflammatory bowel disease. N Engl J Med. 2009;361:2066–78. doi: 10.1056/NEJMra0804647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of inflammatory bowel disease. Nature. 2011;474:307–17. doi: 10.1038/nature10209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bernstein CN, Loftus EV, Jr, Ng SC, Lakatos PL, Moum B. Hospitalisations and surgery in Crohn’s disease. Gut. 2012;61:622–9. doi: 10.1136/gutjnl-2011-301397. [DOI] [PubMed] [Google Scholar]
- 5.Cosnes J, Gower-Rousseau C, Seksik P, Cortot A. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology. 2011;140:1785–94. doi: 10.1053/j.gastro.2011.01.055. [DOI] [PubMed] [Google Scholar]
- 6.Lakatos L, Kiss LS, David G, Pandur T, Erdelyi Z, Mester G, Balogh M, Szipocs I, Molnar C, Komaromi E, Lakatos PL. Incidence, disease phenotype at diagnosis, and early disease course in inflammatory bowel diseases in Western Hungary, 2002–2006. Inflamm Bowel Dis. 2011;17:2558–65. doi: 10.1002/ibd.21607. [DOI] [PubMed] [Google Scholar]
- 7.Solberg IC, Lygren I, Jahnsen J, Aadland E, Hoie O, Cvancarova M, Bernklev T, Henriksen M, Sauar J, Vatn MH, Moum B. Clinical course during the first 10 years of ulcerative colitis: results from a population-based inception cohort (IBSEN Study) Scand J Gastroenterol. 2009;44:431–40. doi: 10.1080/00365520802600961. [DOI] [PubMed] [Google Scholar]
- 8.Targownik LE, Singh H, Nugent Z, Bernstein CN. The epidemiology of colectomy in ulcerative colitis: results from a population-based cohort. Am J Gastroenterol. 2012;107:1228–35. doi: 10.1038/ajg.2012.127. [DOI] [PubMed] [Google Scholar]
- 9.Li Y, Shen B. Evaluating pouch problems. Gastroenterol Clin North Am. 2012;41:355–78. doi: 10.1016/j.gtc.2012.01.013. [DOI] [PubMed] [Google Scholar]
- 10.Graff LA, Walker JR, Bernstein CN. Depression and anxiety in inflammatory bowel disease: a review of comorbidity and management. Inflamm Bowel Dis. 2009;15:1105–18. doi: 10.1002/ibd.20873. [DOI] [PubMed] [Google Scholar]
- 11.Graff LA, Walker JR, Lix L, Clara I, Rawsthorne P, Rogala L, Miller N, Jakul L, McPhail C, Ediger J, Bernstein CN. The relationship of inflammatory bowel disease type and activity to psychological functioning and quality of life. Clin Gastroenterol Hepatol. 2006;4:1491–1501. doi: 10.1016/j.cgh.2006.09.027. [DOI] [PubMed] [Google Scholar]
- 12.Nahon S, Lahmek P, Durance C, Olympie A, Lesgourgues B, Colombel JF, Gendre JP. Risk factors of anxiety and depression in inflammatory bowel disease. Inflamm Bowel Dis. 2012 doi: 10.1002/ibd.22888. [DOI] [PubMed] [Google Scholar]
- 13.Loftus EV, Jr, Guerin A, Yu AP, Wu EQ, Yang M, Chao J, Mulani PM. Increased risks of developing anxiety and depression in young patients with Crohn’s disease. Am J Gastroenterol. 2011;106:1670–7. doi: 10.1038/ajg.2011.142. [DOI] [PubMed] [Google Scholar]
- 14.Fuller-Thomson E, Sulman J. Depression and inflammatory bowel disease: findings from two nationally representative Canadian surveys. Inflamm Bowel Dis. 2006;12:697–707. doi: 10.1097/00054725-200608000-00005. [DOI] [PubMed] [Google Scholar]
- 15.Kurina LM, Goldacre MJ, Yeates D, Gill LE. Depression and anxiety in people with inflammatory bowel disease. J Epidemiol Community Health. 2001;55:716–20. doi: 10.1136/jech.55.10.716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Walker JR, Ediger JP, Graff LA, Greenfeld JM, Clara I, Lix L, Rawsthorne P, Miller N, Rogala L, McPhail CM, Bernstein CN. The Manitoba IBD cohort study: a population-based study of the prevalence of lifetime and 12-month anxiety and mood disorders. Am J Gastroenterol. 2008;103:1989–97. doi: 10.1111/j.1572-0241.2008.01980.x. [DOI] [PubMed] [Google Scholar]
- 17.Lerebours E, Gower-Rousseau C, Merle V, Brazier F, Debeugny S, Marti R, Salomez JL, Hellot MF, Dupas JL, Colombel JF, Cortot A, Benichou J. Stressful life events as a risk factor for inflammatory bowel disease onset: A population-based case-control study. Am J Gastroenterol. 2007;102:122–31. doi: 10.1111/j.1572-0241.2006.00931.x. [DOI] [PubMed] [Google Scholar]
- 18.Levenstein S, Prantera C, Varvo V, Scribano ML, Berto E, Andreoli A, Luzi C. Psychological stress and disease activity in ulcerative colitis: a multidimensional cross-sectional study. Am J Gastroenterol. 1994;89:1219–25. [PubMed] [Google Scholar]
- 19.Maunder RG. Evidence that stress contributes to inflammatory bowel disease: evaluation, synthesis, and future directions. Inflamm Bowel Dis. 2005;11:600–8. doi: 10.1097/01.mib.0000161919.42878.a0. [DOI] [PubMed] [Google Scholar]
- 20.Ananthakrishnan AN, Cai T, Savova G, Chen P, Guzman Perez R, Gainer VS, Murphy SN, Szolovits P, Xia Z, Shaw S, Churchill S, Karlson EW, Kohane I, Plenge RM, Liao KP. Improving Case Definition of Crohn’s Disease and Ulcerative Colitis in Electronic Medical Records Using Natural Language Processing: A Novel Informatics Approach. Inflamm Bowel Dis. 2012 doi: 10.1097/MIB.0b013e31828133fd. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83. doi: 10.1016/0021-9681(87)90171-8. [DOI] [PubMed] [Google Scholar]
- 22.Castro VM, Gallagher PJ, Clements CC, Murphy SN, Gainer VS, Fava M, Weilburg JB, Churchill SE, Kohane IS, Iosifescu DV, Smoller JW, Perlis RH. Incident user cohort study of risk for gastrointestinal bleed and stroke in individuals with major depressive disorder treated with antidepressants. BMJ Open. 2012;2:e000544. doi: 10.1136/bmjopen-2011-000544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wells KB, Golding JM, Burnam MA. Psychiatric disorder in a sample of the general population with and without chronic medical conditions. Am J Psychiatry. 1988;145:976–81. doi: 10.1176/ajp.145.8.976. [DOI] [PubMed] [Google Scholar]
- 24.Ko CY, Rusin LC, Schoetz DJ, Jr, Moreau L, Coller JC, Murray JJ, Roberts PL, Marcello PW. Long-term outcomes of the ileal pouch anal anastomosis: the association of bowel function and quality of life 5 years after surgery. J Surg Res. 2001;98:102–7. doi: 10.1006/jsre.2001.6171. [DOI] [PubMed] [Google Scholar]
- 25.Hauser W, Janke KH, Stallmach A. Mental disorder and psychologic distress in patients with ulcerative colitis after ileal pouch-anal anastomosis. Dis Colon Rectum. 2005;48:952–62. doi: 10.1007/s10350-004-0888-1. [DOI] [PubMed] [Google Scholar]
- 26.Andersson T, Lunde OC, Johnson E, Moum T, Nesbakken A. Long-term functional outcome and quality of life after restorative proctocolectomy with ileo-anal anastomosis for colitis. Colorectal Dis. 2011;13:431–7. doi: 10.1111/j.1463-1318.2009.02163.x. [DOI] [PubMed] [Google Scholar]
- 27.Hauser W, Dietz N, Steder-Neukamm U, Janke KH, Stallmach A. Biopsychosocial determinants of health-related quality of life after ileal pouch anal anastomosis for ulcerative colitis. Inflamm Bowel Dis. 2004;10:399–407. doi: 10.1097/00054725-200407000-00011. [DOI] [PubMed] [Google Scholar]
- 28.Robb B, Pritts T, Gang G, Warner B, Seeskin C, Stoops M, James L, Rafferty J, Azizkhan R, Martin L, Nussbaum M. Quality of life in patients undergoing ileal pouch-anal anastomosis at the University of Cincinnati. Am J Surg. 2002;183:353–60. doi: 10.1016/s0002-9610(02)00804-8. [DOI] [PubMed] [Google Scholar]
- 29.Hauser G, Tkalcic M, Stimac D, Milic S, Sincic BM. Gender related differences in quality of life and affective status in patients with inflammatory bowel disease. Coll Antropol. 2011;35 (Suppl 2):203–7. [PubMed] [Google Scholar]
- 30.Stjernman H, Tysk C, Almer S, Strom M, Hjortswang H. Unfavourable outcome for women in a study of health-related quality of life, social factors and work disability in Crohn’s disease. Eur J Gastroenterol Hepatol. 2011;23:671–9. doi: 10.1097/MEG.0b013e328346f622. [DOI] [PubMed] [Google Scholar]
- 31.Casellas F, Arenas JI, Baudet JS, Fabregas S, Garcia N, Gelabert J, Medina C, Ochotorena I, Papo M, Rodrigo L, Malagelada JR. Impairment of health-related quality of life in patients with inflammatory bowel disease: a Spanish multicenter study. Inflamm Bowel Dis. 2005;11:488–96. doi: 10.1097/01.mib.0000159661.55028.56. [DOI] [PubMed] [Google Scholar]
- 32.Saibeni S, Cortinovis I, Beretta L, Tatarella M, Ferraris L, Rondonotti E, Corbellini A, Bortoli A, Colombo E, Alvisi C, Imperiali G, de Franchis R. Gender and disease activity influence health-related quality of life in inflammatory bowel diseases. Hepatogastroenterology. 2005;52:509–15. [PubMed] [Google Scholar]
- 33.Beaugerie L, Seksik P, Nion-Larmurier I, Gendre JP, Cosnes J. Predictors of Crohn’s disease. Gastroenterology. 2006;130:650–6. doi: 10.1053/j.gastro.2005.12.019. [DOI] [PubMed] [Google Scholar]
- 34.Mahadev S, Young JM, Selby W, Solomon MJ. Self-reported depressive symptoms and suicidal feelings in perianal Crohn’s disease. Colorectal Dis. 2012;14:331–5. doi: 10.1111/j.1463-1318.2011.02613.x. [DOI] [PubMed] [Google Scholar]
- 35.Kasparek MS, Glatzle J, Temeltcheva T, Mueller MH, Koenigsrainer A, Kreis ME. Long-term quality of life in patients with Crohn’s disease and perianal fistulas: influence of fecal diversion. Dis Colon Rectum. 2007;50:2067–74. doi: 10.1007/s10350-007-9006-5. [DOI] [PubMed] [Google Scholar]
- 36.Drossman DA, Leserman J, Li ZM, Mitchell CM, Zagami EA, Patrick DL. The rating form of IBD patient concerns: a new measure of health status. Psychosom Med. 1991;53:701–12. doi: 10.1097/00006842-199111000-00010. [DOI] [PubMed] [Google Scholar]
- 37.Jelsness-Jorgensen LP, Moum B, Bernklev T. Worries and Concerns among Inflammatory Bowel Disease Patients Followed Prospectively over One Year. Gastroenterol Res Pract. 2011;2011:492034. doi: 10.1155/2011/492034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Moser G, Tillinger W, Sachs G, Genser D, Maier-Dobersberger T, Spiess K, Wyatt J, Vogelsang H, Lochs H, Gangl A. Disease-related worries and concerns: a study on out-patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol. 1995;7:853–8. [PubMed] [Google Scholar]
- 39.Sharpe L, Patel D, Clarke S. The relationship between body image disturbance and distress in colorectal cancer patients with and without stomas. J Psychosom Res. 2011;70:395–402. doi: 10.1016/j.jpsychores.2010.11.003. [DOI] [PubMed] [Google Scholar]
- 40.Lask B, Jenkins J, Nabarro L, Booth I. Psychosocial sequelae of stoma surgery for inflammatory bowel disease in childhood. Gut. 1987;28:1257–60. doi: 10.1136/gut.28.10.1257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Bokemeyer B, Hardt J, Huppe D, Prenzler A, Conrad S, Duffelmeyer M, Hartmann P, Hoffstadt M, Klugmann T, Schmidt C, Weismuller J, Mittendorf T, Raspe H. J Crohns Colitis. 2012. Clinical status, psychosocial impairments, medical treatment and health care costs for patients with inflammatory bowel disease (IBD) in Germany: An online IBD registry. [DOI] [PubMed] [Google Scholar]
- 42.Nguyen GC, Saibil F, Steinhart AH, Li Q, Tinmouth JM. Postoperative Health-Care Utilization in Crohn’s Disease: The Impact of Specialist Care. Am J Gastroenterol. 2012 doi: 10.1038/ajg.2012.235. [DOI] [PubMed] [Google Scholar]
- 43.Ananthakrishnan AN, Issa M, Beaulieu DB, Skaros S, Knox JF, Lemke K, Emmons J, Lundeen SH, Otterson MF, Binion DG. History of medical hospitalization predicts future need for colectomy in patients with ulcerative colitis. Inflamm Bowel Dis. 2009;15:176–81. doi: 10.1002/ibd.20639. [DOI] [PubMed] [Google Scholar]
- 44.Dinesen LC, Walsh AJ, Protic MN, Heap G, Cummings F, Warren BF, George B, Mortensen NJ, Travis SP. The pattern and outcome of acute severe colitis. J Crohns Colitis. 2010;4:431–7. doi: 10.1016/j.crohns.2010.02.001. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Table 1: List of International Classification of Diseases, 9th Edition (ICD-9) codes used in defining variables of interest