

Abstract
Studies have shown that false memories can be implanted via innocuous suggestions, and that these memories can play a role in shaping people’s subsequent attitudes and preferences. The current study explored whether participants (N=147) who received a false suggestion that they had become ill drinking a particular type of alcohol would increase their confidence that the event had occurred, and whether their new-found belief would subsequently affect their alcohol preferences. Results indicated that participants who received a suggestion that they had gotten sick drinking rum or vodka before the age of 16 reported increased confidence that the suggested experience had occurred. Moreover, participants who received a false alcohol suggestion also showed a strong trend to report diminished preference for the specified type of alcohol after the false suggestion. Implantation of a false memory related to one’s past drinking experiences may influence current drink preferences and could be an important avenue for further exploration in the development of alcohol interventions.
1. Introduction
For generations, alcohol overindulgences have often resulted in people making oaths of “never again”. In some cases, the oath is kept because of the strong willpower of the regretful drinker. In other cases, avoidance of particular types of alcohol has more to do with a physical aversion brought on by the experience of getting sick after imbibing. Taste aversion research has documented this finding scientifically (see Riley & Freeman, 2004a, 2004b, for an overview). Alcohol researchers, over the years, have capitalized on this classical conditioning learning theory to develop therapies that use aversion to help problem drinkers avoid alcohol. The goal of alcohol aversion therapy is to reduce the undesirable behavior—drinking—through negative pairings of an aversive stimulus with that behavior.
Historically, these types of therapies have included: shock therapy—where an electric shock is used as a negative stimulus pairing when the individual is engaging in thoughts, urges or behaviors related to the substance they wish to avoid (Elkins, 1974, 1980; Maguire & Vallance, 1964); satiation—a technique primarily used with cigarette smokers whereby they must smoke a large number of cigarettes in a short period of time to induce nicotine toxicity (McRobbie & Hajek, 2007); and even chemical aversant pairings with the undesired behavior—administering an aversive smell or taste, or even an intravenous pharmacological agent to induce sickness (Howard, 1991). Ethical concerns, as well as a lack of controlled scientific studies in this area, have led to the demise of traditional aversion therapies amongst the scientific community (see Council on Scientific Affairs, 1987). However, despite this demise, it is important to note that some drug and alcohol treatment programs still regularly incorporate aversion therapy into their curriculum (see for example, http://schickshadel.reachlocal.com). Moreover, current acceptable psychopharmacological treatments for alcohol use disorders include administering inhibitory agents (i.e.,Disulfiram) that act by blocking the breakdown of acetaldehyde (the chemical agent that is believed to contribute to hangover symptoms). The interaction of Disulfiram with any amount of alcohol enhances unpleasant physical symptoms (i.e., throbbing headache, nausea, vomiting, weakness, etc.), such that the individual is presumably deterred from subsequent drinking.
One alternative approach to curbing alcohol use, which avoids the rather invasive and morally objectionable behavior modification techniques usually associated with aversion therapy, may be to take inspiration from the false memory literature. Over the past 20 years, the false memory literature has shown that it is possible to get people to imagine an event that supposedly happened in their past via an innocuous suggestion, and then later come to feel confident that such an event occurred (Garry, Manning, Loftus, & Sherman, 1996; Hyman, Husband, & Billings, 1995; Loftus & Pickrell, 1995). For instance, people have been led to believe that they spilled punch on the parents of the bride at a wedding (Hyman et al. 1995), drank a tastier juice than they actually did (Braun, 1999), took a hot air balloon ride (Wade, Garry, Read, & Lindsay, 2002), and even witnessed a demonic possession (Mazzoni, Loftus, & Kirsch, 2001).
Results from a handful of studies have shown that adopting a false memory as part of one’s personal autobiography can affect an individual’s current and future preferences related to that “memory.” For example, one study showed that people who were falsely led to believe that they got sick as a child on either hard-boiled eggs or dill pickles later indicated that they would be less likely to eat the suggested food when presented with the option of eating it (Bernstein, Laney, Morris, & Loftus, 2005). Similarly, another study showed that people who believed a false suggestion that they loved asparagus in their youth later expressed a willingness to pay more for this vegetable and eat it, as well as also being more likely to rate photographs of the newly loved vegetable as more appetizing, relative to their counterparts who did not receive such a suggestion (Laney, Morris, Bernstein, Wakefield & Loftus, 2008). More recently, researchers have begun asking whether these altered preferences can extend to behavior. Using a false memory implantation technique, several recent studies have shown that participants who received a false suggestion about a negative food experience like eating spoiled peach yogurt ate less of this food item during a subsequent, seemingly unrelated, free eating period, than participants who did not receive such a suggestion (see Geraerts, Bernstein, Merckelbach, Linders, Raemakers, & Loftus, 2008; Scoboria, Mazzoni, & Jarry, 2008;Scoboria, Mazzoni, Jarry, & Bernstein, 2012). Taken together, these findings demonstrate promise for other related behaviors that may carry greater health risks, such as alcohol consumption (see Bernstein, Pernat, & Loftus, 2011 for review).
To date, no previous studies that we are aware of have experimentally examined whether early alcohol related memories would be prone to memory manipulation2. There are reasons why we might not expect to see individuals adopting false alcohol memories as readily as other food-related memories. On the one hand, the cultural cache surrounding alcohol is such that people are more inclined to have strong associations or memories (both positive and negative) with alcohol than they may have with other foods, such as hard-boiled eggs or yogurt. For example, the alcohol expectancy literature tells us that virtually all people in our culture, regardless of whether they have ever consumed an alcoholic drink, hold strong and specific alcohol-related beliefs and expectancies (see Goldman, Del Boca & Darkes, 1999; Kirsch, 1999; Maisto, Carey, Carey, & Gordon, 2002; Vogel-Sprott, & Fillmore, 1999, for example). These expectancies and beliefs would undoubtedly influence how participants respond to an attempted suggestion concerning a prior drinking experience. As such, manipulating memories around alcohol may be more difficult than innocuous food items that may not have such strong cultural and personal associations. On the other hand, it may be that false alcohol memories are actually easier to implant than other types of memories due to the fact that it is commonly accepted that alcohol impairs memory, and thus conceivable that individuals may report blackouts or memory lapses as a direct result of intoxication and then fill in the gaps with false details (see also Nash & Takarangi, 2011).
In the study we present here, we suggested to participants that they had become sick during their early teenage years (prior to age 16) after drinking a particular type of alcohol, and examined whether they would: a) increase their confidence that the suggested event occurred; and if so, b) whether these participants would also show a decrease in preference for the specific alcohol mentioned. Such findings would have implications for subsequent alcohol use and possible intervention development.
2. Methods
2.1. Participants
Participants were 147 psychology undergraduates (Mean age = 19.1 years; 103 female; 44 male) at the University of Washington, Seattle, who received course credit for their participation.
2.2. Experimental Design
A 2 × 2 between-subjects design was used, with alcohol type (rum vs. vodka) and false suggestion (experimental vs. control) as factors. All participants completed 2 sessions, separated by one week. During Session 2, random assignment placed participants into one of the four conditions: Vodka/Experimental, Vodka/Control, Rum/Experimental, Rum/Control.
2.3. Materials and Procedure
The study procedures were approved by the University of Washington’s Institutional Review Board. Participants were led to believe that the nature of the experiment involved foods, beverages, and personality. Upon arrival, participants completed a Food and Beverage History Questionnaire (FBHQ) where they indicated whether they had experienced a series of 24 events before the age of 16 on a scale from 1 (definitely did not happen) to 8 (definitely did happen). This measure was adapted from Garry, Manning, Loftus, & Sherman’s (1996) Life Event Inventory (LEI) where individuals were asked to indicate whether a series of life events had occurred before a certain age. The FBHQ was modified to contain events that were specifically food and beverage related, including the critical items, “Got sick drinking too much vodka” (item 9) and “Felt sick to your stomach after drinking rum” (item 16). These items were worded slightly differently so that the complete verbatim similarity would not capture participants’ attention.
Next, participants completed a Food and Beverage Preference Questionnaire (FBPQ) where they rated 63 different foods and beverages (including vodka and rum) on how much they enjoyed each on a scale that ranged from 1 (definitely don’t like) to 8 (definitely like). Vodka appeared as item 12 and rum appeared as item 46 for all participants. After participants completed this questionnaire, they returned one week later to receive their individualized food and drink profile (Bernstein et al., 2005; Laney et al., 2008).
Upon arrival at Session 2 (one week later), participants were randomly assigned to one of four conditions: Vodka/Experimental (N=32), Rum/Experimental (N=33), Vodka/Control (N=36), Rum/Control (N=31). We chose to use two different types of alcohol spirits (i.e., vodka and rum), to ensure that our main findings were not alcohol specific, but instead generalized across alcohol types. All participants received an “individualized food and drink” history profile about their experiences prior to age 16, allegedly generated by a sophisticated computer program that collated their earlier responses to their questionnaires. All participants’ profiles included four items: 1) disliked broccoli 2) enjoyed eating pizza 3) felt happy when a classmate brought sweets to school and 4) did not like being told what to eat and what not to eat. Experimental participants received a fifth item depending on their condition: “got sick from drinking too much vodka” (Vodka/Experimental) or “felt sick to your stomach after drinking rum” (Rum/Experimental). The critical item appeared in position number 3 on the profile.
Participants in the experimental conditions then completed an exercise where they elaborated on the experience of getting sick drinking rum or vodka (depending on which condition they had been assigned to). They were asked their age at the time of the remembered experience, where they were and what they were doing, who they were with, how it made them feel, and how it tasted when the event happened. If they did not have an explicit memory of the event, participants were asked to imagine what might have happened had the event occurred. Control participants did not complete this exercise. Finally, to lend further credibility to the cover story of the study (i.e. food, beverage, and personality), all participants answered a follow-up question in which they were asked about their most important childhood food or beverage-related incident that was not listed on the profile.
Next, all participants completed the same questionnaires from Session 1. Participants then completed a Memory or Belief task where they indicated whether they had a) a memory of a specific listed event, b) believed it may have occurred, or c) were positive the event never occurred. Three events were listed: 1) Spilled a bowl of punch at a wedding; 2) Got sick drinking [rum, vodka]; and 3) Were overweight for a significant portion of their childhood. Participants were next asked to indicate what they believed the purpose of the study was. This measure was added to determine whether any participants were suspicious and to permit analyses with and without suspicious participants3. Finally, before participants were debriefed, they were asked to describe their first drinking experience, as well as indicate the age at which this experience occurred.
3. Results
Of the 147 participants, 132 completed both Sessions 1 and 2. Of these 132 participants, seven indicated that they were alcohol abstainers and had never drunk alcohol in their lives. Because our results and conclusions did not change whether we included these individuals, we chose to exclude them in the analyses to reduce the noise in our data, leaving us with data from N=125 participants to analyze. The grouping variable (rum, vodka) did not interact with any of the variables of concern, thus to simplify our data analysis and to increase power, we combined these groups for statistical analyses. We report adjusted statistical test results and degrees of freedom whenever we observed unequal variances.
3.1. Increased Confidence that the Alcohol-Related Experience Occurred
We first examined whether people increased their confidence after receiving a false suggestion that they got sick as a teenager drinking either rum or vodka. This increase would be evidenced by an increase in confidence from Session 1 to Session 2 on the Food and Beverage History Questionnaire (FBHQ). Figure 1 shows that overall, experimental participants demonstrated a greater increase in confidence that the suggested event happened, compared to controls. This data pattern was confirmed by a 2 (Group: Experimental, Control) X 2 (Session: 1, 2) ANOVA in which the Group X Session interaction was significant, F (1,123) = 4.27, p = .04, ηp2 = .03. Follow-up paired-sample t-tests revealed no significant differences between Session 1 and Session 2 for control participants, t(62) = .95, p = .34; and a trend for experimental participants t(61) = 1.84, p = .07, Cohen’s d = .23. Follow-up independent sample t-tests revealed that control and experimental participants did not differ during Session 1 t(117.01) =.70, p = .48, but experimental participants showed increased confidence in the critical event compared to control participants during Session 2 t(115.20) = 2.47, p = .01, Cohen’s d = .46.
Figure 1.

Participants’ mean confidence that they got sick after drinking rum or vodka on the Food and Behavior History Questionnaire (FBHQ) during Session 1 and Session 2. Error bars are standard errors.
3.2. Preference Ratings Towards Alcoholic Beverage
We next examined whether being exposed to a false alcohol suggestion had consequences for how individuals subsequently rated their current alcohol preferences, specifically related to alcohol type. Figure 2 shows that experimental participants demonstrated decreased preference for the suggested spirit, compared to controls on the FBPQ from Session 1 to Session 2. This data pattern was confirmed by a 2 (Group: Experimental, Control) X 2 (Session: 1, 2) ANOVA which revealed a significant Group by Session interaction and a medium effect size, F (1,121)= 6.56, p = .01, ηp2 = .05. Follow-up paired-sample t-tests revealed no significant differences between Session 1 and Session 2 for control participants t(60) = .35, p = .73; and a significant difference for experimental participants, t(61) = 3.75, p < .001, Cohen’s d = .48. Follow-up independent sample t-tests revealed that control participants reported lower preference ratings for the critical item during Session 1 than did experimental participants t(121) = 2.06, p = .04, Cohen’s d = .37, whereas control and experimental participants’ preference ratings did not differ during Session 2 t(122) = .55, p = .59 .
Figure 2.

Participants’ mean preference ratings for rum or vodka on the Food and Behavior Preference Questionnaire (FBPQ) during Session 1 and Session 2. Error bars are standard errors.
Another way to examine these data, considering the baseline differences between control and experimental groups, is to: a) use baseline preferences at Time 1 as a covariate predictor for Time 2 ratings (see Wright, 2006), and/or b) blindly equate groups prior to randomization. To ensure that our results were not an artifact or a product of regression to the mean, we chose to examine the data in both the aforementioned ways. First, we ran a univariate ANCOVA on Time 2 preference ratings, entering Time 1 preference ratings as a covariate and Group (Experimental, Control) as the independent variable. This yielded a statistical trend for Group with a small to medium effect size, F(1,120) = 3.40, p = .07, ηp2 = .03, indicating that, even after controlling for Time 1 preference, experimental and control participants tended to differ in terms of their preference for the critical alcohol item at Time 2.The second way we chose to examine our preference findings was by blindly equating groups. We did this by removing every other control and experimental participant who rated his/her preference for the critical item at Time 1 as 8 out of 8 (the highest preference rating possible). This blind randomization process yielded n = 54 experimental and n = 59 control participants. Although this method yielded numerically higher preference ratings for experimental participants (M = 4.31, SEM = .32) than control participants (M = 3.66, SEM = .30) at Time 1, this initial preference difference was not statistically significant t(111) = 1.50, p = .14. Using these equated Time 1 preference ratings, we again ran a univariate ANCOVA on Time 2 preference ratings, entering Time 1 preference ratings as a covariate and Group (Experimental, Control) as the independent variable. As reported previously, our results demonstrate a diminished preference for a specific type of alcohol as a result of the particular false suggestion, F(1,110) = 3.93, p = .05, ηp2 = .03
3.3. Believers vs. Non Believers in the Suggestion Groups
The data that we have presented thus far include all experimental and control participants regardless of whether they adopted the false suggestion. An important question is whether actually believing the false suggestion as part of one’s historical repertoire affected how one portrayed their subsequent preferences, and if so, whether some individuals were more likely than others to adopt the alcohol suggestion.
To answer these questions, we categorized participants as Believers versus Non-believers. Using a stringent set of criteria, we defined Believers as experimental participants who a) scored below the midpoint of the scale (i.e., 4 or below) at Time 1; b) increased their confidence on the critical item (rum, vodka) from Session 1 to Session 2; and c) indicated that they had a memory or belief for this event on the Memory or Belief task at Time 2. Conversely, Non-believers were participants who were exposed to the false suggestion but who did not meet the aforementioned criteria (see “Low-start conservative Believers” in Morris, Laney, Bernstein, & Loftus, 2006 for additional discussion around Believer classification). Additionally, we excluded participants from the analyses who scored above the midpoint at Time 1 AND indicated that they had a memory or belief for the event at Time 2, arguably removing individuals for whom the event was likely true (n = 20 were removed using this criterion). Using these stringent criteria, 10 experimental participants (19.6%) met the definition of believer, while the remaining 41 experimental participants (80%) were non-believers4.
Next, we examined whether Believers indicated lower preference ratings for the critical alcoholic beverage than did Non-believers and controls. Specifically, we calculated a difference score for every participant that was simply the difference between Session 1 and Session 2 preference ratings for the critical item. We then entered this difference score into a one-way ANOVA with Belief (Believer, Non-Believer, Control) as the between-subjects factor (see Figure 3). The ANOVA yielded a significant effect of Belief, F (2,101) = 3.37, p = .04, η2 = .06.
Figure 3.
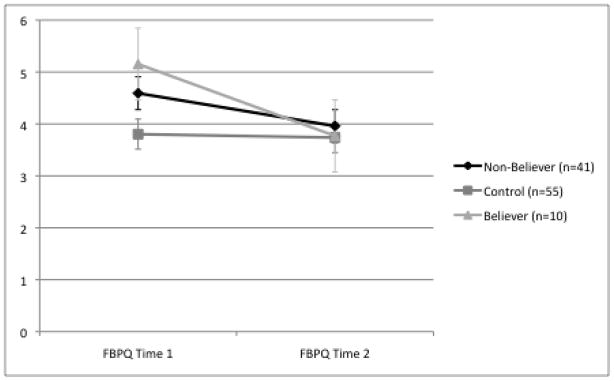
Believers’, Non-believers’, and Controls’ mean preference for rum or vodka on the Food and Behavior Preference Questionnaire (FBPQ) during Session 1 and Session 2. Error bars are standard errors.
Follow-up Bonferoni-corrected individual contrasts for these three Belief groups revealed numerically greater avoidance of the critical item for Believers (M = 1.20, SEM = .85) and Non-Believers (M = .66; SEM = .20) compared to Controls (M = .02; SEM = .21), although the only significant trend to emerge was between Believers and Controls (p = .10).
3.4. Memory vs. Belief
One may wonder about the nature of the recollection for Believers: Did these individuals develop a concrete recollection that the false feedback item occurred (reported by participants during Session 2 as a “Memory”), or were they simply convinced that it happened, needing no concrete recollection from their own memory (reported by participants during Session 2 as a “Belief”)? Of the 10 experimental participants who met our definition of Believer, 4 reported a concrete recollection of the event, and were able to furnish details about it. For example, one of these Believers reported the following during Session 2: “Thanksgiving eggnog; too much rum.” This participant indicated on the FBHQ during Session 1 that she was positive that she had never gotten sick from rum (Confidence rating of 1). However, after receiving the rum false feedback, she indicated on the second administration of the FBHQ that she was fairly confident that she had gotten sick from rum (Confidence rating of 5).
3.5. Who adopted the false suggestion as part of his/her historical repertoire?
One final question we wished to know was, who, in particular, met our definition of Believer. This question may help highlight characteristics of those who may be more prone to alter their preferences as a result of a false suggestion. Recall that we had participants report the age of their first drinking experience. We wondered whether the likelihood of an individual adopting the false suggestion was related to this factor, since presumably the further away in time participants are from their first drinking memory, the more likely that the memory may not be as salient and therefore subsequently more pliable. To determine the relationship between age and willingness to adopt suggestion as a true memory, we computed a Spearman’s rho correlation between the age at which participants indicated their first drink and whether they met our definition of Believer. We did this for both the control and experimental groups separately. Although there was no correlation between age of first drink and belief in the control group (rs = −.12, p = .42), this correlation was significant for experimental participants (rs = −.51, p < .001). Thus, Believers reported a lower mean age of first drink (M = 11.45, SEM = 1.32) than Non-Believers (M = 16.02, SEM = .59). Next, we ran a multiple regression predicting age of first drink. We entered current age of the participant first and then our definition of Believer second. Age (β = .30, p = .02) and, more importantly, Believer (β =.−.46, p = .001) both accounted for significant variance in age of first drink. Therefore, the younger the participants were when they reported having their first drink, the more likely they were to develop a belief or memory for the suggested event.
4. Discussion
We begin by summarizing our major findings. Overall, experimental participants who received a false alcohol suggestion showed a significant increase in confidence compared to controls that the event occurred in their past. More importantly, individuals who received a false suggestion that they had gotten sick from vodka [or rum] showed a trend toward diminished preference for the suggested alcohol type in a follow-up preference rating task. Upon further exploration, our analyses reveal that this preference effect may be related to whether one actually adopts the false suggestion as part of their historical repertoire (i.e., Believers vs. Non-Believers), although further exploration of this variable is warranted before definitive conclusions can be drawn. A third finding, not examined in any prior research, was that participants who reported believing the suggestion tended to report a younger first drinking experience than those who did not come to believe the suggestion. This third finding may shed light on characteristics that might be important in understanding who is susceptible to adopting false memories.
Taken together, a false suggestion about getting sick on a particular type of alcohol in one’s young adulthood (prior to age 16) appears to have implications for an individual’s current and future associations with that specific alcoholic beverage. These findings are consistent with the alcohol expectancy literature, namely the relationship between thoughts and beliefs around alcohol and its connection to future drinking-related behaviors. In other words, the alcohol expectancy literature has shown that positive alcohol expectancies are associated with increased and risky drinking behavior, whereas negative alcohol expectancies are associated with decreased drinking behavior (see also Houben & Weirs, 2007; Zamboanga, Ham, Olthuis, Martens, Grossbard, & Van Tyne, 2012; Scott-Sheldon, Terry, Carey, Garey, & Carey, 2012).
4.1. Limitations
We must acknowledge some limitations in this research. First, it is important to note that only 19.6% of our experimental participants developed a memory or belief that the suggested alcohol memory occurred. Although our Believer rate falls within the range of Believers in other false memory studies5, we speculate on possible explanations for this somewhat lower rate of 19.6%. First, it may be that planting a false underage alcohol memory is more difficult than planting another innocuous memory such as getting sick eating peach yogurt, due to the cultural cache and personal associations surrounding alcohol. Moreover, our Believer rates may be related to the age at which we offered the suggestion (i.e., “prior to the age of 16”), compared to most studies that suggest a younger age (i.e., “prior to the age of 10”). For example, Garry & Hayes (1999) showed that the timing of the false event mattered. In their study, individuals who were asked to imagine recent events (i.e., 5 years prior) did not experience the typical increase in confidence that has been repeatedly shown in the false memory literature. Considering that the mean age of participants in our study was 19.1 and we were asking about events that may have happened as recently as 3 years prior (i.e., 16), this may have made it more difficult for some people to believe our false suggestion. The corollary to this idea, is that the further away in time individuals were to their first drinking experience, the more likely they were to adopt the false suggestion. Regardless of our explanations for our 19.6% Believer rate, one may still be weary of relying on such a small proportion of individuals (N=10) to draw conclusions and/or generalize findings. Given that we used multiple statistical approaches, had a comparable sample size to other similar studies, and our pattern of results replicated existing false memory research in other domains (i.e., false food memories; see Scoboria et al., 2012), we are confident that our results are not merely an artifact, but show an extension of the literature into the alcohol domain.
Second, the fact that differences existed at baseline between our experimental and control participants for alcohol preferences does not allow us to rule out the possibility that these preference findings are due to regression to the mean. Despite this possibility, we analyzed the preference data using a variety of different approaches (i.e., ANOVA, ANCOVA and blindly equating groups) and maintained a consistent patterns of results. Further, previous robust findings outside the alcohol literature indicate that false suggestions affect preferences (i.e. see Bernstein et al., 2005; Geraerts et al., 2008; Scoboria et al. 2008, 2012; for example). These points indicate that regression to the mean is still a viable, albeit unlikely explanation for our findings.
Our data also indicated that those who reported a younger first drinking experience were the individuals who were more likely to adopt the false suggestion. This finding may be of particular interest to alcohol researchers given what we know about the connections between age of first drink (i.e. younger) and subsequent development of alcohol dependence (see Hingson, Heeren, & Winter, 2006 for a review). Hingson and colleagues show that individuals who begin drinking prior to age 14 are approximately 5 times more likely to experience alcohol dependence compared to those who begin drinking at age 21 or older. Thus, our study may illuminate additional cognitive characteristics of individuals who may be at risk for developing alcohol problems.
Further, some may argue that because early onset drinkers are known to be at higher risk for subsequent problem drinking (see also Chou & Pickering, 1992; Le Strat, Grant, Ramoz, & Gorwood, 2010), these individuals may ultimately be remembering true events from their past. Although we cannot rule out the possibility that our suggestion is eliciting a true memory, it is unlikely in this circumstance, given that other false memory research using procedures nearly identical to the ones we use in this study have led people to create memories of things that were implausible (i.e., witnessing a demonic possession: Mazzoni, Loftus, & Kirsch, 2001) or even impossible (i.e., meeting Bugs Bunny at Disneyland—an impossible event because Bugs Bunny is a Warner Brothers character: Braun, Ellis, & Loftus, 2002). However, even if our technique is eliciting true forgotten alcohol memories, as stated previously, our findings that alcohol preference appears to be affected by a “got sick” alcohol suggestion still bears clinical significance.
Another argument that may be made about early age-of-onset drinking is that these individuals might show different cognitive vulnerabilities than their later- drinking counterparts (Corte & Zucker, 2008). Thus, it is possible that some third variable that we are not considering and which is related to cognitive vulnerability is driving both acceptance of the manipulation and early age-of-onset drinking6. Future research may wish to examine this preference effect, its mediating factors and further explore who is more likely to adopt these types of memories.
Despite these stated limitations, our study suggests that, in some cases, preference for a particular type of alcohol may be altered via the suggestion that one had gotten sick from it in their youth. Thus, alcohol memories evoked about one’s past (whether they are true or false) may have particular consequences for one’s current thoughts, preferences and ultimately, drinking behavior.
4.2. Conclusions
Ultimately, our study shows that the current false memory paradigm can be extended to alcohol-related memories despite the cultural significance surrounding alcohol. Future research needs to address the behavioral effects of such an alcohol suggestion and determine whether a “got sick” alcohol suggestion such as the one we used here could be enough to deter individuals from actually drinking the suggested type of alcohol (for a separate but related study on behavioral effects of false alcohol suggestions see Mantonakis, Wudarzewski, Bernstein, Clifasefi, & Loftus, in press). We acknowledge that using techniques to elicit false alcohol memories for the purposes of alcohol deterrence raises ethical concerns that may more than offset any potential benefits of the approach. For example, what happens when people learn that they have received an intervention based on deception? Can we just concoct things and tell them to people if it helps reduce their drinking? Do the ends justify the means?7 These are questions and issues that would need to be considered carefully before ever considering translating these findings into a clinical intervention. Though this particular false memory technique is a long way away from being put into practice for alcohol deterrence, the research provides a foundation by which we can continue to explore underlying cognitive mechanisms that may be associated with drinking behavior, as well as laying the platform for ethical behavioral therapy practices aimed at reducing unwanted or undesirable drinking behaviors.
Supplementary Material
Research highlights.
Participants who received a false alcohol suggestion increased their confidence in a fictitious past drinking episode
Participants who received a false alcohol suggestion showed a trend toward subsequent diminished alcohol preferences
Receiving a false alcohol suggestion about one’s past may influence current alcohol preferences.
Acknowledgments
Dr. Clifasefi would like to acknowledge the National Institutes of Health/National Institute on Alcohol and Alcohol Abuse postdoctoral training grant (#T32 AA07455-19; PI: Larimer) for partially supporting this research effort. Dr. Bernstein would like to acknowledge Kwantlen Polytechnic University’s Professional Development Grant for their support in making this research endeavor possible. Our team would like to thank Briana Wakefield for help with data collection.
Footnotes
A recent study exploring how people choose to reconstruct alcohol blackouts suggests that the reconstructing process can indeed lead to the development of false alcohol beliefs or memories (see Nash and Takarangi, 2011)
The vast majority of participants (over 95%) had little to no idea about the study’s purpose deeming analyses with suspicious versus unsuspicious participants unnecessary. Thus, both suspicious and unsuspicious participants were included in the overall analyses.
The percent of Believers in this study is comparable to other studies with similar or less restrictive Believer criteria (see Morris et al., 2006).
Morris et al. (2006) found a Believer rate of 10% using what they call an ultraconservative definition and 22% using what they call a low-start conservative definition. Our stringent criteria falls somewhere between the midpoint of this ultraconservative and low-start conservative definition, thus resulting in a 19.6% Believer rate.
We would like to thank an anonymous reviewer for this suggestion.
We would like to thank an anonymous reviewer for suggesting these ethical considerations.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Daniel M. Bernstein, Email: daniel.bernstein@kwantlen.ca.
Antonia Mantonakis, Email: amantonakis@brocku.ca.
Elizabeth F. Loftus, Email: eloftus@uci.edu.
References
- Bernstein DM, Laney C, Morris EK, Loftus EF. False memories about food can produce food avoidance. Social Cognition. 2005;23:11–34. [Google Scholar]
- Bernstein DM, Pernat N, Loftus EF. The false memory diet: False memories alter food preference. In: Preedy VR, Watson RR, Martin CR, editors. Handbook of behavior, food, and nutrition. New York: Springer; 2011. pp. 1645–1663. [Google Scholar]
- Brainerd CJ, Reyna VF. The science of false memory. New York: Oxford University Press; 2005. [Google Scholar]
- Braun KA. Post experience advertising effects on consumer memory. Journal of Consumer Research. 1999;25:319–334. [Google Scholar]
- Braun KA, Ellis R, Loftus EF. Make my memory: how advertising can change our memories of the past. Psychology & Marketing. 2002;19:1–23. [Google Scholar]
- Chou SP, Pickering RP. Early onset of drinking as a risk factor for lifetime alcohol-related problems. British Journal of Addiction. 1992;87:1199–1204. doi: 10.1111/j.1360-0443.1992.tb02008.x. [DOI] [PubMed] [Google Scholar]
- Corte C, Zucker RA. Self-concept disturbances: cognitive vulnerability for early drinking and early drunkenness in adolescents at high risk for alcohol problems. Addictive Behaviors. 2008;33:1282–90. doi: 10.1016/j.addbeh.2008.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Council on Scientific Affairs of the American Medical Association. Aversion therapy. Journal of the American Medical Association. 1987;18:2562–2565. [Google Scholar]
- Elkins RL. Aversion therapy for alcoholism: Chemical, electrical, or verbal imaginary? The International Journal of the Addictions. 1975;10:157–209. [Google Scholar]
- Garry M, Hayes JH. Unpublished manuscript. Victoria University of Wellington; Wellington, New Zealand: 1999. Imagination inflation depends on when the imagined event occurred. [Google Scholar]
- Garry M, Manning CG, Loftus EF, Sherman J. Imagination inflation: Imagining a childhood event inflates confidence that it occurred. Psychonomic Bulletin and Review. 1996;3:208–214. doi: 10.3758/BF03212420. [DOI] [PubMed] [Google Scholar]
- Geraerts E, Bernstein DM, Merckelbach H, Linders C, Raymaekers L, Loftus EF. Lasting false beliefs and their behavioral consequences. Psychological Science. 2008;19:749–53. doi: 10.1111/j.1467-9280.2008.02151.x. [DOI] [PubMed] [Google Scholar]
- Goldman MS, Del Boca FK, Darkes J. Alcohol Expectancy theory: the application of cognitive neuroscience. In: Leonard KE, Blane HT, editors. Psychological Theories of Drinking and Alcoholism. 2. Guilford Press; New York: 1999. pp. 203–246. [Google Scholar]
- Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Archives of Pediatric Adolescent Medicine. 2006;160:739–46. doi: 10.1001/archpedi.160.7.739. [DOI] [PubMed] [Google Scholar]
- Howard MO. Pharmacological aversion treatment of alcohol dependence: production and prediction of conditioned alcohol aversion. American Journal Drug Alcohol Abuse. 1991;27:561–585. doi: 10.1081/ada-100104519. [DOI] [PubMed] [Google Scholar]
- Houben &, Weirs RWHJ. Are drinkers implicitly positive about drinking alcohol? Personalizing the alcohol-IAT to reduce negative extrapersonal contamination. Alcohol & Alcoholism. 2007;42:301–307. doi: 10.1093/alcalc/agm015. [DOI] [PubMed] [Google Scholar]
- Hyman IE, Husband TH, Billings FJ. False memories of childhood experiences. Applied Cognitive Psychology. 1995;9:181–197. [Google Scholar]
- Kirsch I. How Expectancies Shape Experience. American Psychological Association; Washington, DC: 1999. [Google Scholar]
- Laney C, Morris EK, Bernstein DM, Wakefield BM, Loftus EF. Asparagus, a love story: Healthier eating could be just a false memory away. Experimental Psychology. 2008;55:291–300. doi: 10.1027/1618-3169.55.5.291. [DOI] [PubMed] [Google Scholar]
- Le Strat Y, Grant BF, Ramoz N, Gorwood P. A new definition of early age at onset in alcohol dependence. Drug and Alcohol Dependence. 2010;108:43–48. doi: 10.1016/j.drugalcdep.2009.11.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Loftus EF, Pickrell JE. The formation of false memories. Psychiatric Annals. 1995;25:720–725. [Google Scholar]
- Maguire RJ, Vallance M. Aversion therapy by electric shock: a simple technique. British Medical Journal. 1964;1:151–153. doi: 10.1136/bmj.1.5376.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maisto SA, Carey MP, Carey KB, Gordon CM. The effects of alcohol and expectancies on risk perception and behavior skills relevant to safer sex among heterosexual young adult women. Journal of Studies on Alcohol. 2002;63:476–485. doi: 10.15288/jsa.2002.63.476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mantonakis A, Wudarzewski A, Bernstein DB, Clifasefi SL, Loftus EF. False beliefs can shape current consumption. Psychology (in press) [Google Scholar]
- Mazzoni GA, Loftus EF, Kirsch I. Changing beliefs about implausible autobiographical events: a little plausibility goes a long way. Journal of Experimental Psychology Applied. 2001;7:51–9. [PubMed] [Google Scholar]
- McRobbie H, Hajek P. Effects of rapid smoking on urges to smoke over the first four weeks of abstinence. Addiction. 2007;102:483–489. doi: 10.1111/j.1360-0443.2006.01730.x. [DOI] [PubMed] [Google Scholar]
- Morris EK, Laney C, Bernstein DM, Loftus EF. Susceptibility to memory distortion: How do we decide it has occurred? American Journal of Psychology. 2006;119:255–276. [PubMed] [Google Scholar]
- Nash RA, Takarangi MKT. Reconstructing alcohol-induced memory blackouts. Memory. 2011;19:566–573. doi: 10.1080/09658211.2011.590508. [DOI] [PubMed] [Google Scholar]
- Riley AL, Freeman KB. Conditioned taste aversion: a database. Pharmacology, Biochemistry and Behavior. 2004a;77:655–656. doi: 10.1016/j.pbb.2004.01.002. [DOI] [PubMed] [Google Scholar]
- Riley AL, Freeman KB. Conditioned flavor aversions: assessment of drug-induced suppression of food intake. In: Crawley JN, Gerfen C, McKay R, Rogawski M, Sibley DR, Skolnick P, editors. Current protocols in Neuroscience. New York: Wiley; 2004b. [DOI] [PubMed] [Google Scholar]
- Scoboria A, Mazzoni G, Jarry JL. Suggesting childhood food illness results in reduced eating behavior. Acta Psychologica. 2008;128:304–9. doi: 10.1016/j.actpsy.2008.03.002. [DOI] [PubMed] [Google Scholar]
- Scoboria A, Mazzoni G, Jarry J, Bernstein DM. Personalized, not general, suggestion affects false memory and suggestion-consistent behavior. Acta Psychologica. 2012;139:225–232. doi: 10.1016/j.actpsy.2011.10.008. [DOI] [PubMed] [Google Scholar]
- Scott-Sheldon LAJ, Terry DL, Carey KB, Garey L, Carey MP. Efficacy of expectancy challenge interventions to reduce college student drinking: A meta-analytic review. Psychology of Addictive Behaviors. 2012;26:393–405. doi: 10.1037/a0027565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vogel-Sprott M, Fillmore MT. Expectancy and behavioral effects of socially-used drugs. In: Kirsch I, editor. Expectancy, Experience and Behavior. American Psychological Association; Washington, DC: 1999. pp. 215–232. [Google Scholar]
- Wade KA, Garry M, Read JD, Lindsay DS. A picture is worth a thousand lies: Using false photographs to create false childhood memories. Psychonomic Bulletin and Review. 2002;9:597–603. doi: 10.3758/bf03196318. [DOI] [PubMed] [Google Scholar]
- Wright DB. Comparing groups in a before–after design: When t test and ANCOVA produce different results. British Journal of Educational Psychology. 2006;76:663–675. doi: 10.1348/000709905X52210. [DOI] [PubMed] [Google Scholar]
- Zamboanga BL, Ham LS, Olthuis JV, Martens MP, Grossbard JR, Van Tyne K. Alcohol expectancies and risky drinking behaviors among high school athletes: “I’d rather keep my head in the game”. Prevention Science. 2012;13:140–149. doi: 10.1007/s11121-011-0252-3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.