

Abstract
An 11-years-old girl with a polyp in the gallbladder is reported. Laparoscopic cholecystectomy was curative.
Keywords: Adenomatous polyp, cholecystectomy, gallbladder polyp, pediatric
INTRODUCTION
Polypoidal lesions of the gallbladder are reported mainly in adults but are rarely seen in the pediatric population.[1,2] The clinical presentation may simulate cholecystitis and cholelithiasis. Till 2006, only 13 cases of gallbladder polyps were reported in the available English literature.[3]
CASE REPORT
A girl, aged 11-years-old, was admitted with colicky pain in the right hypochondrium and nausea. There was history of similar attacks of pain in last 1 year. There was no history of fever and jaundice. Her abdomen was soft, and no lump was palpable.
The hematological investigations and liver function tests were normal. An ultrasonography (USG) of the abdomen revealed a polypoidal mass measuring 12 mm × 8 mm arising from the wall of the gall bladder [Figure 1]. There was no evidence of calculus in the gallbladder. The common bile duct was normal. Contrast-enhanced computed tomogram (CECT) confirmed the presence of gallbladder polyp. There was no evidence of common channel on magnetic resonance cholangio pancreatography (MRCP).
Figure 1.
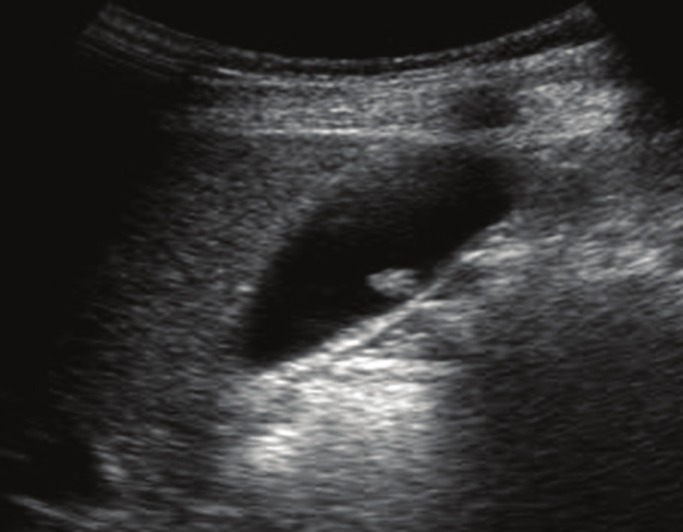
Gall bladder polyp in ultrasonography
Laparoscopic cholecystectomy was done. A sessile polyp measuring 10 mm x 9 mm was revealed in gall bladder [Figure 2]. There was no stone. The patient had a smooth recovery and was discharged on the second day. The patient was seen 6 months after the operation and was symptom-free. Histopathology revealed a benign adenomatous polyp arising from the body of the gallbladder. Other sections of the gallbladder showed features of chronic inflammation.
Figure 2.
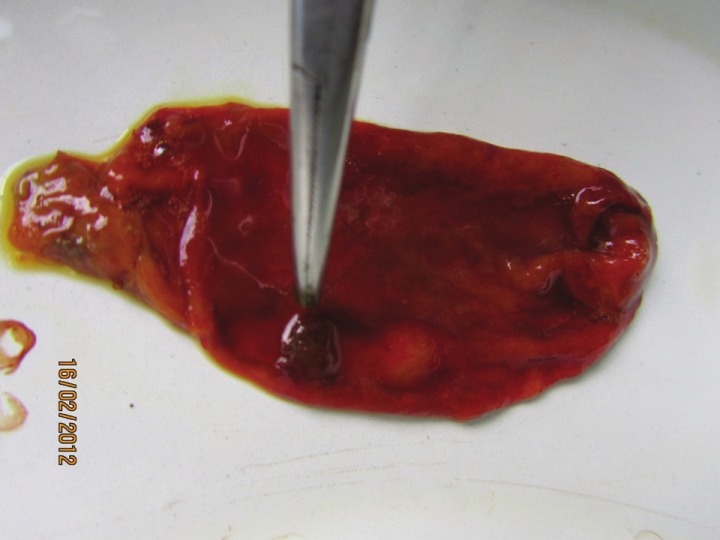
Cut open specimen showing gall bladder polyp
DISCUSSION
By definition, any lesion protruding from the wall of the gallbladder into the lumen is called a polyp.[4] Christensen classified gallbladder polyp as benign tumors, pseudotumors, and malignant neoplasms.[5] Gallbladder polyps are also classified in two groups: Tumorous and non-tumorous.[6] Non-tumorous polyps may be inflammatory and cholesterol. Tumorous variety may be adenoma, adenomyoma, and early gallbladder carcinoma. In addition to tumorous and non-tumorous types, these polyps have been classified into primary and secondary. Pathological spectrum of gallbladder polyp in children is different from adults. Majority of the gallbladder polyps are cholesterol polyps, whereas hyperplastic and adenomatous polyps are next common forms.[7] Gastric heterotopia has also been reported in gallbladder polyp.[1] Hyperplastic polyp of the gall bladder has been associated with pancreato-biliary maljunction.[8] In another interesting study, authors have documented progressive change in the ultrasound pictures of gall bladder and extrahepatic ducts secondary to a common pancreato-biliary channel and pancreato-biliary reflux.[9] Hamartomatous polyp in the gallbladder has been reported in association with Peutz-Jeghers syndrome and choledochal cyst.[4] Gardner's syndrome is also known to develop gallbladder polyp.[7] Gallbladder polyp may be associated with acalculus cholecystitis.
Polyps can be distinguished from gallbladder stones by their lack of a shadow and non-mobile nature, and from sludge balls by their lack of mobility. Larger polyps may have detectable blood flow on color doppler. In different sequences in USG, if the stone is not impacted, it changes its position, but polyp will not change its position.
The experience of polypoidal lesions of the gallbladder in children is limited.[6] Gallbladder polyp is reported to be common in male and obese children.[10] Cholecystectomy is the recommended method of treatment, as these lesions are reported to be associated with acalculus cholecystitis, and their long-term effects are not known. Other indications of cholecystectomy in gallbladder polyp are: (a) When the size of the polyp is more than 1 cm even if asymptomatic. (b) When gallbladder polyp is associated with gallstone disease. (c) The patient is suffering from recurrent attacks of significant biliary symptoms. Fortunately, most polypoidal lesions reported in pediatric age group are benign.[10]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Stringer MD, Ceylan H, Ward K, Wyatt JI. Gallbladder polyp in children- classification and management. J Pediatr Surg. 2003;38:1680–4. doi: 10.1016/s0022-3468(03)00583-9. [DOI] [PubMed] [Google Scholar]
- 2.Barzilai M, Lerner A. Gallbladder polyp in children: A rare condition. Pediatr Radiol. 1997;27:54–6. doi: 10.1007/s002470050063. [DOI] [PubMed] [Google Scholar]
- 3.Coe HJ, Baek SY, Oh JT, Chung KS. A case of Gall Bladder Polyp in Children. Korean J Pediatr Gastroenterol Nutr. 2006;9:280–3. [Google Scholar]
- 4.Karaosmmanoglu AD, Blake M. Hamartomatous Polyp of the Gallbladder with an Associated Choledochal Cyst. JUSM. 2010;29:1663–6. doi: 10.7863/jum.2010.29.11.1663. [DOI] [PubMed] [Google Scholar]
- 5.Christensen AH, Ishak KG. Benign tumors and pseudotumors of the gall bladder. Arch Pathol. 1970;90:423–32. [PubMed] [Google Scholar]
- 6.Stringel G, Beneck D, Bostwick HE. Polypoid lesions of the Gallbladder in Children. JSLS. 1997;1:247–9. [PMC free article] [PubMed] [Google Scholar]
- 7.Beck PL, Shaffer EA, Gall DG, Sherman PM. The natural history and significance of ultrasonographically defined polypoid lesions of the gallbladder in children. J Pediatr Surg. 2007;42:1907–12. doi: 10.1016/j.jpedsurg.2007.07.021. [DOI] [PubMed] [Google Scholar]
- 8.Okada T, Sasaki F, Honda S, Mastuno Y, Kubota K, Todo S. Hyperplastic polyp of the gallbladder associated with pancreaticobiliary maljunction in a 9-year-old girl. Pediatr Surg Int. 2009;25:999–1002. doi: 10.1007/s00383-009-2458-z. [DOI] [PubMed] [Google Scholar]
- 9.Pushparani P, Redkar RG, Howard ER. Progressive biliary pathology associated with common pancreato-biliary channel. J Pediatr Surg. 2000;35:649–51. doi: 10.1053/jpsu.2000.0350649. [DOI] [PubMed] [Google Scholar]
- 10.Lugo-Vicente H. Gallbladder polyp. Pediatr Surg Update. 2004;22:1–3. [Google Scholar]