

Abstract
Congenital coronary artery fistulae may be isolated or may be associated with complex congenital cardiac abnormalities. In patients with complex congenital heart disease, multiple fistulous or sinusoidal communications with a cardiac chamber can occur. The treatment strategy includes surgery, coil embolization and covered stent deployment. The present article describes a case involving a 20-year-old patient with complex congenital heart lesions and multiple sinusoidal coronary to right ventricle fistulous communications, which remained patent despite coil embolization in childhood. Further coil or device embolization was deemed unlikely to be successful due to the presence of multiple communications; therefore, covered stents were deployed across the previously coiled segment of the coronary artery. The patient had an excellent clinical outcome on follow-up nine months later, with significant improvement of symptoms.
Keywords: Coil embolization, Coronary artery fistulae, Covered coronary stents
The incidence of coronary artery fistulae in patients undergoing coronary angiography is 0.1% (1). Patients with significant shunts can be treated surgically or with transcatheter interventions.
CASE PRESENTATION
The patient was a 20-year-old woman who was born with complex congenital heart disease, including pulmonary atresia with intact ventricular septum, tricuspid atresia with a rudimentary right ventricle (RV) and sinusoidal communications between the coronary arteries and the RV. She had undergone various surgical procedures, including shunt surgery at two weeks of age, cavopulmonary connections at five weeks of age and an extracardiac conduit Fontan completion with a 5 mm fenestration. At nine years of age, she underwent coil occlusion of a right coronary artery (RCA) to RV fistula, and a left anterior descending artery (LAD) to RV fistulae, followed by stenting of the RCA and LAD. She was referred for repeat assessment of anginal pains and shortness of breath. Cardiac catheterization revealed excellent patency of her Fontan communications. Coronary angiography revealed RCA in-stent restenosis and residual LAD coronary-to-RV sinusoidal fistulous communications (Figure 1). There was also a residual fistulous communication between the RCA and RV. The stent in the LAD appeared to exhibit mild in-stent restenosis. The circumflex vessel appeared satisfactory. The patient was treated for the in-stent restenosis of the RCA lesion by deployment of a 4.5 mm × 12 mm Taxus stent (Boston Scientific, USA), with excellent results. The patient continued to experience significant anginal symptoms and was, therefore, readmitted for closure of the fistulas and in-stent restenosis of the LAD.
Figure 1).
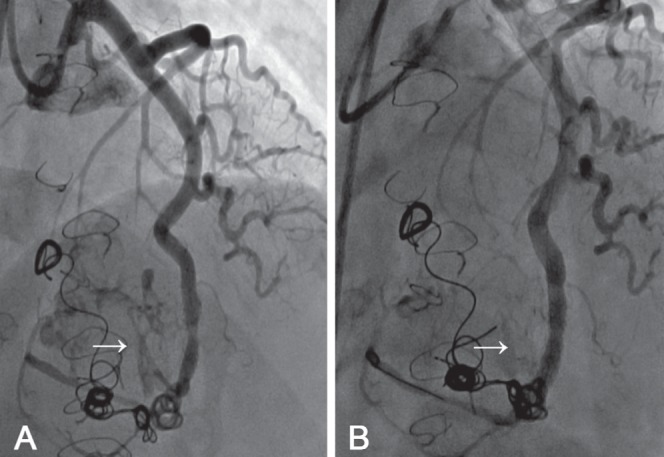
Coronary angiography demonstrating the left anterior descending artery with coils and multiple fistulas (arrow) A Before stenting. B Following covered stent implantation within previous coil embolized lesions
PROCEDURE
A 90 cm JL4 guide catheter (Cordis, USA) was used to intubate the left coronary system. The vessel was wired using a BMW wire (Abbott Vascular, USA). There were multiple sinusoidal communications opening into the RV from the distal LAD, which would have made attempting coil embolization very difficult. The previously stented segment in the LAD also appeared to have a moderate narrowing in the middle segment. A 4.0 mm × 19 mm Graftmaster Jostent covered stent (Abbott Vascular, USA) was deployed at 18 atmospheres in the proximal segment (Figure 2) and 3.0 mm × 16 mm across the coiled segment to cover the fistulous communications. These were postdilated using a 5.0 mm × 5 mm Quantum Balloon (Boston Scientific, USA) up to 16 atmospheres, which resulted in nearly complete obliteration of the fistulous communication from the LAD to RV and preservation of the distal LAD vessel.
Figure 2).
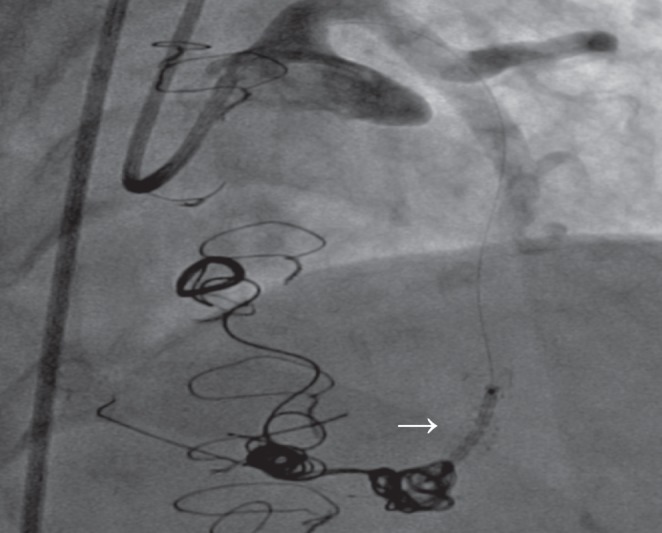
Covered stent (arrow) in a previous coil and previous stent
DISCUSSION
Covered stents have been used in the treatment of a variety of lesions including aneurysmal saphenous vein graft fistulae (2), iatrogenic coronary artery fistulae (3), procedure-related coronary artery perforations, internal mammary artery to pulmonary vasculature fistulae (4), coronary-pulmonary artery fistulae (5,6) and peripheral vascular fistulae. Similarly, transcatheter coil embolization has been successfully used in patients with multiple coronary artery fistulae (7,8). Our patient had multiple sinusoidal coronary-to-RV fistulous communications as a child and underwent coil embolization, but her symptoms recurred and, due to residual multiple fistulas, covered stents were used within the previously coil embolized lesions. In our patient, covered stents were used to treat multiple residual coronary-to-RV sinusoidal communications across an area previously treated with coil embolization.
CONCLUSION
Covered stents can be used to treat residual multiple coronary fistulous communications across a previously coil-embolized region in patients with complex congenital heart disease.
REFERENCES:
- 1.Vavuranakis M, Bush CA, Boudoulas H. Coronary artery fistulas in adults: Incidence, angiographic characteristics, natural history. Cathet Cardiovasc Diagn. 1995;35:116–20. doi: 10.1002/ccd.1810350207. [DOI] [PubMed] [Google Scholar]
- 2.Bell B, Bett N, Walters DL. Fistula from aneurysmal saphenous vein graft to right atrium treated with covered stents. Heart Lung Circ. 2010;19:465–9. doi: 10.1016/j.hlc.2010.05.005. [DOI] [PubMed] [Google Scholar]
- 3.Oreglia JA, Bruschi G, Klugmann S. Percutaneous treatment of iatrogenic left anterior descending artery to right ventricle fistula. Catheter Cardiovasc Interv. 2010;76:975–7. doi: 10.1002/ccd.22551. [DOI] [PubMed] [Google Scholar]
- 4.Jamshidi P, Ghaffari S, Mahmoodi K. Transpulmonary closing of left internal mammary artery to pulmonary artery fistula with polytetrafluoroethylene covered stent: A case report and review of literature. Cardiol J. 2009;16:469–72. [PubMed] [Google Scholar]
- 5.Aur der Maur C, Chatterjee T, Erne P. Percutaneous transcatheter closure of coronary-pulmonary artery fistula using polytetrafluoroethylene-covered graft stents. J Invasive Cardiol. 2004;16:386–8. [PubMed] [Google Scholar]
- 6.Atmaca Y, Altin T, Ozdol C, Pamir G, Caglar N, Oral D. Coronary-pulmonary artery fistula associated with right heart failure: successful closure of fistula with a graft stent. Angiology. 2002;53:613–6. doi: 10.1177/000331970205300519. [DOI] [PubMed] [Google Scholar]
- 7.Raju MG, Goyal SK, Punnam SR, Shah DO, Smith GF, Abela GS. Coronary artery fistula: A case series with review of the literature. J Cardiol. 2009:467–72. doi: 10.1016/j.jjcc.2008.09.009. [DOI] [PubMed] [Google Scholar]
- 8.Hendry C, Mahadevan V, Fath-Ordoubadi F. Successful percutaneous closure of coronary artery fistula with angiographic follow-up at 6 months. Catheter Cardiovasc Interv. 2009;73:581–3. doi: 10.1002/ccd.21830. [DOI] [PubMed] [Google Scholar]