

Abstract
BACKGROUND
Intergenerational transfer patterns in sub-Saharan Africa are poorly understood, despite the alleged importance of support networks to ameliorate the complex implications of the HIV/AIDS epidemic for families.
OBJECTIVE
There is a considerable need for research on intergenerational support networks and transfers to better understand the mechanisms through which extended families cope with the HIV/AIDS epidemic and potentially alleviate some of its consequences in sub-Saharan Africa, and to comprehend how transfers respond—or not—to perceptions about own and other family members' health.
METHODS
Using the 2008 round of the Malawi Longitudinal Study of Families and Health (MLSFH), we estimate the age patterns and the multiple directions of financial and non-financial transfer flows in rural Malawi—from prime-aged respondents to their elderly parents and adult children age 15 and up. We also estimate the social, demographic and economic correlates of financial and non-financial transfers of financial intergenerational transfers in this context.
RESULTS AND CONCLUSIONS
Our findings are that: (1) intergenerational financial and non-financial transfers are widespread and a key characteristic of family relationships in rural Malawi; (2) downward and upward transfers are importantly constrained and determined by the availability of transfer partners (parents or adult children); (3) financial net transfers are strongly age-patterned and the middle generations are net-providers of transfers; (4) non-financial transfers are based on mutual assistance rather than reallocation of resources; and (5) intergenerational transfers are generally not related to health status, including HIV positive status.
1. Introduction
Individuals in sub-Saharan Africa (SSA) are frequently exposed to multiple social, economic and environmental burdens, including poverty levels that are among the highest in the world, volatile incomes, and a living environment characterized by high disease prevalence and high mortality. In addition, individuals and families in these contexts have very limited or no access to formal insurance and social protection systems that can buffer the consequences of frequent economic and health shocks, or that can provide support for frail and less productive individuals. In the absence of formal insurance and institutionalized transfer systems, informal redistribution of resources and reciprocity—often occurring among nuclear family members and extended kin—are the primary mechanisms providing insurance against risks and support in periods of needs (Ben-Porath 1980; Kohler and Hammel 2001; Hammel 2005; Pollak 1985; Rosenzweig 1988; Rosenzweig and Stark 1989; Watkins and Swidler 2007). In this context, the family is a central institution through which shocks are mitigated, investments in human and social capital are secured, and support for dependent children and elderly is provided (Ben-Porath 1980; Frankenberg, Lillard, and Willis 2002; Pörtner 2001). From an intergenerational perspective, nuclear families and kin members act as key providers of income and support through the redistribution of resources from productive prime-aged adults to dependent relatives at younger and older ages. These intergenerational transfer behaviors and transfer flows are constrained by demographic processes such as fertility, mortality, and migration patterns that shape the age-structure of the population and the composition of multigenerational families more specifically, and thus determine the availability of kin resources. In addition, intergenerational transfer patterns are shaped by the underlying social, economic, cultural, normative and political context in which these transfers occur (Wachter, Knodel, and VanLandingham 2002; Hammel 2005; Billari and Liefbroer 2008; Palloni, Pinto, and Wong 2010; Knodel, Chayovan, and Siriboon 1992; Kohler and Hammel 2001; Bianchi et al. 2008; Velkoff and Kowal 2006; Merli and Palloni 2006; Zagheni 2011).
In the context of the HIV/AIDS epidemic in SSA, a focus on transfer relations and behavior is of particular relevance for several important reasons. By affecting fertility, morbidity, and mortality patterns in the region, the HIV/AIDS epidemic has changed the demographic determinants of transfer behavior, resulting in substantial disruptions in social network structure, intergenerational composition of families and availability of kin. Support provided through kin networks, however, may partially alleviate the consequences of the epidemic for those who are directly or indirectly affected by the increased morbidity and mortality resulting from HIV/AIDS. Intergenerational transfers are an important, and perhaps even the most essential component of the existing support networks in SSA. The pattern and extent of these transfers is likely to be shaped by perceptions of own and other family members' health and mortality pattern.
Despite the potentially heightened relevance of intergenerational relationships in the context of HIV/AIDS, the transfers occurring within families in SSA are currently poorly understood and documented.5 The age patterns and directions of financial and non-financial transfers and their relationship to the health status of different generations, have not been described in detail in a SSA context (exceptions include Weinreb 2002; Mtika and Doctor 2002; Mtika 2003). Our knowledge about the flows and distribution of transfers between generations is thus very limited.
For example, since its outbreak in the late 1980s the HIV/AIDS epidemic has transformed the demographic, health, social and economic environment in SSA.6 The impact of the HIV/AIDS epidemic is not only direct, through mortality, but the levels and specifically the characteristic age pattern of the disease have indirect implications for household structure through fertility, household organization and residential patterns. The high levels of HIV/AIDS morbidity and mortality in SSA have been hypothesized in the literature to have disruptive, profound and immediate impacts on multiple aspects of individuals' and their extended families' lives (Merli and Palloni 2006; Bray 2009; Nyasani, Sterberg, and Smith 2009; Knodel, Watkins, and VanLandingham 2003; Hosegood and Timaeus 2006; Mtika 2001; Floyd et al. 2007; Naidu and Harris 2005; Peters, Kambewa, and Walker 2008; Zimmer 2009; Zagheni 2011). HIV/AIDS is also expected to add significantly to the burden of aging in SSA as well as in other developing regions (Wachter, Knodel, and VanLandingham 2002; Ankrah 1994). For instance, while the median age of the Malawi population is still below 17 years, Malawi—similarly to other SSA countries—will age rapidly in the next decades in ways that are significantly different from the aging patterns in other developing countries due to the consequences of the AIDS epidemic (Cohen and Menken 2006; Merli and Palloni 2006; Heuveline 2004; Zaba, Whiteside, and Boerma 2004).
Since a substantial proportion of the elderly in SSA are supported by intra- and inter-generational family networks, AIDS-related morbidity and mortality that peak at primary adult ages affect the ability of families to care for their elderly members, and increases the pressure on existing support networks (Merli and Palloni 2006; Bray 2009; Zagheni 2011). In addition, the HIV/AIDS epidemic increases the importance of older individuals in sustaining the family through financial and non-financial contributions, or taking on care-giver's responsibilities for sick adult children and a rising number of orphaned grandchildren. The observed transfer patterns between family members reflect thus both, the short-term needs for and/or abilities to provide transfers, as well as longer-term life-course considerations in which individuals adjust transfer patterns to changes in household structure and life-course patterns of health, consumption and productivity. In the rapidly changing SSA epidemiological and socioeconomic context, however, individuals' perceptions of own and other family members' health status, including the probability of being infected with HIV, may often be inaccurate (Delavande and Kohler 2009; Anglewicz and Kohler 2009). Empirical evidence from Malawi, for example, suggests that in the presence of the HIV/AIDS epidemic, prime-aged adults perceive their own mortality risks not only to be high, but higher than might be expected based on measured mortality rates (Delavande and Kohler 2009). Arguably, such pessimistic subjective survival expectations may importantly affect intergenerational transfer patterns because they diminish the respondent's perceptions of future life expectancies, earnings and consumption.7 It is therefore possible that the response of transfer patterns to the changing health and social conditions as a result of HIV/AIDS epidemic are suboptimal.
In summary, therefore, there is a considerable need for research on intergenerational support networks and transfers to better understand the mechanisms through which extended families cope with the epidemic and potentially alleviate some of its consequences, and to comprehend how transfers respond—or not—to perceptions about own and other family members' health. Our analyses make an important contribution to this emerging literature on intergenerational relations in SSA in the context of HIV by drawing on innovative and rich new data collection from rural Malawi that includes extensive information on intergenerational transfer relations across three generations living in a context characterized by high poverty, and high morbidity and mortality. Specifically, we describe the age patterns of transfers and the multiple directions in which financial and non-financial transfers flow—from prime-aged respondents to their elderly parents and vice versa, and also between the respondents and their co-resident and non-coresident adult children above age 15. In addition, we investigate to which extent these transfer flows are related to the health status and other socioeconomic characteristics of the transfer providers and transfer recipients. Moreover, we approximate the extent to which these transfers result in an intergenerational redistribution of resources, as compared to mutual assistance across generations that results in balanced resource flows in both directions. While most of the prior research on transfers has focused on dyads and specifically the exchanges between an older parent and one randomly selected adult child (Wong, Kitayama, and Soldo 1999), an innovation of our analysis is that we take a multi-generational perspective by describing intergenerational transfer patterns that involve individuals aged 20–60 years (i.e., the primary respondents in our data), their elderly parents and their adult children aged 15 and above. In addition, a noteworthy aspect of our analyses is that we include both co-resident and non-coresident parents and children.8 This aspect of our analysis is of particular importance because adult children who co-reside with their parents may have different motivations and obligations for the provision of transfers than their non-coresiding siblings, and the decision to co-reside is likely to depend on parental preferences as well as their health status (Stecklov 1999; Agree et al. 2002).
In light of the current gaps in the literature, several new findings emerge from the analyses in this paper: First, intergenerational financial and non-financial transfers are widespread and a key characteristic of family relationships in rural Malawi. Second, downward and upward transfers are importantly constrained and determined by the availability of transfer partners (parents or adult children): conditional on parents being alive, financial transfers from prime-aged individuals to their parents are widespread and do not follow a strong age pattern, despite the fact that there is a marked decline of parental health among older prime-aged respondents. From a life-cycle perspective for the overall sample, however, the transfers from respondents to parents are strongly age-patterned with a decline in their frequency with age as the probability of having living parents diminishes with respondent's age. Our data show that downward transfers to the respondents from their elderly parents are less common than upward transfers, and if they occur, they are concentrated at early adult ages (20–30 years) rather than the later adult ages (30–35 years) when AIDS-related morbidity is more likely to occur. Third, while a large fraction of males and females at ages 40–60 provided to and received transfers from their living adult children—with the provision of transfers to children dominating at early adult ages and the receipt of transfers from children rising at later adult ages—only a relatively small number of children seems to be engaged in these transfers. Fourth, our analyses of net transfer flows between respondents and their parents/children indicate that non-financial assistance is relatively unimportant in terms of resource reallocation between generations, despite the fact that there is extensive—and also in some cases age-patterned—mutual non-financial help across the generations. Net financial transfers to both children and parents are, in contrast, strongly age-patterned and peak in mid-to-late adult ages: both male and female respondents age 40–45 in our data provide substantial upward transfers to their parents (possibly more extensive for female than for male respondents), and at the same time, they make substantial downward transfers to their living adult children (possibly more extensive for male than for female respondents). Fifth, multivariate analyses of transfers between respondents and their elderly parents suggest that, quite surprisingly in light of the existing literature, transfers do not strongly vary by the respondent's or the parents' health status including HIV positive status and perception of HIV risk. These transfers, however, do vary with respondent's wealth and in some cases education. They differ across regions, and they are positively associated with the transfers (giving and receiving) to and from adult children age 15 and up. Sixth, transfers between respondents and their adult children are strongly associated with the adult children's age and sex composition, and they are positively associated with the transfer patterns between the respondents and their elderly parents. Similar to the transfer patterns between the respondents and their elderly parents, financial and non-financial transfers from respondents to children do not vary significantly by the health status of the respondents or that of their living adult children.
2. Data and descriptive statistics
Data used in this analysis are from the Malawi Longitudinal Study of Families and Health (MLSFH; formerly, Malawi Diffusion and Ideational Change Project, MDICP), a longitudinal panel survey with survey waves in 1998, 2001, 2004, 2006, 2008 and 2010 that is currently focused on studying the mechanisms that individuals, families, households, and communities develop and use in a poor rural setting to cope with the impact of high morbidity and mortality in their immediate living environment. The MLSFH is implemented in three sites in rural Malawi: Rumphi (in the northern region), Mchinji (in the central region), and Balaka (in the southern region).9 The project started in 1998 with a sample of 1,541 women ever having been married aged 15–49 and 1,065 of their spouses. In 2001, respondents were re-interviewed, along with any new spouses since 1998. In 2004, the study added two new components to the data-collection: a new additional sample of approximately 1,500 adolescents, and free HIV testing and a voluntary counseling on the HIV test results for all respondents. The MLSFH returned for a fourth wave of survey data collection and a second round of HIV testing in 2006, and it was followed-up in 2008 and 2010 by two additional rounds of wide-ranging survey data, including the collection of the extensive transfer data used in this analysis.
Table 1 summarizes demographic and socioeconomic characteristics for the MLSFH respondents in 2008, the MLSFH round on which the present analysis is based. The sample is comprised of 1,839 female respondents and 1,303 male respondents 20 to 60 years old in 2008.10 The mean age of female respondents is 36.5 years, while male respondents are on average one year older. Men are on average better educated than women. For instance, only 13% of male respondents have no formal schooling, while twice as many women fall into this category. 21% of men have secondary or higher level of schooling, but only 8.6% of women have completed this level of schooling. The largest fraction of respondents rated their health status as good, very good or excellent, and only 6% of women and 2% of men rated their health status as poor or very poor. In response to questions about their subjective probability of being infected with HIV, the majority of men (55%) and about half of the women (47%) responded that there is some likelihood of being infected. About one third of both sexes rates this likelihood as low, and only 5% of men and 9% of women rated the likelihood of being HIV positive as high.11 Based on HIV test results, 8% of female respondents and 4% of male respondents were HIV positive.12
Table 1.
Descriptive statistics for respondents aged 20–60 (in 2008)
| Mean (std. dev.) | Females | Males | Total |
|---|---|---|---|
| # of observations | 1839 | 1303 | 3142 |
| Age (in years, 2008) | 36.5 (11.4) | 37.6 (12.0) | 37.0 (11.6) |
| Age (proportion in 5yr age groups, 2008) | |||
| ≤ 25 | 0.22 | 0.21 | 0.22 |
| 26 – 30 | 0.15 | 0.15 | 0.15 |
| 31 – 35 | 0.13 | 0.10 | 0.12 |
| 36 – 40 | 0.14 | 0.13 | 0.14 |
| 41 – 45 | 0.12 | 0.10 | 0.11 |
| 46 – 50 | 0.09 | 0.11 | 0.10 |
| 51 – 55 | 0.08 | 0.09 | 0.09 |
| 56 – 60 | 0.07 | 0.10 | 0.08 |
| Schooling attainment (proportion) | |||
| No school | 0.29 | 0.13 | 0.22 |
| Primary level | 0.63 | 0.66 | 0.64 |
| Secondary level | 0.09 | 0.21 | 0.14 |
| Subjective health (proportion) | |||
| Excellent | 0.11 | 0.23 | 0.16 |
| Very good | 0.48 | 0.50 | 0.49 |
| Good | 0.35 | 0.24 | 0.31 |
| Poor | 0.05 | 0.02 | 0.04 |
| Very poor | < 0.01 | < 0.01 | < 0.01 |
| Subj. prob. of being HIV infected (proportion) | |||
| No likelihood | 0.45 | 0.53 | 0.48 |
| Low | 0.33 | 0.30 | 0.32 |
| Medium | 0.14 | 0.12 | 0.13 |
| High | 0.09 | 0.05 | 0.07 |
| Some subj. likelihood of being HIV infected (proportion) | 0.55 | 0.47 | 0.52 |
| HIV+ | 0.08 | 0.04 | 0.06 |
A key innovation of the 2008 data collection was the expansion of the family and transfer information. The 2008 household and family roster includes not only all individuals who currently live in the household, as frequently done in other studies, but it also asked for information about all parents and children, independent of their survival and resident status, including their demographic, socioeconomic characteristics and transfers received and given from the respondent's perspective. In addition, approximately 800 parents of MLSFH respondents were interviewed. The present analysis is based on the 2008 MLSFH data since they provide the most comprehensive and detailed information on transfers and intergenerational relations within the MLSFH.13 In total, 3,850 fathers (1,570 of whom were alive), 3,830 mothers (2,150 of whom were alive), and 22,000 children (16,050 of whom are alive) were listed in the approximately 3,900 household/family rosters that were collected in 2008.
Specifically, for each listed parent or child, MLSFH respondents were asked a set of questions, including: “What is [name's] relationship to you?”, with our analyses focusing on the respondent's parents and adult children. “Is [name] alive? ”For all living parents/children, respondents were asked: (i) “How old is [name]?”, with children above age 15 considered as “adults” in our analyses; (ii) “Where does [name] usually live?”, where we classify parents or children living in the same household or compound as the respondent as co-resident; (iii) “How would you rate [name's] health in general?”, with response categories including excellent, very good, good, poor, very poor. Because few respondents used poor or very poor to describe the health of their children or parents, which is similar to the response pattern for the respondents themselves (see Table 1), these categories were further collapsed in our analyses into excellent health, good health, and very poor, poor or good health; and (iv) “What is the highest level of schooling [name] has attended?”, from which we establish whether respondents have completed less than primary schooling, primary schooling, secondary schooling or more.
Since the quantitative measurement of transfers in contexts such as Malawi is inherently difficult, the MLSFH did not attempt to monetize the financial and non-financial transfers between respondents and their children or parents. Instead, for all living parents and children above age 15, MLSFH respondents were asked a set of questions about financial and non-financial assistance during the last two years, including: (i) “In the past two years, have you given [name] any money or financial assistance?”, with responses ranging from: 0 = no; 1 = yes, a little; 2 = yes, some; and 3 = yes, a lot; (ii) “In the past two years, have you given [name] any non-financial help? This could include help that takes time like collecting firewood, cooking, taking care of people, or helping with farming.”, with responses ranging from 0 = no; 1 = yes, once; 2 = yes, several times a year; 3 = yes, at least once a month; 4 = yes, at least once a week; and 5 = Yes, daily; (iii) “In the past two years, has [name] given you any money or financial assistance?”, with responses ranging from: 0 = no; 1 = yes, a little; 2 = yes, some; and 3 = yes, a lot; and (iv) “In the past two years, has [name] given you any non-financial help? This could include help that takes time like collecting firewood, cooking, taking care of people, or helping with farming.”, with responses ranging from 0 = no; 1 = yes, once; 2 = yes, several times per year; 3 = yes, at least once a month; 4 = yes, at least once per week; and 5 = yes, daily.
For each of the above questions about financial or non-financial transfers among respondents and their parents or children 15 years old and older, a further binary variable was created that indicates whether a respondent has given or has received a substantial amount of transfers, defined as either “2 = yes, some and 3 = yes, a lot” for financial transfers and “3 = yes, at least once a month; 4 = yes, at least once per week; and 5 = yes, daily” for non-financial transfers.
Table 2 presents descriptive statistics for the survival and health of the respondent's parents, and the transfers that the respondent gave to and/or received from his/her parents during the two years prior to the survey. More than 60% of female and male respondents have living mothers, but only 45% of respondents have living fathers. The mean age of mothers is about 60 years (if alive), while fathers are about 4 years older. Mothers are on average about 25–26 and fathers are about 32 years older than the respondents. About 13–15% of living mothers, and 15–17% of living fathers are assessed by the respondents as being in excellent health, and 57% of mothers and 51–52% of fathers are described as being in very poor, poor or good health. Transfer patterns also vary by sex of the parents. Both male and female respondents are more likely to have given money or help to their mothers than to their fathers during the past two years. For instance, 43% of female respondents and 22% of male respondents stated that they have not given any financial assistance to their fathers, as compared to 24% and 14% respectively to their mothers. 12% of female respondents and twice as many male respondents give a lot of financial support to their mothers, but only 7% of female and 18% of male respondents gave a lot of financial assistance to their fathers.
Table 2.
Descriptive statistics for transfer patterns between respondents aged 20–60 and their parents in 2008
| Mean (std. dev.) | Females | Males | Total | |||
|---|---|---|---|---|---|---|
| Mother | Father | Mother | Father | Mother | Father | |
| Parent Survival and Health | ||||||
| Mother/father is alive | 0.64 | 0.46 | 0.63 | 0.45 | 0.63 | 0.45 |
| If mother/father is alive: | ||||||
| Mean age of mother/father | 59.5 (13.1) | 63.4 (12.6) | 59.0 (13.8) | 63.9 (12.4) | 59.3 (13.4) | 63.6 (12.5) |
| Age diff. between mother/father and respondent | 26.1 (9.75) | 31.9 (10.3) | 24.9 (10.3) | 31.8 (9.99) | 25.6 (9.99) | 31.8 (10.1) |
| Mother/father is in excellent health | 0.13 | 0.15 | 0.15 | 0.17 | 0.14 | 0.16 |
| Mother/father is in very poor/poor/good health | 0.57 | 0.52 | 0.57 | 0.51 | 0.57 | 0.52 |
| Transfers to or from living parents during past 2 years | ||||||
| R has given money or financial assistance | ||||||
| No | 0.24 | 0.43 | 0.14 | 0.22 | 0.20 | 0.34 |
| Yes, a little | 0.36 | 0.30 | 0.27 | 0.27 | 0.32 | 0.29 |
| Yes, some | 0.28 | 0.20 | 0.35 | 0.32 | 0.31 | 0.25 |
| yes, a lot | 0.12 | 0.07 | 0.24 | 0.18 | 0.17 | 0.12 |
| R has given non-financial help | ||||||
| No | 0.11 | 0.28 | 0.12 | 0.21 | 0.12 | 0.25 |
| Yes, once | 0.07 | 0.07 | 0.10 | 0.09 | 0.08 | 0.08 |
| Yes, several times per year | 0.45 | 0.39 | 0.51 | 0.48 | 0.48 | 0.43 |
| Yes, at least once per month | 0.13 | 0.12 | 0.10 | 0.10 | 0.11 | 0.11 |
| Yes, at least once per week | 0.14 | 0.08 | 0.11 | 0.09 | 0.13 | 0.08 |
| Yes, daily | 0.10 | 0.06 | 0.07 | 0.04 | 0.08 | 0.05 |
| R has received money or financial assistance | ||||||
| No | 0.51 | 0.51 | 0.56 | 0.50 | 0.53 | 0.51 |
| Yes, a little | 0.27 | 0.22 | 0.25 | 0.19 | 0.26 | 0.21 |
| Yes, some | 0.16 | 0.17 | 0.11 | 0.15 | 0.14 | 0.16 |
| yes, a lot | 0.07 | 0.10 | 0.08 | 0.15 | 0.08 | 0.12 |
| R has received non-financial help | ||||||
| No | 0.34 | 0.56 | 0.29 | 0.46 | 0.32 | 0.52 |
| Yes, once | 0.09 | 0.09 | 0.08 | 0.08 | 0.09 | 0.08 |
| Yes, several times per year | 0.36 | 0.25 | 0.37 | 0.30 | 0.36 | 0.27 |
| Yes, at least once per month | 0.11 | 0.06 | 0.08 | 0.07 | 0.10 | 0.06 |
| Yes, at least once per week | 0.06 | 0.03 | 0.08 | 0.06 | 0.07 | 0.04 |
| Yes, daily | 0.05 | 0.02 | 0.10 | 0.04 | 0.07 | 0.02 |
| Summary measures of transfers to or from living parents during past 2 years | ||||||
| R has given substantial amount of financial assistance | 0.40 | 0.27 | 0.59 | 0.50 | 0.48 | 0.37 |
| R has given substantial amount of non-financial help | 0.36 | 0.25 | 0.27 | 0.22 | 0.32 | 0.24 |
| R has received substantial amount of financial assistance | 0.23 | 0.27 | 0.20 | 0.31 | 0.21 | 0.29 |
| R has received substantial amount of non-financial help | 0.21 | 0.11 | 0.26 | 0.16 | 0.23 | 0.13 |
While most respondents gave some assistance to their parents, half of the respondents have not received any financial assistance from their parents during the last two years. The summary measures of transfers shown in the bottom of Table 2 suggest that fathers had been more likely to support their prime-aged adult children financially during the past two years than mothers, with slightly more male than female respondents (31% versus 27%) having received a substantial amount of financial help from their fathers. In contrast, mothers were more likely to provide non-financial support than fathers, and female respondents benefited somewhat more than male respondents from these non-financial transfers.
Descriptive statistics for transfers between respondents 30–60 years old and their children are shown in Table 3.14 Female respondents in our sample have on average 6.7 children ever born, and male respondents have 7.1 ever-born children. The number of living children is lower, about 4.9 children for women and 5.6 children for men. Female and male respondents have on average around 2.5 living adult children above age 15. The number of adult children among respondents with at least one alive child 15 or more years old is higher, and these respondents have on average more than 3 adult children with a mean age of about 22 years. Both men and women have more living adult daughters than sons. Not surprisingly, many adult children do not reside in the same household or compound as the respondent (=parent), and the mean number of co-residing adult children is slightly higher for female respondents than for males (1.64 and 1.47 respectively). Less than one half of the respondent's living adult children were reported to be in excellent health status, and about one fifth of adult children were reported to be in very poor, poor or good health.
Table 3.
Descriptive statistics for transfer patterns between respondents aged 30–60 and and their children aged 15+ in 2008
| Mean (std. dev.) | Female | Male | Total |
|---|---|---|---|
| Children | |||
| # of children (alive and deceased) | 6.66 (2.81) | 7.14 (3.38) | 6.86 (3.07) |
| # of living children | 4.91 (2.09) | 5.59 (2.63) | 5.19 (2.35) |
| # of living adult children | 2.58 (2.27) | 2.33 (2.54) | 2.48 (2.39) |
| Among respondents with at least one living adult child | |||
| # of living adult children | 3.35 (2.02) | 3.66 (2.30) | 3.46 (2.13) |
| Mean age of living adult children | 22.7 (6.62) | 22.3 (7.02) | 22.6 (6.77) |
| Sex ratio (# of sons / # of daughters) among living adult children | .92 | .95 | .93 |
| # of adult children who are coresident (same household or compound) | 1.64 (1.36) | 1.47 (1.46) | 1.58 (1.40) |
| in excellent health | 1.31 (1.66) | 1.46 (1.93) | 1.37 (1.76) |
| in very poor, poor or good health | 0.73 (1.33) | 0.84 (1.56) | 0.77 (1.42) |
| Transfers to/from children during past two years (Among respondents with at least one living adult child) | |||
| # of living adult children to whom respondent has | |||
| given substantial amount of financial assistance | 1.16 (1.34) | 1.48 (1.54) | 1.28 (1.42) |
| given substantial amount of non-financial help | 1.08 (1.26) | 0.70 (1.26) | 0.94 (1.28) |
| # of living adult children from whom respondent has | |||
| received substantial amount of financial assistance | 1.15 (1.51) | 0.81 (1.32) | 1.03 (1.45) |
| received substantial amount of non-financial help | 0.98 (1.27) | 0.81 (1.25) | 0.92 (1.26) |
| Sex ratio (# of sons / # of daughters) among children to whom respondent has | |||
| given substantial amount of financial assistance | 1.05 | 1.09 | 1.07 |
| given substantial amount of non-financial help | 1.09 | 1.36 | 1.15 |
| Sex ratio (# of sons / # of daughters) among children from whom respondent has | |||
| received substantial amount of financial assistance | .95 | 1.41 | 1.06 |
| received substantial amount of non-financial help | .72 | .93 | .78 |
Table 3 also reveals that received and given financial and non-financial transfers during the last two years were concentrated between respondents and mostly one child on average. For instance, substantial financial help was given on average only to slightly more than one child (1.16 children for female and 1.48 children for male respondents). Female respondents provided non-financial help to about the same number of children, whereas male respondents provided non-financial help to fewer children than the number of children to whom they provided financial assistance. However, the basic pattern for received financial and non-financial help from children to respondents is very similar: during the past two years, both types of transfers were primarily given by the respondent to a small number of children (often only one). Similarly, respondents received substantial amounts of financial or non-financial assistance from just one child during the past two years. Separating the transfer patterns by gender of the respondent's children furthermore reveals that both male and female respondents provide more financial transfers to their sons than to their daughters. Specifically, the sex ratio of number of sons to number of daughters among adult children with whom the respondent has exchanged transfers shows that parents give substantial amounts of financial help to 5–10% more sons than daughters, which is striking, given the fact that they report to have 4–10% fewer sons than daughters. Respondents also tend to give non-financial help more to sons than daughters, and this is particularly the case for male respondents. Male respondents also tend to receive financial assistance more from sons than daughters, whereas non-financial help—especially for females—is more often provided by daughters.
In summary, the descriptive statistics in Table 3 about transfer patterns between respondents and their adult children during the two years preceding the survey reveal several intriguing patterns: First, on average financial and non-financial transfers of large amounts did not occur between parents and multiple children, but they were mostly concentrated among parents and a small number of children (and often one child). Second, respondents tended to transfer more to their sons, which is striking given the fact that they report having more daughters than sons in the household/family rosters. In addition, there is a clear pattern of an alignment of transfers by gender: male respondents gave considerably more non-financial help to their sons than daughters, and sons were much more likely than daughters to provide financial assistance to their fathers.
3. Age patterns of intergenerational transfers in rural Malawi
3.1 Family structure and health
To provide the demographic context in which intergenerational transfers occur, we begin our analysis with a description of the family composition in rural Malawi. Specifically, we focus on the number of children and living parents respondents have and how these numbers change with respondent's age. The left panel of Figure 1 shows the mean number of children ever born, children living, children below age 15 and adult children above age 15 by age of female respondents, and the right panel shows the same information for male respondents. The observed means of number of children in 5-years age intervals are shown by the dots, and the lines are estimated by using a local polynomial regression fitting procedure from the individual-level data.15 With very few exceptions, we find similar patterns for male and female respondents. At age 20, female respondents have on average less than 2 children, but the number of children increases with age, and at age 60 female respondents report on average more than 8 children ever born. The difference between children ever born and surviving children increases sharply with age. At age 50, for example, female respondents have on average 7.8 children ever born, of whom approximately 70% were alive at the time of the interview. The mean number of living children below age 15 is highest around age 30 (about 3 children) and declines with age, while the number of older children 15 and up years increases with age. At age 20 almost none of the male respondents have children, but by age 60 they have on average about 9.5 children ever born. The higher number of children for men is likely due to the fact that about 7% of men in the sample are in polygamous unions, and unmarried men are underrepresented in the MLSFH sample at older ages.16 By age 50 the difference between children ever-born and children alive is about 2. The mean number of alive young children (aged < 15) is highest at age 35–40 for men, which is about 5 years later than for women.17
Figure 1.
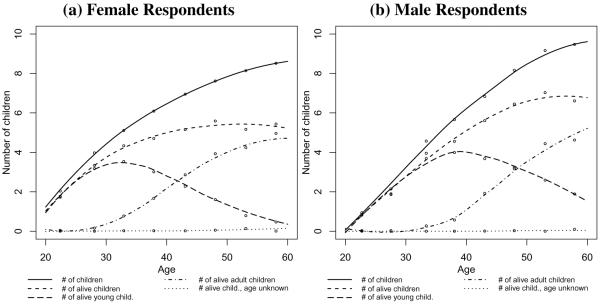
Children of respondents, by respondent's age and gender: Number of children ever born, living children, living young children (age < 15), living adult children (age ≥ 15), and living children of unknown age
Figure 2 shows the proportion of female and male respondents with living parents, by age of the respondent. The pattern is strikingly similar for both male and female respondents. About 83–94% of men and women in the age range 20–30 years report having at least one parent alive. 72–91% of respondents below age 30 have alive mothers, while the proportion of those with an alive father in this young age range is lower (56–74%), which reflects higher male mortality and that husbands tend to be older than their wives. The probability of having living parents declines with age, and at age 60 only about 26–29% of respondents report having at least one parent alive, but a much smaller fraction (about 2–6%) of elderly respondents have both parents alive. In addition, to allow for the assessment of data quality, both panels present information on surviving biological parents that was elicited outside the family/household roster in a separate part of the questionnaire. The two dashed gray lines referring to biological parents and mother or father in general are almost identical with the survival lines for mothers or fathers obtained from the household/family roster, which suggests that respondents primarily list their biological parents when asked about “parents” in the household roster and that they provide information about parents consistent across different parts of the questionnaire and question formats. More importantly, this implies also that the transfer behavior from the respondent's perspective described later in the paper occurs in most instances among biological children and parents. In addition, calculations from our data show that around 3/4 of female respondents around age 30 do not co-reside with their mother, and this probability declines with the respondent's age as a result of the lower probability of having an alive mother. Conditional on the mother being alive, the probability of female respondents aged 30 and up residing with the mother is relatively constant around 35%.18 Coresidence with fathers is less common, which is to a substantial extent related to the lower probability of fathers being alive, but is also the case for respondents whose father is alive. For example, around age 30, only 10% of female respondents coreside with their fathers in the same household or compound, and this probability declines with age; conditional on the father being alive, around 17–19% of female respondents aged 30–40 coreside with their fathers.
Figure 2.
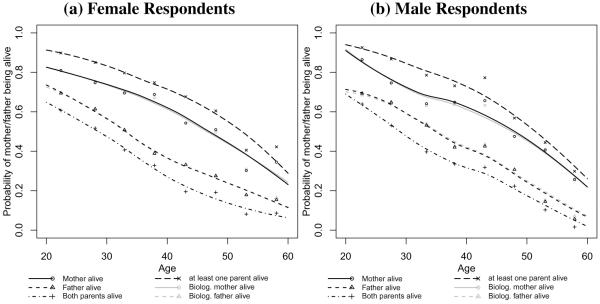
Survival of respondent's parents, by respondent age and gender: Probability of mother being alive, father being alive, both parents being alive, at least one parent being alive, biological mother being alive, and biological father being alive
The perceived health of alive parents declines strongly with the respondent's age. For example, in Figure 3 we show the probability that the mother or the father is perceived to be in excellent health or in very poor/poor/good health, conditional on the mother or the father being alive (broken lines) and in the overall sample (full lines). An “excellent” perceived health status among the parents occurs primarily at the lower end of the respondent's age range, and as respondents age, their perceived parental health declines. For mothers (Figure 3a,c), for example, we observe: conditional on the mother being alive, a relatively poor health assessment (defined as very poor/poor/good health status) increases from about 40–45% at age 20 to about 75% at age 60. Because of the declining probabilities of parents being alive however, in the overall sample this poor health status is relatively constant at around 35–40% up to about age 45, and at older respondent ages it decreases rapidly. Based on the overall sample, at age 60, less than 20% of respondents have a mother in relatively poor perceived health and virtually no respondents have parents in excellent perceived health status. These probabilities are even smaller for fathers. In summary, Figure 3 suggests that the probability of having dependent parents because of perceived poor health status peaks relatively early in adulthood around respondent's ages 30–40, and decreases substantially with age because of high parental mortality in rural Malawi.
Figure 3.

Parental health, by respondent's age and gender: Probability that mother or father is in (1) excellent health or in (2) very poor/poor/good health, conditional on mother or father being alive and in the overall sample
3.2 Age patterns of given and received transfers between respondents and their parents
We begin our analyses of intergenerational transfers by investigating the age profile of transfer flows between respondents and their parents. In particular, we draw on the responses to the household/family roster questions on financial and non-financial transfers (see above) that list a parent as a recipient or provider of transfers. Since we are primarily interested in regular—rather than occasional—transfers among respondents and parents, we focus on the indicator of whether the respondent has given or received a substantial amount of financial or non-financial transfers in the two years prior to the survey. Because the survival of parents is an important determinant of whether the respondent can receive from, or give transfers to his or her mother or father, we show in the subsequent figures (i) the transfer patterns conditional on the respondent's mother or father being alive (in the text, we refer to this type of transfers as 'conditional transfers'), and (ii) the transfer patterns for the entire sample, unconditional on parental survival (in the text, we refer to this type of transfers as 'unconditional transfers'). The latter is useful to assess the contribution of parental survival to transfers with parents at different stages of a respondent's life-course. For example, the fact that a respondent did not receive transfers from his or her mother can be due to the fact the respondent's mother is deceased, or that the respondent did not receive transfers from the mother despite the fact that the mother is alive.
The comparison between the conditional and unconditional transfers is important since it reflects the contribution of parental survival to the observed transfer patterns.
The two upper panels in Figure 4 show the age patterns of financial and non-financial transfers made by female respondents aged 20 years and older to their mothers and fathers separately, and the two bottom panels show the patterns of transfers observed for male respondents. Conditional on the mother being alive, surprisingly, neither financial nor non-financial transfers follow a strong age pattern (Figure 4a): around 35–45% make financial transfers to a living mother across all ages, and about 30–40% gave non-financial help to a living mother. A declining probability of having a living mother for older female respondents, however, causes a strong age pattern in the unconditional transfers with the mother, and after age 35, the probabilities of having made financial or non-financial transfers to the mother declines rapidly. While female respondents are less likely to made financial or non-financial transfers to their fathers as compared to their mothers (Figure 4b), the broad age-patterns are similar: conditional on the father being alive, there is only a modest age pattern in the fraction of respondents who have made financial or nonfinancial transfers, and the unconditional transfer pattern declines strongly with age due to the reduced probabilities of respondents having a living father at older ages.
Figure 4.

Financial and non-financial transfers to mother and father, by respondent's age and gender: Probability that respondent has given “substantial amount” of financial/non-financial transfers to mother or father, conditional on mother/father being alive (broken lines) and in the overall sample (full lines)
Conditional on the mother being alive, male respondents were fairly likely (at most ages, between 50–70%) of having given financial help to their mothers (Figure 4c). Unconditional on parental survival, the fraction of respondents who do so declines strongly with age, especially after age 35, due to reduced probability of having a living mother. Male respondents are less likely to have given non-financial help than financial assistance to their mothers, and they are less likely to have done so as compared to female respondents. Male respondents' transfers to their fathers (Figure 4d) are also characterized by relatively high probabilities of having made financial transfers, conditional on the father being alive, and a declining proportion of male respondents at older ages who have given financial help to fathers due to the reduced paternal survival probabilities. Male respondents are also less likely to have given non-financial help to their fathers as compared to financial help.
An important dimension of Figure 4 is the large discrepancy between conditional and unconditional transfers to parents. In particular, the unconditional probabilities for transfers of both types to parents are substantially lower than the ones observed conditional on having alive parents. Due to the lower probabilities of having living parents for older respondents, the fraction of respondents giving any type of help to elderly parents decreases with age, especially after age 40. For instance, about 27–29% of female respondents aged 30–40 gave substantial amounts of financial assistance to their mothers, a probability that declines to less than 10% at age 60.
Because respondents, particularly at older ages, are less likely to have a surviving father as compared to a surviving mother, only 11–15% of female respondents aged 30–40 gave substantial amounts of financial assistance to their fathers, and at age 60, less than 5% of female respondents did so. These broad age-patterns of financial transfers to parents for male respondents are similar to those for female respondents, although the level—both conditional on parents being alive and unconditional—tend to have been higher for male respondents than for female respondents. Also, at almost all ages and both conditional on parental survival and not, male respondents provided less non-financial help to their parents than female respondents.
In Figure 5 we show the transfer patterns from the parents to the respondents, conditional on the mother or father being alive and for the overall sample. Even at relatively young adult ages, the conditional and unconditional probabilities of having received transfers from parents are not large, despite the fact that young respondents are fairly likely to have living parents (see Figure 2 for the survival probabilities). For example, considerably less than 50% of the respondents in their 20s received financial and non-financial transfers from their parents, and the unconditional probabilities of having received transfers decline markedly with age, especially for respondents aged 20–40. Very few respondents aged 40 and over received transfers from their parents. What is striking is that this basic pattern holds even if we make it conditional on parental survival: over much of respondent's age range, the probability of having received financial assistance from mother or father declines with age even among respondents whose mother or father is still alive. This is also true for non-financial help from parents to female respondents, whereas the conditional transfer pattern to parents for male respondents is less regular (potentially due to the small number of observations). In summary, therefore, financial and non-financial transfers from parents to respondents occurred primarily at relatively young adult ages, and they became less common for older respondents. Respondents older than 40 years received only very limited financial/non-financial support from their parents, which is a function of both survival probabilities of parents and transfer behaviors conditional on parents being alive.
Figure 5.

Financial and non-financial transfers from mother or father, by respondent's age and gender: Probability that respondent has received “substantial amount” of financial/non-financial transfers from mother or father, conditional on mother/father being alive (broken lines) and in the overall sample (full lines)
In Figure 6 we estimate the age pattern of net transfers to the respondent's parents. Under the assumption that the categorical description “a substantial amount of financial assistance” reflects an approximately equal amount of transfers when a respondent describes the transfers given to and received from one particular parent,19 we can use it to approximate the net transfers between the respondent and a particular parent. For this purpose, we construct a variable net transfer to mother (or father) as follows: it equals one (1) if the respondent has given a substantial amount of financial assistance to his or her mother (father) and received from her (him) little or no financial assistance in the last two years; it equals zero (0) if the respondent has given a substantial amount of financial assistance to his or her mother (father) and has also received a substantial amount of financial assistance from his or her mother (father), and it equals also zero (0) if the respondent has given no or only little financial assistance to his or her mother (father) and has also received little financial transfer from his or her mother (father); and it equals minus one (−1) if the respondent has given no or only a little financial assistance to his or her mother (father), but has received a substantial amount of financial assistance from his or her mother (father). Moreover, to reflect the net resource flows unconditional on the respondent's parents survival, we assign the net transfer variable a value of zero (0) if the respondent's mother or father has deceased. An analogous calculation to approximate the net transfers to a respondent's mother or father is performed for non-financial transfers, using the binary indicator that the respondents has given to, or received from a parent a substantial amount non-financial help (i.e, help with a frequency of “at least once a month/at least once per week”). It is easiest to interpret the resulting measure of net transfers in terms of a net resource flow that is measured in units of substantial amounts of non-financial transfers.
Figure 6.

Net financial and non-financial transfers to mother or father, by respondent's age and gender, conditional on mother/father being alive (broken lines) and in the overall sample (full lines)
Note: See text for the definition and calculation of net transfers.
Figure 6 then plots the average net transfers (financial and non-financial) by respondent's age. Several aspects of these net transfers to mothers or fathers are worth noting. First, as shown in the previous figures, while there are clear age patterns for the gross non-financial transfers (non-financial transfers help given or non-financial transfers help received) for females and to a slightly lesser extent for males, the average non-financial net transfers are relatively low and without any strong age pattern. For example, for female respondents between ages 20–40, there is a net resource flow of .09–.12 of such units from the respondents to her mother and of .06–.10 such unites to her father. At older ages this net resource flow further diminishes, in part because the frequency of transfers declines (see Figures 4–5) and because parents are less likely to be alive. For male respondents, the net non-financial resource flow across all ages are very small.
For financial transfers, the net resource flow in Figure 6 follows a marked age pattern and is not as balanced as for non-financial help. Between female respondents and their mothers, the net financial flow are fairly balanced around age 20, and then rises to a net upward flow—of an average of .16 units of “a substantial amount” of financial assistance—when respondents are in their mid to late 30s. After age 30, the net financial resource flow remains towards the parents, with some marked decline that is only the result of a declining probability of the respondent's mother being alive (Figures 4–5). The net financial transfers between female respondents and their fathers are negative when respondents are in their 20s, indicating an average net resource flow of about .05–.1 units of “a substantial amount” of financial assistance from the father to the respondent; after age 30, the average net resource flow between female respondents and their fathers is very close to zero. This decline of the net resource flow with age is initially the result of a declining probability of fathers making financial transfers to their daughters, and at older ages the result of a declining probability of respondents having a living father (see Figure 5b).
The net transfer flow in Figure 6c,d is larger and more age-patterned for male respondents. Across all ages, there is a net financial transfer from male respondents to their mothers, starting off at about .1 units of “a substantial amount” of financial assistance and peaking at about .33 of such units when respondents are in their mid to late 30s. This increase in the net upward transfer at young ages is primarily driven by the decline in the downward transfers to the respondents from their mothers combined with a fairly constant probability of making upward transfers conditional on the mother being alive (see Figures 4–5), while the decline of the net transfer after age 40 results from the declining probability of respondents having alive mothers. The net financial transfer in Figure 6 between male respondents and their fathers follows a similarly inverted U-shape. At young ages in the early 20s, there is a net resource flow to respondents from their fathers, resulting from a high probability of fathers making downward transfers combined with a more moderate probability of making upward financial transfers. The net transfer flow is towards the father for respondents age 25 and higher, and peaks also in the mid to late 30s at about .18 units of “a substantial amount” of financial assistance; this increase is primarily driven by a declining probability of receiving downward transfers from the father, while male respondents maintain a fairly constant probability of making upward financial transfers conditional on the father being alive (see Figure 4d). The decline of the net transfer towards zero above age 40 is again importantly driven by the declining probability of a respondent having a living father.
In summary, while recognizing the limitations of this approach due to the lack a detailed quantitative measurement of transfers, our analyses in Figure 6 suggest that net non-financial transfers are relatively insignificant across all ages for both male and female respondents. At the respondent's early adult ages, when parents are likely to be alive, there is a fair extent of mutual assistance between respondents and their parents (see Figures 4–5), but in terms of net flows the help given and received are approximately balanced and results in a relatively insignificant re-allocation of resources between generations. In contrast, the net resource flows are both significant and strongly age patterned—following an inverted U-shape—for financial assistance. In particular, male respondents provide significant net upward transfers to their parents (mother and father) in their primary adult ages (30–50 years of age). The increase in the net upward resource flow between male respondents and their parents at young ages is primarily the result of a declining probability of receiving financial assistance from parents, while the decline in the net upward flow after age 40 is primarily the result of declining parental survival (Figures 4–5). The transfers between female respondents and their mothers follow a similar pattern, albeit with a smaller net resource reallocation, while the transfers between female respondents and their fathers are the only ones that are characterized by a net downward transfers to the respondent from their fathers at ages 20–30 that is not followed by a significant net upward transfer at older ages.
3.3 Age patterns of transfers between respondents and their children
As shown in Figure 1, MLSFH respondents themselves have a relatively large number of children, and in addition to transfer interactions with their parents, they have potentially been engaged in a rich set of intergenerational transfer relations with their children. Therefore, it is of interest to investigate the transfer behavior between them and their adult children, especially since transfers to their children are in a way competing with the amount of transfers given to their parents. Our focus is on transfer relationships between respondents and their adult children, who are defined in our analyses as children at least 15 years old. Since virtually no respondents below age 30 have adult children, we restrict this analysis to respondents 30 years old and above. We present results for female re spondents, but the transfer patterns between male respondents and their children are very similar and we summarize them later in this section.
The upper left panel of Figure 7 shows the flow of transfers between respondents and their adult children conditional on a respondent having at least one child 15 and over years old. When in their early 30s, about 50% of female respondents who have at least one living adult child provide substantial amount of financial help to at least one adult child. This fraction increases to more than 60% among respondents age 50, and declines sharply afterward to 40% for respondents around age 60. Non-financial help from respondents to children follows a very similar inverted U-shaped age pattern, and this inverted U-shape of giving financial/non-financial help differs markedly from the age-pattern of receiving financial help.
Figure 7.

Transfers to and from living adult children (LAC) (female respondents)
In particular, while very few respondents receive financial help from their adult children at younger ages, even in the presence of an alive adult child, around 80% of women who have living adult children receive financial transfers from at least one adult child after age 50. In contrast, the fraction of respondents with living adult children who receive non-financial support from at least one adult child is substantially lower. For example, at age 50 and above, on average only 50–57% of female respondents who have living adult children receive substantial non-financial help from at least one of their adult children.
The upper right panel of Figure 7 shows the transfers between respondents and their adult children unconditional on having at least one child 15 and over years old. The graph shows that the proportion of female respondents who have at least one living adult child increases rapidly between ages 30–40, and among female respondents aged 40 and over, almost all (> 90%) have at least one living adult child. Among female respondents in their early 30s, very few female respondents have given financial transfers to adult children, and even fewer received such transfers from their children, primarily because a low proportion of female respondents who have living adult children. The peaks of transfer flows are observed after age 50, when about 60% of respondents give substantial financial help to at least one adult child, and 80% receive substantial amount of financial support from at least one adult child. The age pattern of giving non-financial help follows closely that for financial help, while the probability of receiving of non-financial help rises more gradually with respondent age and levels off around age 50.
The bottom two panels of Figure 7 show the transfer patterns depending on the number of children respondents have. Conditional on having at least one child 15 and over years old, female respondents have on average close to five alive adult children by age 55–60 (lower left panel). The most striking feature revealed in this graph is that although respondents have high numbers of adult children at age 45–50, which is the peak age when transfers to children occur, financial help is given to only a small number of these adult children, on average to only 1.4–1.5 children. By age 55, when the peak for received financial help from children occurs, respondents received on average transfers from 2.2 adult children. Hence, there is a sizable gap between a respondent's number of living adult children, and the number of children to whom a respondent has given, or from whom he/she has received financial transfers during the past two years. This asymmetry between the number of potential transfer partners (number of living adult children) and the number of actual transfer partners also occurs for non-financial transfers, where respondents aged 40–55 gave help to, or received help from about .9–1.3 children on average.
The bottom right panel shows the above transfer patterns unconditional on having at least one alive adult child. The primary difference between this graph and the bottom left panel occurs below age 40, when very few respondents have children age 15 and above and thus almost no transfers are observed.
With few exceptions, the patterns of intergenerational transfers between male respondents and their adult children are very similar to the ones for female respondents. For male respondents we estimate a slightly older age pattern for providing financial help to adult children, the peak of which occurs around respondent's age 55. The peak of received transfers from adult children occurs also at older age, and by age 55–60 male respondents receive help on average from one child which is in contrast to the estimates for female respondents who on average received help from a larger number of children.
Figure 8 summarizes the transfers from respondents to their living adult children (LAC) in terms of net resource flows, following a similar approach as for parents that approximates the net resource flow from the respondent's categorical responses (see previous section). For non-financial transfers, Figure 8 reveals a pattern similar to that observed for transfers between respondents and their parents: despite the fact that the number of LAC varies substantially across a respondent's life course, and that there is a reasonable amount of mutual non-financial help between respondents and their children (Figure 7), the net resource flow as a result of these non-financial transfers seems to be relatively small and there is no marked age pattern for either male or female respondents. In contrast, net resource flows as a result of financial transfers between respondents and their LAC follow a marked age-pattern that indicates important differences in the flow of resources between respondents and their children across the life course. Around age 30, the net transfers to LAC are very small because respondents tend to have a very small number of LAC (conditional on having an LAC, respondents are likely to make a net downward transfers even around age 30; see Figure 7a). At somewhat older ages, for both male and female respondents, a net financial transfer towards children arises. For female respondents, the net financial transfers to children peak at an age around 40 years, and decline thereafter; after age 50, the direction of net transfers changes and female respondents become net recipients of transfers from their children. This net resource flow from children to their mothers (female respondents) is relatively substantial, allocating up 1-unit of “a substantial amount of financial assistance” from children to their mothers at ages 55 and over. For men, we estimate an inverted U-shape with a peak of the net financial transfer flow to children when respondents are about 50 years old. Moreover, in contrast to female respondents, adult children remain recipients of net financial transfers from male respondents until about respondent's age of 60.
Figure 8.

Net transfers (financial and non-financial) to living adult children (LAC)
In summary, while recognizing again the limitations due to the lack of a quantitative measurement of resource flows, our analyses of net transfer flows between respondents and their parents/children in Figures 6 and 8 point to some important patterns: first, in terms of resource allocation between generations, non-financial assistance is relatively unimportant despite the fact that there is extensive—and also sometimes age-patterned—mutual non-financial help across the generations. Second, financial transfers to both children and parents are strongly age-patterned and peak in mid-to-late adult ages: both male and female respondents age 40–45 provide substantial upward transfers to their parents (possibly more extensive for female than for male respondents), and at the same time, they make substantial downward transfers to their LAC (possibly more extensive for male than for female respondents).
4. Correlates of transfer patterns to/with parents
In this section, we investigate the correlates of financial and non-financial transfer patterns between respondents and their parents. Because of the limited information about intergenerational transfer patterns in the sub-Saharan African context we focus here on descriptive analyses that identify the main correlates of intergenerational transfers in the context of rural Malawi, and we do not attempt to identify causal relationships. The regression analyses summarized below are also conditional on the potential transfer partner—respondent's mother or father—being alive, and the analyses thus do not consider the correlates of parental survival or the potential selective nature of respondents whose mother or father was alive in 2008. Despite these limitations, the analyses are useful because they provide for the first time in a sub-Saharan context evidence about the extent to which transfers between individuals and their parents are correlated with respondent's demographic, socioeconomic and health conditions, and with the health of their parents.
Our analyses of the correlates of transfer patterns are based on two sets of models. First, we discuss OLS regressions for the net financial and net non-financial transfers to parents as dependent variables; second, we present corresponding logistic regression analyses for the dependent variables indicating whether a respondent has given or has received a substantial amount of transfers as defined earlier in the data description. To limit the number of analyses that need to be reported, we tested whether the estimated relationships differ between male and female respondents, and between regions. With few exceptions discussed below, the correlates of transfer patterns did not differ by sex of the respondents or the parents, and thus we pooled the regressions for male and female respondents as well as for fathers and mothers. We report in Tables 4–5 the results of these pooled analyses for net financial and non-financial transfers to parents, and additional analyses for providing and receiving financial or non-financial transfers are summarized in the Appendix Tables A.1–A.4.
Table 4.
Pooled analyses: OLS regressions for net financial transfers to parents
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | −0.002 (0.034) | −0.031 (0.035) | −0.030 (0.038) | −0.026 (0.035) | −0.025 (0.040) | −0.022 (0.041) | −0.029 (0.035) | −0.031 (0.034) | −0.029 (0.035) | −0.030 (0.034) |
| Secondary schooling or more | −0.085+ (0.049) | −0.137** (0.050) | −0.136* (0.054) | −0.125* (0.050) | −0.104+ (0.057) | −0.090 (0.059) | −0.122* (0.050) | −0.122* (0.050) | −0.122* (0.050) | −0.121* (0.050) |
| Respondent's wealth quintile | 0.044** (0.009) | 0.037** (0.010) | 0.043** (0.009) | 0.033** (0.011) | 0.031** (0.011) | 0.043** (0.009) | 0.042** (0.009) | 0.043** (0.009) | 0.041** (0.009) | |
| Respondent is HIV+ | 0.008 (0.051) | |||||||||
| Respondent's subj. likelihood of HIV infection† | 0.000 (0.013) | |||||||||
| Respondent's and parent's subjective health | ||||||||||
| Resp. is in very poor/poor/good health | 0.025 (0.030) | 0.017 (0.031) | ||||||||
| Resp. is in excellent health | 0.038 (0.037) | 0.033 (0.038) | ||||||||
| Parent is in very poor/poor/good health | 0.054+ (0.029) | |||||||||
| Parent is in excellent health | −0.003 (0.040) | |||||||||
| Respondent's children | ||||||||||
| # of young living children | 0.023** (0.008) | 0.023** (0.008) | 0.023** (0.008) | 0.022** (0.008) | ||||||
| # of living adult children | 0.004 (0.010) | −0.002 (0.010) | 0.004 (0.010) | −0.002 (0.010) | ||||||
| Total net transfers to living adult children | ||||||||||
| Net financial transfer | 0.034* (0.014) | 0.036** (0.014) | ||||||||
| Net non-financial transfer | −0.016 (0.021) | −0.021 (0.021) | ||||||||
|
| ||||||||||
| Observations | 3325 | 3238 | 2811 | 3177 | 2523 | 2463 | 3238 | 3238 | 3238 | 3238 |
Robust standard errors in parentheses. Standard errors are adjusted for clustering within respondents.
p-values:
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2, coresidence of parent, and region (3 regions). These coefficients are allowed to vary by gender of the respondent and gender of the parent. Analyses are conditional on parent being alive.
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only children who were given or provided substantial amount of financial/non-financial transfers.
Table 5.
Pooled analyses: OLS regressions for net non-financial transfers to parents
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.006 (0.026) | 0.003 (0.026) | −0.018 (0.029) | −0.003 (0.026) | 0.005 (0.031) | 0.002 (0.032) | 0.001 (0.026) | 0.002 (0.026) | 0.002 (0.026) | 0.002 (0.026) |
| Secondary schooling or more | 0.001 (0.035) | −0.007 (0.037) | −0.024 (0.042) | −0.009 (0.037) | −0.015 (0.045) | −0.015 (0.047) | −0.011 (0.037) | −0.011 (0.037) | −0.011 (0.037) | −0.011 (0.037) |
| Respondent's wealth quintile | 0.007 (0.007) | 0.004 (0.007) | 0.008 (0.007) | 0.010 (0.008) | 0.008 (0.008) | 0.007 (0.007) | 0.007 (0.007) | 0.007 (0.007) | 0.007 (0.007) | |
| Respondent is HIV+ | 0.003 (0.037) | |||||||||
| Respondent's subj. likelihood of HIV infection† | 0.014 (0.009) | |||||||||
| Respondent's and parent's subjective health | ||||||||||
| Resp. is in very poor/poor/good health | −0.005 (0.022) | −0.007 (0.022) | ||||||||
| Resp. is in excellent health | 0.000 (0.027) | −0.002 (0.027) | ||||||||
| Parent is in very poor/poor/good health | 0.029 (0.021) | |||||||||
| Parent is in excellent health | 0.017 (0.029) | |||||||||
| Respondent's children | ||||||||||
| # of young living children | −0.001 (0.006) | −0.001 (0.006) | −0.001 (0.006) | −0.001 (0.006) | ||||||
| # of living adult children | −0.011 (0.008) | −0.010 (0.008) | −0.010 (0.007) | −0.009 (0.007) | ||||||
| Total net transfers to living adult children | ||||||||||
| Net financial transfer | −0.006 (0.009) | −0.004 (0.009) | ||||||||
| Net non-financial transfer | −0.020 (0.016) | −0.019 (0.016) | ||||||||
|
| ||||||||||
| Observations | 3324 | 3237 | 2810 | 3176 | 2523 | 2463 | 3237 | 3237 | 3237 | 3237 |
Robust standard errors in parentheses. Standard errors are adjusted for clustering within respondents.
p-values:
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2, coresidence of parent, and region (3 regions). These coefficients are allowed to vary by gender of the respondent and gender of the parent. Analyses are conditional on parent being alive.
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only children who were given or provided substantial amount of financial/non-financial transfers.
In terms of explanatory variables, the particular focus in these analyses is on the associations of transfer patterns with demographic and socioeconomic characteristics of the respondents such as respondent's age, education, and wealth; respondent's and parent's health status, including self-reported health status, actual HIV positive status and self-perception of being infected with HIV; the respondent's number of living young (below age 15) and adult (age 15 and over) children, as well as the total net financial and net non-financial transfers given from and to LAC. Respondent's wealth is measured by the respondent's household wealth quintile (ranging from 1 to 5). HIV positive status is obtained from the most recent HIV test in which a respondent participated. The respondent's subjective likelihood of HIV infection is coded as 0 equals no likelihood, 1 equals some likelihood, 2 equals medium likelihood, and 3 equals high likelihood, while for a respondent's subjective health we created indicators of whether the respondent is in excellent health, in very good heath (reference category), and in very poor or poor or good health. Similar indicators were also created to describe the health of a respondent's mother or father (see also Tables 1–2). In addition to the coefficients shown in Tables 4–5, all analyses control for respondent's age, age squared, co-residence of the parents, and region of residence (north, south, central). The coefficients for these control variables are allowed to vary by sex of the respondents and parents.
The key findings of our analyses about the correlates of transfers between respondents and their parents are as follows (see Tables 4–5 and Appendix Tables A.5–A.8):
Respondent's level of schooling: In general we do not find a strong association between respondent's level of schooling and financial and non-financial transfers given to parents and received from parents. One exception to this pattern is noticeable: contrary to hypotheses expected from the parental repayment hypothesis for intergenerational transfers (Becker and Tomes 1976; Lillard and Willis 1997; Raut and Tran 2005), there tends to be a negative association of secondary schooling with net financial transfers to parents, which is reflected in the fact that respondents with a secondary or higher level of schooling have more than twice the odds of receiving a substantial amount of financial transfers from their parents as opposed to respondents with low level of schooling (Table A.3).
Respondent's wealth quintile: Respondent's wealth quintile is strongly associated with the net financial transfers provided to parents, and wealthier respondents are therefore more likely to be the net providers of financial transfers to parents. This association results from the fact that wealthier respondents are more likely to provide substantial financial assistance to their parents (Table A.1). Respondent's wealth is generally not associated with the net flow of non-financial transfers between respondents and their parents.
Measures of respondent's health status: One of the most intriguing results shown in Tables 4–5 is that measures of respondent's health status—including the respondent's HIV positive status, his/her perception of being infected with HIV, and subjective health—are generally not associated with net financial or net non-financial transfers given to parents.
Measures of parental health status: Parental health status is also not generally associated with the provision of both financial and non-financial transfers between respondents and parents. The only exception to this pattern is a weak association indicating that respondents provide somewhat higher net financial transfers to parents who are in relatively poor health (classified in the analyses as “very poor/poor/good health”), which is due to the fact that parents in relatively poor health are somewhat less likely to provide a substantial amount of transfers to their children (respondents) (Table A.3). An excellent health status of the respondent's parent is associated with a higher probability for the respondent of both receiving and providing a substantial amount of non-financial transfers to his or her parents (Tables A.2 and A.4), resulting in a pattern where the net non-financial flow in Table 5 is not associated with an excellent parental health status.
Presence of, and intergenerational transfers with, respondent's children: Respondents with higher numbers of young children make higher net financial transfers to their parents, which is due to a negative association of the respondent's number of young children with the probability of receiving a substantial number of financial transfers from their parents (Table A.3). The respondent's amount of adult children is not associated with the net or gross financial transfers of the respondent with his or her parents. We also find strong positive association between respondent's making net financial transfers to their parents and their children, which occurs because respondents who make higher net transfers to their children are more likely to provide a substantial amount of financial transfers to their parents.
Coresidence with parents: While we do not report the coefficients indicating the association of net financial or non-financial transfers with coresidence of parents (i.e., mother or father living in the same household or compound as the respondent), we comment briefly on these relationships. Coresidence is important since the transfer questions included in the MLSFH may only partially capture the exchange relations between respondents and their parents if they live in the same household or compound. Our data do not permit us to investigate this possibility in detail. However, while in general there is no association between coresidence and gross or net transfers measured in the MLSFH, some specific associations suggest that the MLSFH survey was able to capture differences in transfer patterns by coresidence. For example, for female respondents, coresidence with the mother is associated with fewer financial transfers to mothers, and with slightly higher levels of non-financial transfers to mothers. Females' financial transfers to fathers are not associated with co-residence of the father, while non-financial transfers have a positive association with coresidence. For male respondents, co-residence with the mother is weakly associated with higher net financial transfers to the mother. In all cases, controlling for the respondent's or parent's health status tends to reduce these associations of coresidence with net transfers, often rendering the associations statistically insignificant.
5. Correlates of transfer patterns to/with adult children
Tables 6–7 provide a corresponding set of analyses describing the net financial and net non-financial transfers of respondents with their living adult children, and the corresponding analyses of the gross transfers with adult children are reported in Appendix Tables A.5–A.8.
Table 6.
Pooled respondents: OLS regressions for the net financial transfers to living adult children (LAC)
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.147 (0.106) | 0.038 (0.109) | 0.032 (0.120) | 0.024 (0.111) | 0.072 (0.124) | 0.066 (0.124) | 0.072 (0.106) | 0.013 (0.108) | 0.032 (0.106) | 0.052 (0.121) |
| Secondary schooling or more | −0.004 (0.235) | −0.207 (0.242) | −0.112 (0.243) | −0.218 (0.249) | −0.065 (0.256) | −0.076 (0.257) | −0.108 (0.242) | −0.256 (0.243) | −0.186 (0.238) | −0.049 (0.251) |
| # of living adult sons | 0.017 (0.051) | −0.002 (0.052) | 0.006 (0.055) | 0.006 (0.053) | 0.013 (0.060) | −0.025 (0.072) | 0.127** (0.049) | 0.030 (0.047) | 0.143** (0.049) | 0.133* (0.063) |
| # of living adult daughters | 0.012 (0.042) | −0.003 (0.042) | 0.014 (0.047) | −0.004 (0.043) | 0.037 (0.046) | −0.012 (0.059) | 0.169** (0.047) | 0.016 (0.041) | 0.175** (0.048) | 0.195** (0.057) |
| Mean age of living adult children (LAC) | −0.053** (0.010) | −0.057** (0.011) | −0.053** (0.011) | −0.058** (0.011) | −0.053** (0.012) | −0.053** (0.012) | −0.052** (0.010) | −0.055** (0.011) | −0.053** (0.010) | −0.051** (0.011) |
| # of alive young children | 0.019 (0.027) | 0.009 (0.027) | 0.013 (0.027) | 0.009 (0.027) | 0.008 (0.027) | 0.005 (0.028) | 0.012 (0.026) | 0.000 (0.027) | 0.003 (0.026) | 0.003 (0.027) |
| Respondent's wealth quintile | 0.177** (0.031) | 0.180** (0.033) | 0.179** (0.032) | 0.167** (0.033) | 0.165** (0.033) | 0.175** (0.031) | 0.173** (0.032) | 0.160** (0.031) | 0.153** (0.033) | |
| Respondent is HIV+ | 0.084 (0.148) | |||||||||
| Respondent's subj. likelihood of HIV infection† | 0.010 (0.043) | |||||||||
| Resp. is in very poor/poor/good health | −0.041 (0.097) | −0.050 (0.096) | −0.002 (0.096) | |||||||
| Resp. is in excellent health | 0.155 (0.135) | 0.162 (0.136) | 0.072 (0.133) | |||||||
| # of LAC who are in very poor/poor/good health | 0.109+ (0.061) | 0.096+ (0.058) | ||||||||
| # of LAC who are in excellent health | 0.040 (0.051) | 0.009 (0.047) | ||||||||
| # of non-coresident LAC | −0.252** (0.049) | −0.234** (0.046) | −0.241** (0.046) | |||||||
| # of parents who are alive | 0.103+ (0.058) | 0.050 (0.058) | 0.028 (0.064) | |||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 0.212** (0.071) | 0.278** (0.076) | ||||||||
| Net non-financial transfer | −0.116 (0.076) | −0.158+ (0.081) | ||||||||
|
| ||||||||||
| Observations | 1472 | 1439 | 1248 | 1409 | 1145 | 1145 | 1439 | 1404 | 1389 | 1105 |
Standard errors in parentheses.
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2 and region (3 regions), and are conditional on the respondent having at least one living adult child (LAC).
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only parents who were given or provided substantial amount of financial/non-financial transfers.
Table 7.
Pooled respondents: OLS regressions for the net non-financial transfers to living adult children (LAC)
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.026 (0.056) | 0.021 (0.060) | 0.010 (0.065) | 0.026 (0.061) | 0.034 (0.068) | 0.034 (0.068) | 0.031 (0.059) | −0.001 (0.060) | 0.004 (0.059) | 0.028 (0.068) |
| Secondary schooling or more | 0.119 (0.133) | 0.099 (0.138) | 0.071 (0.150) | 0.117 (0.141) | 0.063 (0.152) | 0.062 (0.152) | 0.129 (0.138) | 0.085 (0.140) | 0.101 (0.141) | 0.089 (0.155) |
| # of living adult sons | 0.083* (0.032) | 0.081* (0.033) | 0.048 (0.031) | 0.079* (0.034) | 0.053 (0.034) | 0.058 (0.040) | 0.120** (0.032) | 0.085* (0.034) | 0.116** (0.032) | 0.115** (0.040) |
| # of living adult daughters | −0.065* (0.030) | −0.067* (0.031) | −0.072* (0.035) | −0.067* (0.032) | −0.038 (0.029) | −0.034 (0.033) | −0.015 (0.037) | −0.062* (0.031) | −0.017 (0.038) | 0.047 (0.038) |
| Mean age of living adult children (LAC) | −0.010+ (0.005) | −0.012* (0.006) | −0.012* (0.006) | −0.011* (0.006) | −0.008+ (0.005) | −0.008+ (0.005) | −0.010+ (0.005) | −0.011+ (0.006) | −0.010+ (0.006) | −0.006 (0.005) |
| # of alive young children | 0.011 (0.017) | 0.008 (0.017) | 0.003 (0.019) | 0.009 (0.018) | −0.005 (0.020) | −0.004 (0.020) | 0.009 (0.017) | 0.008 (0.017) | 0.006 (0.017) | −0.007 (0.019) |
| Respondent's wealth quintile | 0.011 (0.021) | 0.015 (0.022) | 0.009 (0.021) | 0.011 (0.022) | 0.012 (0.022) | 0.011 (0.021) | 0.008 (0.021) | 0.010 (0.021) | 0.009 (0.022) | |
| Respondent is HIV+ | −0.104 (0.090) | |||||||||
| Respondent's subj. likelihood of HIV infection† | −0.005 (0.026) | |||||||||
| Resp. is in very poor/poor/good health | −0.075 (0.059) | −0.078 (0.059) | −0.065 (0.059) | |||||||
| Resp. is in excellent health | 0.022 (0.101) | 0.022 (0.101) | −0.006 (0.100) | |||||||
| # of LAC who are in very poor/poor/good health | 0.001 (0.037) | −0.010 (0.038) | ||||||||
| # of LAC who are in excellent health | −0.015 (0.030) | −0.022 (0.029) | ||||||||
| # of non-coresident LAC | −0.075* (0.036) | −0.066+ (0.037) | −0.100** (0.034) | |||||||
| # of parents who are alive | −0.020 (0.036) | −0.004 (0.040) | −0.037 (0.043) | |||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | −0.037 (0.047) | 0.024 (0.044) | ||||||||
| Net non-financial transfer | −0.050 (0.057) | −0.090 (0.065) | ||||||||
|
| ||||||||||
| Observations | 1472 | 1439 | 1248 | 1409 | 1145 | 1145 | 1439 | 1404 | 1389 | 1105 |
Standard errors in parentheses.
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2 and region (3 regions), and are conditional on the respondent having at least one living adult child (LAC).
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only parents who were given or provided substantial amount of financial/non-financial transfers.
The dependent variables in Tables 6–7 are the net financial and net non-financial transfers given to living adult children (LAC) aged 15 and over that are calculated as the sum of the gross transfers (having provided and having received substantial amounts of financial/non-financial transfers to/from children; see Section 2 for detailed discussion of the transfer measures included in the data) across all adult children.20 The particular focus of our analyses in Tables 6–7 is on the association of the respondent's net transfers to his or her children with respondent's and adult children's health, respondent's demographic and family characteristics and respondent's transfer patterns with his or her elderly parents. As with the analyses for transfers with parents, we pool respondents by sex since we did not find any sex-specific differences in the transfer behavior between men and women and their children. All of the analyses that focus on transfer patterns with adult children are conditional on the respondent having at least one LAC age 15 and up. The analyses therefore show the extent to which parents who have at least one LAC give transfers to, or receive transfers from, their adult children, and how these transfer patterns vary by respondent's health and socioeconomic or demographic contexts. As a consequence of conditioning on having at least one LAC, our results do not reflect the extent to which these factors affect the probability of having at least one LAC. The results, however, do shed light on the question of whether transfers with children—among respondents who have LAC—do vary by health, wealth or family structure.
Specifically, the explanatory variables in these analyses include: the respondent's number of living adult sons and daughters aged 15 and above, the mean age of LAC, the respondent's number of young living children below age 15; the respondent's wealth (measured by the wealth quintile, coded 1–5), HIV positive status, subjective likelihood of HIV positive infection, and subjective health using indicators of whether the respondent is in excellent health, in very good heath (reference category), and in very poor/poor or good health. The respondent's family or household context is described by: the number of LAC who are in very poor/poor/good health, in excellent health, non-coresident with the respondent (not living in same household or compound); the number of respondent's parents who are alive (coded as zero, one or two), and the net financial and non-financial transfers given to the respondent's parents. In addition, in our models we control for respondent's age, age2, respondent's level of schooling (less than primary schooling, primary schooling, secondary or higher schooling), and region of residence (north, south, central).
The key findings of our analyses in Tables 6–7 are as follows:
Respondent's schooling and wealth: Respondent's level of schooling is not associated with the net financial and non-financial transfers to adult children. Wealthier respondents provide higher net transfers to their adult children, which is due to the fact that they are more likely to provide substantial amount of financial transfers to them (Table A.5); receiving financial transfers from children is not associated with the respondent's wealth. Wealth is also not associated with the net non-financial transfers with adult children, and neither are the underlying patterns of providing or receiving substantial amounts of non-financial help).
Respondent's family composition: A higher number of living adult sons and daughters is generally associated with higher levels of financial and non-financial transfers given to and received from adult children (Tables A.5 and A.7), and as a result, the net financial transfer to children in Table 6 is not much associated with the number of living sons and daughters. The number of living adult sons is in most models in Table A.7 positively associated with the net non-financial transfers to children, whereas there tends to be a negative association between the number of daughters and the net non-financial transfers to children. This pattern occurs because the respondent's giving of non-financial help to children is more strongly associated with the number of sons, where as he respondent's receiving of non-financial help to children is more strongly associated with the number of daughters (Tables A.6 and A.8). The mean age of LAC is negatively associated with the net financial transfers from respondents, which reflects the pattern that respondents provide fewer substantial amounts of financial help to older children and receive more gross financial transfers from older children (Tables A.5 and A.7). Mean age of adult children is negatively associated with the net non-financial help to adult children, although this is not significant in all models. The total number of young living children (i.e., children be low age 15), which possibly compete with adult children for parental time and resources, does not predict net transfer patterns between respondents and their adult children. A larger number of non-co-resident LAC is associated with less net financial transfers to adult children. This pattern is due to the fact that respondents are less likely to provide substantial amounts of financial help to non-coresiding children, and are more likely to receive substantial amounts of financial help from these children. Net financial transfers are also weakly positively correlated with the number of living parents. Net non-financial transfers are negatively correlated with the number of non-co-resident LAC, although less markedly than for financial transfers, while the number of respondent's parents who are alive is generally not associated with the net non-financial transfers between respondents and their LAC.
Measures of respondent's and children's health status: Similar to our findings regarding transfers between respondents and their parents, the net financial and non-financial transfers between respondents and their adult children are generally not associated with the respondent's health status, including the respondent's HIV positive status, perception of HIV infection and self-rated health (and neither are the underlying gross financial or non-financial transfers). There is weak positive association between the number of LAC in relatively poor health and the net financial transfers to LAC.
Presence of, and intergenerational transfers with respondent's parents: Similarly to the results shown for net financial transfers between respondents and their parents, we find a strong positive relationship between respondent's providing net financial transfers to their adult children and their elderly parents. That is, respondents who provide more net financial transfers to their parents are also providing larger net financial transfers to their adult children. This pattern is consistent with an interpretation that some unobserved factors—such as unobserved aspects of wealth, income, health or levels of altruism towards parents or children—affect a respondents provision of transfers to both parents and children, and this pattern is inconsistent with a notion that transfers from parents to the respondents are passed onto the respondent's children with the respondent serving as an “intermediary” in these transfers.
6. Conclusions
Sub-Saharan Africa provides an important and interesting context to investigate patterns of transfers and relationships between generations that is distinguished from other less developed regions through the conjunction of high poverty levels, high morbidity and mortality, and the world's highest HIV/AIDS prevalence. The relevance of these conditions for the well-being of generations is heightened by the absence of institutionalized formal systems that can protect individuals from the consequences of frequently occurring economic, social, environmental and health shocks. As a result, vertical and lateral family support networks are an integral aspect of families in this context that can importantly contribute to the well-being of individuals and that can ameliorate the impact of health or economic shocks or crises. Despite the increasing interest devoted to the well-being of families in the era of generalized HIV/AIDS epidemics and the mechanisms used to cope with the consequences of the epidemic (Section 1) very few studies have investigated transfer behaviors and transfer patterns from a multigenerational perspective in SSA even though the latter are widespread and represent an essential element of support for family members in daily life and in periods of needs. Instead, a large body of prior research has focused on remittances and living arrangements as a form of support, partly due to the paucity of detailed data on kin and transfers outside the immediate household (Davies 2007). Although the household provides the main unit for financial and non-financial transfers, most prior studies have not been able to account for the fact that the family economy extends beyond the household and includes exchanges with non-coresiding kin members, more distant relatives, friends and neighbors. Moreover, prior studies have not taken into account that intergenerational and kin relationships are multi-directional and that transfers occur in multiple forms and currencies; specifically non-financial transfers can be given and received in different forms such as help with household activities, personal care, supervision of small children, etc. If this multi-directionality and multiplicity of transfers is not considered in the analyses, an incomplete and distorted representation of the intergenerational transfers in SSA emerges.
This study overcomes the limitations of existing analyses by using innovative data from rural Malawi that comprises detailed information on intergenerational transfer relationships across three generations extending beyond the immediate household and including information on deceased and non-coresiding family members. By focusing on the transfer relationships between the study participants, their elderly parents and their adult children aged 15 and above, we reflect the multi-directionality of flows and the multiplicity of transfers currencies (i.e., financial and non-financial transfers) and make several important contributions to the existing literature summarized and discuss below.
In our analyses, we address the fact that demographic factors such as fertility and mortality determine the age structure of the population and the availability of potential transfer partners, and thus influence the observed transfer behavior (Wolf 1994; Henretta, Grundy, and Harris 2001). To reflect the role of these important demographic constraints on transfers, we estimated the age patterns of transfers and showed their flows conditional on having transfer partners available (e.g., parents being alive or having adult children) as well as unconditional, from a life-cycle perspective for the overall sample. Our results showed some important differences in these two approaches that are requisite for understanding the transfer behavior and patterns in rural Malawi. For instance, conditional on having living parents, financial transfers from the prime-aged respondents to their elderly parents do not follow a strong age pattern, despite the declining health of the elderly generation with age. From a life-cycle perspective, financial transfers from respondents to their parents are strongly age-patterned and decline substantially with the respondent's age as a result of diminishing probability with age of having living parents. We estimated a similarly large discrepancy between conditional and unconditional non-financial transfers from respondents to their adult children that is importantly related to life-cycle changes in family composition as resulting from fertility and childbearing and parental or child mortality.
Recognizing the limitations of our measurements of net transfer flows in SSA due to the difficulties of monetizing transfers, we present in this paper analyses for both gross and net financial and non-financial transfers between respondents and their parents as well as adult children. Our findings suggest that although there is an extensive and sometimes age-patterned exchange of non-financial help between generations, the average net non-financial transfers are relatively low and without strong age pattern, which suggest the presence of mutual help rather than substantial allocation of non-financial assistance across generations. In striking contrast to this finding, financial transfers are strongly age-patterned and the net financial transfers show a strong allocation of financial resources from the generation of prime-aged respondents to their elderly parents and their adult children. This latter finding questions the results of some existing studies that have suggested that the role of younger and especially elderly individuals in SSA for sustaining the family has dramatically increased in the era of the HIV epidemic since they are providing more transfers and resources to prime-aged adults who are mostly affected by the epidemic (Foster 2000; Cheng and Siankam 2009; Aboderin and Ferreira 2008; Schatz and Ogunmefun 2007; Sagner and Mtatt 1999; Bray 2009; Nyasani, Sterberg, and Smith 2009). In particular, existing studies have often hypothesized that in households where prime-aged adults are affected by HIV/AIDS, younger and especially elderly individuals take upon more financial and non-financial responsibilities. However, by investigating the net transfers flow between respondents and their parents as well as children, our analyses point towards a situation where prime-aged adults are important net providers of financial resources to both adult children and parents in rural Malawi. A major characteristic of these families' relationships is therefore the allocation of financial resources from the middle generation to younger adults and the elderly. From this perspective of the responsibilities they carry within their families, prime-aged adults in SSA seem to be in the position of the “sandwich generations” in developed countries, which has been described as mid-life adults who care concurrently for dependent children and old parents (Grundy and Henretta 2006; Bengtson 2001).
In addition to documenting these age patterns of transfers, we investigate in this paper how transfers depend on the health status of the providers (i.e., the working-age adults who bear the highest health and economic burden of the HIV epidemic) and the recipients (i.e., the respondent's adult children or elderly parents). A surprising finding in these analyses is that financial and non-financial net transfers—and the underlying gross transfers of giving and receiving—are not strongly associated with the health status of the respondents, their adult children and their elderly parents. Moreover, neither net transfers, nor the provision and receipt of transfers, is associated with the respondent's HIV positive status or perception of being infected with HIV. This latter result is particularly surprising since the HIV/AIDS epidemic has increased uncertainty among individuals about their current and future health status and their survival, and as a consequence, one would expect that the high risk disease environment prevailing in rural Malawi and other SSA contexts would have affected transfer motivations and behavior among family members. For example, Delavande and Kohler (2009) have shown that prime-aged adults in rural Malawi perceive their own mortality risks not only to be high, but higher than might be expected based on measured mortality rates, which may translate into overly pessimistic perceptions about future life expectancy, earnings and consumption. The lack of a strong and systematic association of net and gross financial/non-financial transfers with the respondent's health status in our analyses is surprising in this context. It is possibly related to the fact that the study population—like similar populations in SSA—has been exposed to high mortality and high morbidity environment for a considerable period, also predating the HIV/AIDS epidemic, and that the culture, norms and expectations about transfers in a high risk disease environment have been established over a long term and have not yet been fundamentally altered by the AIDS epidemic.
While we did not set out in this paper to test the theories of intergenerational transfers in developing countries (e.g., Willis 1980; Lillard and Willis 1997; Frankenberg, Lillard, and Willis 2002; Becker and Tomes 1976), our findings are nevertheless informative about the motivations for transfers in SSA contexts. For example, one robust finding from the multivariate analyses is the strong positive association between a respondent's net transfers to adult children and net transfers to parents. That is, controlling for current wealth and other socioeconomic and demographic characteristics, respondents who provide higher net transfers to their children are more likely to provide a substantial amount of financial help to their parents. Our results therefore suggest a pattern that is consistent with an interpretation that some unobserved factors—such as unobserved aspects of wealth, income, health or levels of altruism towards parents and children (Becker 1974, 1991; Grundy and Henretta 2006)—affect the respondent's provision of transfers to both parents and children, and this pattern is inconsistent with a notion that transfers from parents to the respondents are passed on to the respondent's children with the respondent serving as an “intermediary” in these transfers. Moreover, a surprising aspect of the transfers documented in the present analyses is that, while transfers with adult children are commonplace, only a relatively small number of adult children seems to be engaged in this exchange of transfers. For instance, respondents aged 40–60 years provide on average financial transfers to only one out of four living adult children during the two-year period prior to the survey, and they receive financial transfers from only two out of almost five children during this period. We do not know based on our data if the set of children engaged in these transfers changes over time or is relatively constant. Nevertheless, this relative concentration of transfers between respondents and few adult children during a two-year period at least raises concerns about the sustainability of transfer flows in case of a health deterioration or the death of the transfer partners. Future research will need to investigate if other adult children step into these transfer relationships in case of a death or health shock of the child (or one of the children) with whom the respondent is primarily engaged in transfer relations.
Acknowledgments
The authors gratefully acknowledge the generous support for this research through National Institute of Child Health and Development (grant numbers R03HD058976, R21HD050652, R01HD044228, R01HD053781), the National Institute on Aging (grant number P30 AG12836), the Boettner Center for Pensions and Retirement Security at the University of Pennsylvania, and the National Institute of Child Health and Development Population Research Infrastructure Program (grant number R24 HD-044964), all at the University of Pennsylvania.
Appendix: Additional analyses and tables
Table A.1.
Pooled analyses: Logistic regressions for providing substantial amount of financial transfers to parents (odds ratios)
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 1.192 (0.164) |
1.030 (0.146) |
1.063 (0.167) |
1.051 (0.151) |
1.061 (0.172) |
1.081 (0.178) |
1.027 (0.146) |
1.024 (0.146) |
1.028 (0.146) |
1.026 (0.146) |
| Secondary schooling or more | 1.400+ (0.253) |
1.049 (0.201) |
1.105 (0.233) |
1.094 (0.212) |
1.215 (0.268) |
1.296 (0.291) |
1.039 (0.201) |
1.045 (0.202) |
1.041 (0.201) |
1.048 (0.203) |
| Respondent's wealth quintile | 1.238** (0.044) |
1.216** (0.047) |
1.234** (0.044) |
1.186** (0.048) |
1.171** (0.048) |
1.240** (0.044) |
1.233** (0.044) |
1.240** (0.044) |
1.232** (0.044) |
|
| Respondent is HIV+ | 0.914 (0.182) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | 1.011 (0.048) |
|||||||||
| Respondent's and parent's subjective health | ||||||||||
| Resp. is in very poor/poor/good health | 0.948 (0.105) |
0.947 (0.106) |
||||||||
| Resp. is in excellent health | 0.942 (0.133) |
0.934 (0.133) |
||||||||
| Parent is in very poor/poor/good health | 1.091 (0.118) |
|||||||||
| Parent is in excellent health | 0.973 (0.139) |
|||||||||
| Respondent's children | ||||||||||
| # of young living children | 0.997 (0.031) |
0.997 (0.031) |
0.997 (0.031) |
0.997 (0.031) |
||||||
| # of living adult children | 0.973 (0.036) |
0.946 (0.038) |
0.976 (0.036) |
0.949 (0.038) |
||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 1.166** (0.066) |
1.171** (0.067) |
||||||||
| Net non-financial transfer | 0.953 (0.071) |
0.931 (0.070) |
||||||||
| Observations | 3334 | 3247 | 2820 | 3186 | 2530 | 2470 | 3247 | 3247 | 3247 | 3247 |
Robust standard errors in parentheses. Standard errors are adjusted for clustering within respondents.
p-values:
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2, coresidence of parent, and region (3 regions). These coefficients are allowed to vary by gender of the respondent and gender of the parent. Analyses are conditional on parent (mother/father) being alive.
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only children who were given or provided substantial amount of financial/non-financial transfers.
Table A.2.
Pooled analyses: Logistic regressions for providing substantial amount of non-financial transfers to parents (odds ratios)
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 1.001 (0.151) |
0.945 (0.146) |
0.922 (0.157) |
0.908 (0.141) |
0.942 (0.164) |
0.907 (0.161) |
0.926 (0.143) |
0.927 (0.143) |
0.928 (0.143) |
0.928 (0.143) |
| Secondary schooling or more | 1.087 (0.219) |
0.951 (0.203) |
1.027 (0.241) |
0.929 (0.200) |
0.915 (0.224) |
0.903 (0.225) |
0.877 (0.187) |
0.877 (0.187) |
0.880 (0.188) |
0.880 (0.188) |
| Respondent's wealth quintile | 1.094* (0.045) |
1.090* (0.047) |
1.108* (0.046) |
1.128** (0.052) |
1.115* (0.052) |
1.099* (0.045) |
1.099* (0.045) |
1.098* (0.045) |
1.098* (0.045) |
|
| Respondent is HIV+ | 0.854 (0.190) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | 1.083 (0.056) |
|||||||||
| Respondent's and parent's subjective health | ||||||||||
| Resp. is in very poor/poor/good health | 1.079 (0.138) |
1.078 (0.139) |
||||||||
| Resp. is in excellent health | 0.908 (0.146) |
0.894 (0.145) |
||||||||
| Parent is in very poor/poor/good health | 1.043 (0.125) |
|||||||||
| Parent is in excellent health | 1.595** (0.243) |
|||||||||
| Respondent's children | ||||||||||
| # of young living children | 0.928+ (0.035) |
0.928+ (0.035) |
0.928* (0.035) |
0.928* (0.035) |
||||||
| # of living adult children | 0.905* (0.041) |
0.905* (0.043) |
0.906* (0.042) |
0.906* (0.043) |
||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 0.997 (0.059) |
1.002 (0.059) |
||||||||
| Net non-financial transfer | 0.858 (0.083) |
0.858 (0.083) |
||||||||
| Observations | 3333 | 3246 | 2819 | 3185 | 2529 | 2469 | 3246 | 3246 | 3246 | 3246 |
Robust standard errors in parentheses. Standard errors are adjusted for clustering within respondents.
p-values:
p < 0.10,
p < 0.05,
p <0.01.
Analyses additionally control for respondent age, age2, coresidence of parent, and region (3 regions). These coefficients are allowed to vary by gender of the respondent and gender of the parent. Analyses are conditional on parent (mother/father) being alive.
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only children who were given or provided substantial amount of financial/non-financial transfers.
Table A.3.
Pooled analyses: Logistic regressions for receiving substantial amount of financial transfers from parents (odds ratios)
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 1.327+ (0.220) |
1.319 (0.226) |
1.369 (0.261) |
1.304 (0.224) |
1.306 (0.250) |
1.311 (0.260) |
1.288 (0.220) |
1.289 (0.220) |
1.286 (0.220) |
1.288 (0.220) |
| Secondary schooling or more | 2.471** (0.491) |
2.358** (0.492) |
2.483** (0.578) |
2.302** (0.484) |
2.320** (0.566) |
2.325** (0.580) |
2.101** (0.440) |
2.102** (0.440) |
2.099** (0.439) |
2.100** (0.440) |
| Respondent's wealth quintile | 1.014 (0.040) |
1.029 (0.044) |
1.011 (0.040) |
1.023 (0.047) |
1.020 (0.047) |
1.016 (0.039) |
1.017 (0.039) |
1.016 (0.039) |
1.017 (0.039) |
|
| Respondent is HIV+ | 0.886 (0.211) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | 1.012 (0.057) |
|||||||||
| Respondent's and parent's subjective health | ||||||||||
| Resp. is in very poor/poor/good health | 0.801+ (0.102) |
0.840 (0.107) |
||||||||
| Resp. is in excellent health | 0.735+ (0.117) |
0.748+ (0.119) |
||||||||
| Parent is in very poor/poor/good health | 0.809+ (0.096) |
|||||||||
| Parent is in excellent health | 0.977 (0.151) |
|||||||||
| Respondent's children | ||||||||||
| # of young living children | 0.854** (0.035) |
0.854** (0.035) |
0.854** (0.035) |
0.854** (0.035) |
||||||
| # of living adult children | 0.910 (0.057) |
0.912 (0.057) |
0.908 (0.056) |
0.910 (0.056) |
||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 0.986 (0.073) |
0.983 (0.072) |
||||||||
| Net non-financial transfer | 1.049 (0.159) |
1.051 (0.159) |
||||||||
| Observations | 3326 | 3239 | 2812 | 3178 | 2523 | 2463 | 3239 | 3239 | 3239 | 3239 |
Robust standard errors in parentheses. Standard errors are adjusted for clustering within respondents.
p-values:
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2, coresidence of parent, and region (3 regions). These coefficients are allowed to vary by gender of the respondent and gender of the parent. Analyses are conditional on parent (mother/father) being alive.
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only children who were given or provided substantial amount of financial/non-financial transfers.
Table A.4.
Pooled analyses: Logistic regressions for receiving substantial amount of non-financial transfers from parents (odds ratios)
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.940 (0.171) |
0.898 (0.169) |
1.019 (0.216) |
0.884 (0.168) |
0.869 (0.183) |
0.833 (0.177) |
0.885 (0.166) |
0.884 (0.166) |
0.885 (0.166) |
0.883 (0.166) |
| Secondary schooling or more | 1.082 (0.252) |
0.967 (0.238) |
1.201 (0.331) |
0.947 (0.235) |
0.942 (0.267) |
0.913 (0.262) |
0.897 (0.223) |
0.900 (0.224) |
0.898 (0.224) |
0.900 (0.224) |
| Respondent's wealth quintile | 1.067 (0.049) |
1.079 (0.053) |
1.074 (0.049) |
1.085 (0.057) |
1.078 (0.057) |
1.070 (0.049) |
1.067 (0.049) |
1.070 (0.049) |
1.067 (0.049) |
|
| Respondent is HIV+ | 0.796 (0.201) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | 1.003 (0.062) |
|||||||||
| Respondent's and parent's subjective health | ||||||||||
| Resp. is in very poor/poor/good health | 1.168 (0.171) |
1.177 (0.174) |
||||||||
| Resp. is in excellent health | 0.893 (0.159) |
0.881 (0.158) |
||||||||
| Parent is in very poor/poor/good health | 0.851 (0.114) |
|||||||||
| Parent is in excellent health | 1.594** (0.271) |
|||||||||
| Respondent's children | ||||||||||
| # of young living children | 0.913* (0.040) |
0.912* (0.040) |
0.912* (0.040) |
0.911* (0.040) |
||||||
| # of living adult children | 0.938 (0.066) |
0.926 (0.065) |
0.939 (0.066) |
0.927 (0.065) |
||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 1.068 (0.082) |
1.070 (0.081) |
||||||||
| Net non-financial transfer | 0.956 (0.152) |
0.951 (0.149) |
||||||||
| Observations | 3326 | 3239 | 2812 | 3178 | 2524 | 2464 | 3239 | 3239 | 3239 | 3239 |
Robust standard errors in parentheses. Standard errors are adjusted for clustering within respondents.
p-values:
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2, coresidence of parent, and region (3 regions). These coefficients are allowed to vary by gender of the respondent and gender of the parent. Analyses are conditional on parent (mother/father) being alive.
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only children who were given or provided substantial amount of financial/non-financial transfers.
Table A.5.
Pooled respondents: OLS regressions for the number of living adult children (LAC) to whom the respondent provides financial transfers
| (1) | (2) | (3) | (4) | (5) | (6) | (V) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.158+ (0.084) |
0.037 (0.084) |
0.050 (0.091) |
0.018 (0.085) |
0.068 (0.093) |
0.065 (0.093) |
0.051 (0.083) |
0.016 (0.083) |
0.012 (0.081) |
0.034 (0.088) |
| Secondary schooling or more | 0.158 (0.190) |
−0.036 (0.190) |
0.016 (0.208) |
−0.008 (0.192) |
−0.018 (0.216) |
−0.025 (0.216) |
0.005 (0.190) |
−0.075 (0.191) |
−0.056 (0.183) |
−0.037 (0.203) |
| # of living adult sons | 0.327** (0.034) |
0.307** (0.034) |
0.312** (0.037) |
0.307** (0.035) |
0.319** (0.039) |
0.298** (0.044) |
0.360** (0.037) |
0.318** (0.034) |
0.370** (0.036) |
0.387** (0.045) |
| # of living adult daughters | 0.282** (0.033) |
0.260** (0.031) |
0.260** (0.034) |
0.265** (0.032) |
0.270** (0.036) |
0.242** (0.042) |
0.331** (0.038) |
0.270** (0.031) |
0.341** (0.037) |
0.361** (0.046) |
| Mean age of living adult children (LAC) | −0.026** (0.005) |
−0.029** (0.005) |
−0.028** (0.005) |
−0.029** (0.005) |
−0.031** (0.006) |
−0.031** (0.006) |
−0.027** (0.005) |
−0.029** (0.005) |
−0.029** (0.005) |
−0.031** (0.006) |
| # of living young children | −0.013 (0.020) |
−0.017 (0.020) |
−0.007 (0.020) |
−0.017 (0.020) |
−0.013 (0.021) |
−0.015 (0.022) |
−0.016 (0.020) |
−0.022 (0.020) |
−0.020 (0.020) |
−0.015 (0.021) |
| Respondent's wealth quintile | 0.177** (0.025) |
0.161** (0.026) |
0.176** (0.026) |
0.157** (0.028) |
0.156** (0.028) |
0.177** (0.025) |
0.179** (0.026) |
0.157** (0.026) |
0.142** (0.028) |
|
| Respondent is HIV+ | 0.077 (0.122) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | 0.049 (0.034) |
|||||||||
| Resp. is in very poor/poor/good health | −0.003 (0.078) |
−0.010 (0.078) |
−0.000 (0.077) |
|||||||
| Resp. is in excellent health | 0.143 (0.114) |
0.148 (0.114) |
0.088 (0.111) |
|||||||
| # of LAC who are in very poor/poor/good health | 0.065 (0.049) |
0.049 (0.048) |
||||||||
| # of LAC who are in excellent health | 0.017 (0.039) |
−0.010 (0.038) |
||||||||
| # of non-coresident LAC | −0.104** (0.037) |
−0.097** (0.037) |
−0.129** (0.039) |
|||||||
| # of parents who are alive | 0.060 (0.044) |
−0.025 (0.045) |
−0.041 (0.050) |
|||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 0.341** (0.056) |
0.375** (0.060) |
||||||||
| Net non-financial transfer | −0.063 (0.064) |
−0.080 (0.069) |
||||||||
| Observations | 1472 | 1439 | 1248 | 1409 | 1145 | 1145 | 1439 | 1404 | 1389 | 1105 |
Standard errors in parentheses.
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2 and region (3 regions), and are conditional on the respondent having at least one living adult child (LAC).
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only parents who were given or provided substantial amount of financial/non-financial transfers.
Table A.6.
Pooled respondents: OLS regressions for the number of living adult children (LAC) to whom the respondent provides non-financial transfers
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.052 (0.080) |
0.045 (0.083) |
0.018 (0.091) |
0.045 (0.084) |
0.077 (0.095) |
0.073 (0.094) |
0.088 (0.078) |
0.030 (0.083) |
0.085 (0.079) |
0.102 (0.089) |
| Secondary schooling or more | −0.166 (0.159) |
−0.181 (0.163) |
−0.293 (0.178) |
−0.147 (0.166) |
−0.304 (0.185) |
−0.307 (0.187) |
−0.059 (0.156) |
−0.199 (0.166) |
−0.061 (0.161) |
−0.179 (0.182) |
| # of living adult sons | 0.258** (0.038) |
0.265** (0.039) |
0.267** (0.042) |
0.266** (0.040) |
0.280** (0.045) |
0.229** (0.044) |
0.423** (0.043) |
0.275** (0.039) |
0.424** (0.044) |
0.392** (0.050) |
| # of living adult daughters | 0.182** (0.028) |
0.189** (0.029) |
0.172** (0.032) |
0.192** (0.030) |
0.161** (0.033) |
0.110** (0.036) |
0.400** (0.040) |
0.197** (0.029) |
0.400** (0.041) |
0.340** (0.046) |
| Mean age of living adult children (LAC) | −0.020** (0.005) |
−0.023** (0.005) |
−0.022** (0.005) |
−0.023** (0.005) |
−0.021** (0.006) |
−0.021** (0.006) |
−0.017** (0.004) |
−0.021** (0.005) |
−0.015** (0.005) |
−0.015** (0.005) |
| # of living young children | 0.029 (0.019) |
0.027 (0.020) |
0.013 (0.021) |
0.029 (0.020) |
0.015 (0.022) |
0.011 (0.022) |
0.030 (0.019) |
0.023 (0.020) |
0.027 (0.019) |
0.011 (0.021) |
| Respondent's wealth quintile | 0.008 (0.024) |
0.016 (0.025) |
0.008 (0.024) |
0.029 (0.026) |
0.026 (0.026) |
0.005 (0.023) |
−0.001 (0.024) |
−0.004 (0.023) |
0.017 (0.025) |
|
| Respondent is HIV+ | −0.146 (0.118) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | −0.005 (0.036) |
|||||||||
| Resp. is in very poor/poor/good health | −0.134+ (0.075) |
−0.112 (0.074) |
−0.089 (0.072) |
|||||||
| Resp. is in excellent health | −0.020 (0.121) |
−0.021 (0.120) |
−0.088 (0.114) |
|||||||
| # of LAC who are in very poor/poor/good health | 0.038 (0.041) |
0.035 (0.042) |
||||||||
| # of LAC who are in excellent health | 0.120** (0.039) |
0.106** (0.037) |
||||||||
| # of non-coresident LAC | −0.309** (0.038) |
−0.299** (0.039) |
−0.323** (0.039) |
|||||||
| # of parents who are alive | 0.064 (0.046) |
0.063 (0.050) |
0.028 (0.053) |
|||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | −0.004 (0.057) |
0.032 (0.056) |
||||||||
| Net non-financial transfer | 0.088 (0.080) |
0.056 (0.081) |
||||||||
| Observations | 1472 | 1439 | 1248 | 1409 | 1145 | 1145 | 1439 | 1404 | 1389 | 1105 |
Standard errors in parentheses.
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2 and region (3 regions), and are conditional on the respondent having at least one living adult child (LAC).
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only parents who were given or provided substantial amount of financial/non-financial transfers.
Table A.7.
Pooled respondents: OLS regressions for the number of living adult children (LAC) from whom the respondent receives financial transfers
| (1) | (2) | (3) | (4) | (5) | (6) | (V) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.008 (0.081) |
−0.003 (0.083) |
0.016 (0.089) |
−0.008 (0.084) |
−0.006 (0.092) |
−0.004 (0.092) |
−0.023 (0.082) |
0.001 (0.082) |
−0.021 (0.081) |
−0.020 (0.091) |
| Secondary schooling or more | 0.164 (0.165) |
0.175 (0.166) |
0.134 (0.157) |
0.214 (0.169) |
0.053 (0.165) |
0.057 (0.165) |
0.117 (0.166) |
0.185 (0.169) |
0.134 (0.170) |
0.021 (0.172) |
| # of living adult sons | 0.307** (0.037) |
0.305** (0.037) |
0.301** (0.040) |
0.298** (0.038) |
0.301** (0.043) |
0.320** (0.052) |
0.229** (0.038) |
0.284** (0.036) |
0.224** (0.038) |
0.250** (0.050) |
| # of living adult daughters | 0.270** (0.032) |
0.263** (0.031) |
0.246** (0.032) |
0.269** (0.031) |
0.233** (0.032) |
0.256** (0.041) |
0.161** (0.034) |
0.254** (0.030) |
0.165** (0.034) |
0.167** (0.041) |
| Mean age of living adult children (LAC) | 0.027** (0.006) |
0.028** (0.007) |
0.025** (0.007) |
0.029** (0.007) |
0.022** (0.007) |
0.022** (0.007) |
0.025** (0.007) |
0.026** (0.007) |
0.024** (0.007) |
0.020** (0.007) |
| # of living young children | −0.033+ (0.018) |
−0.028 (0.019) |
−0.021 (0.018) |
−0.026 (0.019) |
−0.023 (0.018) |
−0.021 (0.019) |
−0.029 (0.018) |
−0.023 (0.019) |
−0.023 (0.019) |
−0.019 (0.019) |
| Respondent's wealth quintile | −0.000 (0.024) |
−0.021 (0.025) |
−0.004 (0.025) |
−0.011 (0.026) |
−0.010 (0.026) |
0.001 (0.024) |
0.005 (0.025) |
−0.004 (0.025) |
−0.013 (0.026) |
|
| Respondent is HIV+ | −0.019 (0.113) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | 0.039 (0.032) |
|||||||||
| Resp. is in very poor/poor/good health | 0.036 (0.072) |
0.037 (0.072) |
−0.002 (0.073) |
|||||||
| Resp. is in excellent health | −0.024 (0.093) |
−0.027 (0.094) |
0.003 (0.093) |
|||||||
| # of LAC who are in very poor/poor/good health | −0.044 (0.045) |
−0.047 (0.044) |
||||||||
| # of LAC who are in excellent health | −0.025 (0.039) |
−0.022 (0.039) |
||||||||
| # of non-coresident LAC | 0.149** (0.036) |
0.138** (0.034) |
0.112** (0.037) |
|||||||
| # of parents who are alive | −0.047 (0.042) |
−0.080+ (0.044) |
−0.075 (0.048) |
|||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 0.131* (0.051) |
0.101+ (0.055) |
||||||||
| Net non-financial transfer | 0.059 (0.058) |
0.085 (0.063) |
||||||||
| Observations | 1472 | 1439 | 1248 | 1409 | 1145 | 1145 | 1439 | 1404 | 1389 | 1105 |
Standard errors in parentheses.
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2 and region (3 regions), and are conditional on the respondent having at least one living adult child (LAC).
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only parents who were given or provided substantial amount of financial/non-financial transfers.
Table A.8.
Pooled respondents: OLS regressions for the number of living adult children (LAC) from whom the respondent receives non-financial transfers
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Respondent schooling | ||||||||||
| Primary schooling | 0.022 (0.082) |
0.022 (0.084) |
0.006 (0.093) |
0.017 (0.086) |
0.040 (0.097) |
0.036 (0.096) |
0.054 (0.082) |
0.029 (0.085) |
0.078 (0.083) |
0.070 (0.094) |
| Secondary schooling or more | −0.288* (0.131) |
−0.282* (0.137) |
−0.366* (0.156) |
−0.266+ (0.140) |
−0.369* (0.159) |
−0.371* (0.164) |
−0.190 (0.132) |
−0.287* (0.140) |
−0.164 (0.135) |
−0.271+ (0.160) |
| # of living adult sons | 0.174** (0.030) |
0.184** (0.031) |
0.218** (0.034) |
0.187** (0.031) |
0.227** (0.036) |
0.172** (0.036) |
0.304** (0.036) |
0.190** (0.032) |
0.307** (0.037) |
0.277** (0.042) |
| # of living adult daughters | 0.248** (0.031) |
0.256** (0.032) |
0.245** (0.036) |
0.259** (0.033) |
0.200** (0.033) |
0.146** (0.035) |
0.416** (0.042) |
0.260** (0.033) |
0.419** (0.042) |
0.294** (0.046) |
| Mean age of living adult children (LAC) | −0.011* (0.005) |
−0.011* (0.005) |
−0.010+ (0.005) |
−0.012* (0.005) |
−0.013* (0.005) |
−0.014** (0.005) |
−0.007 (0.005) |
−0.010+ (0.005) |
−0.005 (0.005) |
−0.009+ (0.005) |
| # of living young children | 0.018 (0.018) |
0.019 (0.019) |
0.010 (0.021) |
0.020 (0.019) |
0.019 (0.022) |
0.015 (0.022) |
0.021 (0.018) |
0.015 (0.019) |
0.020 (0.019) |
0.018 (0.022) |
| Respondent's wealth quintile | −0.004 (0.025) |
−0.001 (0.027) |
−0.002 (0.026) |
0.017 (0.028) |
0.014 (0.027) |
−0.006 (0.025) |
−0.010 (0.026) |
−0.015 (0.025) |
0.007 (0.027) |
|
| Respondent is HIV+ | −0.044 (0.123) |
|||||||||
| Respondent's subj. likelihood of HIV infection† | −0.000 (0.035) |
|||||||||
| Resp. is in very poor/poor/good health | −0.057 (0.076) |
−0.031 (0.075) |
−0.022 (0.074) |
|||||||
| Resp. is in excellent health | −0.041 (0.118) |
−0.043 (0.117) |
−0.081 (0.117) |
|||||||
| # of LAC who are in very poor/poor/good health | 0.037 (0.039) |
0.045 (0.040) |
||||||||
| # of LAC who are in excellent health | 0.134** (0.036) |
0.128** (0.035) |
||||||||
| # of non-coresident LAC | −0.234** (0.035) |
−0.232** (0.036) |
−0.222** (0.041) |
|||||||
| # of parents who are alive | 0.086* (0.043) |
0.070 (0.047) |
0.069 (0.051) |
|||||||
| Total net transfers to parents | ||||||||||
| Net financial transfer | 0.030 (0.055) |
0.005 (0.057) |
||||||||
| Net non-financial transfer | 0.136+ (0.072) |
0.145+ (0.074) |
||||||||
| Observations | 1472 | 1439 | 1248 | 1409 | 1145 | 1145 | 1439 | 1404 | 1389 | 1105 |
Standard errors in parentheses.
p < 0.10,
p < 0.05,
p < 0.01.
Analyses additionally control for respondent age, age2 and region (3 regions), and are conditional on the respondent having at least one living adult child (LAC).
Coded as 0 = no likelihood, 1 = some likelihood, 2 = medium likelihood, and 3 = high likelihood.
Only parents who were given or provided substantial amount of financial/non-financial transfers.
Footnotes
This open-access work is published under the terms of the Creative Commons Attribution NonCommercial License 2.0 Germany, which permits use, reproduction & distribution in any medium for non-commercial purposes, provided the original author(s) and source are given credit. See http://creativecommons.org/licenses/by-nc/2.0/de/
In contrast, extensive research has documented and analyzed the intergenerational relations in many developed countries that face rapid population aging; see for instance Lee and Mason (2011) or Silverstein and Giarrusso (2010).
AIDS is currently the leading cause of adult mortality in many SSA countries (Porter and Zaba 2004; Crampin et al. 2002; Blacker 2004; Bradshaw et al. 2003, 2004; Palloni 1996; Heuveline 2003, 2004). At the turn of the century, the probability of a 15-year old dying before reaching age 60 was estimated to be in the range of 30–60% (Zaba, Whiteside, and Boerma 2004). In 2003–2005, a time when the HIV/AIDS epidemic reached its maturity in most SSA countries, a study in the Karonga District in Northern Malawi estimated that 60% of men and 66% of women aged 15–44 years died as a result of HIV/AIDS (Hosegood et al. 2007; Jahn et al. 2005). In a different context, Wachter, Knodel, and VanLandingham (2002) simulated that despite low HIV prevalence of 2%, 13% of elderly Thais over age 50 will lose one adult child to AIDS, and 2% of them will lose multiple children. This impact is expected to be much higher in SSA (Zagheni 2011), where the estimated adult (aged 15–49) HIV+ prevalence ranges from 0.7 to 25.9 percent (UNAIDS 2009).
For example, in the context of investments in children's schooling, Grant (2008) has showed that women's real and perceived anticipation of future health shocks has a positive impact on their children's educational attainment.
Although we acknowledge the importance of lateral familial ties and other supportive networks in the SSA context (Lee 2000), we focus our analysis on vertical intergenerational transfers that have received widespread attention in other contexts as a major source for pooling and transferring resources between generations (Mason and Miller 2000; Lee 2000; Knodel, Chayovan, and Siriboon 1992; Knodel and Saengtienchai 1999).
Detailed descriptions of the MLSFH sample selection, data collection, and data quality are provided on the project website http://www.malawi.pop.upenn.edu, in a Special Collection of the online journal Demographic Research that is devoted to the MLSFH (Watkins et al. 2003), and in a recent follow-up publication that incorporates the 2004 and 2006 MLSFH data (Anglewicz et al. 2009). Comparisons with the Malawi Demographic and Health Survey showed that the MLSFH sample population is reasonably representative of the rural Malawi population (Anglewicz et al. 2009; Bignami-Van Assche, Reniers, and Weinreb 2003; Watkins et al. 2003).
The larger number of female than male respondents is in part due to the sample design of the MLSFH dating back to 1998, and the somewhat higher response rates and lower rates of temporary migration for females as compared to males; see Anglewicz et al. (2009) for additional information.
For more detailed analysis of HIV/AIDS risk perceptions, see Anglewicz and Kohler (2009), Delavande and Kohler (2009), and Delavande and Kohler (forthcoming).
The average 2004 HIV prevalence was about 9% in the MLSFH study population, with considerable regional variation: 2006 HIV prevalence among MLSFH respondents was 6.6% in Rumphi, 7.7% in Mchinji and 12.6% in Balaka (Obare et al. 2009).
The sixth survey wave has been collected in summer 2010, but the data were not available for analyses at the time of this writing.
Because we are interested in reciprocal transfers among parents and adult children and very few respondents below age 30 have children older than 15 years, we focus here on respondents 30 to 60 years old.
The same fitting procedure is used throughout this paper.
Because of the MLSFH sampling design, dating in part back to 1998, men above age 30 in the sample where ever married to a female MLSFH respondent; in 2004, the MLSFH recruited an adolescent and young adult sample that was not conditional on marital status also included unmarried men.
As an indicator for the data quality of the listing of children in the household/family roster, we also show in Figure 1 the mean number of alive children with unknown age that is fairly small and constant by age of respondents.
There are marked regional differences in the probability of co-residing with the mother or father due to differential marriage patterns. In the southern region (Balaka), where marriage is matrilineal, co-residence of female respondents with their mother is more common, and coresidence with the father is less common, than in the central and northern region where marriage patterns are mixed or patrilineal. For example, conditional on the mother being alive, 61% of female respondents aged 30+ co-reside in the same household or compound with their mother in Balaka (southern region), while this is the case for only 28% of female respondents in Mchinji (central region) and 10% in Rumphi (northern region). For male respondents age 30+, the corresponding probabilities of co-residing with the mother are 17% (Balaka), 48% (Mchinji) and 58% (Rumphi). The analogous regional pattern exists for fathers and for male respondents.
As long as the transfers to and from a particular parent are comparable, it is not problematic for this calculation of net transfers if “a lot of financial assistance” describes different amounts of transfers between the respondent and his or her mother and the respondent and his/her father.
The dependent variable in the regressions in the Appendix Tables A.5–A.8 is the number of living adult children (LAC) to whom the respondent has given to or received from a substantial amount of financial/non-financial transfers.
References
- Aboderin I, Ferreira M. Linking ageing to development agendas in sub-Saharan Africa: Challenges and approaches. Journal of Population Ageing. 2008;1(1):51–73. doi: 10.1007/s12062-009-9002-8. doi:10.1007/s12062-009-9002-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Agree EM, Biddlecom AE, Chang MC, Perez AE. Transfers from older parents to their adult children in Taiwan and the Philippines. Journal of Cross-Cultural Gerontology. 2002;17(4):269–294. doi: 10.1023/a:1023085818629. doi:10.1023/A:1023085818629. [DOI] [PubMed] [Google Scholar]
- Anglewicz P, Adams J, Obare F, Kohler HP, Watkins S. The Malawi Diffusion and Ideational Change Project 2004-06: Data collection, data quality and analyses of attrition. Demographic Research. 2009;20(21):503–540. doi: 10.4054/demres.2009.20.21. doi:10.4054/DemRes.2009.20.21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anglewicz P, Kohler HP. Overestimating HIV infection: The construction and accuracy of subjective probabilities of HIV infection in rural Malawi. Demographic Research. 2009;20(6):65–96. doi: 10.4054/DemRes.2009.20.6. doi:10.4054/DemRes.2009.20.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ankrah EM. The impact of HIV/AIDS on the family and other significant relationships: The African clan revisited. In: Bor R, Elford J, editors. The Family and HIV. Cassell; New York: 1994. pp. 23–44. [DOI] [PubMed] [Google Scholar]
- Becker GS. A theory of social interaction. Journal of Political Economy. 1974;82(6):1063–1093. [Google Scholar]
- Becker GS. A Treatise on the Family. 2nd ed Harvard University Press; Cambridge, MA: 1991. [Google Scholar]
- Becker GS, Tomes N. Child endowments and the quantity and quality of children. Journal of Political Economy. 1976;84:S143–S162. doi:10.1086/260536. [Google Scholar]
- Ben-Porath Y. The F-connection: Families, friends and firms in the organization of exchange. Population and Development Review. 1980;6(1):1–30. doi:10.2307/1972655. [Google Scholar]
- Bengtson V. Beyond the nuclear family: The increasing importance of multigenerational bonds. Journal of Marriage and Family. 2001;63(1):1–16. doi:10.1111/j.1741-3737.2001.00001.x. [Google Scholar]
- Bianchi SM, Hotz JV, McGarry K, Seltzer JA. Intergenerational ties: Theories, trends and challenges. In: Booth A, Crouter AC, Bianchi SM, Seltzer JA, editors. Intergenerational Caregiving. The Urban Instititute Press; Washington D.C.: 2008. pp. 3–43. [Google Scholar]
- Bignami-Van Assche S, Reniers G, Weinreb AA. An assessment of the KDICP and MDICP data quality: Interviewer effects, question reliability and sample attrition. Demographic Research. 2003;1(2):31–76. Special Collection. [Google Scholar]
- Billari FC, Liefbroer AC. Intergenerational ties: What can be gained from an international perspective? In: Booth A, Crouter AC, Bianchi SM, Seltzer JA, editors. Intergenerational Caregiving. The Urban Instititute Press; Washington D.C.: 2008. pp. 53–66. [Google Scholar]
- Blacker J. The impact of AIDS on adult mortality: Evidence from national and regional statistics. AIDS. 2004;18(Supplement 2):S19–S26. doi: 10.1097/00002030-200406002-00003. [DOI] [PubMed] [Google Scholar]
- Bradshaw D, Groenewald P, Laubscher R, Nannan N, Nojilana B, Norman R, Pieterse D, Schneider M, Bourne D, Timæus I, et al. Initial burden of disease estimates for South Africa, 2000. South African Medical Journal. 2003;93(9):682–688. [PubMed] [Google Scholar]
- Bradshaw D, Laubscher R, Dorrington R, Timaeus IM. Unabated rise in number of adult deaths in South Africa. South African Medical Journal. 2004;94(4):278–279. [PubMed] [Google Scholar]
- Bray R. How does AIDS illness affect women's residential decisions? Findings from an ethnographic study in a Cape Town township. Ajar-African Journal of Aids Research. 2009;8(2):167–179. doi: 10.2989/AJAR.2009.8.2.5.857. [DOI] [PubMed] [Google Scholar]
- Cheng ST, Siankam B. The impacts of the HIV/AIDS pandemic and socioeconomic development on the living arrangements of older persons in sub-Saharan Africa: A country-level analysis. American Journal of Community Psychology. 2009;44(1–2):136–147. doi: 10.1007/s10464-009-9243-y. doi:10.1007/s10464-009-9243-y. [DOI] [PubMed] [Google Scholar]
- Cohen B, Menken J. Aging in Sub-Saharan Africa: Recommendations for Further Research. National Academy Press; Washington, D.C.: 2006. [PubMed] [Google Scholar]
- Crampin A, Floyd S, Glynn J, Sibande F, Mulawa D, Nyondo A, Broad-bent P, Bliss L, Ngwira B, Fine P. Long-term follow-up of HIV-positive and HIV-negative individuals in rural Malawi. AIDS. 2002;16(11):1545–1550. doi: 10.1097/00002030-200207260-00012. doi:10.1097/00002030-200207260-00012. [DOI] [PubMed] [Google Scholar]
- Davies S. Remittances as insurance for idiosyncratic and covariate shocks in Malawi: The importance of distance and relationship. 2007 MPRA Paper No. 4463. [Google Scholar]
- Delavande A, Kohler HP. Subjective expectations in the context of HIV/AIDS in Malawi. Demographic Research. 2009;20(31):817–874. doi: 10.4054/DemRes.2009.20.31. doi:10.4054/DemRes.2009.20.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delavande A, Kohler HP. The impact of HIV testing on subjective expectations and risky behavior in Malawi. Demography. doi: 10.1007/s13524-012-0119-7. forthcoming. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Floyd S, Crampin AC, Glynn JR, Madise N, Mwenebabu M, Mnkhondia S, Ngwira B, Zaba B, Fine PEM. The social and economic impact of parental HIV on children in northern Malawi: Retrospective population-based cohort study. Aids Care–Psychological and Socio-Medical Aspects of AIDS/HIV. 2007;19(6):781–790. doi: 10.1080/09540120601163227. doi:10.1080/09540120601163227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foster G. The capacity of the extended family safety net for orphans in Africa. Psychology, Health and Medicine. 2000;5(1):55–62. doi:10.1080/135485000106007. [Google Scholar]
- Frankenberg E, Lillard L, Willis R. Patterns of intergenerational transfers in Southeast Asia. Journal of Marriage and the Family. 2002;64(3):627–641. doi:10.1111/j.1741-3737.2002.00627.x. [Google Scholar]
- Grant MJ. Children's school participation and HIV/AIDS in rural Malawi: The role of parental knowledge and perceptions. Demographic Research. 2008;19(45):1603–1634. doi:10.4054/DemRes.2008.19.45. [Google Scholar]
- Grundy E, Henretta J. Between elderly parents and adult children: A new look at the intergenerational care provided by the `sandwich generation'. Ageing and Society. 2006;26(05):707–722. doi:10.1017/S0144686X06004934. [Google Scholar]
- Hammel EA. Chayanov revisited: A model for the economics of complex kin units. PNAS—Proceedings of the National Academy of Sciences of the United States of America. 2005;102(19):7043–7046. doi: 10.1073/pnas.0501987102. doi:10.1073/pnas.0501987102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henretta JC, Grundy E, Harris S. Socioeconomic Differences in Having Living Parents and Children: A U.S.-British Comparison of Middle-Aged Women. Journal of Marriage and Family. 2001;63(3):852–867. doi:10.1111/j.1741-3737.2001.00852.x. [Google Scholar]
- Heuveline P. HIV and population dynamics: A general model and Maximum-Likelihood standards for east Africa. Demography. 2003;40(2):217–245. doi: 10.1353/dem.2003.0013. doi:10.1353/dem.2003.0013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heuveline P. Impact of the HIV epidemic on population and household structure: The dynamics and evidence to date. AIDS. 2004;18(Supplement 2):S45–S53. doi: 10.1097/00002030-200406002-00006. doi:10.1097/00002030-200406002-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hosegood V, Floyd S, Marston M, Hill C, McGrath N, Isingo R, Crampin A, Zaba B. The effects of high HIV prevalence on orphanhood and living arrangements of children in Malawi, Tanzania, and South Africa. Population Studies. 2007;61(3):327–336. doi: 10.1080/00324720701524292. doi:10.1080/00324720701524292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hosegood V, Timaeus I. HIV/AIDS and older people in South Africa. In: Cohen B, Menken J, editors. Aging in Sub-Saharan Africa: Recommendations for furthering research. National Academies Press; 2006. pp. 250–275. [PubMed] [Google Scholar]
- Jahn A, Mwaungulu F, Msiska V, Crampin A, Kachiwanda L, Kasimba S, Mc-Grath N, Fine P, Zaba B. Population Estimates from the Karonga Continuous Registration System. National AIDS Commission Annual Meeting Abstracts; Lilongwe, Malawi: Apr, 2005. What is the true death toll of AIDS in rural Malawi? unpublished manuscript. 2005. [Google Scholar]
- Knodel J, Chayovan N, Siriboon S. The impact of fertility decline on familial support for the elderly: An illustration from Thailand. Population and Development Review. 1992;18(1):79–103. doi:10.2307/1971860. [Google Scholar]
- Knodel J, Saengtienchai C. Studying living arrangements of the elderly: Lessons from a quasi-qualitative case study approach in Thailand. Journal of Cross-Cultural Gerontology. 1999;14(3):197–220. doi: 10.1023/a:1006620314634. doi:10.1023/A:1006620314634. [DOI] [PubMed] [Google Scholar]
- Knodel J, Watkins S, VanLandingham M. AIDS and older persons: An international perspective. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2003;33:S153. doi: 10.1097/00126334-200306012-00012. doi:10.1097/00126334-200306012-00012. [DOI] [PubMed] [Google Scholar]
- Kohler HP, Hammel EA. On the role of families and kinship networks in pre-industrial agricultural societies: An analysis of the 1698 Slavonian census. Journal of Population Economics. 2001;14(1):21–49. doi:10.1007/s001480050158. [Google Scholar]
- Lee RD. Intergenerational transfers and the econbomic life cycle: A cross-cultural perspective. In: Mason A, Tapinos G, editors. Sharing the Wealth: Demographic Change and Economic Transfers between Generations. Oxford University Press; 2000. pp. 17–56. [Google Scholar]
- Lee RD, Mason A. Generational economics in a changing world. Population and Development Review. 2011;37(Supplement S1):115–142. doi: 10.1111/j.1728-4457.2011.00380.x. doi:10.1111/j.1728-4457.2011.00380.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lillard LA, Willis RJ. Motives for intergenerational transfers: Evidence from Malaysia. Demography. 1997;34(1):115–134. doi:10.2307/2061663. [PubMed] [Google Scholar]
- Mason A, Miller T. Dynasties, intergenerational transfers, and life-cycle income: A case study of Taiwan. In: Mason A, Tapinos G, editors. Sharing the Wealth: Demographic Change and Economic Transfers between Generations. Oxford University Press; 2000. pp. 57–84. [Google Scholar]
- Merli GM, Palloni A. The HIV/AIDS epidemic, kin relations, living arrangements and the elderly in South Africa. In: Cohen B, Menken J, editors. Aging in Sub-Saharan Africa: Recommendations for Furthering Research. National Academy Press; Washington, D.C.: 2006. [Google Scholar]
- Mtika MM. The AIDS epidemic in Malawi and its threat to household food security. Human Organization. 2001;60(2):178–188. [Google Scholar]
- Mtika MM, Doctor HV. Matriliny, patriliny, and wealth flow variations in Malawi. African Sociological Review. 2002;6(2):71–97. doi:10.4314/asr.v6i2.23215. [Google Scholar]
- Mtika M. Family transfers in a subsistence economy and under a high incidence of HIV/AIDS: the case of rural Malawi. Journal of Contemporary African Studies. 2003;21(1):69–92. doi:10.1080/02589000305453. [Google Scholar]
- Naidu V, Harris G. The impact of HIV/AIDS morbidity and mortality on households—A review of household studies. South African Journal of Economics. 2005;73(Supplement S1):533–544. doi:10.1111/j.1813-6982.2005.00037.x. [Google Scholar]
- Nyasani E, Sterberg E, Smith H. Fostering children affected by AIDS in Richards Bay, South Africa: A qualitative study of grandparents' experiences. African Journal of AIDS Research. 2009;8(2):181–192. doi: 10.2989/AJAR.2009.8.2.6.858. [DOI] [PubMed] [Google Scholar]
- Obare F, Fleming P, Anglewicz P, Thornton R, Martinson F, Kapatuka A, Poulin M, Watkins SC, Kohler HP. Acceptance of repeat population-based Voluntary counseling and testing for HIV in rural Malawi. Sexually Transmitted Infections. 2009;85(2):139–144. doi: 10.1136/sti.2008.030320. doi:10.1136/sti.2008.030320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palloni A. Demography of HIV/AIDS. Population Index. 1996;62(4):601–652. doi:10.2307/3646371. [Google Scholar]
- Palloni A, Pinto G, Wong R. Family Support and Population Aging in Latin American and Carribbean. Paper presented at the Population Association Meetings; Dallas. April 15-17, 2010; 2010. [Google Scholar]
- Peters P, Kambewa D, Walker P. The Effects of Increasing Rates of HIV/AIDS-related Illness and Death on Rural Families in Zomba District. A Longitudinal Study; Malawi: 2008. IFPRI Working Paper. [Google Scholar]
- Pollak RA. A transaction cost approach to families and households. Journal of Economic Literature. 1985;23(2):581–608. [Google Scholar]
- Porter K, Zaba B. The empirical evidence for the impact of HIV on adult mortality in the developing world: Data from serological studies. AIDS. 2004;18(Supplement 2):S9–S17. doi: 10.1097/00002030-200406002-00002. doi:10.1097/00002030-200406002-00002. [DOI] [PubMed] [Google Scholar]
- Pörtner C. Children as insurance. Journal of Population Economics. 2001;14:119–136. [Google Scholar]
- Raut L, Tran L. Parental human capital investment and old-age transfers from children: Is it a loan contract or reciprocity for Indonesian families? Journal of Development Economics. 2005;77(2):389–414. doi:10.1016/j.jdeveco.2004.04.003. [Google Scholar]
- Rosenzweig MR. Risk, implicit contracts and the family in rural areas of low-income countries. Economic Journal. 1988;98(393):1148–1170. doi:10.2307/2233724. [Google Scholar]
- Rosenzweig MR, Stark O. Consumption smoothing, migration, and marriage: Evidence from rural India. Journal of Political Economy. 1989;97(4):905–926. doi:10.1086/261633. [Google Scholar]
- Sagner A, Mtatt RZ. Politics of pension sharing in urban South Africa. Ageing and Society. 1999;19(4):393–416. doi:10.1017/S0144686X99007424. [Google Scholar]
- Schatz E, Ogunmefun C. Caring and contributing: The role of older women in rural South African multi-generational households in the HIV/AIDS era. World Development. 2007;35(8):1390–1403. doi:10.1016/j.worlddev.2007.04.004. [Google Scholar]
- Silverstein M, Giarrusso R. Aging and family life: A decade review. Journal of Marriage and Family. 2010;72(5):1039–1058. doi: 10.1111/j.1741-3737.2010.00749.x. doi:10.1111/j.1741-3737.2010.00749.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stecklov G. Evaluating the economic returns to childbearing in Côte d'Ivoire. Population Studies. 1999;53(1):1–17. doi:10.1080/00324720308072. [Google Scholar]
- UNAIDS . AIDS epidemic update December 2009. World Health Organization; 2009. [Google Scholar]
- Velkoff VA, Kowal PR. Aging in Sub-Saharan Africa: The Changing Demography of the Region. In: National Research Council, editor. Aging in Sub-Saharan Africa: Reccommendations for Furthering Research. The National Academies Press; Washington, D.C.: 2006. pp. 55–91. [Google Scholar]
- Wachter K, Knodel J, VanLandingham M. AIDS and the elderly of Thailand: Projecting familial impacts. Demography. 2002;39(1):25–41. doi: 10.1353/dem.2002.0012. doi:10.1353/dem.2002.0012. [DOI] [PubMed] [Google Scholar]
- Watkins S, Behrman JR, Kohler HP, Zulu EM. Introduction to “Research on demographic aspects of HIV/AIDS in rural Africa”. Demographic Research. 2003;1(1):1–30. Special Collection. doi:10.4054/DemRes.2003.S1.1. [Google Scholar]
- Watkins SC, Swidler A. Ties of Dependence: AIDS and Transactional Sex in Rural Malawi. Studies in Family Planning. 2007;38(3):147–162. doi: 10.1111/j.1728-4465.2007.00127.x. [DOI] [PubMed] [Google Scholar]
- Weinreb AA. Lateral and vertical intergenerational exchange in rural Malawi. Journal of Cross-Cultural Gerontology. 2002;12:1–38. doi: 10.1023/a:1015834300553. [DOI] [PubMed] [Google Scholar]
- Willis R. The old age security hypothesis and population growth. In: Burch T, editor. Demographic behavior: Interdisciplinary Perspectives on Decision-making. Westview Press; Boulder: 1980. pp. 43–69. [Google Scholar]
- Wolf DA. Elderly and their kin: Patterns of availability and access. In: Martin L, Preston S, editors. Demography of Aging. National Academy Press; Washington, D.C.: 1994. pp. 146–194. [PubMed] [Google Scholar]
- Wong R, Kitayama K, Soldo BJ. Ethnic differences in time transfers from adult children to elderly parents: Unobserved heterogeneity across families. Research on Aging, Special Issue on Multilevel Analysis in Aging Research. 1999;21(2):144–175. doi:10.1177/0164027599212002. [Google Scholar]
- Zaba B, Whiteside A, Boerma JT. Demographic and socioeconomic impact of AIDS: Taking stock of the empirical evidence. AIDS. 2004;18(Supplement 2):S1–S7. doi: 10.1097/00002030-200406002-00001. doi:10.1097/00002030-200406002-00001. [DOI] [PubMed] [Google Scholar]
- Zagheni E. The impact of the HIV/AIDS epidemic on kinship resources for orphans in Zimbabwe. Population and Development Review. 2011;37(4):761–783. doi: 10.1111/j.1728-4457.2011.00456.x. doi:10.1111/j.1728-4457.2011.00456.x. [DOI] [PubMed] [Google Scholar]
- Zimmer Z. Household composition among elders in Sub-Saharan Africa in the context of HIV/AIDS. Journal of Marriage and the Family. 2009;71(4):1086–1099. doi:10.1111/j.1741-3737.2009.00654.x. [Google Scholar]