

Abstract
Purpose
To evaluate the accuracy and applicability of the modified Clavien classification system (CCS) in evaluating complications following photoselective vaporization of the prostate by use of the 120W GreenLight high-performance system (HPS-PVP).
Materials and Methods
The medical records of 342 men who underwent HPS-PVP were retrospectively analyzed. Patients were older than 40 years and had a prostate volume >30 mL and an International Prostate Symptom Score (IPSS) ≥8. Patients with prostatic malignancy, neurogenic bladder, urethral stricture, large postvoid residual volume (>250 mL), previous prostatic surgery, or urinary tract infection were excluded. All operations were done by a single surgeon, and patients were followed up for uroflowmetry and IPSS postoperatively. All complications were recorded and classified according to the modified CCS, and methods of management were also recorded.
Results
The patients' mean age was 71.6±7.3 years; mean prostate volume was 50.0±17.0 mL, and 95 cases (27.7%) had volumes greater than 70 mL. The mean total IPSS was 21.7±7.9 preoperatively and 12.3±8.1 at the first month postoperatively. A total of 59 patients (17.3%) experienced postoperative complications until the first month after the surgery. Among them, 49 patients (14.3%) showed grade I complications, 9 patients (2.6%) showed grade II complications, and 1 patient (0.3%) showed a grade IIIb complication. No patients had complications graded higher than IIIb.
Conclusions
Although the modified CCS is a useful tool for communication among clinicians in allowing comparison of surgical outcomes, this classification should be revised to gain higher accuracy and applicability in the evaluation of postoperative complications of HPS-PVP.
Keywords: Complications, Lasers, Prostatic hyperplasia, Transurethral resection of prostate, Transurethral vaporesection of prostate
INTRODUCTION
Although many variables must be considered in the quality assessment of surgical outcomes, previous investigations have shown that the Clavien classification system (CCS) for the evaluation of postoperative complications has been accepted since 1992 as a desirable, standardized platform of accuracy and reliability for comparing surgical outcomes among different institutions, surgeons, or operative techniques [1]. This classification system was based on the therapy used to treat complications that occurred within the first month postoperatively. The CCS was modified in 2004 according to the reporting manner of perioperative life-threatening and permanently disabling conditions [2].
This new grading system has been widely accepted by many urologists to report the perioperative outcomes of laparoendoscopic single-site surgery (LESS) in the upper urinary tract [3], radical cysto-urethrectomy [4], and robot-assisted radical prostatectomy [5]. Besides these major oncologic surgeries, the modified CCS has also been validated for grading perioperative complications in patients who underwent transurethral resection of the prostate (TURP) [6,7], percutaneous nephrolithotomy [8,9], or laparoscopic pyeloplasty [10]. However, there have been few reports on less-invasive procedures such as holmium laser enucleation of the prostate or photoselective vaporization of the prostate (PVP) by use of the KTP laser. Because the distribution of complications for these less-invasive procedures must differ from the distribution of complications for invasive procedures, the applicability of the modified CCS should be evaluated for less-invasive procedures.
Therefore, the aim of this study was to evaluate the accuracy and applicability of the modified CCS in evaluating complications after the Seoul technique of modified PVP with the 120W GreenLight high performance system (HPS-PVP).
MATERIALS AND METHODS
The present study was a retrospective analysis of the medical records of patients who underwent HPS by a single surgeon between January 2008 and September 2011. A total of 353 patients who underwent HPS-PVP were included. Patients were older than 40 years and had a prostate volume >30 mL and an International Prostate Symptom Score (IPSS) ≥8. Patients with prostatic malignancy, neurogenic bladder, urethral stricture, large postvoid residual volume (>250 mL), previous prostatic surgery, and urinary tract infection were excluded from the analysis, because patients with these conditions could have experienced voiding problems or bladder dysfunction preoperatively. Thus, in such a case, the postoperative complications could be confused with the underlying abnormalities. According to the exclusion criteria, 11 patients were excluded. Finally, the records of 342 patients were analyzed in this study. This study was approved by the Institutional Review Board of SMG-SNU Boramae Medical Center, and the procedures complied with the Declaration of Helsinki (revised Edinburgh, 2000).
A GreenLight HPS laser that generates up to 120W with a lithium triborate crystal was used for the operation. The Seoul technique, a modified vaporization-resection technique, was used [11]. Age, body mass index, and preoperative conditions including past medical history, transrectal ultrasonography, uroflowmetry, and American Society of Anesthesiologists score were reviewed from the medical records. Patients were followed up for uroflowmetry and IPSS postoperatively at 2 weeks, 1 month, 3 months, 6 months, and yearly from 1 year. All complications that arose within the first month postoperatively were recorded and classified according to the modified Clavien-Dindo System [6]. According to the modified CCS, the complications were graded as I (any deviation from the normal postoperative course without interventions), II (pharmacological treatment, blood transfusion, or total parenteral nutrition), IIIa (intervention not under general anesthesia), IIIb (intervention under general anesthesia), IVa (single organ dysfunction), IVb (multiorgan dysfunction), and V (death) [2]. For each complication, the managements were also recorded.
Variables are presented as mean±standard deviations. All preoperative and postoperative variables were analyzed for statistically significant differences by use of the independent t-test. To compare pre- and postoperative clinical parameters, a paired t-test was used. A p<0.05 was considered statistically significant, and commercially available SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA) was used.
RESULTS
The patients' demographics and perioperative profiles are shown in Table 1. The patients' mean age was 71.6±7.3 years. The patients' mean prostate volume was 50.0±17.0 mL, and 95 cases (27.7%) had volumes greater than 70 mL. The mean total IPSS score was 21.7±7.9 preoperatively, which was significantly improved at 1 month postoperatively (12.3±8.1).
TABLE 1.
Demographics
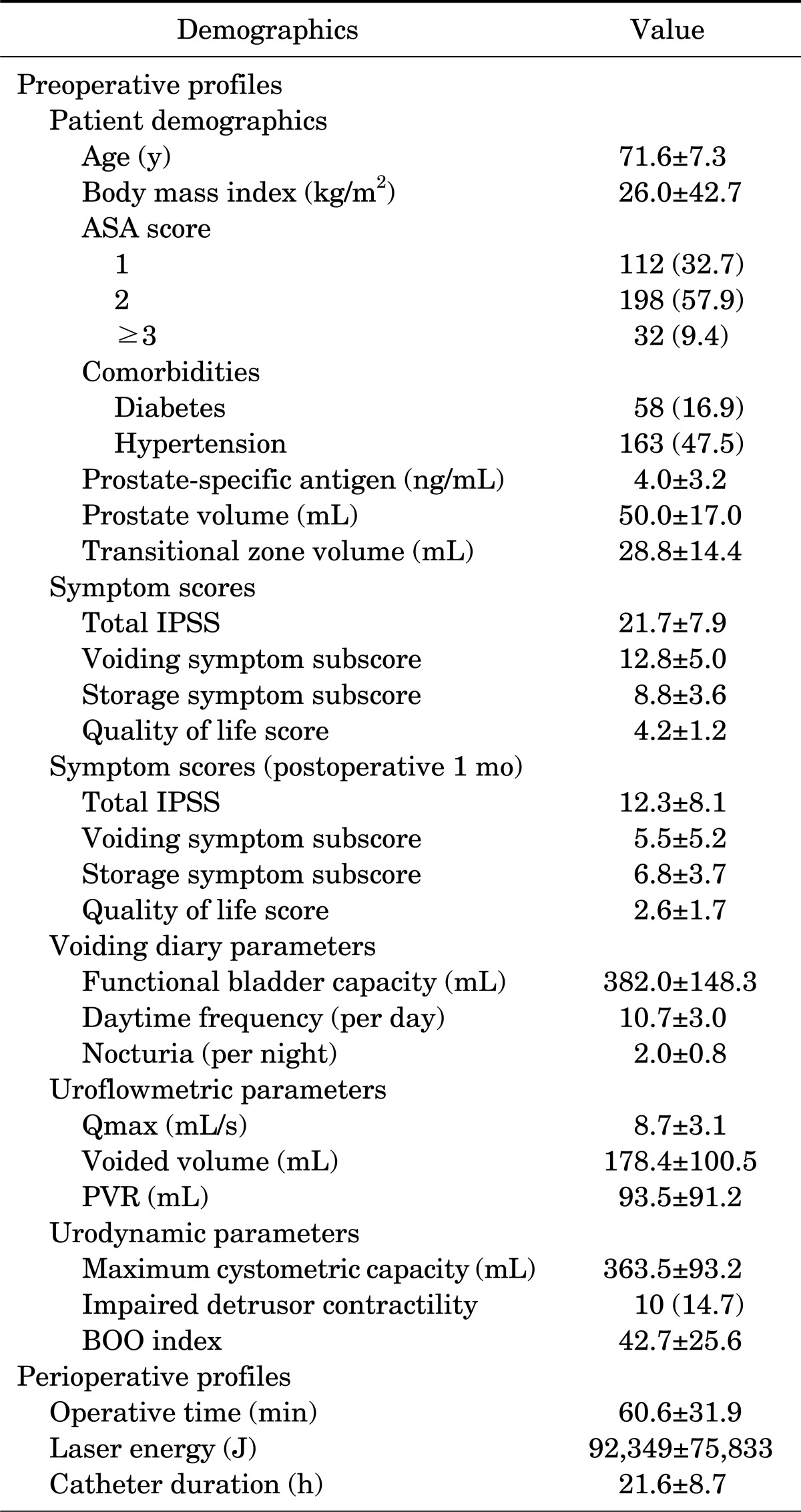
Values are presented as mean±standard deviation or number (%).
ASA, American Society Of Anesthesiologists; IPSS, International Prostate Symptom Score; Qmax, maximal flow rate; PVR, postvoid residual urine; BOO, bladder outlet obstruction.
Table 2 shows the distrubution of all complications and detailed methods of management for each complication. Among the 342 patients, 59 cases (17.3%) experienced postoperative complications within 1 month. Most of them (49 cases, 14.3%) showed grade I complications. Nonspecific urinary symptoms resolved spontaneously without any medications. Patients complained of mild hematuria, frequency, dysuria, and urgency. According to the records, however, the symptoms were too mild to treat with any medications and were relieved at the next visit. Two patients with grade I complications showed postoperative gross hematuria, which was improved by indwelling of a urethral Foley catheter and manual irrigation for several days. Another two patients showed urinary retention after the urethral catheters were removed. One of the patients did not void well until the first year postoperatively, and he was not followed up thereafter. Patients with grade II complications (nine cases, 2.6%) showed some transient urinary symptoms (urgency, dysuria, or slow stream) that improved after taking medications such as anticholinergic agents, antibiotics, and alpha-blockers. One patient (0.3%) showed a grade IIIb complication that was resolved after transurethral coagulation under general anesthesia. None had complications graded higher than IIIb.
TABLE 2.
Postoperative complications and management
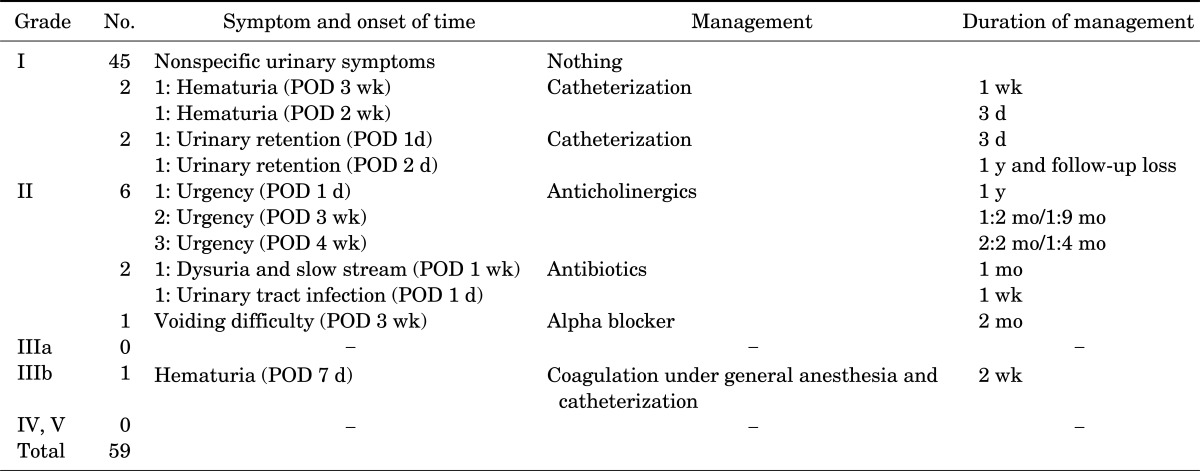
POD, postoperative day.
DISCUSSION
The necessity of a standardized guideline for comparing surgical outcomes and for grading complications among different hospitals has been repeatedly mentioned since 1992 [1]. In particular, previous studies investigated the applicability of the CCS in major urologic oncological surgeries in the early years; since then, modifications have been made after validation in a large patient cohort to enable the CCS to be more generalized to elective general surgery [2,3]. These procedures have various complications ranging from nonspecific minor to life-threatening conditions; therefore, it appears to be appropriate to grade complications on the basis of the treatments used.
In general, total complication rates are similar between oncological and nononcological surgeries. Elshal et al. [4] demonstrated that the total complication rate in radical cysto-urethrectomy was 24.7% (46 of 186 patients); 25 cases of grade I to II, 12 of grade III, 6 of grade IV, and 3 of grade V. Recently, some efforts have been made to utilize the modified CCS in nononcological procedures as well. As a result, the modified CCS has been more widely used recently than during the early years. Greco et al. [3] applied this grading system in LESS procedures of the upper urinary tract and reported that the overall complication rate was 17% (31 of 192 patients): 4 cases of grade I, 22 of grade II, 4 of grade III, and 1 of grade IV. Additionally, Tefekli et al. [8] used this grading system in percutaneous nephrolithotomy and demonstrated that the system was helpful for understanding the complexity of cases before actual procedures. More recently, Mamoulakis et al investigated the applicability of the modified CCS for grading perioperative complications in patients who underwent TURP [6], and the overall perioperative morbidity rate was 15.7%. Grade I complications occurred in 26 cases out of 44 (59.1%) and grade II events in 13 (29.5%). Grade III or higher complications were not as common (9.1%). The modified CCS was demonstrated to be an easily applied method for grading postoperative TURP complications [6]. Capitan et al. [12] compared the surgical results of GreenLight HPS 120W laser PVP with TURP. In that study, PVP showed similar safety to TURP. Also, Bachmann et al. [13] reported that 180W XPS laser therapy for benign prostatic hyperplasia was a safe treatment modality.
The present study is the first investigation to report perioperative complications of surgery after the introduction of the Seoul technique as a modified method for HPS-PVP by use of the modified CCS. In this study, the overall complication rate was 17.3%, which was higher than that of previous investigations. However, most of the patients (49 of 59 cases, 83.1%) showed grade I complications (49 of 342 patients, 14.3%), 9 patients showed grade II (2.6% of the overall patients), and only 1 patient showed a grade IIIb complication (0.3%). None of the patients had complications graded IVa or higher. We can conclude that the distribution of all complications in less-invasive procedures differs from that of previous investigations and that we should evaluate complication rates in less-invasive procedures from a different point of view.
Because complications rates within the first month after surgery differ from long-term complication rates, it is difficult to identify exactly the overall results of the treatment. In this study, one patient with neurogenic bladder could not void by himself for over 1 year after surgery, whereas another patient who suffered from bleeding after 3 weeks postoperatively underwent endoscopic coagulation under general anesthesia and was able to overcome the problem. According to the modified CCS, the former patient had a grade I complication, whereas the latter had a grade IIIb complication. However, because the grade IIIb complication was completely resolved, it is difficult to accept that the patient with the grade I complication had a more minor complication from a quality of life perspective. In addition, the classification system does not indicate anything about the degree of disease improvement [14]. Therefore, it would be optimal to report early and long-term complications together to avoid such misinterpretations. In particular, less-invasive procedures have a higher likelihood of having lower grade complications.
Thus, we may consider it helpful to attach greater importance to complications that persist for more than 1 month or to make to a new subgrade to predict possible long-term complications. For example, we may consider adding new subgrades such as grade IF, IIF, and IIIF for functional problems that may persist longer than 1 month after surgery. Grade IF is a group of patients who have urinary incontinence or urinary symptoms that do not need treatment with medication. Grade IIF is a group for which medications are necessary. Grade IIIF is a state for which long-term interventions such as intermittent catheterization and suprapubic or urethral catheter indwelling are helpful. Otherwise, we could classify the complications according to duration of symptoms including long-term complications over 1 month. Further study with a larger group would be helpful to suggest new classifications for less-invasive surgeries.
There are a few limitations to this study. The results of this study are from a retrospective analysis; thus, it was difficult to describe some nonspecific urinary symptoms postoperatively. Also, this study was from a single surgeon at a single center. The period used in this study may not affect the complication rates because the technique does not require a learning curve. With larger-scale studies using data from multiple centers, the accuracy of the findings will be higher.
CONCLUSIONS
The modified CCS has been a useful tool for evaluating and grading postoperative outcomes, but most complications following HPS-PVP have been classified into either grade I or II. Although this modified CCS is useful for communication among clinicians in allowing comparison of surgical outcomes, the classifications need to be revised to acquire higher accuracy and applicability in the evaluation of postoperative complications of HPS-PVP.
Footnotes
The authors have nothing to disclose.
References
- 1.Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery. 1992;111:518–526. [PubMed] [Google Scholar]
- 2.Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213. doi: 10.1097/01.sla.0000133083.54934.ae. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Greco F, Cindolo L, Autorino R, Micali S, Stein RJ, Bianchi G, et al. Laparoendoscopic single-site upper urinary tract surgery: assessment of postoperative complications and analysis of risk factors. Eur Urol. 2012;61:510–516. doi: 10.1016/j.eururo.2011.08.032. [DOI] [PubMed] [Google Scholar]
- 4.Elshal AM, Barakat TS, Mosbah A, Abdel-Latif M, Abol-Enein H. Complications of radical cysto-urethrectomy using modified Clavien grading system: prepubic versus perineal urethrectomy. BJU Int. 2011;108:1297–1300. doi: 10.1111/j.1464-410X.2010.09987.x. [DOI] [PubMed] [Google Scholar]
- 5.Jeong J, Choi EY, Kim IY. Clavien classification of complications after the initial series of robot-assisted radical prostatectomy: the Cancer Institute of New Jersey/Robert Wood Johnson Medical School experience. J Endourol. 2010;24:1457–1461. doi: 10.1089/end.2010.0027. [DOI] [PubMed] [Google Scholar]
- 6.Mamoulakis C, Efthimiou I, Kazoulis S, Christoulakis I, Sofras F. The modified Clavien classification system: a standardized platform for reporting complications in transurethral resection of the prostate. World J Urol. 2011;29:205–210. doi: 10.1007/s00345-010-0566-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mamoulakis C, Skolarikos A, Schulze M, Scoffone CM, Rassweiler JJ, Alivizatos G, et al. Results from an international multicentre double-blind randomized controlled trial on the perioperative efficacy and safety of bipolar vs monopolar transurethral resection of the prostate. BJU Int. 2012;109:240–248. doi: 10.1111/j.1464-410X.2011.10222.x. [DOI] [PubMed] [Google Scholar]
- 8.Tefekli A, Ali Karadag M, Tepeler K, Sari E, Berberoglu Y, Baykal M, et al. Classification of percutaneous nephrolithotomy complications using the modified clavien grading system: looking for a standard. Eur Urol. 2008;53:184–190. doi: 10.1016/j.eururo.2007.06.049. [DOI] [PubMed] [Google Scholar]
- 9.Wezel F, Mamoulakis C, Rioja J, Michel MS, de la Rosette J, Alken P. Two contemporary series of percutaneous tract dilation for percutaneous nephrolithotomy. J Endourol. 2009;23:1655–1661. doi: 10.1089/end.2009.0213. [DOI] [PubMed] [Google Scholar]
- 10.Rassweiler JJ, Teber D, Frede T. Complications of laparoscopic pyeloplasty. World J Urol. 2008;26:539–547. doi: 10.1007/s00345-008-0266-z. [DOI] [PubMed] [Google Scholar]
- 11.Son H, Ro YK, Min SH, Choo MS, Kim JK, Lee CJ. Modified vaporization-resection for photoselective vaporization of the prostate using a GreenLight high-performance system 120-W Laser: the Seoul technique. Urology. 2011;77:427–432. doi: 10.1016/j.urology.2010.06.034. [DOI] [PubMed] [Google Scholar]
- 12.Capitan C, Blazquez C, Martin MD, Hernandez V, de la Pena E, Llorente C. GreenLight HPS 120-W laser vaporization versus transurethral resection of the prostate for the treatment of lower urinary tract symptoms due to benign prostatic hyperplasia: a randomized clinical trial with 2-year follow-up. Eur Urol. 2011;60:734–739. doi: 10.1016/j.eururo.2011.05.043. [DOI] [PubMed] [Google Scholar]
- 13.Bachmann A, Muir GH, Collins EJ, Choi BB, Tabatabaei S, Reich OM, et al. 180-W XPS GreenLight laser therapy for benign prostate hyperplasia: early safety, efficacy, and perioperative outcome after 201 procedures. Eur Urol. 2012;61:600–607. doi: 10.1016/j.eururo.2011.11.041. [DOI] [PubMed] [Google Scholar]
- 14.Morgan M, Smith N, Thomas K, Murphy DG. Is Clavien the new standard for reporting urological complications? BJU Int. 2009;104:434–436. doi: 10.1111/j.1464-410X.2009.08516.x. [DOI] [PubMed] [Google Scholar]