

Abstract
The azygos lobe is a well-known and well-described anatomical variation of the right lung. Primary lung cancer arising from an azygos lobe, however, is exceedingly rare. Only a handful of cases have been previously reported in the literature. We report the first case with operative demonstration of a primary adenocarcinoma arising from an azygos lobe, which was treated with robot-assisted azygos lobectomy.
Keywords: Azygos lobe, Robot-assisted thoracoscopic surgery, Non-small-cell lung cancer
INTRODUCTION
The azygos lobe is one of the most common lung malformations; it ordinarily occurs on the right with rare association with the left upper lobe [1]. It is formed by a defect in migration of the azygos vein during embryonic development, resulting in a lobe detached from the superior-medial portion of the upper lobe of the lung above the hilum by a fold of parietal pleura containing the azygos vein [2]. The latter occupies the bottom of the fissure that separates the azygos lobe from the rest of the right upper lobe. The incidence of an azygos lobe has been reported to be ∼1% [1]. We herein report an extremely unusual case of primary adenocarcinoma arising from an azygos lobe of the right lung treated with robot-assisted lobectomy of the azygos lobe.
CASE REPORT
A 74-year old male smoker with chronic obstructive pulmonary disease was found to have a 2-cm solitary nodule in the azygos lobe of the right lung (Fig. 1). The azygos lobe was supplied by segmental branches (B1a and B2a, A1a and A2a and V1a and V2a) of the bronchovascular trees of the right upper lobe. Conventional CT guided biopsy of this lesion was inconclusive. Robot-assisted right upper azygos lobectomy and mediastinal lymph node dissection was performed (Supplementary Video 1).
Figure 1:

Computed tomography of the chest showing the tumour within the azygos lobe (thick arrow).
Supplementary Video 1:

Robot-assisted azygos lobectomy of the right upper lobe.
Initial exploration revealed an azygos lobe that was completely separate from the remainder of the right upper lobe (Fig. 2A). The arcuate vein was located anteriorly with visualization of its entrance at the superior vena cava. A curtain of pleura, the so-called mesoazygos pleura, separated the azygos lobe from the right upper lobe (Fig. 2B). The azygos vein was not fixed to the mediastinum and was well mobilized. The tumour itself did not invade the pleura or extend into the rest of the right upper lobe. The azygos lobe was fully mobilized circumferentially without difficulty. The venous drainage branching from the azygos vein was identified and divided. The bronchovascular pedicle was then divided using an Endo GIA stapling device (Fig. 2C). Systematic mediastinal lymph node dissection including superior mediastinal, paratracheal and subcarinal areas was then performed. The tumour measured 2 cm in greatest dimension and the final pathological diagnosis was moderately differentiated adenocarcinoma with negative lymph nodes or pleural extension (pT1a N0 M0, stage IA). Surgical margin was free of disease. Postoperative course was uneventful. The patient was discharged on the second postoperative day.
Figure 2:
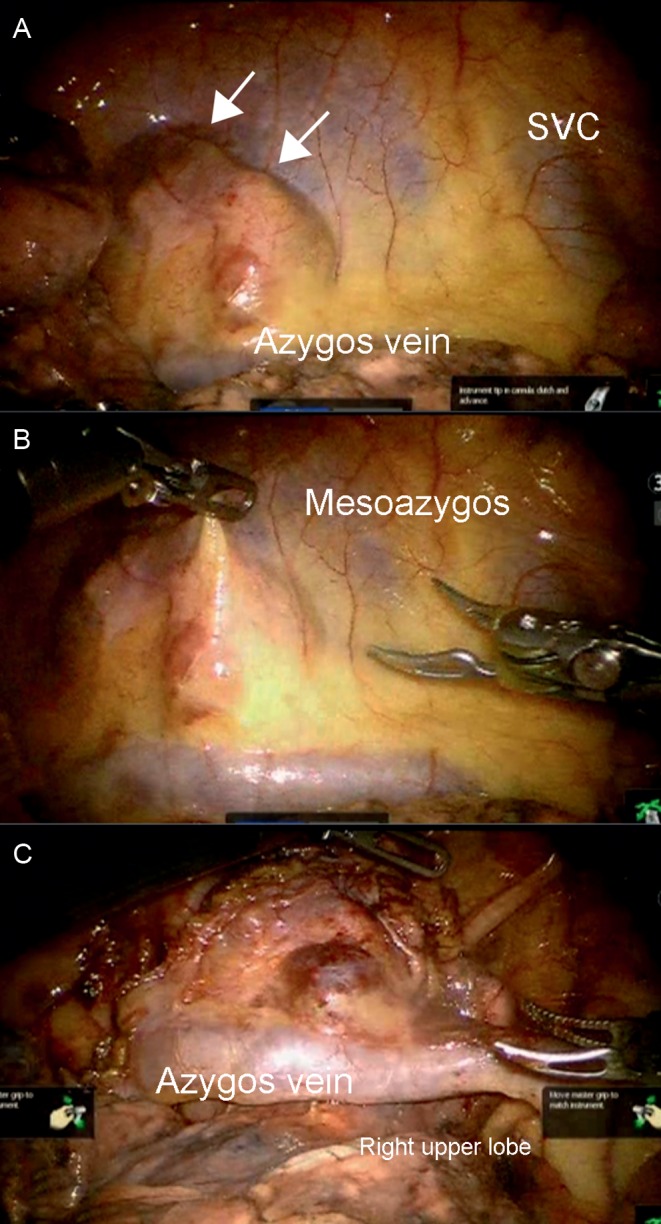
Operative images of robot-assisted thoracoscopic azygos lobe lobectomy.
DISCUSSION
An azygos lobe is a well-known anatomical variation of the right lung. Primary lung cancer arising from an azygos lobe, however, is exceedingly rare. To the best of our knowledge, there have been only three cases reported in the English literature, consisting of two non-small-cell lung cancers (NSCLC) and one small-cell cancer [3]. Of note, none of these cases provided any operative demonstrations. One recently published case report described by an adenocarcinoma associated with an azygos lobe treated video-assisted thoracic surgery (VATS) [1]. However, this lesion did not arise from the azygos lobe itself, but instead originated primarily from the right upper lobe. Therefore, our case is in fact the first VATS (robot-assisted) case with operative demonstration of lung cancer arising from an azygos lobe.
The presence of an azygos lobe is assumed to be of little clinical significance. However, neither the surgical/oncological implication of having a tumour confined to an azygos lobe, nor the reasons for rarity of cancer development in this lobe is known, despite its being a common anatomical variance. One theory hypothesizes that this rarity of cancer development results from decreased ventilation of the azygos lobe. While this is a controversial assumption, the ventilation of an azygos lobe may be relatively limited due to constriction by the azygos vein, possibly resulting in less oxygen delivery and particle deposition of carcinogens thereby restricting carcinogenesis within this lobe despite its apparent segmental or subsegmental bronchovascular supply, as evidenced in the present case.
The controversy concerning this present case is the surgical management. In stage IA NSCLC, the standard surgical management is anatomical lobectomy with mediastinal lymph node dissection. As the azygos lobe is a portion of the right upper lobe isolated by the azygos vein and not a developmentally separate lobe [2], lobectomy of the azygos lobe without concurrent resection of the right upper lobe is considered to be a limited resection and may not be an adequate oncological resection. However, an azygos lobectomy with mediastinal lymph node dissection may be an acceptable therapeutic alternative for elderly individuals with significant medical comorbidities or poor pulmonary function as in the case of our patient, considering better preservation of postoperative pulmonary function and reduced morbidity and mortality [4].
SUPPLEMENTARY MATERIAL
Supplementary material is available at ICVTS online.
Acknowledgments
Conflict of interest: none declared.
REFERENCES
- 1.Arai H, Inui K, Kano K, Nishii T, Kaneko T, Mano H, et al. Lung cancer associated with an azygos lobe successfully treated with video-assisted thoracoscopic surgery. Asian J Endosc Surg. 2012;5:96–9. doi: 10.1111/j.1758-5910.2011.00125.x. doi:10.1111/j.1758-5910.2011.00125.x. [DOI] [PubMed] [Google Scholar]
- 2.Ndiaye A, Ndiaye NB, Ndiaye A, Diop M, Ndoye JM, Dia A. The azygos lobe: an unusual anatomical observation with pathological and surgical implications. Anat Sci Int. 2012;87:174–8. doi: 10.1007/s12565-011-0119-5. doi:10.1007/s12565-011-0119-5. [DOI] [PubMed] [Google Scholar]
- 3.Imširović B, Mekić-Abazović A, Omerhodžić I, Zerem E, Vegar-Zubović S. Atypical localization of lung cancer located in lobus v. azygos. Med Glas Ljek komore Zenicko-doboj kantona. 2012;9:408–11. [PubMed] [Google Scholar]
- 4.Wisnivesky JP, Henschke CI, Swanson S, Yankelevitz DF, Zulueta J, Marcus S, et al. Limited resection for the treatment of patients with stage IA lung cancer. Ann Surg. 2010;251:550–4. doi: 10.1097/SLA.0b013e3181c0e5f3. doi:10.1097/SLA.0b013e3181c0e5f3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.