

Abstract
Mesenteric cysts are rare abdominal tumours. They are found in the mesentery of small bowel (66%) and mesentery of large intestine (33%), usually in the right colon. Very few cases have been reported of tumours found in mesentery of descending colon, sigmoid or rectum. Mesenteric cysts do not show classical clinical findings and are detected incidentally during imaging due to absent or non-specific clinical presentation or during management of one of their complications. Ultrasonography (USG)/computed tomography (CT)/ magnetic resonance imaging (MRI) are used in diagnosing mesenteric cyst but they cannot determine the origin of cyst. Laparoscopy not only helps in diagnosing the site and origin of the mesenteric cyst but also has a therapeutic role. Laparoscopic treatment of mesenteric cyst is a safe, preferred method of treatment and is a less-invasive surgical technique. Here, we present an unusual case of mesenteric cyst arising from the sigmoid mesocolon treated by laparoscopic excision.
Keywords: Benign, laparoscopy, mesenteric cyst, mesocolon, sigmoid
INTRODUCTION
Mesenteric cysts are uncommon benign tumours with an incidence of 1/10,500-25,000 adult surgical patients.[1] Mesenteric cysts rarely cause abdominal symptoms. The most common symptom is chronic undefined abdominal pain. Mesenteric cysts are usually diagnosed with imaging modalities like USG, CT scan or MRI, which determine the exact site of the cyst but cannot detect the cyst origin. Laparoscopy plays a vital role in the diagnosis of cyst, its site, origin and has a therapeutic role in the same sitting. Surgical excision of the cyst is the treatment of choice. We report a rare case of mesenteric cyst arising from sigmoid mesocolon in a middle-aged female patient diagnosed on imaging confirmed and treated by laparoscopic method.
CASE REPORT
A 42-years old female patient was admitted for vague intermittent lower abdominal pain, mainly in hypogastrium and left iliac fossa since 1 year. Physical examination revealed a palpable mobile intra-abdominal lump in left lower quadrant and was bimanually palpable on per vaginal examination. All laboratory investigations were within normal limits (including CA 125). USG and CT revealed a well-defined cystic lesion of size 5 × 6 cm in posterior and superior to the bladder with no evidence of septations, calcification or enhancement on post-contrast studies, likely to be mesenteric cyst [Figure 1]. Both ovaries and uterus were found to be normal.
Figure 1.
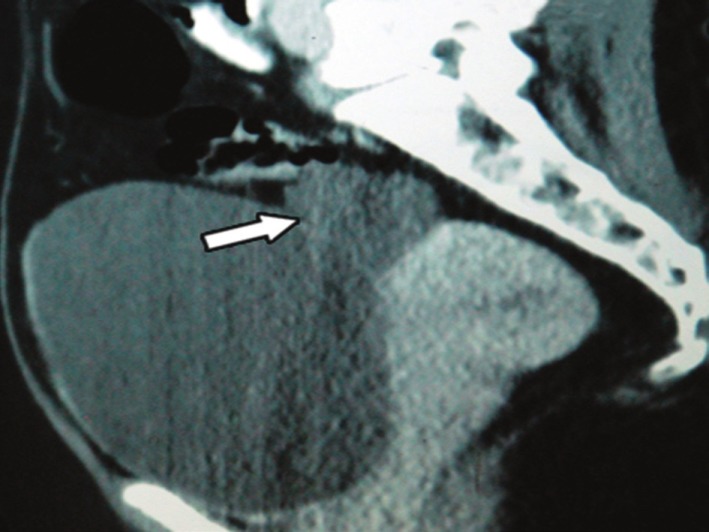
Arrow- Computed tomography shows well-defined cystic lesion of size 5 × 6 cm, posterior and superior to the bladder
Laparoscopic exploration was done to confirm the site and origin of the mesenteric cyst. Three trocars were used: a 10 mm trocar was placed at the midline, 2 cm below the umbilicus: two 5 mm trocar were placed lateral to the rectus abdominus muscle in the right and left lower quadrant. It revealed the presence of 5 × 6 cm cystic swelling arising from mesentery of sigmoid colon [Figure 2]. Cyst was dissected carefully from the mesentery by sharp and blunt dissection. After complete cyst excision, it was put into an endobag. Cyst was aspirated (clear fluid) and was then removed with the endobag through 10-mm trocar site. The final pathological diagnosis was benign lymphangioma. Patient was discharged on the first postoperative day. She was symptom-free at 2 years follow-up.
Figure 2.
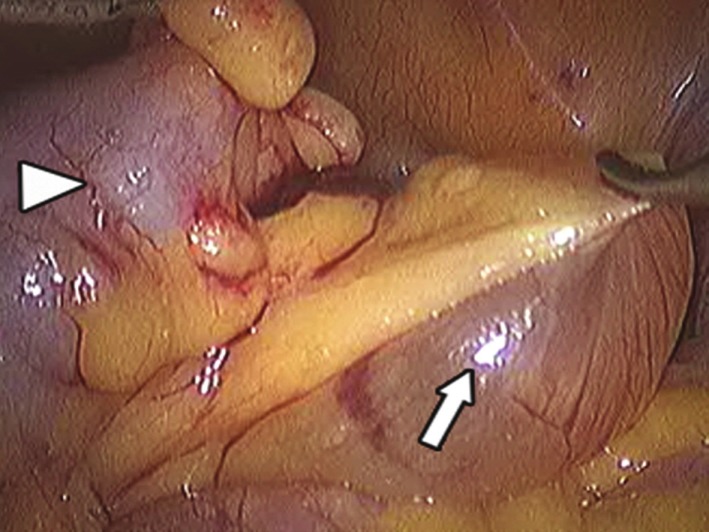
Arrow- Mesenteric cyst arising from mesentery of sigmoid mesocolon. Arrow head- Sigmoid colon
DISCUSSION
Primary mesenteric cysts are rare abdominal findings. These are usually found in the mesentery of the small bowel (66%), mesentery of large intestine (33%), usually in the right colon. Very few cases have reported cysts present in the mesentery of the descending colon, sigmoid or rectum (around 1%), including our case.[2]
Mesenteric cyst was first described in 1507 by Benevieni, a Florentine anatomist. In 1880, Tillaux performed the first successful resection of cystic tumour of mesentry.[3] Pean reported the first marsupialisation of mesenteric cyst in 1883. First laparoscopic resection was done by Mackenzie.
The aetiology of mesenteric cyst is variable.[2,3] These usually arise from developmental abnormalities of the mesenteric lymphatics or from their traumatic rupture. Simple lymphatic and mesothelial cysts are most likely congenital, while the benign cystic mesothelioma is frequently associated with a history of previous pelvic inflammatory process or surgery and endometriosis.[3]
Mesenteric cyst occur with very small incidence, usually in fifth decade and with female predominance. Cystic lymphangioma is the only exception that mostly occurs in the first decade of life (up to 12 yrs of age) with male predominance.[3]
Mesenteric cysts are mostly asymptomatic and if present, symptoms are quite non-specific.[4] Most of these cysts are discovered incidentally during an abdominal imaging done for another reason. USG and CT scan can distinguish between solid and cystic characteristics of abdominal mass. MRI is most accurate in the diagnosis of the cyst origin as compared to CT scan.
Surgical excision of mesenteric cyst is the preferred method of treatment.[5] Recently laparoscopic cyst excision or resection have been advocated in many centres and is well-documented. There are no larger series of laparoscopic excision of mesenteric cysts done to allow more thorough evaluation of this technique. Shimura et al. has reported two cases of successful resection of mesenteric cysts (cyst contents were aspirated before excision for easy handling) located in mesentery of caecum and ascending colon. Vu et al. have also documented total laparoscopic excision of mesenteric cyst where cyst content was aspirated after adequate mobilization for easy extraction. Dursun et al. have reported a case of laparoscopic enucleation of mesenteric cyst of ileum. Depending on the size and site of mesenteric cyst where difficulty is faced for easy handling, aspiration of cyst is done initially or at a later stage to ensure safe and complete excision in order to prevent recurrences or risk of malignant transformation (<3%). Though the operating time is longer with laparoscopy, it has advantages of minimal access, which includes less postoperative pain, shorter hospital stay, early return to normal activity and better cosmesis. In the present case, diagnostic laparoscopy was done with total excision of mesenteric cyst. Mesenteric cysts have good prognosis and no recurrence have been reported following complete excision of the cyst. Hence, laparoscopic cyst removal is the preferred approach and can be done without any complications in properly selected patients. There are no studies available to compare and contrast laparoscopic excision of mesenteric cysts in the small bowel versus colonic/sigmoid mesentery.
ACKNOWLEDGEMENT
This article will be incomplete if we do not acknowledge the efforts of Dr. Sushant Supe, Dr. Sudarshan Daga and Anil Ghandat who helped us prepare this paper with great enthusiasm. Also our sincere and heartfelt thanks to Padmashree Dr. T P Lahane, Dean, GMC and Sir JJ Group of Hospitals for guiding and permitting us to publish this article.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kwan E, Lau H, Yuen WK. Laparoscopic resection of a mesenteric cyst. Gastrointest Endosc. 2004;59:154–6. doi: 10.1016/s0016-5107(03)02365-4. [DOI] [PubMed] [Google Scholar]
- 2.Al Mulhim AA. Laparoscopic excision of a mesenteric cyst during pregnancy. JSLS. 2003;7:77–81. [PMC free article] [PubMed] [Google Scholar]
- 3.Dursun AS, Gokhan A, Volkan S, Osman S, Cigdem T, Osman ND. Laparoscopic enucleation of mesenteric cyst: A case report. Mt Sinai J Med. 2006;73:1019–20. [PubMed] [Google Scholar]
- 4.Iida T, Suenaga M, Takeuchi Y, Kobayashi T, Tobinaga J, Sakai M. Mesenteric pseudocyst of the Sigmoid Mesocolon. J Gastroenterol. 2003;38:081–5. doi: 10.1007/s00535-003-1200-1. [DOI] [PubMed] [Google Scholar]
- 5.Shamiyeh A, Rieger, Schrenk P, Wayand W. Role of laparoscopic surgery in resection of mesenteric cyst. Surg Endosc. 1999;13:937–9. doi: 10.1007/s004649901140. [DOI] [PubMed] [Google Scholar]