

Abstract
Purpose
The goal of our efforts was to develop a modified drill that allows a safe milling of the dorsal osteophytes located close to the dura.
Methods
Usually a normal high-speed drill is used for the resection of uncarthrotic and spondylophytic bone. In one patient, we used our new high-speed drill close to the dura in an area, which is not easy reachable with a normal drill or a rongeur.
Results
Employing the new drill with a polished tip, the spine surgeon is able to overcome the anatomical restrictions, which he has to face when the anterior approach to the cervical spine. The resection of dorsal osteophytes is easy and safe.
Conclusion
The newly developed drill with the polished tip is a safe and high-quality alternative to conventional drills. Further investigations have to be done, to proof the advantages of the new drill.
Keywords: New drill, Anterior approach, Anterior cervical decompression and fusion, Cervical spine
Objectives
Degenerative disease of the cervical spine is diagnosed in more than 75 % of the population over the age of 65 [1]. Cervical spinal canal stenosis (CSCS) is a leading cause of cervical cord affection, cervical spondylotic myelopathy (CSM), and cervical radiculopathy (CR) in the elderly. Anterior cervical discectomy with fusion is a well-established treatment for symptomatic degenerative cervical disc disease [2, 3]. The anatomical situation, even in elderly people, with an increased diameter of the chest and difficulties in patient positioning during surgery impede the anterior cervical approach and the resection of dorsal osteophytes. The goal of our efforts was to develop a modified drill that allows a safe milling of the dorsal osteophytes located close to the Dura, followed by resection of the posterior longitudinal ligament.
Material
For the blank, a stainless steel material was used with the reference 1.4034. This material is martensitic, rustproof, hardened chrome steel. It is mostly used for cutting tools, scissors, and surgical instruments. The diamond grits are bonded to the blank by means of a special electroplating process as follows.
A preparation nickel layer playing an anti-vibrations role.
An anchorage layer, bonding the grits.
A hard nickel layer to strongly fix the naturally made diamond grits.
The octahedral shape of natural diamond grits allows a high diamond density and regular inter-grit spaces, which are both necessary for an optimal removal of shavings. The grits must be calibrated to ensure an optimal and regular concentration on the instrument. The even distribution will guarantee a perfect concentric rotation of the burr.
The irregular surface of natural diamond grits has very good retentive effects on the nickel-bonding layer and improves the abrasive performance thanks to their sharp cutting edges. For this diamond burr, a medium diamond grit has been used which has 106 μ (Fig. 1).
Fig. 1.
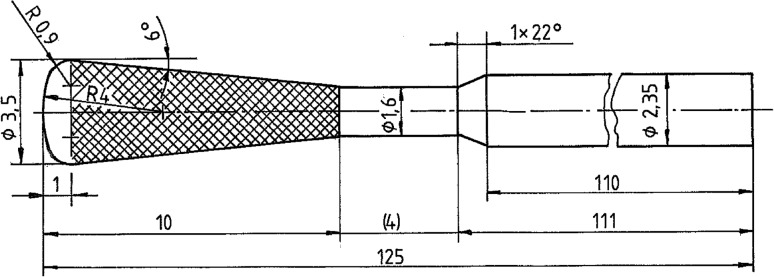
Shape and technical details of the modified drill
Patients and methods
In total, three patients underwent an anterior cervical discectomy with fusion by a spinal canal stenosis with application of the new drill. In two cases, the operative procedure was undertaken on level C5–6 and in one case on C3–4 (Fig. 2). Our operative procedure includes the following steps. (1) Incision of the the anterior longitudinal ligament (ALL) and the annulus fibrosus after exposure of the spine. (2) Insertion of a distraction device (Fig. 3). (3) Resection of dorsally located osteophytes. (4) Usually a high-speed drill for the resection of uncarthrotic and spondylophytic bone. However, care must be taken to avoid relevant drilling of the osseous endplates and injuries of the dura or subdural structures, especially in areas which are not easily reachable with a normal high-speed drill or a rongeur. In our small series with three cases, we saw many advantages in resecting all structures which might compress the dura or spinal cord using the new drill with the polished tip (Fig. 4a–c). (5) Insertion of disc spacer under radiographic control after adequate decompression of the nerve roots and the spinal cord. Figure 2 shows pre–post CT scans of all three cases, demonstrating the effectiveness of the new drill in removing the dorsal osteophytes without any complications (dural injuries, bleeding). The median operation time in all three cases was, with 75 min (63–87 min.), comparable with our usual times before using the new drill (68 min in median).
Fig. 2.

Pre and postoperative computed tomography scans obtained in our series with three patients
Fig. 3.

View of the different shapes of the modified drill
Fig. 4.

Schematic illustration of some of the advantages of the modified drill including overcoming anatomical restrictions during anterior disectomy, especially the resection of dorsal osteophytes
Discussion
As shown in our small series, through employing the new drill with a polished tip, the spine surgeon is able to overcome the anatomical restrictions that he has to face using the anterior approach to the cervical spine, especially the resection of dorsal osteophytes. Furthermore, we had the impression that intraoperative bleeding from the bone was less compared to Kerrison rongeurs. Remarkably, using the new drill, the surgical method is not just comparable to decompression with Kerrison rongeurs; even in patients with a highly degenerated and small intervertebral space, an easy decompression is possible (Fig. 5). We did not experience an injury of the dura in any of the cases with application of the new drill at a speed (rotation) of 40,000 rpm.
Fig. 5.
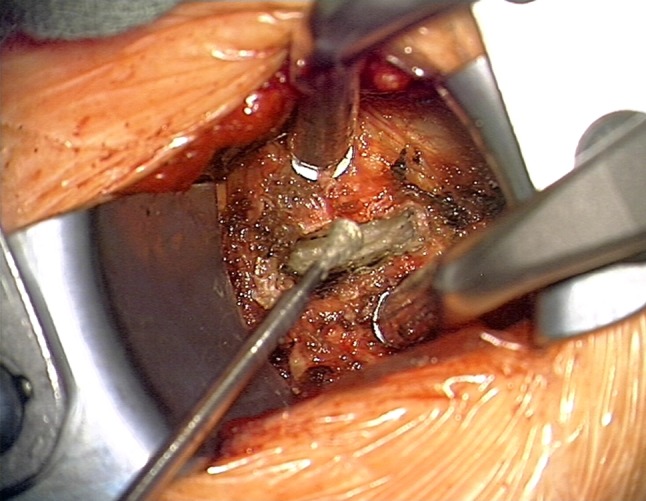
Intraoperative ventral view during an anterior cervical disectomy after insertion of the distraction device
One can suppose that the new drill might be very helpful and easy to use even in the microsurgical treatment of the lateral recess syndrome of the lumbar spine, in particular, in combination of new microinvasive approaches.
Conclusion
The new drill with the polished tip is safe and perhaps a high-quality alternative to conventional drills. Further investigations in randomized prospective trials should be approved to prove its advantages due to rates of complication in the cervical as well as lumbar spinal stenosis. Such trials have already been planned in our institution.
Conflict of interest
None.
References
- 1.Cauthen JC, Kinar RE, Vogler JB, et al. Outcome analysis of noninstrumented anterior cervical discectomy and interbody fusion in 348 patients. Spine. 1998;23:188–192. doi: 10.1097/00007632-199801150-00008. [DOI] [PubMed] [Google Scholar]
- 2.Gore DR, Sepic SB. Anterior discectomy and fusion for painful cervical disc disease: a report of 50 patients with an average follow-up of 21 years. Spine. 1998;23:2047–2051. doi: 10.1097/00007632-199810010-00002. [DOI] [PubMed] [Google Scholar]
- 3.Harrop JS, Hanna A, Silva MT, Sharan A. Neurological manifestations of cervical spondylosis: an overview of signs, symptoms and pathophysiology. Neurosurgery. 2007;60(1 Suppl 1):S14–S20. doi: 10.1227/01.NEU.0000215380.71097.EC. [DOI] [PubMed] [Google Scholar]