

Abstract
Objective. To integrate pharmacy education into a diabetes and hypertension screening program to improve pharmacy student disease knowledge and screening skills and provide a valuable service to the community.
Methods. One hundred eighty third-year PharmD students were trained and subsequently screened people aged ≥35 years in 2 Thai communities. Those with high risk factors were encouraged to see a pharmacist or nurse for further evaluation and referral to a physician for diagnosis.
Results. After training, the third-year students showed significantly higher knowledge scores on diabetes and hypertension than a control group of second-year students (p<0.05). More than 80% of the third-year students were rated by pharmacist observers as having good community screening skills. More than 95% of community participants were satisfied or very satisfied with the screening session. The active screening program improved the screening coverage in the targeted communities from 41 people/month under the passive screening program to 127 people/month and improved the coverage rate over a 6-month period from 24% to 73%.
Conclusion. This active screening project by pharmacy students enhanced the health knowledge and awareness of members of the targeted communities and increased pharmacy students’ knowledge of and ability to screen for hypertension and diabetes.
Keywords: pharmacy education, diabetes, hypertension, screening, service learning
INTRODUCTION
Diabetes mellitus and hypertension are major global health problems. The International Diabetes Federation estimated that in 2011, 366 million people worldwide had diabetes mellitus; its prevalence is expected to increase to 552 million by the year 2030.1 Around 80% of people with diabetes are in low- and middle-income countries such as Thailand.2 The World Health Organization reported that in 2011, 600 million people worldwide had hypertension, and that by the year 2025 they expect the prevalence of that disease to increase to 1.5 billion people.3-5 Hypertension is the third leading cause of death in the world. Because the incidences of diabetes and hypertension are expected to increase and because serious complications from these diseases cause disability, reduction of quality of life, and global mortality, the diseases were identified as the most challenging health problems of the 21st century.6 In Thailand, a country with middle to low income, the Ministry of Public Health (MoPH) reported that hypertension prevalence was 35.82% in people over 15 years of age (17.64 million people) and diabetes prevalence was 6% in Thai male adults and 7% in female adults.7 The main problems for disease management were people’s lack of concern and understanding about these diseases and lack of compliance with treatment. Thailand’s national statistics center reported that among a sample of 100,000 Thai people, 71% were not concerned about their health and did not know whether they had hypertension. In a study of patients newly diagnosed with diabetes, more than 50% had not been previously diagnosed and only 34.2% knew and had subsequently been treated.8,9
The National Health Security Office (NHSO) proposed an improvement plan for health promotion and primary care services in Thailand. For the year 2008, they promoted a screening project through primary care services for early detection of people at risk for diabetes and/or hypertension and to establish lifestyle modification services for those identified as being in the at-risk population.10 Subsequently, the Thai government assigned health services throughout the country to campaign for disease prevention and health promotion in the general population. Screening for diabetes mellitus and hypertension was made a priority. Primary care personnel and health volunteers have been responsible for performing capillary fasting blood glucose tests and blood pressure measurements, while health care professionals such as nurses, pharmacists, and physicians have been responsible for monitoring and educating those patients identified as being at risk.
The Thai Pharmacy Council has cooperated with the Thai Food and Drug Administration to assess suitable pharmacies for accreditation to participate in the NHSO’s primary care project.11,12 An accredited pharmacy can screen people and refer those who are found to be at risk to a physician in a community hospital or medical health center for further evaluation. Patients who were diagnosed with diabetes and/or hypertension and controlled their blood sugar and/or blood pressure within normal limits would be referred back to a primary care provider at the primary care unit (PCU) or to the accredited community pharmacy for monitoring and medication refills. This would reduce the number of hospital visits by these patients.
The Faculty of Pharmacy, Mahasarakham University (MSU), 1 of 3 institutions producing qualified pharmacists in the Northeast region of Thailand, has accepted the concept of health promotion as its institutional mission and policy. Based on the faculty’s philosophy of “be knowledgeable about medicines and able to lead people to promote their healthy lifestyles,” we have integrated the health promotion concept into all courses in the doctor of pharmacy (PharmD) curriculum. This integration gives PharmD students a holistic viewpoint on health and will help them provide health promotion in their future workplace.13,14 Three factors are involved in achieving the faculty’s integrated teaching aim: the mission of the faculty and the integration of education, the mission of the MoPH on primary care services in community settings, and the academic service of the 3 university pharmacies established for students’ practice.
The 3 university pharmacies have been accredited by the Thai pharmacy council and have joined with the government primary care units in the local area to promote primary care services; one of which is chronic disease screening. The MoPH has set the key performance indicator as screening coverage of at least 60% of the population aged ≥35 years in each primary care unit’s area of responsibility. In Thailand, each primary care unit is commissioned to provide health prevention, promotion, treatment, and rehabilitation for 10,000 people in its area.13 There are many thousands of districts in Thailand, which has a population of approximately 70 million. With the high workload of personnel in primary care units, the passive screening practices used in the primary care units and the university pharmacies were not effective in reaching the screening coverage target (60%). Through cooperation among primary care units, university pharmacies, and faculty members, we created an active screening process and jointly agreed on how the screening would be conducted.
The active screening process is the product of integrating pharmacy education, academic service, and primary care service. We trained third-year PharmD students to make home visits to people within designated communities and use a screening questionnaire to screen for diabetes and hypertension under the supervision of a registered pharmacist from a university pharmacy. After detecting that a person is at risk, students invite that person to have their blood glucose and blood pressure measured at 1 of the university pharmacies by a pharmacist or at a primary care unit by a registered nurse. If the tests indicate the person has diabetes or hypertension, the pharmacist or nurse refers the patient to a physician at a hospital to confirm the diagnosis. This active screening process is an innovative solution to supporting primary care services in the university area and reaching the performance indicators for screening coverage in Thai communities. This study describes the integration of PharmD education with the work of university pharmacies to support their coverage of diabetes and hypertension screening in their communities.
METHODS
This quasi-experimental study evaluated and compared the effect of integrating training about diabetes mellitus and hypertension on pharmacy students’ disease screening and community visiting skills. The experimental group was 184 third-year PharmD students. The 2 comparison groups were comprised of 40 second-year students who served as a negative control in that they had not yet received any classroom education regarding diabetes, hypertension, or screening methods, and 40 fourth-year students who served as a positive control in that they had received education in these areas but had not participated in the screening project in their third year. This research was approved by the ethical committee of MSU.
Before this research, all students were taught in theory about community visit skills in the second-year course in social pharmacy. In addition, all study students had learned about community visit skills before the study. However, the control group of the second-year students had not been taught about disease screening skills and the suitable manner in which to conduct themselves when practicing in the real community. The control group of fourth-year students had already been taught about community visits and screening from both training when they were in the third year and from PharmD education in the fourth year from courses in pharmacotherapy, drug system management, and integration.
The third-year students in the study group underwent 1 week of lectures and 3 weeks of community visit skills training by registered pharmacists from the university pharmacies and a registered nurse from a primary care unit. After 1 week of lectures, students’ posttest knowledge on disease and patient screening was assessed using a self-administered validated questionnaire. The control groups’ knowledge was also assessed with this questionnaire.
After completing the training session, third-year students began visiting households in 2 areas served by the university pharmacies: the Takhonyang district and the Nakwichai district. The screening visits were made over 3 months (from June to October 2009). The teams who went to each house consisted of 2 students and either a pharmacist from the university pharmacy or a sixth-year student. Residents of the communities who were willing to participate in the study were asked to sign an informed consent form. One of the students then completed the disease screening form with the resident and provided the person with printed materials on diabetes, hypertension, and the importance of disease screening. If the participant was identified as being at risk for diabetes, the student invited and strongly encouraged the person to visit either 1 of the university pharmacies or 1 of the primary care units to have their blood glucose and blood pressure measured by a pharmacist or nurse.
During the screening, the student’s screening skills were observed and evaluated by the pharmacist or sixth-year PharmD student accompanying the students. The observer used a constructed assessment form to evaluate the following: community visit and screening skills, suitable social interactive manner, self-esteem, and attitude during the community visits.
If the subsequent tests performed by a pharmacist or nurse indicated that the person was at risk for having diabetes and/or hypertension, the patient was referred to a physician at a hospital to confirm the diagnosis and prescribe care.
For the control group, the second-year students were assessed their screening skill and community visit skill when they had visited community in the course of social pharmacy and the fourth-year students were assessed their skills in the course of integration 4 by either a pharmacist or the trained sixth-year students.
After completing the project, the third-year students were interviewed by a sixth-year pharmacy student regarding their opinions about the project. A semi-structured questionnaire with standardized questions was used to ensure consistency of interviews between different groups of students.
Forty-nine of the community residents from 49 (70%) of the 70 families screened were randomly selected to assess the students using a self-administered questionnaire which asked them to rate their satisfaction with the experience on a 5-point Likert scale.
The chi-square test was used to compare the difference in correction skills (satisfied-unsatisfied) between the experimental group and the control group. The independent t test or Mann Whitney U test was used to compare the average knowledge score and skill score between students in the experimental group and those in the control group. The significant differences of the outcomes between groups was set at the level of p<0.05.
RESULTS
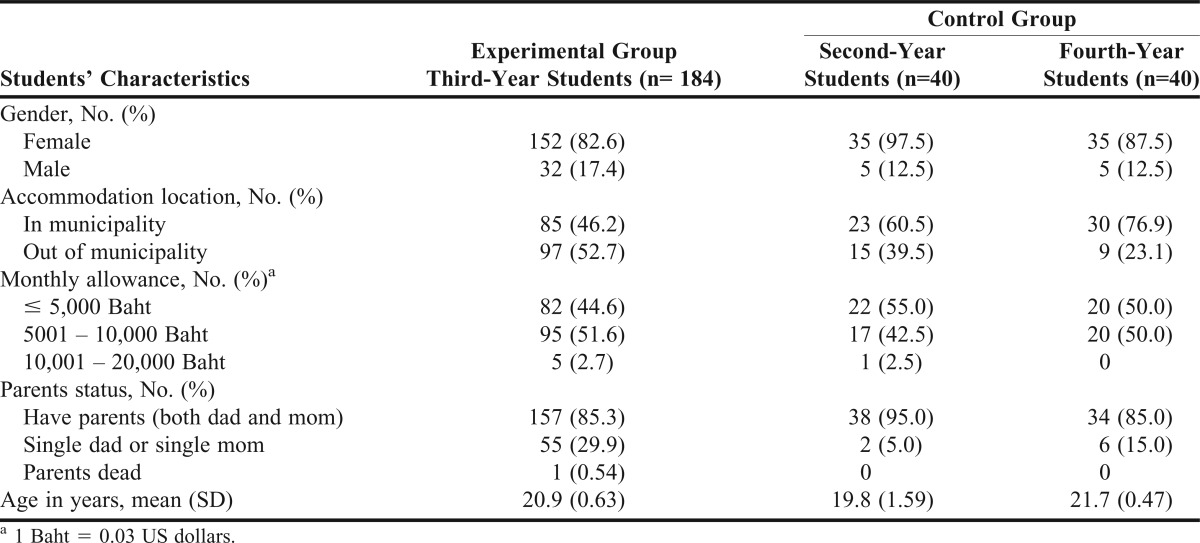
Students within the 3 groups (1 experimental group of third-year students and 2 control groups comprised of second- and fourth-year students, respectively), had similar basic characteristics such as ratio of male to female students, student housing located in or outside the municipality area, monthly allowance from parents or guardians, and parental status (Table 1). Even though their ages were different because of their year of study, they only differed by 1 year.
Table 1.
Basic Characteristics of Pharmacy Students in a Study to Determine the Effectiveness of Integrating Pharmacy Education With Diabetes and Hypertension Screening in Thai Communities (n=264)
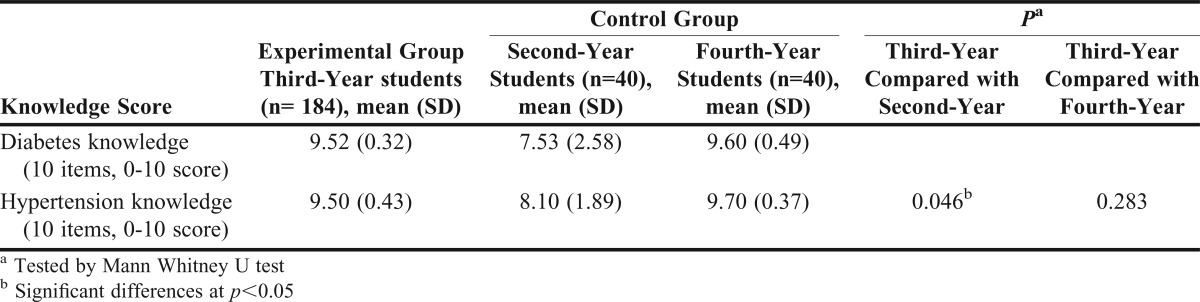
Students in the experimental group (the third-year students) had significantly higher scores in knowledge of diabetes mellitus and hypertension than the control group of second-year students (p=0.038 and p=0.046, respectively). However, there was no significant difference in knowledge between the third-year students and the control group of fourth-year students (Table 2).
Table 2.
Comparison of Knowledge Scores on Diabetes and Hypertension Between Students Who Did and Did Not Participate in a Community Screening Project for Diabetes and Hypertension
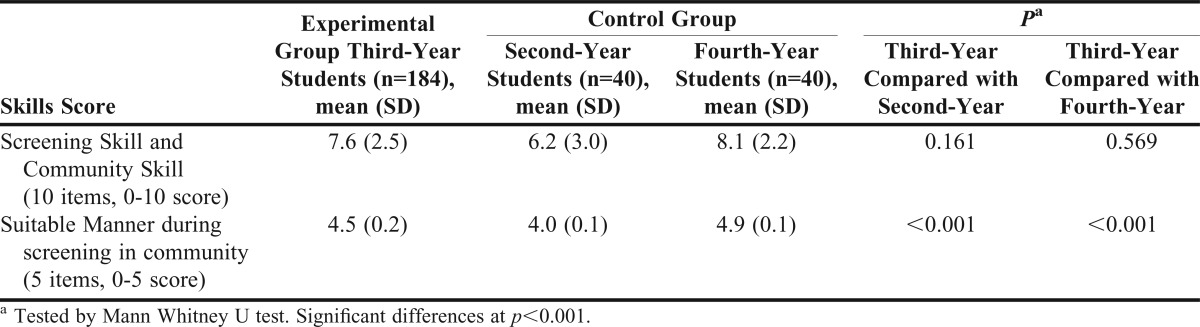
No differences in community visit and disease screening skills scores were found between the experimental group and the control groups. In terms of having a suitable manner during community visits, the fourth-year students had the highest mean score, significantly higher than the experimental group of third-year students (4.9 ± 0.1 and 4.5 ± 0.2 , p<0.001) The experimental group of third-year students had significantly higher scores than the control group of second-year students (4.5 ± 0.2 and 4.0 ± 0.1, p<0.001). These results are shown in Table 3.
Table 3.
Skills Score on Screening, and a Suitable Manner During Screening in the Community of PharmD Students Between the Experimental Group and Control Group
The differences in knowledge between the experimental group and the positive control group was found because the fourth-year students have learned about disease management in PharmD courses when they were in both the third year and the fourth year, whereas the control group of the second-year students had not learned about disease screening skills and suitable manner for visiting community.
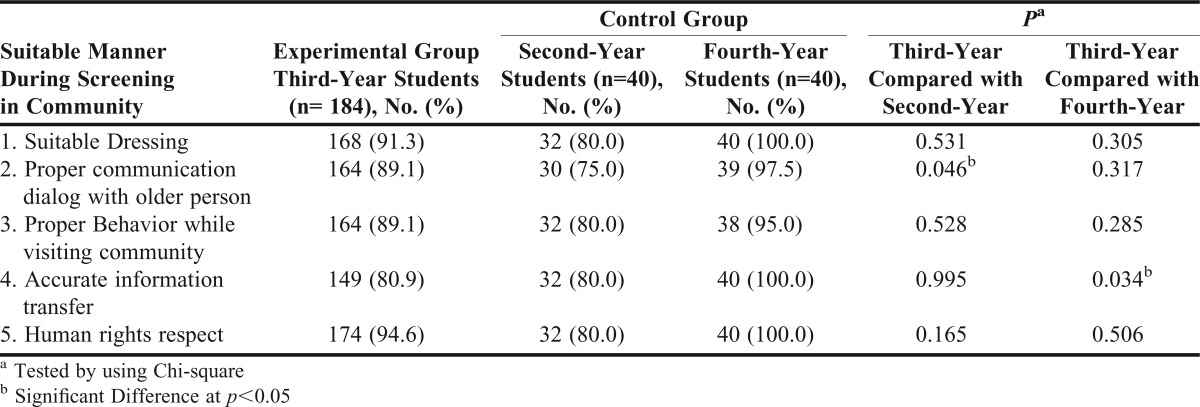
Table 4 shows students’ average score on each item of the suitable manner question, which was rated by a registered pharmacist from 1 of the university pharmacies or a trained sixth-year PharmD student. The results showed that after 1 month of training, the experimental group showed a better manner in the proper communication dialog when interviewing an older person in the community compared with the control group of second-year students (89% vs 75%, p=0.046). However, on the item regarding accurate information transfer, the control group of fourth-year students scored higher than the experimental group (80.9% and 100%, p=0.038).
Table 4.
Number and Percentage of PharmD Students with Suitable Manner During Screening in the Community Between the Experimental Group and Control Group
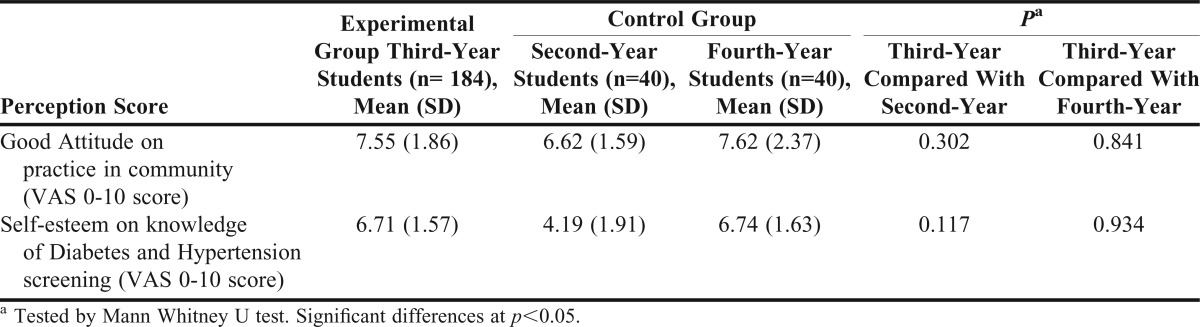
When using the constructed questionnaire to assess students’ self-esteem and attitude regarding practice in the community, no difference was found between the experimental group and the control group (Table 5).
Table 5.
Visual Analog Scale (VAS) Score on Good Attitude on Practice in the Community and Self-Esteem on Diabetes and Hypertension Knowledge Between Experimental Group and Control Group
After completing the active screening in the community, 20 of the third-year students were randomly selected to interview about the project. Two trained sixth-year students used a semi-structured questionnaire to conduct the interview.
From the interview, we found when asked what they liked best about the projects, most of the students stated how the experience allowed them to apply knowledge learned in the classroom in a real-life situation and to provide an active and valuable service for the community.
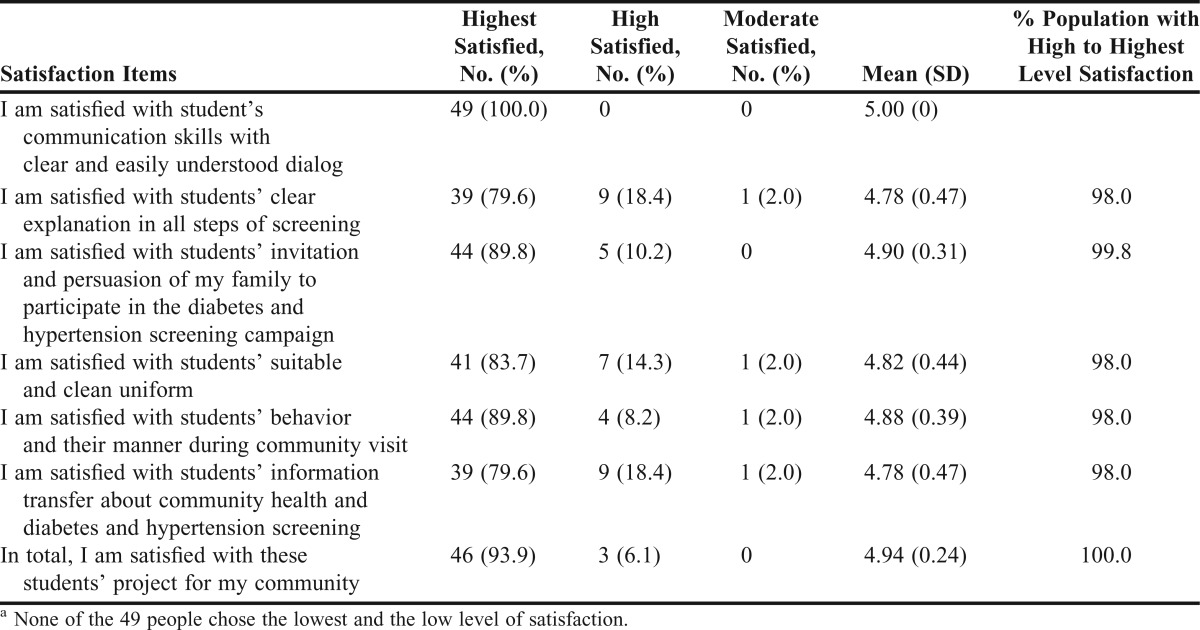
Most of the 49 community residents who completed the post-screening assessment (>95%) were satisfied with the students’ service and rated all questionnaire items at the highest 2 levels.
In terms of the success of the project, the active screening program was more effective than the passive screening. The active screening program had an estimated screening coverage rate over a 6-month of 73.1% compared to a coverage rate of 23.6% under the passive screening program. The active screening program exceeded the 60% target coverage rate set by the MoPH (Table 6).
Table 6.
Satisfaction Score of People in the Community with Third-Year PharmD Students’ Screening Service (n=49)a
DISCUSSION
By integrating health promotion concepts into the PharmD curriculum of MSU, the faculty has established new strategies for teaching and introduced new student learning methods. The network collaborative service, one of those strategies, was developed by the primary care units, university pharmacies, and facutly of pharmacy. To meet the target missions of 3 institutes, the active screening in communities by PharmD students was initiated. Students’ knowledge and skills and screening coverage improvement were the successful indicators.
Most of the students behaved in a suitable manner during the active screening visits and demonstrated good practice skills while they worked in the community. More than 95% of people who completed the satisfaction survey instrument were satisfied with this active screening program. Active screening in the community by students also enhanced customers’ health knowledge and improved the screening coverage from the passive screening rate of 41 persons/month to 127 persons/month, or by 209.8%.
This active screening project fulfilled the main mission of the PharmD program to produce qualified pharmacists who are able to integrate knowledge into real practice in the community. It also fulfilled the mission of the accredited university pharmacy as a primary care provider in screening diseases. In addition, it fulfills the target of the national campaign on diabetes and hypertension for screening people aged ≥ 35 years in Thai communities.
CONCLUSION
The integration of PharmD education with the academic services of the university pharmacies and the services of the primary care units in providing an active screening service enhanced third-year students’ knowledge of diabetes and hypertension and their screening technique. This was demonstrated when they were compared with the second-year students who were used as a control group.
ACKNOWLEDGEMENTS
This study received financial support from the Health Promotion Association and the Faculty of Pharmacy, Mahasarakham University. We would like to thank Professor RME Richards, the Founding Dean of the Faculty of Pharmacy MSU, for his kind contributions on grammatical correction and useful suggestions for this study.
REFERENCES
- 1.International Diabetes Federation. Diabetes Atlas, 3rd ed. Brussels, Belgium: International Diabetes Federation; 2006. [Google Scholar]
- 2.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047–1053. doi: 10.2337/diacare.27.5.1047. [DOI] [PubMed] [Google Scholar]
- 3.Fleming BB, Greenfield S, Engelgan MM, Pogach LM, Clauser SB, Parrott MA. The diabetes quality improvement project: moving science into health policy to gain an edge on the diabetes epidemic. Diabetes Care. 2001;24(10):1815–1820. doi: 10.2337/diacare.24.10.1815. [DOI] [PubMed] [Google Scholar]
- 4.Aekohakorn W, Stolk RP, Neal B, et al. The prevalence and management of diabetes in Thai adults: the international collaborative study of cardiovascular disease in Asia. Diabetes Care. 2003;26(10):2758–2763. doi: 10.2337/diacare.26.10.2758. [DOI] [PubMed] [Google Scholar]
- 5.Wolf-Maier K, Cooper RS, Kramer H, et al. Hypertension treatment and control in five European countries, Canada, and the United States. Hypertension. 2004;43(1):10–17. doi: 10.1161/01.HYP.0000103630.72812.10. [DOI] [PubMed] [Google Scholar]
- 6.Chobanain AV, Bakris Gl, Black HR, et al. Seventh report of the Joint National Committee on prevention, detection, evaluation and treatment of high blood pressure. Hypertension. 2003;42(6):1206–1252. doi: 10.1161/01.HYP.0000107251.49515.c2. [DOI] [PubMed] [Google Scholar]
- 7.Faculty of Pharmacy, Mahasarakham University. Development a connection between accredited drugstores and the national health insurance for disease screening and monitoring 2009. 2010 19 April 2010. http://www.kpi.msu.ac.th/upload/ag_tor_ref_bymst/ag_16_in_4.1.1_4_92.pdf. Accessed October 10. [Google Scholar]
- 8.Bunnag P, Plengvidhya N, Deerochanawong C, et al. Thailand diabetes registry project: prevalence of hypertension, treatment and control of blood pressure in hypertensive adults with type 2 diabetes. J Med Assoc Thai. 2006;89(Suppl 1):S72–S77. [PubMed] [Google Scholar]
- 9.Bureau of information. News for public relations. Ministry of Public Health. 2009 April 23, 2007. http://www.moph.go.th/ops/iprg/include/admin_hotnew/show_hotnew.php?idHot_new=4842.. Accessed September 9. [Google Scholar]
- 10.Mungklaton N. Screening Chronic Diseases in the New Patients by the Cooperation Between Accredited Drugstores and Primary Care Units. [PharmD thesis]. Maha Sarakham, Thailand: Faculty of Pharmacy, Mahasarakham University; 2008. [Google Scholar]
- 11.Chaiyasong S. Primary Care Service of Drugstore in the Health Insurance: Case Study of University Pharmacy Under the Universal Coverage Project. [Special problem report]. Maha Sarakham, Thailand: Faculty of Pharmacy, Mahasarakham University; 2005. [Google Scholar]
- 12.Thongroj P. Drug system situation. 2009 January 16, 2008. http://www.medicthai.net/admin/news_cpe_detail.php?id=318.. Accessed October 28. [Google Scholar]
- 13.Sookaneknun P, Suttajit S, Ploylearmsang C, Kanjanaslip J, Maleewong U. Health promotion integrates into a Thai PharmD curriculum to improve pharmacy practice skills. Am J Pharm Educ. 2007;73(5):Article 78. doi: 10.5688/aj730578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Faculty of Pharmacy, Mahasarakham University. Health promotion project in faculty of pharmacy. May 20, 2008. 2010 http://www.plan.msu.ac.th/kpi/upload/ag_tor_ref_bymst/ag_16_in_2.1.2_1_417.pdf . Accessed December 15. [Google Scholar]