

Abstract
OBJECTIVE
The two major classes of antidiabetic drugs, sulfonylureas and metformin, may differentially affect macrovascular complications and mortality in diabetic patients. We compared the long-term effects of glipizide and metformin on the major cardiovascular events in type 2 diabetic patients who had a history of coronary artery disease (CAD).
RESEARCH DESIGN AND METHODS
This study is a multicenter, randomized, double-blind, placebo-controlled clinical trial. A total of 304 type 2 diabetic patients with CAD, mean age = 63.3 years (range, 36–80 years), were enrolled. Participants were randomly assigned to receive either glipizide (30 mg daily) or metformin (1.5 g daily) for 3 years. The primary end points were times to the composite of recurrent cardiovascular events, including death from a cardiovascular cause, death from any cause, nonfatal myocardial infarction, nonfatal stroke, or arterial revascularization.
RESULTS
At the end of study drug administration, both groups achieved a significant decrease in the level of glycated hemoglobin (7.1% in the glipizide group and 7.0% in the metformin group). At a median follow-up of 5.0 years, 91 participants had developed 103 primary end points. Intention-to-treat analysis showed an adjusted hazard ratio (HR) of 0.54 (95% CI 0.30–0.90; P = 0.026) for the composites of cardiovascular events among the patients that received metformin, compared with glipizide. The secondary end points and adverse events were not significantly different between the two groups.
CONCLUSIONS
Treatment with metformin for 3 years substantially reduced major cardiovascular events in a median follow-up of 5.0 years compared with glipizide. Our results indicated a potential benefit of metformin therapy on cardiovascular outcomes in high-risk patients.
The prevalence of type 2 diabetes has been increasing rapidly throughout the world during the past decades (1). Since cardiovascular disease is the major complication of type 2 diabetes, and cardiovascular mortality accounts for the majority of diabetic patient deaths, there has been growing interest in developing strategies for blood glucose control in type 2 diabetic patients to reduce cardiovascular risk and mortality (2–6).
Among various oral glucose-lowering medications, metformin and sulfonylureas have been the mainstay treatments for type 2 diabetes. Several studies have examined the effects of these medications on cardiovascular risk among diabetic patients; the results, however, are inconsistent (2,7–9). In an early, large-scale, randomized trial, an increased risk of cardiovascular mortality was observed in diabetic patients treated with sulfonylurea (tolbutamide) or biguanide (phenformin) medications (7,8). Some other studies suggest that these two classes of medications might differentially affect cardiovascular risk (9–14). For example, in the open-label UK Prospective Diabetes Study (UKPDS) (9), it was found that diabetic patients with metformin treatment had a reduced risk of macrovascular and microvascular complications as well as all-cause mortality compared with those treated with sulfonylurea or insulin. However, the combined treatment of metformin and sulfonylurea led to an increased risk of all-cause mortality. Taken together, how these two major hypoglycemic agents may affect cardiovascular risk and mortality among diabetic patients remains unclear.
Therefore, we performed a randomized, double-blind, placebo-controlled trial to compare the effects of the two major classes of blood glucose–lowering agents, sulfonylurea (glipizide) and metformin, on the cardiovascular events and mortality in 304 Chinese type 2 diabetic patients who had a history of coronary artery disease (CAD).
RESEARCH DESIGN AND METHODS
Study design and participants
The Study on the Prognosis and Effect of Antidiabetic Drugs on Type 2 Diabetes Mellitus with Coronary Artery Disease (SPREAD-DIMCAD) was a prospective, randomized, double-blind, placebo-controlled trial that evaluated the different effects of glipizide and metformin on the major cardiovascular events and mortality among type 2 diabetic patients with a history of CAD. The patients were recruited from 15 clinical centers in China. The study was approved by the institutional review board of Ruijin Hospital, and written informed consent was obtained from each patient. The study was conducted in accordance with the principles of the Declaration of Helsinki.
The targeted participants in the current study were patients with both type 2 diabetes and CAD. The eligibility criteria included the following: 1) diagnosed as CAD by either having a history of acute myocardial infarction diagnosed by a representative set of electrocardiograms, cardiac enzyme values, and typical symptoms or by angiographically identified stenosis of >50% of lumen diameter in at least one major epicardial coronary artery (15); 2) diagnosed as type 2 diabetic according to the 1999 World Health Organization criteria (fasting plasma glucose ≥7 mmol/L and/or 2-h oral glucose tolerance test ≥11.1 mmol/L (16) and fasting plasma glucose <15 mmol/L); and 3) no more than 80 years of age (both men and women). The exclusion criteria included the following: 1) severe liver dysfunction, including serum alanine aminotransferase concentration >2.5 times above the upper limit of normal range and abnormal renal function (serum creatinine >132 μmol/L); 2) severe dysfunction of the heart (New York Heart Association class >phase III); 3) psychiatric disease, severe infection, severe anemia, or neutropenia; 4) other severe organic heart diseases, including, but not limited to, congenital heart disease, rheumatic heart disease, and hypertrophic or dilated cardiomyopathy; 5) pregnant or lactating; 6) allergic to study drugs; 7) using insulin therapy for type 2 diabetes and could not be changed to oral glucose-lowering drugs; and 8) recent drug or alcohol abuse.
The primary study end points were the composite of recurrent cardiovascular events, including nonfatal myocardial infarction, nonfatal stroke or arterial revascularization by percutaneous transluminal coronary angioplasty (PTCA) or by coronary artery bypass graft, death from a cardiovascular cause, and death from any cause. The end points were obtained and confirmed by the medical records and death certificates that were kept in each center. The secondary cardiovascular end points included new or worsening angina, new or worsening heart failure, new critical cardiac arrhythmia, and new peripheral vascular events. Other adverse events, including hypoglycemia (severe hypoglycemia in which the subject required assistance and/or a plasma glucose level <56 mg/dL [3.1 mmol/L] was recorded as a hypoglycemic attack and would be reported in this manuscript) and microvascular complications, were also monitored.
Randomization and study medication
After a 2-week run-in period, the eligible study participants were required to withdraw from all antidiabetic agents and were randomly assigned in double-blind to receive either glipizide plus metformin placebo or metformin plus glipizide placebo for 3 years. The baseline metabolic values were obtained immediately after the withdrawal of previous antidiabetic therapy. The randomization codes were generated by the study’s biostatistician at Shanghai Jiao Tong University School of Medicine. Study sites did not have access to the codes.
For both groups, the targeted glycated hemoglobin level was <7.0%, the fasting blood glucose concentration was <7 mmol/L, and the postload 2-h blood glucose concentration was <10 mmol/L. The study drugs and the matched placebo were prepared in indistinguishable tablets. For the glipizide group, the initial dose was 15 mg daily (5 mg per one pill, three times daily) and titrated to 30 mg (10 mg per two pills, three times daily) within 3 months, if not to target. The mean daily dose of glipizide was 28.3 ± 3.9 mg. For the metformin group, the initial dose was 0.75 g daily (0.25 g per one pill, three times daily), and titrated to 1.5 g (0.5 g per two pills, three times daily) within 3 months, if not to target. The mean daily dose of metformin was 1.4 ± 0.2 g. After 3 months, insulin was added for patients with the maximum dose of study drug administration in either group who did not achieve targeted glucose control level (see Supplementary Data). Lifestyle intervention and other treatments for CAD and modifiable cardiovascular risk factors were identical in both groups through all research centers according to the recommendation of the Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III) (17).
The study drug administration was 3 years for each participant. The follow-up for primary end points began at randomization and continued until the end of the study. The original protocol invited all participants to continue with the follow-up of primary outcomes until the end of the whole study (last subject finished the study drug administration) after the initial 3-year study drug administration. In the postdrug follow-up period, the primary end points were obtained and no attempts were made to maintain their previous therapies. During study drug administration, information on adherence and tolerability of study drugs, concomitant medication, adverse events, and occurrence of study outcomes were collected, and physical examination, vital signs, and plasma glucose concentrations were obtained. Glycated hemoglobin levels were measured at 6, 12, 18, 24, 30, and 36 months (extra results might be required according to the investigator’s judgment), and lipid concentration, biochemical safety laboratory analysis, electrocardiograms, and echocardiographic results were obtained.
Ruijin Hospital served as the coordinating center. There was no central laboratory for biochemical analysis for the study.
Statistical analysis
This study was designed in accordance with a predetermined statistical analysis plan. Given a constant rate of events of 10% per year, a sample size of 150 patients in each of the two study groups would provide an 85% power at a type 1 error rate of 0.05 to detect a 30% reduction in the relative risk of the composite primary outcomes during the follow-up. This analysis was designed to test the primary hypothesis that glipizide and metformin would have a different effect on the recurrence of composite cardiovascular events. The follow-up for primary end points began at randomization and continued until the end of the study (last subject finished the study drug administration) after the initial 3-year study drug administration.
Statistical analysis was performed with SAS (version 9.2; SAS Institute, Cary, NC). Data were expressed as means and SDs or as medians with IQRs when specified. Logarithmic transformation was used for variables that were not normally distributed. Within-group comparisons were performed with paired-sample Student t tests to evaluate the differences from baseline in each group. A Student t test (for data that were normally distributed) or a Mann-Whitney U test (not normally distributed) and an ANCOVA analysis with a model that included the baseline value of the dependent variable as a covariate were also used for comparison between groups. A χ2 test was used to analyze the differences in categorical variables. The primary end point of this trial was time to recurrent events. Multiple event analysis was performed with the use of the proportional means regression model (18). A multivariate proportional means regression model was used to control for the duration of diabetes, duration of CAD, age, sex, and smoking history at baseline. For all analyses, glipizide use was treated as the reference group. The intention-to-treat principle was used for end point analyses.
All reported P values are two sided, and P values <0.05 were considered to be statistically significant.
RESULTS
Recruitment ran from 1 June 2004 to 30 July 2007. Of 565 patients who were screened, a total of 304 patients were enrolled in the study, with follow-up ending in July 2010. Figure 1 showed the process of screening and randomization. The 31 patients in the glipizide group and 32 in the metformin group that terminated early with the study drug administration were still encouraged to continue the follow-up of primary outcomes. The median follow-up period was 5.0 years (range, 3.7–5.7 years). The mean age of the participants was 63.3 years (range, 36–80 years). Type 2 diabetes had been diagnosed for a mean of 5.6 years and CAD for a mean of 2.9 years before recruitment. The distribution and doses of glucose-lowering agents at baseline (Table 1 and Supplementary Table 1) and the other baseline characteristics of the participants in the glipizide and metformin groups were generally similar except for the 2-h plasma glucose levels. There was no significant differences between the two groups in the concomitant medication (Table 1).
Figure 1.

SPREAD-DIMCAD trial profile.
Table 1.
Characteristics of the patients at baseline and end of follow-up
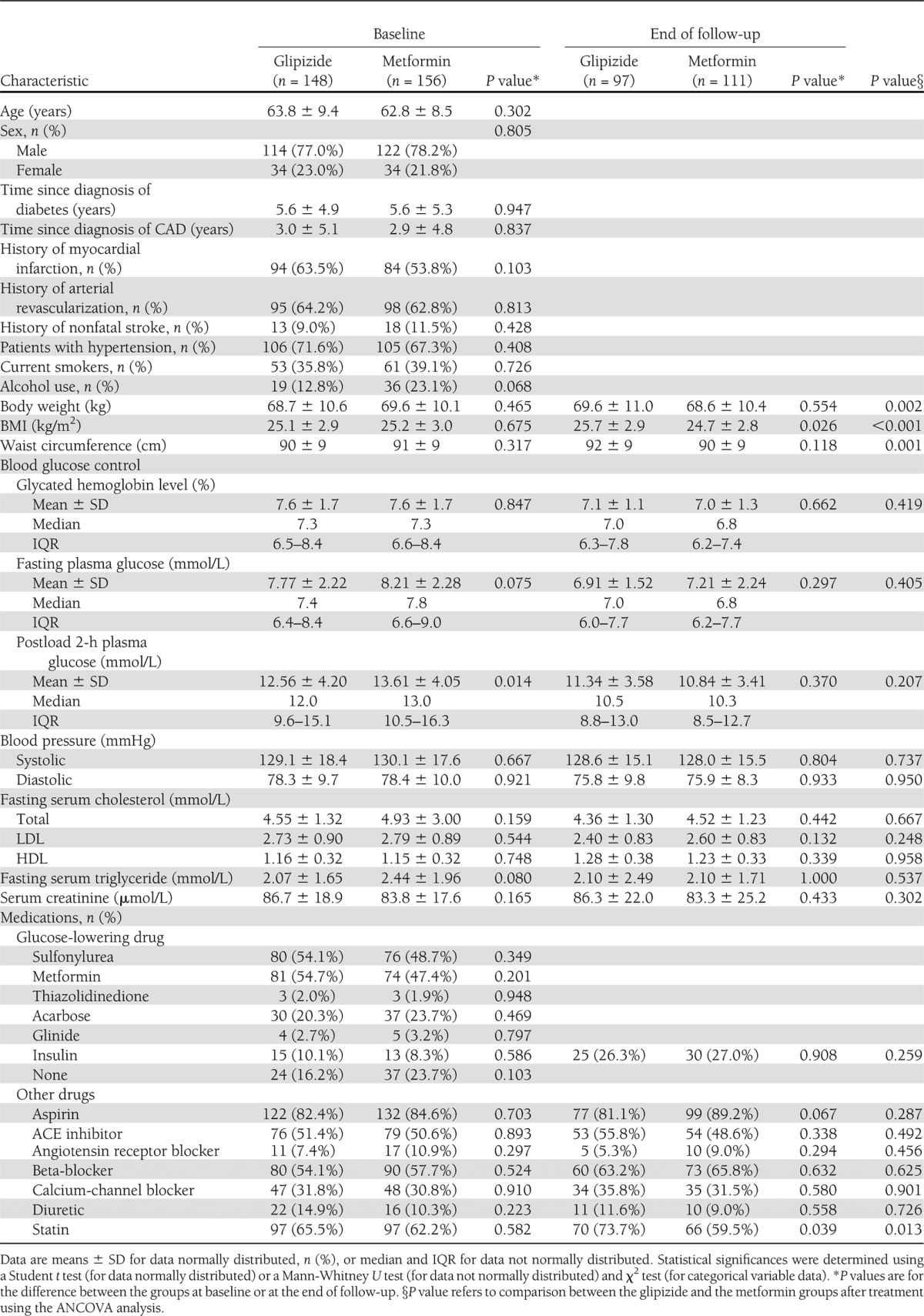
At the end of the 3-year study drug administration, the glycated hemoglobin levels were significantly improved in both groups, and no difference was found between the two groups (Table 1). The mean glycated hemoglobin values had fallen from 7.6% at baseline to 7.1% in the glipizide group and from 7.6 to 7.0% in the metformin group within 6 months after randomization and remained stable thereafter (Fig. 2A). Both groups showed a significant decrease in fasting and 2-h plasma glucose concentrations after treatment, and no difference was found between the two groups (Table 1 and Fig. 2B). At baseline, no difference was found in the BMI between the groups. However, after treatment, it was significantly lower in the metformin group than in the glipizide group (Table 1 and Fig. 2C). Similar differences were observed for body weight and waist circumference between these two groups (Table 1). Detailed changes and a comparison of the other clinical and biochemical characteristics of the two groups are shown in Table 1 and Fig. 2.
Figure 2.

Changes of major clinical and biochemical characteristics at baseline and during follow-up in different groups. HbA1c (A), fasting plasma glucose (B), BMI (C), triglycerides (D), total cholesterol (E), LDL cholesterol (F), HDL cholesterol (G), and estimated glomerular filtration rate (eGFR) (H). Data displayed as means ± SD. P value refers to comparison between the groups.
In order to reach the targeted glycated hemoglobin level, insulin was prescribed for 25 patients in the glipizide group and 30 patients in the metformin group, respectively (P = 0.259). The percentage of patients using insulin between the two groups at each visit was not significantly different (all P > 0.05). Furthermore, the dose used per person who was added with insulin in both groups increased but with no difference between the two groups (Table 1 and Supplementary Fig. 1). Drugs prescribed for other risk factors did not differ significantly at the end of the follow-up between the two groups, except for statins, which were used less in the metformin group compared with the glipizide group (P = 0.013) (Table 1).
A total of 103 composite primary end points occurred in 91 patients (52 [35.1%] in the glipizide group and 39 [25.0%] in the metformin group) (characteristics of these patients are shown in Supplementary Table 2) during the whole study period: 60 events in the glipizide group (14 deaths from any causes [including 11 deaths from cardiovascular events and 3 from sudden death; unfortunately autopsies were not performed to confirm the 3 patients’ precise causes of death], 6 nonfatal myocardial infarctions, 15 nonfatal strokes, and 25 arterial revascularizations), as compared with 43 events in the metformin group (7 deaths from any causes [all were deaths from cardiovascular events], 5 nonfatal myocardial infarctions, 10 nonfatal strokes, and 21 arterial revascularizations). As compared with the patients treated with glipizide, the HR for the composite cardiovascular events for metformin treatment was 0.54 (95% CI 0.30–0.90; P = 0.026) after adjustment for the duration of diabetes, duration of CAD, age, sex, and smoking history at baseline (Supplementary Table 3). No significant difference in the mortality rate between the two groups was found; P = 0.55.
During the study drug administration, the following secondary end points occurred: new or worsening heart failure developed in 10 (6.8%) patients in the glipizide group and 9 (5.8%) patients in the metformin group (adjusted HR 0.82 [95% CI 0.31–2.13]; P = 0.677); new critical cardiac arrhythmia occurred in 27 (18.2%) patients in the glipizide group and 30 (19.2%) patients in the metformin group (1.01 [0.60–1.72]; P = 0.958); new or worsening angina occurred in 71 (48%) patients in the glipizide group and 77 (49.4%) patients in the metformin group (1.07 [0.77–1.48]; P = 0.696); and 6 (4.1%) patients in the glipizide group and 1 (0.6%) patient in the metformin group developed peripheral vascular events (0.13 [0.02–1.08]; P = 0.059). Furthermore, the two groups did not differ significantly with respect to the number of patients who reported one or more hypoglycemic attacks during study drug administration (four in the glipizide group and three in the metformin group, P = 0.651; when excluding insulin users, three in glipizide group and zero in metformin group, P = 0.080).
CONCLUSIONS
SPREAD-DIMCAD was the first double-blind, randomized, controlled trial to compare the different effects of glipizide and metformin on the major cardiovascular events among patients with type 2 diabetes and CAD. After a median of 5.0 years of follow-up, treatment with metformin showed a significant reduction of the recurrence of composite cardiovascular events compared with glipizide, which indicated a protective effect of metformin on cardiovascular events in high-risk patients. Such a protective effect of metformin may also be present in a later stage of type 2 diabetes during insulin therapy (19).
Cardiovascular disease is the most common complication and the leading cause of mortality in patients with type 2 diabetes (20,21). Sulfonylureas and metformin have been the cornerstone of drug therapy for type 2 diabetes, either alone or in combination, for a quarter of a century (22). Experimental studies have shown different effects of these two kinds of antidiabetic drugs on cardiovascular disease besides their glucose-lowering effect (23–29). However, studies comparing these two classes of medications on cardiovascular risk in humans generated highly inconsistent results (7–14). Several reasons may account for the discrepancies among these studies. First, most of the previous studies are retrospective and observational in design. The patients included in different studies varied in the severity of diabetes and cardiovascular disorders as well as other characteristics, such as BMI and glucose levels, which might influence drug choice. Second, the uses of cardiovascular medications were not well controlled in some studies and might also contribute to the diverse associations with cardiovascular events. Moreover, few previous studies directly compared the effects of sulfonylureas and metformin on cardiovascular events, and the evidence from randomized clinical trials is sparse (12).
Our study was the first to compare the effects of sulfonylureas (glipizide) and metformin on the recurrence of major cardiovascular events in a prospective, randomized, double-blind, placebo-controlled trial. We found that, compared with glipizide, metformin showed a significant reduction in composite cardiovascular end points. Furthermore, since the primary outcome occurring within 1 year (nine patients in the glipizide group and eight patients in the metformin group) seems unlikely to have been caused by the effects of glipizide or metformin treatment, we performed a stratified analysis and only looked at the events after 1 year (HR 0.48 [95% CI 0.31–0.72]; P < 0.001), showing a better effect of metformin on the primary outcome. Several lines of evidence may explain the different effects of sulfonylureas and metformin on cardiovascular and all-cause mortality. Sulfonylureas can increase pancreatic β-cell insulin release by inhibiting the ATP-sensitive potassium (KATP) channel through binding to β-cell sulfonylurea receptor 1. While binding to sulfonylurea receptor 2 on cardiac myocytes, sulfonylureas inhibit cardiac KATP channels and reduce the protective effects of myocardial preconditioning (14,23–25). On the other hand, metformin reduces hepatic gluconeogenesis and increases insulin-stimulated glucose uptake in skeletal muscle and fat tissue (26). Recent evidence shows that metformin has antiatherogenic effects through the reduction of inflammatory markers, vascular adhesion molecules, and coagulation parameters, as well as the reduction of endothelial dysfunction (27–29). In addition, sulfonylureas are associated with weight gain, whereas metformin is associated with weight loss. Weight gain may negate the beneficial effects of sulfonylureas on glucose and increase mortality (30). Moreover, in our present study, statin use was significantly lower in the metformin group as compared with the glipizide group (59.5 vs. 73.7%; P = 0.013) at the end of the study. However, no significant difference was found in the lipid levels between the two groups after treatment, even with a tendency of slightly higher triglyceride levels during the first part (18 months) in the metformin group. These findings further strengthened the beneficial long-term effects of metformin, which might be associated with the antiatherosclerotic properties beyond glucose lowering (31,32).
The prospective, randomized, and controlled design of our study minimizes the potential bias and confounding. However, several limitations need to be considered. First, we used glipizide to represent the sulfonylureas because it is one of the most commonly used sulfonylureas in China. However, various sulfonylureas may differ in their effects on glucose control and cardiovascular risk in diabetic patients (14–16). Second, the secondary end points and adverse events were recorded only during the 3-year period of study drug administration, which might decrease the power of analysis. Third, we did not have a washout period in the current study due to safety concerns. Moreover, although the training of a lifestyle approach was implemented to reduce the risk for cardiovascular outcome in both groups and through all research centers according to the National Cholesterol Education Program Adult Treatment Panel III recommendation, we did not monitor and record the change of diet and exercise during the study. However, the double-blind, randomized study design and the intent-to-treat approach might minimize these limitations. Therefore, we would be cautious in interpreting the findings.
In summary, metformin therapy for 3 years substantially reduced major cardiovascular events in high-risk patients compared with glipizide, one of the commonly used sulfonylureas. Our results, taken in conjunction with recent research, indicated a potential benefit of metformin therapy on cardiovascular outcomes in diabetic patients.
Acknowledgments
This study was supported by grants from the 863 Project (2006 AA 02A409), the National Natural Science Foundation of China (30971077, 81170784), the Shanghai Shenkang Hospital Development Center (Shdc12007309), the Key Laboratory for Endocrine and Metabolic Diseases of Ministry of Chinese Public Health (1994DP131044), the National Key New Drug Creation and Manufacturing Program (2008ZX09312/019), the Shanghai Committee on Science and Technology (10dz1920802), the Program for Innovative Research Team of Shanghai Municipal Education Commission, the Sector Funds of Ministry of Health (No. 201002002), and the National Key New Drug Creation and Manufacturing Program of Ministry of Science and Technology (No. 2012ZX09303006-001). Both glipizide and metformin were provided by Xinyi Pharmaceutical Co. (Shanghai, China). All the funding sources of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript. No other potential conflicts of interest relevant to this article were reported.
J.H. and Y.Z. contributed to the implementation of the protocol and to writing the research design and methods, results, and conclusions. S.L. performed the statistical analysis and reviewed the manuscript. A.L., D.Zh., W.W., and W.S. contributed to the design and implementation of the protocol and to writing the conclusions. Q.S., Y.D., Z.Z., W.T., J.Z., L.C., D.Zo., D.W., H.L., C.L., G.W., and J.S. contributed to the implementation of the protocol and coordinated preparation of the conclusions. G.N. designed and implemented the protocol and was lead author. All authors approved the final manuscript. G.N. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
APPENDIX
SPREAD-DIMCAD CLINICAL SITES
The investigators and coordinators of this study are as follows: Guang Ning, MD, PHD; Jie Hong, PHD; Yifei Zhang, PHD; Weiqing Wang, MD, PHD; Minghui Gui, PHD; Ying Chen, MD; Zhenni Chi, MD; Qun Yan, MD; Ying Zhai, MD (Shanghai Clinical Center for Endocrine and Metabolic Diseases, Ruijin Hospital); Weifeng Shen, MD, PHD; Ankang Lv, MD; Ruiyan Zhang, MD, PHD (Department of Cardiology, Ruijin Hospital); Jialin Yang, PHD; Yu Zhang, MD; Xiaofang Fan, MD (Department of Endocrinology, Min Hang Center Hospital, Shanghai, China); Dadong Zhang, MD, PHD (Department of Cardiology, Min Hang Center Hospital); Qing Su, PHD; Yan Dong, PHD; Huili Xing, MD (Department of Endocrinology, Xinhua Hospital); Zhiguang Zhou, MD, PHD; Xing Li, MD; Weili Tang, PHD (Department of Endocrinology, The Second Xiangya Hospital of Central South University); Jiajun Zhao, MD, PHD; Qingbo Guan, MD; Xu Zhang, MD (Department of Endocrinology, Shandong Provincial Hospital); Lianqun Cui, MD, PHD; Liming Chen, MD (Department of Cardiology, Shandong Provincial Hospital); Dajin Zou, MD, PHD; Juan Li, MD; Yue Chen, PHD (Department of Endocrinology, Chang Hai Hospital); Dawang Wang, MD, PHD; Feixia Shen, MD, PHD; Wenjun Wu, MD (Department of Endocrinology, The First Affiliated Hospital of Wenzhou Medical College); Hong Li, MD, PHD; Jiaqiang Zhou, MD (Department of Endocrinology, Sir Run Run Shao Hospital); Chao Liu, MD, PHD; Tao Yang, MD, PHD; Bei Shen, MD (Department of Endocrinology, Jiangsu Province Hospital); Guoting Wu, MD, PHD; Shen Qu, MD, PHD; Chunjun Sheng, MD; Xiaoyun Cheng, MD (Department of Endocrinology, Shanghai Ten’s People’s Hospital of Tongji University); Jie Shen, MD, PHD; Yaoming Xue, MD, PHD; Min Wang, MD; Xiangrong Luo (Department of Endocrinology, Nanfang Hospital); Dalong Zhu, MD, PHD; Shanmei Shen, MD (Department of Endocrinology, Nanjin Drum Tower Hospital); Shenghua Yao, MD; Xiuhua Yu, MD (Department of Endocrinology, Putuo Hospital, Shanghai, China); Huigen Jin, MD; Jia Shi, MD (Department of Cardiology, Putuo Hospital); Bo Feng, MD, PHD; Yafang Ni, MD (Department of Endocrinology, East Hospital, Shanghai, China); Shengli Yan, MD; Yangang Wang, MD; and Xingji Gong, MD (Department of Endocrinology, The Affiliated Hospital of Qindao University Medical College, Shandong Province, China).
Footnotes
Clinical trial reg. no. NCT00513630, clinicaltrials.gov.
This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc12-0719/-/DC1.
A complete list of the investigators of SPREAD-DIMCAD can be found in the appendix.
References
- 1.Yang W, Lu J, Weng J, et al. China National Diabetes and Metabolic Disorders Study Group Prevalence of diabetes among men and women in China. N Engl J Med 2010;362:1090–1101 [DOI] [PubMed] [Google Scholar]
- 2.UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837–853 [PubMed] [Google Scholar]
- 3.Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008;359:1577–1589 [DOI] [PubMed] [Google Scholar]
- 4.Patel A, MacMahon S, Chalmers J, et al. ADVANCE Collaborative Group Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008;358:2560–2572 [DOI] [PubMed] [Google Scholar]
- 5.Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med 2003;348:383–393 [DOI] [PubMed] [Google Scholar]
- 6.Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008;358:580–591 [DOI] [PubMed] [Google Scholar]
- 7.Meinert CL, Knatterud GL, Prout TE, Klimt CR. A study of the effects of hypoglycemic agents on vascular complications in patients with adult-onset diabetes. II. Mortality results. Diabetes 1970;19(Suppl.):789–830 [PubMed] [Google Scholar]
- 8.The University Group Diabetes Program The University Group Diabetes Program. A study of the effects of hypoglycemic agents on vascular complications in patients with adult-onset diabetes. V. Evaluation of pheniformin therapy. Diabetes 1975;24(Suppl. 1):65–184 [PubMed] [Google Scholar]
- 9.UK Prospective Diabetes Study (UKPDS) Group Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998;352:854–865 [PubMed] [Google Scholar]
- 10.Johnson JA, Majumdar SR, Simpson SH, Toth EL. Decreased mortality associated with the use of metformin compared with sulfonylurea monotherapy in type 2 diabetes. Diabetes Care 2002;25:2244–2248 [DOI] [PubMed] [Google Scholar]
- 11.Evans JM, Ogston SA, Emslie-Smith A, Morris AD. Risk of mortality and adverse cardiovascular outcomes in type 2 diabetes: a comparison of patients treated with sulfonylureas and metformin. Diabetologia 2006;49:930–936 [DOI] [PubMed] [Google Scholar]
- 12.Kahn SE, Haffner SM, Heise MA, et al. ADOPT Study Group Glycemic durability of rosiglitazone, metformin, or glyburide monotherapy. N Engl J Med 2006;355:2427–2443 [DOI] [PubMed] [Google Scholar]
- 13.Jørgensen CH, Gislason GH, Andersson C, et al. Effects of oral glucose-lowering drugs on long term outcomes in patients with diabetes mellitus following myocardial infarction not treated with emergent percutaneous coronary intervention—a retrospective nationwide cohort study. Cardiovasc Diabetol 2010;9:54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schramm TK, Gislason GH, Vaag A, et al. Mortality and cardiovascular risk associated with different insulin secretagogues compared with metformin in type 2 diabetes, with or without a previous myocardial infarction: a nationwide study. Eur Heart J 2011;32:1900–1908 [DOI] [PubMed] [Google Scholar]
- 15.Fiévet C, Nuttens MC, Ducimetière P, Fruchart JC, Bertrand M, Salomez JL. Relation of arteriographically defined coronary artery disease to serum lipoprotein particles mapped with monoclonal antibodies. Circulation 1991;84:153–159 [DOI] [PubMed] [Google Scholar]
- 16.Gabir MM, Hanson RL, Dabelea D, et al. The 1997 American Diabetes Association and 1999 World Health Organization criteria for hyperglycemia in the diagnosis and prediction of diabetes. Diabetes Care 2000;23:1108–1112 [DOI] [PubMed] [Google Scholar]
- 17.Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486–2497 [DOI] [PubMed] [Google Scholar]
- 18.Lin DY, Wei LJ, Yang I, Ying Z. Semiparametric regression for the mean and rate functions of recurrent events. J R Stat Soc Series B Stat Methodol 2000;62:711–730 [Google Scholar]
- 19.Kooy A, de Jager J, Lehert P, et al. Long-term effects of metformin on metabolism and microvascular and macrovascular disease in patients with type 2 diabetes mellitus. Arch Intern Med 2009;169:616–625 [DOI] [PubMed] [Google Scholar]
- 20.Gu K, Cowie CC, Harris MI. Mortality in adults with and without diabetes in a national cohort of the U.S. population, 1971-1993. Diabetes Care 1998;21:1138–1145 [DOI] [PubMed] [Google Scholar]
- 21.Bertoni AG, Krop JS, Anderson GF, Brancati FL. Diabetes-related morbidity and mortality in a national sample of U.S. elders. Diabetes Care 2002;25:471–475 [DOI] [PubMed] [Google Scholar]
- 22.DeFronzo RA. Pharmacologic therapy for type 2 diabetes mellitus. Ann Intern Med 1999;131:281–303 [DOI] [PubMed] [Google Scholar]
- 23.O’Rourke B. Evidence for mitochondrial K+ channels and their role in cardioprotection. Circ Res 2004;94:420–432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yellon DM, Downey JM. Preconditioning the myocardium: from cellular physiology to clinical cardiology. Physiol Rev 2003;83:1113–1151 [DOI] [PubMed] [Google Scholar]
- 25.Riveline JP, Danchin N, Ledru F, Varroud-Vial M, Charpentier G. Sulfonylureas and cardiovascular effects: from experimental data to clinical use. Available data in humans and clinical applications. Diabetes Metab 2003;29:207–222 [DOI] [PubMed] [Google Scholar]
- 26.Kirpichnikov D, McFarlane SI, Sowers JR. Metformin: an update. Ann Intern Med 2002;137:25–33 [DOI] [PubMed] [Google Scholar]
- 27.Davis BJ, Xie Z, Viollet B, Zou MH. Activation of the AMP-activated kinase by antidiabetes drug metformin stimulates nitric oxide synthesis in vivo by promoting the association of heat shock protein 90 and endothelial nitric oxide synthase. Diabetes 2006;55:496–505 [DOI] [PubMed] [Google Scholar]
- 28.Mather KJ, Verma S, Anderson TJ. Improved endothelial function with metformin in type 2 diabetes mellitus. J Am Coll Cardiol 2001;37:1344–1350 [DOI] [PubMed] [Google Scholar]
- 29.De Jager J, Kooy A, Lehert P, et al. Effects of short-term treatment with metformin on markers of endothelial function and inflammatory activity in type 2 diabetes mellitus: a randomized, placebo-controlled trial. J Intern Med 2005;257:100–109 [DOI] [PubMed] [Google Scholar]
- 30.Rao AD, Kuhadiya N, Reynolds K, Fonseca VA. Is the combination of sulfonylureas and metformin associated with an increased risk of cardiovascular disease or all-cause mortality? A meta-analysis of observational studies. Diabetes Care 2008;31:1672–1678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fidan E, Onder Ersoz H, Yilmaz M, et al. The effects of rosiglitazone and metformin on inflammation and endothelial dysfunction in patients with type 2 diabetes mellitus. Acta Diabetol 2011;48:297–302 [DOI] [PubMed] [Google Scholar]
- 32.Papanas N, Maltezos E. Oral antidiabetic agents: anti-atherosclerotic properties beyond glucose lowering? Curr Pharm Des 2009;15:3179–3192 [DOI] [PubMed] [Google Scholar]