

Abstract
Within health and health care, medical informatics and its subspecialties of biomedical, clinical, and public health informatics have emerged as a new discipline with increasing demands for its own work force. Knowledge and skills in medical informatics are widely acknowledged as crucial to future success in patient care, research relating to biomedicine, clinical care, and public health, as well as health policy design. The maturity of the domain and the demand on expertise necessitate standardized training and certification of professionals. The American Medical Informatics Association (AMIA) embarked on a major effort to create professional level education and certification for physicians of various professions and specialties in informatics. This article focuses on the AMIA effort in the professional structure of medical specialization, e.g., the American Board of Medical Specialties (ABMS) and the related Accreditation Council for Graduate Medical Education (ACGME). This report summarizes the current progress to create a recognized sub-certificate of competence in Clinical Informatics and discusses likely near term (three to five year) implications on training, certification, and work force with an emphasis on clinical applied informatics.
Keywords: Education, Professional training, Clinical informatics, Training and education requirements, General healthcare providers, Informatics specialists, Strategies for health IT training, Continuing professional development and continuing education
Clinical Informatics: A new specialty
New medical specialties and subspecialties emerge over time like Anesthesia in the 19th century or Emergency Medicine in the 20th century [1]. Medical Informatics and its subspecialties of Biomedical, Clinical, and Public Health informatics have emerged as a new discipline within health and health care in the 21st century - after a gestation period of roughly sixty years [1]. The formative period coincides with the development of computer science – information and communications technology – and the emergence of electronic health records as essential technology for health care. It also coincides with the development of training programs in biomedical, clinical, and public health informatics. The American Medical Informatics Association (AMIA) is the professional home for biomedical and health informaticians. In response to the needs of a growing work force in Clinical Informatics, AMIA developed a professional code of ethics as well as a front ranking scientific research journal, Journal of the American Medical Informatics Association (JAMIA). In 2006, AMIA was elected to full membership in the Council of Medical Specialty Societies [1], in recognition of its importance as an emerging specialty area in healthcare.
Clinical Informatics is not only one of the first new subspecialties that have emerged in this century, in the authors’ opinion; it is fundamentally different from all prior subspecialties. Even though the knowledge and skills of a medical informatician are unique, the need for informatics as an essential component of daily medical care and research cuts across all primary specialties [4]. For example, clinical specialties like surgery, pediatrics, and internal medicine rely on informaticians and to a lesser extent information and communication technologists to implement, manage, and advance electronic health record systems, aid in designing clinical decision support and manage research data. Imaging and laboratory specialties have long had a need for experts in clinical information systems. Expertise in Clinical Informatics has been recognized as crucial for the operation of clinical institutions as demonstrated by the large number of newly created Chief Medical Informatics Officer (CMIO) [5] and Chief Nursing Informatics Officer (CNIO) [6] positions. Because Clinical Informatics is of growing importance and value to all existing medical specialties, at this point it is possible if not probable that it will be incorporated as a subspecialty certification option open to all existing primary specialties.
Workforce Demands
In 2004, then President George W. Bush called for the widespread use of electronic health records (EHRs) by 2014 [7]. This challenge generated an important goal for those in Clinical Informatics but it quickly became apparent that the US health care system was sorely lacking the informatics savvy workforce sufficient in number and knowledge to accomplish this goal. These work force demands dictated that it was time for Clinical Informatics to evolve from an avocational or part time activity of self-identified informaticians to a fully professional career track with training, standards, codes of ethics and certification. Clinical Informatics needed to shed its status as a ‘club’ sport and become a fully recognized profession within the house of medicine.
Knowledge and skills in Clinical Informatics are widely acknowledged as crucial to future success in patient care, research related to biomedicine, and public health, as well as to health policy design and implementation. It is apparent that success in realizing electronic health record systems depends more on knowledge and expertise like needs assessment, organizational leadership, and change management skills than on information technology itself. The core expertise of a medical informatician is thus more strategic than tactical in nature. The training requirements proposed by AMIA incorporate these competencies as a central element of the training for clinical informaticians.
Certification Process
AMIA is the professional home to clinical informaticians representing a variety of health professions including medicine. Clinical Informatics professionals are not the first to develop a professional model: The nursing profession created a certified nurse informatician [8] and as of November 2000, 381 nurses had been certified as nurse informaticians by the American Nurses Credentialing Center [9]. Several years ago, pathologists within AMIA started an unsuccessful effort to create formal informatics specialty training and certification.
In 2005, the membership of AMIA concluded at a town hall meeting that AMIA should move forward with creating a formal certification program for health professionals in Clinical Informatics, beginning with physicians. The AMIA Board then formally approved a strategic plan to pursue a Clinical Informatics subspecialty within the structure of the American Board of Medical Specialties. In 2010, AMIA will embark upon an effort to create an Advanced Inter-Professional Informatics Certification process to supplement the existing nurse certification and support professional education for practicing dentists, pharmacists, as well as physicians and others who do not wish to seek certification through ABMS. This paper will focus solely on establishing physician sub-certification in Clinical Informatics.
Requirements to establish a subspecialty in Clinical Informatics
While options other than the America Board of Medical Specialties (ABMS) for physician certification and the Accreditation Council for Graduate Medical Education (ACGME) for training program accreditation exist, the importance and leadership of these two organizations [10] are so solidly established that essentially, they oversee the approval of new specialties in medicine. The ABMS approves the content of a medical specialty and through their member boards oversees the creation of a competency examination and the certification of physicians, who meet their training standards. . The ACGME offers accreditation to training programs that meet the subspecialty’s formal training criteria. . Before the ACGME would establish the program accreditation process, a new specialty would traditionally first receive approval from the ABMS. AMIA officers have also communicated with ACGME officials in the past so they are aware that work is moving forward in a timely manner.
The establishment of Clinical Informatics as a sub-certification requires that several conditions be met. First, one must convince physician peers within the ABMS governance structure that the emerging discipline is substantive and essential to the health care needs of patients. In short, the specialty must pass the test of being vital to comprehensive care (e.g., the vital importance of the EHR for the ‘Medical Home’ [11]) for the sick and injured as well as being important to preventing illness and maintaining health status. Markers to determine the essential nature of a specialty include the availability of formal educational programs of sufficient rigor and length and the definition of knowledge and skills relevant and critical to working as a professional in the discipline. The presence of one or more scholarly publications in the field that offer peer reviewed articles is another marker. The existence of an organizational home for such professionals like AMIA is a prerequisite, as is a professional code of ethics.
Other criteria include documentation of regular well organized meetings, with a national scale and scope that offer relevant high quality continuing educational programs. It is necessary that the subspecialty demonstrate the existence of a ‘population’ of practicing medical professionals in the discipline. Both, the American College of Medical Informatics (ACMI – a college of elected fellows who have made significant and sustained contributions to the field of medical informatics) and an active well established Clinical Informatics working group within AMIA, are indicators of stability and permanence.
Further requirements include demonstration of well structured collection of the knowledge and skills that comprise competence in the field and well formulated training requirements. While AMIA as an organization fulfilled several other criteria simply by serving as the professional home for biomedical and health informaticians, and by providing continuing medical education and means to disseminate scholarly activity; the requirements for formal descriptions of the core content and training requirements specifically for Clinical Informatics had not been met until recently. The generation of core content and training requirements involved substantial AMIA efforts supported though funding from the Robert Wood Johnson Foundation (RWJ) under the leadership of RWJ’s Vice President John R. Lumpkin, MD [12].
Two groups were created and empowered by the AMIA Board of Directors to create the core content [3] and training requirements [13] documents to frame the approach to the ABMS. Participants in the groups included clinical informaticians from medicine, nursing, dentistry, and pharmacy in the belief that Clinical Informatics needs to be focused primarily on informatics rather than medicine per se. Close attention was given to assuring that the documentation met the ABMS requirements. ►Table 1 shows the committee membership for the core content [13] and training requirements [12] task forces.
Table 1.
Committee membership for the development of core content and training requirements
| Committee | Core Content | Training Requirements |
|---|---|---|
| Chair | Reed M. Gardner | Charles Safran |
| Vice Chair | J. Marc Overhage | M. Michael Shabot |
| Members | Joan S. Ash James J. Cimino H. Dominic Covvey Don E. Detmer John H. Holmes Nancy C. Nelson Charles Safran Richard N. Shiffman Heiko Spallek |
Christopher Cimino Don E. Detmer Reed M. Gardner Carole A. Gassert William Hersh John H. Holmes Stasia Kahn Christoph U. Lehmann Gretchen Purcell Jackson John R. Lumpkin |
| Staff | Benson S. Munger (Consultant) Jeffrey J. Williamson Elaine B. Steen |
|
Currently there are twenty-four specialty boards and 121 sub-specialties. There have been no new primary specialties approved by the ABMS for many years. Given the evolution of medicine, the development and approval of another primary specialty is unlikely in the near term. Further, the unique nature of Clinical Informatics – potentially transcending all existing medical specialties – made it an ideal candidate for a subspecialty available to diplomates of all primary specialties. Subspecialties must be governed and administered by at least one primary specialty board, but through cross-board agreements, certification may be available to members of other specialties who then receive a sub-board certificate in their parent specialty or the sponsoring specialty. Clinical Informatics clearly is of potential interest to all specialty boards as a new subspecialty.
Once the core content [13] and training documents [13] were created and published, attention turned to identifying a specialty board recognized by the ABMS that was willing to serve as the ‘parent’ for the Clinical Informatics subspecialty through its certification authority. In the summer of 2009, the American Board of Preventive Medicine (ABPM) formally agreed to become the home for the Clinical Informatics certification for physicians. Further, ABPM designated AMIA as the organization of record for issues related to this emerging specialty. Preventive Medicine is a primary specialty that takes a broad systems view of its discipline and focuses both on individual patients and on populations. This philosophy corresponds well with AMIA’s commitment to systems thinking, using informatics to support both individual and population health, and its aim to be the professional home for both clinical and public health informaticians.
Clinical Informatics subspecialty: A Prediction for the early years.
This section describes the process to move from submission of the appropriate documentation from ABPM to the ABMS for formal review and action. The ABPM has formally notified ABMS that the documents will be forthcoming in early 2010 for initial review and subsequent formal action by 2011 or possibly 2012 if more time is essential to meet all the ABMS requirements. While there is no guarantee of success until the vote by ABMS, nearly all boards have expressed support for Clinical Informatics and ABPM will offer it to all of the 24 boards. When and if it is approved, Clinical Informatics will become a sub-board of the ABPM. ABPM will provide resources and set basic requirements, e.g., minimum standards for a formal certification examination and a process for Maintenance Of Certification (MOC)”.
Establishing a new Subspecialty
Currently, AMIA is collaborating with the ABPM in the preparation of the formal application. The application must include extensive information about the specialty, proposed requirements for initial certification and maintenance of certification. Many details related to the way this subspecialty will conduct its work have to be discussed and decided, for example wording of the certificate, expiration period of the certificate, managing of ‘practice’ tracks, etc.
The proposed process for the initial certification and the MOC will be examined by ABMS in its internal review. This will first involve the Committee on Certification, Subcertification, and Maintenance of Certification (COCERT), prior to review and approval from the ABMS Board of Directors and the ABMS Assembly. Gaining approval from COCERT is a key hurdle.
Once approved, a sub-board examination committee will be created consisting of 9 to 11 experts. AMIA and perhaps other organizations will nominate members for the examination committee. These experts will be trained by ABPM in test development and will create a set of examination specifications and a pool of candidate ‘items’ (examination questions). A standard setting exercise is involved to test ‘items’ as well as to determine the pass point on the initial examination. A pool of 300 questions must be created and many candidate questions will in all likelihood fail the requirements to be part of the examination. The process for creating and maintaining examinations will involve the annual committee meeting to review new items contributed to the pool, removing outdated items from the pool, and selecting items for the forthcoming examination. After each examination cycle, the committee meets to review experiences with the examination itself as well as any issues relating to its administration.
Policies based on those adopted by the ABPM must be developed by the sub-board examination committee for reviewing and scoring the examinations. Applications for those wishing to sit for the examination need to be developed and reviewed prior to the first examination. This entire process must be repeated every five years to assure currency of the examination. The initial process involves some additional steps since Clinical Informatics is a new subspecialty.
ABPM will have administrative and legal responsibility for the certification examination and it will collect the fees and pay sub-board expenses. ABPM is responsible to ABMS for compliance of its Clinical Informatics sub-board and maintains oversight. Currently unresolved is whether or not AMIA will have a liaison seat on the ABPM Board or be given a formal seat.
Individual Certification Process
Like other sub-specialties, eligibility of physicians to sit for the certification examination in Clinical Informatics will require successful completion of a Clinical Informatics fellowship. Once ABMS approval is obtained, fellowships must be established and must meet the standards for ACGME. Existing and new fellowship programs must become accredited through the Accreditation Council for Graduate Medical Education, which will designate a residency review committee (RRC) to peer-review fellowship programs. All formal training programs must have a sponsoring institution. Most likely, this will be a medical school. Fellowship programs that have more than one training site must have a formal agreement (program letter of agreement) with all training site(s) that must be renewed at least every five years [12].
Initially there will be two tracks to become eligible for the board examination. Successful completion of an accredited fellowship program will be available indefinitely and is the gold standard. Initially there will likely be an option of a ‘practice’ track. A practice track for a new subspecialty typically is limited to five years (starting with the initial examination); a minimum set of practice requirements are identified. Typically, the minimum practice requirements do not require full time practice but demonstration of concentrated practice of some duration in the field is required. ►Figure 1 shows the complete process for both tracks from eligibility to recertification. Usually, it takes 18-24 months from the initiation of a new subspecialty board until the examination becomes available.
Fig. 1.
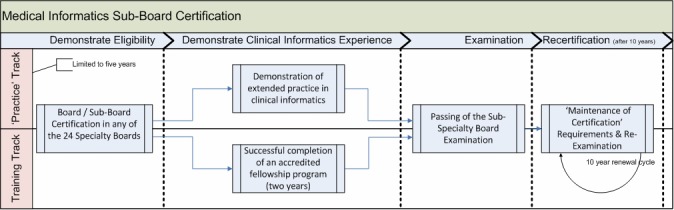
Medical informatics sub-board certification
Maintenance of Certification
After the first examination, a MOC process must be developed. Due to the nature of Clinical Informatics and the anticipation of widespread EHRs use by then, some novel evaluation approaches might be possible. AMIA will develop continuing education opportunities to meet standards for maintenance of competency. AMIA expects that the presence of the Academic Forum will generate a number of distributed programs in the early years. The standard cycle for board re-certification is ten years, when candidates have to demonstrate that they met the requirements for re-certification and have to sit again for a proctored examination.
AMIA will be a major provider for credits to meet the Part II (Lifelong learning & self assessment) MOC requirements and develop programs to meet the ABPM MOC Part IV (Practice Performance Assessment) program.
Subspecialty Board Timelines (Caveat emptor)
The following timelines are estimates. Final approval from ABMS is sought in the fall of 2011 with sub-board requirements and examination development complete by the summer of 2012 (no later than 2013). Potentially, the first certification examinations in Clinical Informatics would be administrated in the Fall of 2012 and initial certificates issues would be issued in January 2013. If all goes as hoped, the ABPM will decide in the spring of 2012 whether or not the first examination can be offered in the fall of 2012.
Conclusion
AMIA, as the specialty home for Clinical Informatics, has initiated the genesis of a Subspecialty Board. AMIA members have supported this effort enthusiastically. Medical Informaticians will be able to become Subspecialty Board Certified as early as 2012.
Acknowledgement
The authors wish to acknowledge the ongoing efforts of Elaine B. Steen, MS, Editorial and Research Consultant; Jeffrey J. Williamson, Vice President of Education and Academic Affairs, AMIA; and, Edward Shortliffe, MD, PhD, President and CEO of AMIA.
References
- 1.American Board of Medical Specialties ABMS Extended History: Approval of New Member Boards. Available online athttp://www.abms.org/About_ABMS/ABMS_History/Extended_History/Approving_New_Boards.aspx[last accessed 11/25/2009]
- 2.Shortliffe EH, Cimino JJ. (eds) Biomedical Informatics: Computer Applications in Health Care and Biomedicine. New York: Springer-Verlag, 2006 [Google Scholar]
- 3.Council of Medical Specialty Societies Member Societies. Available online athttp://www.cmss.org/index.cfm?p=display&detail=Member%20Societies[last accessed 11/25/2009]
- 4.Detmer DE, Lumpkin JR, Williamson JJ. Defining the medical subspecialty of Clinical Informatics. J Am Med Inform Assoc. 2009Mar-Apr;16(2):167-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leviss J, Kremsdorf R, Mohaideen MF. The CMIO--a new leader for health systems. J Am Med Inform Assoc. 2006Sep-Oct;13(5):573-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Eriksen AB. Informatics: How nurses will take record keeping into the future. Available online athttp://www.modernmedicine.com/modernmedicine/Modern+Medicine+Now/Informatics-How-nurses-will-take-record-keeping-in/ArticleStandard/Article/detail/608947[last accessed 1/17/2010] [Google Scholar]
- 7.Cronin K, Department of Health and Human Services. The Office of the National Coordinator of Health Information Technology, 2004. Available online athttps://www.clinicalresearchnetworks.org/documents%5CJune%201%5CKeynote%20Speech.pdf[last accessed 11/25/2009] [Google Scholar]
- 8.American Nurses Credentialing Center Informatics Nursing. Available online athttp://www.nursecredentialing.org/NurseSpecialties/Informatics.aspx[last accessed 11/25/2009]
- 9.Terreline (Shellie) Sims American Nurses Credentialing Center, Silver Spring, MD.Personal communication; 11/25/2009 [Google Scholar]
- 10.American Board of Medical Specialties. http://www.abms.org/ Available online at. [last accessed 11/25/2009]
- 11.Carney PA, Eiff MP, Saultz JW, Douglass AB, Tillotson CJ, Crane SD, Jones SM, Green LA. Aspects of the Patient-centered Medical Home currently in place: initial findings from preparing the personal physician for practice. Fam Med. 2009Oct;41(9):632-9 [PubMed] [Google Scholar]
- 12.Safran C, Shabot MM, Munger BS, Holmes JH, Steen EB, Lumpkin JR, Detmer DE; AMIA Board of Directors. Program requirements for fellowship education in the subspecialty of Clinical Informatics. J Am Med Inform Assoc. 2009Mar-Apr;16(2):158-66 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gardner RM, Overhage JM, Steen EB, Munger BS, Holmes JH, Williamson JJ, Detmer DE; AMIA Board of Directors. Core content for the subspecialty of Clinical Informatics. J Am Med Inform Assoc. 2009Mar-Apr;16(2):153-7 [DOI] [PMC free article] [PubMed] [Google Scholar]