

Abstract
Objective
Nonverbal and verbal communication elements enhance and reinforce the consent form in the informed consent process and need to be transferred appropriately to multimedia formats using interaction design when re-designing the process.
Methods
Observational, question asking behavior, and content analyses were used to analyze nonverbal and verbal elements of an informed consent process.
Results
A variety of gestures, interruptions, and communication styles were observed.
Conclusion
In converting a verbal conversation about a textual document to multimedia formats, all aspects of the original process including verbal and nonverbal variation should be one part of an interaction community-centered design approach.
Keywords: Informed consent, gestures, user-computer interface, multimedia
1. Introduction
An informed consent process usually contains a standard IRB approved textual document, which is typically described to a participant by a research coordinator using variable verbal language and body gestures. Previous studies focused on improving the textual document, or changing the presentation medium [1–12], but little research has been conducted to determine the variability inherent in the verbal consent process. Little research has focused specifically on how written consent forms are integrated into a verbal dialogue between a potential research participant and the person administering the consent.
Marshfield Clinic’s Personalized Medicine Research Project (PMRP) conducts genetic studies in which they collect blood, and plasma samples, and requires written informed consent for participation. A recent study of PMRP participants shows that although the participants understood the overall goals of the project, many were unsure or incorrect about key factors of the study [13]. Results of this study suggest that incorrect responses were due to a lack of comprehension, rather than a loss of memory of specific details, since the percentage of correct responses was not related to the time since consenting to the PMRP project [13, 14].
Marshfield Clinic identified a need to improve their methods of informed consent to ensure that participants are fully informed when they consent to be in the study and that they retain that information. This study is one phase of a larger project to develop a multi-media informed consent process that is acceptable to potential research participants and improves the retention of information. The purpose of this phase of the study was to determine the relationship between the nonverbal and verbal elements of the informed consent process for PMRP prior to determining how to transform the content and process to a multi-media format. This study fills a gap in knowledge by formally analyzing the current consent process in a novel way using human factors methods that include observational, question asking behaviors and content analyses. The application of this research is a proof-of-concept guide to the incorporation of both nonverbal and verbal communication elements in a multi-media informed consent application.
2. Background
The researchers’ role in the informed consent process is to inform participants as to the true nature, aims, and intent of the study by describing what to expect if they agree to participate, and through full disclosure of the purpose, anticipated benefits, risks, alternatives, and expected outcomes of the study; to answer any questions the participant may have; and to respect the participants consent or dissent [7–10]. Based on previous research, potential study subjects are more likely to actually read the consent form if it is given to them to review at their leisure; thus, it follows that multimedia education materials, which are self-paced, are also more likely to be reviewed [15].
Multimedia education consists of a variety of combinations of text, audio, video, interactive questionnaires, visualizations, graphics, or even immersion into a virtual 3D environment [7]. Agre and Rapkin measured comprehension of consent information among 204 participants randomized to one of four consent processes: standard, video, computer-assisted instruction, or booklet, and reported that comprehension was unchanged across all groups on the post test regardless of the delivery method, suggesting that the media used to present the informed consent process does not matter [1, 12].
A multimedia tool has the potential to standardize the quality of informed consent; however, previous studies have failed to create a generalized solution [7]. These studies fail to assess either the competence of the patient, the appropriateness of the educational level of the material, or the effectiveness of the electronic consent process [7]. Although a computer-based informed consent process adds a level of standardization, it must be tailored to the individual participants’ learning style as one-size-fits-all interventions may not be universally generalize-able [16]. Agre and Rapkin argue that a successful consent process must, at a minimum, include both a written and a verbal component, perhaps even using the technique of asking the participant to repeat what he or she understands, and the participant should interact one on one with someone knowledgeable about the study at some point in time [1, 12]. A counterintuitive result identified in Agre and Rapkin’s study is that participant comprehension of an informed consent form increases when participants had a higher level of formal education, or when the study protocol was very complex (i.e. the study had more risks, side effects, or procedures to explain), requiring a simplified, longer explanation [1, 12]. However, the transferability of verbal and nonverbal communication elements to multimedia technologies is impeded by the tacit nature of these elements.
3. Methods
Data was obtained by conducting “mock” informed consent sessions with a convenience sample of six Marshfield Clinic employees and six Biomedical Informatics Research Centers’ usability community volunteers. Since the PRMP project is a population-based biobank that recruits from the community, including Marshfield Clinic employees, these subjects were typical of PRMP subjects. The sample size is considered adequate for a proof-of-concept paper. The nonverbal and verbal elements were captured by videotaping and digitally recording twelve mock consent sessions.
All 12 “mock” sessions were conducted by the same research coordinator, who was also responsible for administering actual PRMP consents and was well acquainted with the process, with subjects as though they were enrolling in a study. Subjects were consented to the videotaping of the study of the consent process, and were aware that the purpose of the research was to study the consent process itself rather than to enroll them into the PMRP project. Certified medical transcriptionists at the Marshfield Clinic professionally transcribed audio from the twelve sessions.
3.1. Analysis
The nonverbal elements of the informed consent process were analyzed using an observational analysis [17], where the investigator observed the videos and documented the nonverbal behaviors of the research coordinator. Eleven videos were analyzed for gesture, eye gaze, and body posture for nonverbal cues that the research coordinator used within the consent process in communication with the research participant. For the observational analysis, one session was excluded due to technical issues that resulted in the loss of the video. Observational analysis was used to generate a list of gestures with classifications similar to Bickmore et al. and Whishaw et al [18, 19]. Analysis of eye gaze and body posture is used to show how the research coordinator uses the written consent form as a form of external scaffolding, where one places knowledge in the environment that the research coordinator relies on to aid their thoughts in order to remind the coordinator to cover elements of the consent form within their verbal explanation [20]. Gestures are also used as perceptual-motor information scaffolding for perceptual-motor information, where their hand gestures reflect properties of the particular objects and the actions they have previously used to remember and convey the concepts in a verbal consent [21]. Analysis of gestures is used to describe and make inferences about the characteristics of communication to analyze style and techniques of persuasion.
The verbal elements of the informed consent process were analyzed for question asking behaviors initiated by the participant that created dialogue using a content analysis [22, 23]. Question asking behavior analysis highlights the important function of the research coordinator in answering questions from the research participant and shows the usefulness of supplementary materials in a multimedia version as a means of tailoring to the needs of a particular participant. The question asking behavior analysis uses frequency of questions asked by the participants as a means to analyze the flow of information. The written consent form consists of 20 specific sections or content areas.
A content analysis was used to describe trends in communication content, to analyze techniques in persuasion, and to determine the balance of personalized narrative for paraphrasing within the current verbal consent process [23]. The content analysis is a qualitative method used to analyze the content of communication and is validated using inter-rater reliability. A content analysis was conducted on four transcripts to determine how the verbal process compliments and extends the written consent form in terms of content and style of delivery. One transcript was analyzed by a second coder to establish interrater reliability using Cohen’s Kappa. In this study, the focus was on the words used by the research coordinator that could be a paraphrasing of information in the consent form or a personalized narrative to connect to the individual participant’s situation or even a joke to elicit participant response.
4. Results
The data for non-verbal observational analysis included 1,903 observations that were classified, and analyzed from the 11 videotaped sessions. The types of observations that were gathered within the observational analysis include:
-
1.
General hand gestures refers to any waving of the hand, conducting, paddling, arcing, or tapping in air gestures that are not specific.
-
2.
Specific conversational hand gestures are actions made by the research coordinator that communicate more than a wave of the hand to the participant, which may add value to the consent process by representing a concept or by re-assuring the participant.
-
3.
Highlighting gestures are where the research coordinator points to, traces, or taps a sentence or word.
-
4.
Resting gestures are where the research coordinator’s hands are folded or placed face down on the table or along the corners at the top of the consent document, which add value to the consent process by removing unnecessary movement and by inviting the participant to ask questions of the research coordinator.
-
5.
Repositioning gestures are where the research coordinator does something with the paper document, by either straightening the consent document, or turning to a new page, which are necessary to help the participant follow along with the paper consent process.
-
6.
Other specific hand gestures are actions where the research coordinator, for example, is: touching their chest, counting, ‘what-ever’, sliding hands across the table, simulating a needle prick in the arm vein, creates a circle, creates a crossing out or stopping gesture to cancel something out, or presents something as ‘door number 1 vs. door number 2’.
-
7.
Head gestures are where the research coordinator is nodding or shaking their own head within the conversation and may be used to reassure the participant.
-
8.
Eye gaze refers to when the research coordinator gazes down at the written consent document, or into the participant’s eyes, which is important for communicating ideas or focusing attention elsewhere.
-
9.
Body posture refers to where the research coordinator leans forward towards the participant, or leans back against the chair.
-
10.
Transition patterns are combinations of gestures that form a common pattern that occur in the transition at the beginning of a new section where the research coordinator leans forward gazing down at the page and either points to or traces the important text.
Of the 1,903 observations presented in ►Figure 1,77% were hand gestures (29% general hand waving, 13% specific hand waving, 20% highlighting, 10% resting, and 5% repositioning), 12% were head gestures, 5% were body posture shifts, and 5% were eye gazes.
Fig. 1.
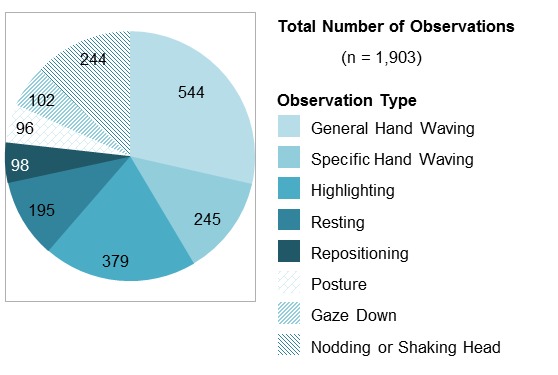
Observations by type
For the verbal analysis of the mock informed consent, there was a total of 61 questions asked by participants over the 12 sessions, corresponding to 14 of the 20 sections on the consent form that were analyzed using question asking behavior analysis. ►Figure 2 presents the frequency of questions organized by section of the consent form where the participant interrupted the research coordinator to ask a question or to get further clarification on an idea. Content in ►Figure 2 is presented in the same order as the 20 sections of the consent form, excluding the final section on “statement of consent” (i.e., where the participant is asked to sign the consent form).
Fig. 2.
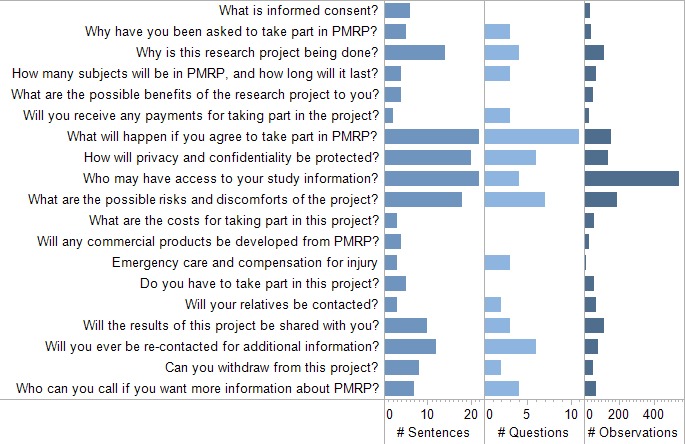
Number of observations, questions, and sentences by section of the personalized medicine research project (PMRP) consent form ordered temporally
The informed consent sections with the most questions in decreasing order were: what will happen if you agree to take part in PMRP, how will privacy and confidentiality be protected, who may have access to your study information, what are the possible risks and discomforts of the project and, will you ever be re-contacted for additional information. The sections with no questions are: what is informed consent, what are the possible benefits of the research project to you, what are the costs for taking part in this project, will any commercial products be developed from PMRP, do you have to take part in this project, and the statement of consent.
Paraphrased explanations were typically followed by a personalized communication style to reduce the complexity of the message into more simplified version to improve the comprehension of the participant. The research coordinator never read the text of the consent form verbatim and only comes close to doing so when initially describing the consent form section why they were asked to take part in the research study. ►Table 1 shows the breakdown of the content analysis between paraphrased and personalized sentences. Inter-rater reliability was calculated on one transcript using a Cohen’s Kappa with a “good agreement” result of 73.8%.
Table 1.
Method of communication by transcript
| Communication Method | Transcript A | Transcript B | Transcript C | Transcript D | |
|---|---|---|---|---|---|
| Reviewer 1 | Reviewer 2 | ||||
| n | n | n | n | n | |
| Personalization/Narrative | 25 | 27 | 21 | 35 | 32 |
| Error | 1 | 1 | 2 | 0 | 2 |
| Joke | 0 | 3 | 2 | 2 | 1 |
| Question | 5 | 8 | 8 | 5 | 6 |
| Subtotal: Personalized | 31 | 39 | 33 | 42 | 41 |
| Paraphrased | 71 | 63 | 22 | 79 | 61 |
| Total Sentences | 102 | 102 | 55 | 121 | 102 |
5. Discussion
The purpose of this the study was to determine the relationship between the nonverbal and verbal elements of the informed consent process for PMRP prior to determining how to transform the content and process into a multi-media format. The written informed consent is reinforced through a process that involves both nonverbal and verbal communication. Our main finding was to identify which sections of the informed consent were complex for participants to understand based on the frequency of questions asked. We also identified that different types of gestures, body postures, and verbal communication were used to reinforce the consent process.
The key finding of the observational analysis is the variability in types and frequency of gestures, body posture, and eye gaze. The results of this study are similar to results by Bickmore et al, which showed that face-to-face consents are effective because researchers use verbal and nonverbal behaviors, such as head nods, hand gesture, eye gaze cues and facial displays to communicate factual information to patients, as well as to communicate empathy and immediacy to elicit participant trust [18]. A transition pattern may indicate where the research coordinator uses the paper consent as a way to jog their own memory to ensure that important aspects of the consent are covered. The implication of these findings for the design of multi-media informed consent applications is that developers should ensure that the new application replaces the nonverbal communication with appropriate interaction techniques.
Information that is currently conveyed in gestures need not be replaced with video of the same gestures. The information might be presented using textual cues, pictures, or multimedia to enhance the consent form. For example, highlighting gestures like pointing, tapping, or tracing could be replaced with a stylized text that is bolded or italicized, or with a bigger font size. In the same line of thought, counting gestures, which indicate a list of items, could be replaced with bullet points or numbers. By virtue of the new presentation medium, certain types of gestures including: general hand waving, resting gestures, posture, and eye gaze would be irrelevant and thus could be discarded.
Other types of specific hand waving gestures could similarly be replaced or discarded as appropriate. Repositioning gestures are generally due to the confines of the paper medium where page turns are necessary to bring forward new content, and can probably be discarded. However, the concept of repositioning will need to be replaced by a “next” button at appropriate intervals.
Another application to the replace-ability of nonverbal communication might be to use a animated conversational avatar with a range of nonverbal behaviors, including: hand gestures, body posture shifts, gazing at and away from the patient, raising and lowering eyebrows, head nods, different facial expressions and variable proximity, which is described in greater detail in Bickmore et al., [18].
The benefits of using conversational avatars include: use of verbal and nonverbal conversational behaviors that signify understanding and mark significance, and convey information in redundant channels of information (e.g., hand gestures, such as pointing, facial display of emotion, and eye gaze); use of verbal and nonverbal communicative behaviors to maximize comprehension; use of verbal and nonverbal communicative behaviors used by providers to establish trust and rapport with their patients in order to increase satisfaction and adherence to treatment regimens; and adaptation of their messages to the particular needs of patients and to the immediate context of the conversation [18].
The location of the most challenging concepts within the consent form are visually shown in ►Figure 2, indicating areas where additional material should be made available at the request of the participant in the form of a Frequently Asked Question (FAQ) handout or additional on-demand content. Similar to Bickmore et al., results in this study demonstrate that face-to-face interaction allows researchers to dynamically assess a participant's level of understanding based on the participant's verbal and nonverbal behavior and to repeat or elaborate information as necessary [18].
The benefits of using a FAQ for further clarifying information on the consent form is that it presents information in consistent manner in a low-pressure environment in which patients are free to take as much time as they need to thoroughly understand it [18]. Although research coordinators encourage participants to ask questions, they frequently fail to elicit participant’s questions and participants with limited health literacy are even less likely than others to ask questions [18].
Research coordinators rarely, if ever, read the text of the consent form verbatim. The key finding of the content analysis is that researcher coordinator used both paraphrased and personalized communications and the level of paraphrasing vs. personalization is variable by transcript and by section of the consent form. The communication analysis suggests that information is tailored to the participant using non-legalistic conversational language. Tailoring information to a particular research participant within a computer-based training environment could be done using a comprehension test as a part of the informed consent process similar to that used by Taub et al. through the study of the effect of vocabulary level and corrected feedback [7].
There are several limitations to this study that affect the generalizability of the results. The study was conducted with a small convenience sample in a single lab setting where participants were not actually enrolling in the study and were encouraged to ask questions. The limitation of having subjects who weren’t enrolling in the PMRP project may have affected the number and types of questions participants asked, but this is mitigated by the fact that all subjects were eligible to enroll in PMRP through the standard protocol.
Despite the camera’s being unobtrusively mounted in the ceiling, there is still a chance that performance anxiety affected the nonverbal behaviors of the research coordinator as they attempted to habituate to the setting. Future studies should balance the researcher’s benefits of a naturalistic setting (e.g., potentially better quality interactions) against the research subject’s protections in a “mock” lab setting (e.g., better privacy and blinding of researchers). Having only one research coordinator administer all of the consents presents a bias due to the small sample size, and personal nature of nonverbal and verbal behaviors, however this may be offset by their familiarity and expertise with administering the PMRP consent process that allows them to habituate to the setting better than someone who is less familiar with administering the consent, and to explain things in a more consistent way due to increased practice. Another limitation for the observational analysis was that inter-rater reliability was not formally calculated, as a second reviewer did observe a similar set of gestures for two transcripts but at a coarser granularity than the first reviewer did. For the content analysis, only four transcripts were used due to availability.
This study uses several unique methods of analysis to reinforce the importance of capturing the nonverbal and verbal communication of the informed consent process in a more complete way than previous research studies demonstrate.
6. Conclusion
In the consenting process, a large number and variety of non-verbal and verbal communications supplemented the textual information. This study presents a systematic analysis of the nonverbal and verbal elements of an informed consent process, with the ultimate goal of developing a multimedia informed consent application. By extension, any multi-media informed consent process should take into account the nonverbal, verbal, and textual elements make up the consenting process as experienced by the research subject.
Clinical Relevance Statement
Effective patient-provider or participant-researcher communication and consumer education relies on the coordination of nonverbal, verbal, textual, and potentially multimedia communication. The application of our proof-of-concept results can be used to improve informed consent processes and consumer education materials to increase patient understanding and retention.
Conflict of Interest
The authors have no conflicts to report. Joseph Plasek had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Human Subjects Review
The study was performed in compliance with the World Medical Association Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects and was reviewed and approved by the Institutional Review Boards of Marshield Clinic and the University of Minnesota.
Acknowledgments
This study was grant funded by NIH National Human Genome Research Institute as a part of the eMERGE project, grant number 5 U01 U01HG04608. The authors would like to thank Wendy Foth, the primary research coordinator for PMRP at the Marshfield Clinic for participating in the study. The authors would also like to thank the Marshfield Clinic staffs who were involved with the larger study objectives: Valerie D. McManus, Carol J. Waudby, Joe Ellefson, Dave G. Hoffman, Nancy Stueland-Adamski. The authors would also like to thank the four anonymous reviewers for their comments.
References
- 1.Cohn E, Larson E. Improving participant comprehension in the informed consent process. J Nurs Scholarsh 2007; 39: 273–280 [DOI] [PubMed] [Google Scholar]
- 2.Eakin BL, Brady JS, Lusk SL. Creating a tailored, multimedia, computer-based intervention. Comput Nurs 2001; 19: 152–160; quiz 161–163 [PubMed] [Google Scholar]
- 3.Flory J, Emanuel E. Interventions to improve research participants' understanding in informed consent for research: a systematic review. JAMA 2004; 292: 1593–1601 [DOI] [PubMed] [Google Scholar]
- 4.Green MJ. Use of an educational computer program before genetic counseling for breast cancer susceptibility: Effects on duration and content of counseling sessions. Genetics in Medicine 2005; 7: 221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Green MJ, Biesecker BB, McInerney AM, Mauger D, Fost N. An interactive computer program can effectively educate patients about genetic testing for breast cancer susceptibility. Am J Med Genet 2001; 103: 16–23 [DOI] [PubMed] [Google Scholar]
- 6.Jefford M, Moore R. Improvement of informed consent and the quality of consent documents. Lancet Oncol 2008; 9: 485–493 [DOI] [PubMed] [Google Scholar]
- 7.Jimison HB, Sher PP, Appleyard R, LeVernois Y. The use of multimedia in the informed consent process. J Am Med Inform Assoc 1998; 5: 245–256 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Philipson SJ, Doyle MA, Gabram SG, Nightingale C, Philipson EH. Informed consent for research: a study to evaluate readability and processability to effect change. J Investig Med 1995; 43: 459–467 [PubMed] [Google Scholar]
- 9.Reider AE, Dahlinghaus AB. The impact of new technology on informed consent. Compr Ophthalmol Update 2006; 7: 299–302 [PubMed] [Google Scholar]
- 10.Rosoff AJ: Informed consent in the electronic age. Am J Law Med 1999; 25: 367–386 [PubMed] [Google Scholar]
- 11.Ryan RE Prictor MJ Mc Laughlin KJ Hill SJ Audio-visual presentation of information for informed consent for participation in clinical trials. Cochrane Database Syst Rev 2008; (1)(1):CD003717 [DOI] [PubMed] [Google Scholar]
- 12.Agre P, Rapkin B. Improving informed consent: A comparison of four consent tools. IRB: Ethics and Human Research 2003; 25: 1–7 [PubMed] [Google Scholar]
- 13.McCarty CA, Nair A, Austin DM, Giampietro PF. Informed consent and subject motivation to participate in a large, population-based genomics study: the Marshfield Clinic Personalized Medicine Research Project Community. Genet 2007; 10: 2–9 [DOI] [PubMed] [Google Scholar]
- 14.McCarty CA, Chapman-Stone D, Derfus T, Giampietro PF, Fost N, Marshfield Clinic PMRP Community Advisory Group. Community consultation and communication for a population-based DNA biobank: the Marshfield clinic personalized medicine research project. Am J Med Genet A 2008; 146A(: 3026–3033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Issa MM, Setzer E, Charaf C, Webb AL, Derico R, Kimberl IJ, Fink AS. Informed versus uninformed consent for prostate surgery: the value of electronic consents. J Urol 2006; 176: 694–9; discussion 699 [DOI] [PubMed] [Google Scholar]
- 16.Paterick TJ, Paterick BB, Paterick TE. Expanding electronic transmissions in the practice of medicine and the role of electronic informed consent. Journal of Patient Safety 2008; 4: 217 [Google Scholar]
- 17.Tang JC. Findings from observational studies of collaborative work. International Journal of Man-Machine Studies 1991; 34: 143–160 [Google Scholar]
- 18.Bickmore TW, Pfeifer LM, Paasche-Orlow MK. Using computer agents to explain medical documents to patients with low health literacy. Patient Educ Couns 2009; 75: 315–320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Whishaw IQ, Sacrey LR, Travis SG, Gholamrezaei G, Karl JM. The functional origins of speech-related hand gestures. Behav Brain Res 2010; 214: 206–215 [DOI] [PubMed] [Google Scholar]
- 20.Clark A. Being there: putting brain, body, and world together again Cambridge, Mass.: MIT Press; 1997. [Google Scholar]
- 21.Cook SW, Tanenhaus MK. Embodied communication: Speakers’ gestures affect listeners’ actions. Cognition 2009; 113: 98–104 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Galliher JM, Post DM, Weiss BD, Dickinson LM, Manning BK, Staton EW, Brown JB, Hickner JM, Bonham AJ, Ryan BL, Pace WD. Patients' question-asking behavior during primary care visits: A report from the AAFP national research network. Ann Fam Med 2010; 8: 151–159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs 2008; 62: 107–115 [DOI] [PubMed] [Google Scholar]