

Abstract
Background and Aims:
Complementary alternative medicine (CAM) covers many types of treatments and procedures that are usually not included in conventional medicine and are used in addition to physician-prescribed drugs to “complement” treatment. Although liver disease is prevalent in Saudi Arabia, not much is known about CAM use among Saudi liver disease patients. Thus, this study aimed to assess the prevalence of CAM use in these patients and their attitudes toward it.
Materials and Methods:
Patients were recruited randomly from a tertiary care hepatology clinic at King Khalid University Hospital (KKUH), Riyadh, Saudi Arabia from February 4 to March 20, 2012. A four-page questionnaire was used to interview patients.
Results:
Of all the 232 participants surveyed, 55.6% have used or are using CAM to treat their liver disease with 45.0% of CAM users stating that they believe it has a positive effect on their treatment. Honey was the most used CAM treatment among the participants (39.0%). Herb use was represented by 31.8% of all users, while 13.5% used bloodletting as a treatment. Cautery was the least used CAM method (3.4%). Nearly 76.6% of CAM users were satisfied with using alternative treatments to help control their disease. Nearly 69.4% of users and nonusers stated that they believe CAM treatments to have numerous beneficial effects. Nearly 60.5% of CAM users stated that their physician had no knowledge of their CAM use. Of the factors included in linear multivariate regression analysis (including: Age, gender, and family CAM use, among other socioeconomic factors) only family CAM use was considered a significant independent factor affecting participants CAM use (Beta = 0.582, 95% CI: 0.372-0.754, P = 0.0001).
Conclusion:
More than half of the patients have reported CAM use. Overall, more than two-thirds of the entire sample believed that CAM treatments have numerous health benefits.
Keywords: Complementary alternative medicine, herbs, liver disease, Saudi Arabia
The term complementary alternative medicine (CAM) covers many types of treatments and procedures that are usually not included in conventional medicine. Most of these alternative treatments are based on traditions and are not scientifically proven. Many of these practices have survived to this day and are still used as a way to “complement” physician-prescribed drugs.[1] Despite the lack of sufficient evidence for its clinical efficacy, the CAM industry continues to be profitable as the worldwide annual market for these products approaches US$ 60 billion.[2]
There are many studies worldwide that have investigated the use of CAM and general opinions toward it. Some of these studies have focused on certain diseases like diabetes[3] and cancer,[4,5] while others have studied general populations. Most of these studies revealed a surprisingly high prevalence and an overall positive attitude toward the use of CAM. For example, a study conducted by the Centers for Disease Control and Prevention (CDC) in the United States showed that 40.0% of adults have used CAM in a period of 12 months.[6] One particular study performed in the Kingdom of Saudi Arabia showed a 68.0% prevalence of CAM use among the Saudi participants living in the region of Riyadh who showed generally positive attitudes toward it, referring to it as “natural materials”.[7]
The prevalence of liver diseases in Saudi Arabia is relatively high, and the mortality and morbidity rates are significant.[8,9] Hepatitis C seroprevalence has been reported to be between 1% and 3% in Saudi Arabia, while 1-7% of the population has been reported to be hepatitis B surface antigen carriers.[10] Many of the common liver diseases are chronic, including but not limited to, hepatitis B and C, liver cirrhosis and hepatocellular carcinoma. Hence patients might, in desperation, resort to using CAM in addition to prescribed medication in the hope of finding a cure for their disease.
A study conducted in the United States addressing the prevalence of CAM in liver disease patients showed a relatively high prevalence reaching 39.0%.[11] Unfortunately, local and regional studies addressing the issue of CAM use in liver disease patients are scarce. Therefore, this study was conducted with the goal of establishing CAM prevalence in liver disease patients attending outpatient clinics at King Khalid University Hospital (KKUH) in Riyadh. We also sought to explore the attitude of Saudi liver disease patients toward CAM and document the most common types used in this country.
MATERIALS AND METHODS
A cross-sectional survey was used to collect data from random consecutive patients attending the liver disease clinic in KKUH from February 4 to March 20, 2012. The two inclusion criteria in this study were that the participants had to be Saudi citizens and that they had to have a confirmed diagnosis of a liver disease by their physicians. A full explanation of the study was provided with the questionnaires given to each participant prior to their recruitment, explaining the purpose of this study. Participants were assured that all of their personal information was confidential.
Four types of CAM were explored, namely herbs, honey, bloodletting, and cautery while taking into account other possible alternative treatments used by patients. Patients were interviewed by the researchers personally through a four-page questionnaire that was used to collect data regarding the use of complementary alternative treatments and attitudes toward it. Various epidemiological, social, and medical data were also collected.
The sample size was determined to be 232 using 6.0% as the margin of error, 95.0% as the confidence interval (CI) and estimating the prevalence rate to be 68.0% based on a previous study conducted in Riyadh, Saudi Arabia.[4] The study protocol was approved by the Institutional Review Board in the College of Medicine, King Saud University.
The data was entered into an Excel sheet and then analyzed using the SPSS statistic analysis program: “PASW Statistics 18”. Results were summarized as mean ± standard deviation or frequency (percentage) as appropriate. The Chi-square test was used to analyze differences among categorical variables. A P value of less than 0.05 was considered significant. Odds ratios (OR) and 95% CIs were also used to determine the association between these significant factors and the possibility of patient CAM use. Linear multivariate regression analysis was also done to identify significant independent predictors of CAM use.
RESULTS
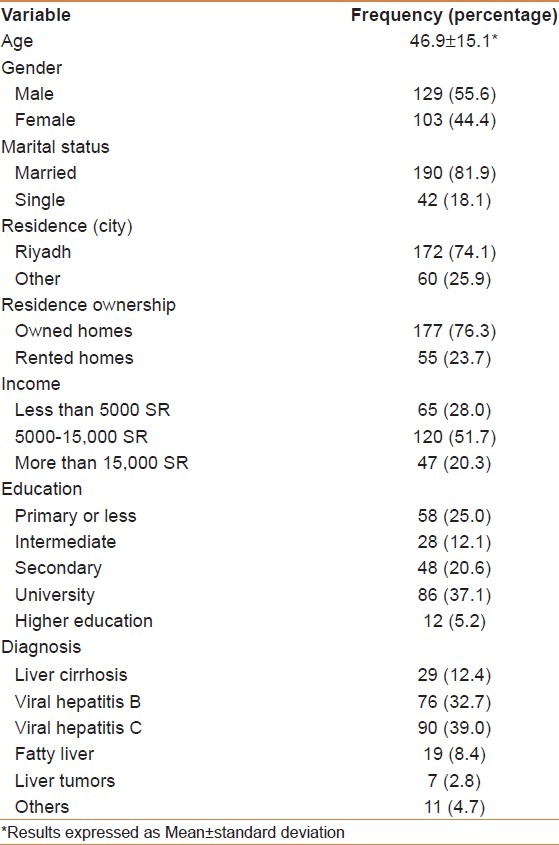
A total of 232 patients were included in this study. Out of these participants, 129 (55.6%) were male. The mean age was 46.9 ± 15.1 years. Overall, there were 51.3% who were aged 45 years or younger. Of the whole sample, 81.9% were married. The most common diagnoses were hepatitis C (39.0%) and hepatitis B (32.7%). Other characteristics describing the sample are summarized in Table 1. Patients with a secondary education or less represented 60.0% of all CAM users. Those earning 5000 Saudi Riyals (SR) and more a month represented 70.8%. The majority of CAM users (60.0%) consisted of participants who had liver disease for more than 5 years. Of all CAM users, 51.5% were aged 45 years or younger.
Table 1.
General characteristics of the study population (N=232)
The results showed that 55.6% of participants have used CAM in an attempt to treat their liver disease. Of all CAM users, 45.0% believed it had a positive effect on their treatment. Nearly 76.6% of CAM users were satisfied with their alternative treatments and only 37.9% believed that it could have future adverse effects.
In this study, we have decided to focus on CAM treatments that we assumed might have a high prevalence. The most common treatments used by our participants are: honey (39.0%), herbs (31.8%), bloodletting (13.5%), and cautery (3.4%). Honey also had the highest acceptance level with 86.3% of its users stating that they consider it as an appropriate treatment for liver diseases. Herb use was prevalent among 31.8% of CAM users, with “black seed (Nigella sativa)” being the most commonly used herb (39.1%) reported by participants [Figure 1]. Out of all herb users surveyed, 40.7% stated they would advise other liver disease patients to use herbal treatment while 23.3% remained neutral. Bloodletting was used by 13.5% of users, with 61.1% of them approving of it as a valid treatment for liver disease. Of the provided treatments, cautery was the least used CAM method among participants as only 3.4% of them reported using it, with only half of them approving of it as a valid treatment.
Figure 1.
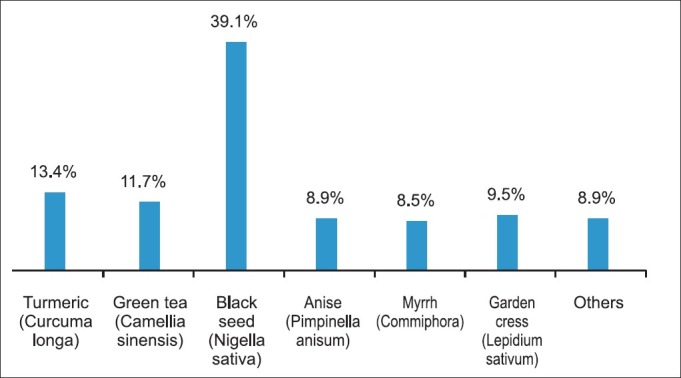
Herb use by liver disease patients attending KKUH
In addition to the treatments mentioned above, the most commonly reported treatments added by CAM users were camel products with 9.8% stating that they have used either camel milk (3.4%) or camel urine (1.1%) or both in combination (5.3%) [Figure 2]. Nearly 1.5% of participants also reported using water blessed by the Holy Quran to treat their liver disease. Participants were given the freedom to select more than one answer and as a result, the most used combination method of treatment was a combination of honey and herbs, which made up 29.7% of all CAM treatments. CAM treatments, in general, were purchased either from local providers (31.4%) (e.g., “Attar” meaning local herbalist shops), commercial stores (17.0%), local farms (5.3%), pharmacies (0.5%), ordered through television or internet (6.4%) or practiced at local clinics (22.9%). Nearly 95.5% of the participants who have used either bloodletting or cautery reported “special” clinics as their source of treatment. The use of all CAM treatments (including: herbs, honey, bloodletting, and cautery, among others) was at its highest in patients with viral hepatitis C followed by viral hepatitis B patients representing 45.2% and 32.1%, respectively, compared with fatty liver (7.7%), liver cirrhosis (12.5%) and liver cancer (1.4%), all of which, showed lower prevalence.
Figure 2.
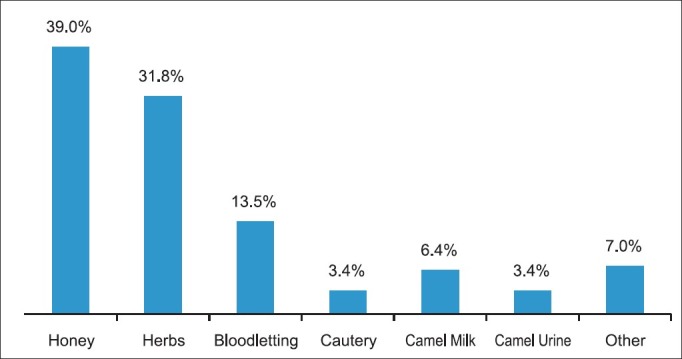
Specific CAM use by liver disease patients attending KKUH
Family and friends were reported as the most common source of information regarding CAM treatments, with family constituting 41.6% and friends representing 17.3% of all suggested sources [Figure 3]. Most participants (39.3%) have stated religious guidance (Quran and Hadith, considered to be the main Islamic religious resources) as their biggest motive for using CAM treatments, with 27.9% reporting that the reputation of success using these treatments was their motivation.
Figure 3.
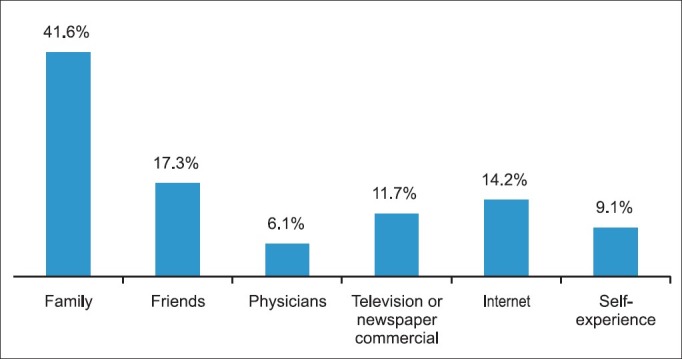
Knowledge of CAM by liver disease patients attending KKUH
When asked about the benefits of CAM, 69.4% of users and nonusers stated that they believe it to have numerous beneficial effects. In contrast, when asked about the side-effects, 32.8% of them believed that CAM treatments had no negative side-effects. A large portion (60.5%) of participants stated that their physician had no knowledge of their CAM use. However, most CAM users (84.6%) revealed that they would stop these treatments if they were asked to do so by their physicians.
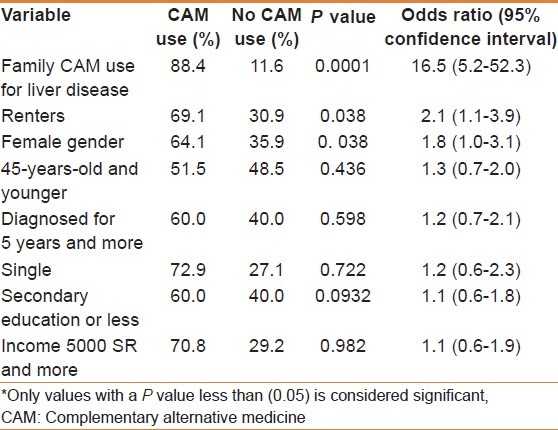
The factors significant in increasing the likelihood of CAM use in this sample were: Gender (more likely for females, OR = 1.8, 95% CI: 1.0-3.1, P = 0.038), type of residence (renters were more likely to be users, OR = 2.1, 95% CI: 1.1-3.9, P = 0.038) and having relatives who have used CAM to treat their liver disease (OR = 16.5, 95% CI: 5.2-52.3, P = 0.0001). Significant and nonsignificant results are summarized in Table 2. However, on multivariate regression analysis, only family CAM use was a significant independent factor on patient CAM use (Beta = 0.582, 95% CI: 0.372-0.754, P = 0.0001).
Table 2.
Factors increasing the likelihood of CAM use (Univariate analysis)
DISCUSSION
Of the 232 patients surveyed, over half (55.6%) reported using at least one form of CAM for the purpose of treating their liver disease. This figure shows that using CAM treatments is common practice among Saudi liver disease patients. This can also be seen in the general Saudi public according to the Saudi Arabia-based study, which reported a 68.0% prevalence of CAM use in the Saudi general public in Riyadh city.[7] This reduction in prevalence can be explained by the fact that the latter study assessed CAM use in the general public and not in a specific population such as liver disease patients. In contrast, the prevalence in our study seems higher than what has been reported by some other regional studies. For example, a study on diabetic patients in Jordan found a prevalence of 31.0%.[3] Two different studies concerning CAM use by cancer patients in Jordan and Turkey found a prevalence of 35.5%[4] and 41.1%,[5] respectively. Similarly, one study based in the United States, which looked at a similar population of interest, found a prevalence of 39.0%, which is considerably lower than the prevalence that we have found.[11] The higher prevalence found in our study compared with regional and international studies might be explained by the cultural differences, as well as social and religious differences between these countries.
CAM seems to have wide acceptance in the Saudi population, as 69.4% of users and nonusers surveyed stated that they believed CAM to have numerous health benefits and 32.8% believed it had no harmful side-effects. This has also been observed in various studies worldwide such as the Jordanian study where 79.2% of CAM users reported they were planning to keep using medicinal herbs as 86.5% of them were content with their diabetes control.[3] This might be related to the strong religious views that many of the patients base their CAM use on (seen in this study and others), and also possibly the unawareness of the lack of scientific evidence and the potential for serious side effects and complications. We have also noticed that usage of camel milk and urine was low, which can be explained by them not being seen as preferred treatments for liver diseases specifically. Another treatment that we have encountered in a surprisingly low prevalence was the use of religious recitations of the verses of the Holy Quran, and prayer for treatment (Ruqiya), the use of which is a distinctive trait of Saudi society, in comparison to other societies assessed in the studies that we have used for reference. The reason behind that seems to be that “Ruqiya” is used generally and as we asked for treatments specifically aimed at liver disease, we assume that patients decided against including it.
When asked about the source of these CAM treatments, most participants stated local providers or local clinics as their source. These sources might not be approved by the Saudi Ministry of Health, which raises concerns over the possible risk of infections and the standards of hygiene, storage, processing, and distribution, since they may not meet the necessary regulations and standards.
The most frequently stated sources of information regarding CAM use were family with 41.6% and friends with 17.3%, which correlates with findings in the Jordanian diabetic study where 47.9% admitted that the reason behind their use was due to advice from their friends.[3] Thirty-nine percent of, participants also stated religious guidance (Quran and Hadith, considered to be the main Islamic religious resources) as their main motivation for their CAM use. These two factors suggest that CAM use is positively affected by cultural and societal influences. However, factors like education, income, and young age did not prove to be statistically significant and thus did not affect CAM prevalence significantly, which stands in contrast to the US study, which described these factors as being predictive of CAM use.[11] Interestingly, we have found that younger participants showed a higher inclination toward using CAM treatments, which is contrary to the belief that CAM is a dying practice, as new generations continue to use it. We have also found that 70.8% of participants earning 5000 SR or more a month used CAM, and that 60.0% of those with a secondary education or less reported using it as well. These results show that socioeconomic factors do not influence CAM use drastically in this sample.
The significant factors found to increase the likelihood of CAM use were female gender, type of residency (more likely for renters), and having relatives who have used CAM to treat their liver disease. Comparing these factors to the US study, female gender is the only common significant factor in increasing the likelihood of CAM use.[11] The last factor was especially noteworthy as it had a considerably large OR of 16.5, meaning that family influence has a very strong impact on the decision to use CAM in this population. Based on our results, we can conclude that family seems to be the most important factor when it comes to using CAM treatments in this population of Saudi liver disease patients. This is expected, seeing that the Saudi community is mostly made-up of close-knit families. We can assume that the strength of these relationships results in placing a substantial amount of trust in the opinions of family members.
When the participants were asked whether they have discussed their CAM use with their physicians or not, 60.5% revealed that their physicians did not know about it, which is much higher than the 26.0% reported by the United States liver study.[11] This is an unfortunate result, as 84.6% of our participants have stated that they would readily discontinue their CAM use if asked to do so by their physician. These results urgently call for physicians to explore these issues with their patients and be more open about it. Being less critical and more understanding may encourage patients to volunteer this information.
Our study, like any other, suffers from a number of limitations. This study was based on an interview survey. This method might have introduced interviewer bias. However, this issue was addressed by ensuring that interviewers did not interfere with participants’ response except for necessary clarification and asking specific and direct questions. In addition, this is a small-scale study, which only addressed patients attending a tertiary care clinic in a referral university hospital, and so the results may not represent the larger population. In contrast, since data in this area is lacking, this study is important as it adds to the literature regarding CAM use in Saudi Arabia. This study provides a stepping stone to conduct future larger scale studies to evaluate CAM use in the general population or other disease areas.
In conclusion, our results have shown that a high percentage of patients attending hepatology clinics have used or are using CAM to treat their liver disease. Honey and herbs were the most common methods of treatment. The study also showed that religious guidance and family influence were strong motivators for the use of CAM treatments. The majority of CAM users reported that their physicians did not know about their CAM use but they would stop using it if instructed by their physicians.
Further studies are needed to explore this extremely important medical issue both in liver diseases and other chronic medical illnesses. As such, physicians are encouraged to delve into this issue with their patients and to enquire about the nature of these alternative treatments. It is also important to stress the need for educational programs directed at the Saudi community discussing the potential harms of CAM use and its possible interactions with physician-prescribed medications and overall risk on health.
ACKNOWLEDGMENT
This project was partially funded by the National Plan for Science and Technology in Saudi Arabia.
Footnotes
Source of Support: This project was partially funded by the National Plan for Science and Technology in Saudi Arabia
Conflict of Interest: None declared.
REFERENCES
- 1.WThe National Center for Complementary and Alternative Medicine. What Is Complementary and Alternative Medicine?.? [Last cited on 2011 Nov 05]. Available from: http://www.nccam.nih.gov/health/whatiscam 2008 .
- 2.United Nations Conference on Trade and Development. Systems and National Experiences for protecting Traditional Knowledge, Innovations and Practices. Background Note by the UNCTAD Secretariat. Geneva, United Nations Conference on Trade and Development, 2000 (document reference TD/B/COM.1/EM.13/2) [Last cited on 2011 Nov 05]. Available from: http://unctad.org/en/docs/c1em13d2.en.pdf .
- 3.Otoom SA, Al-Safi SA, Kerem ZK, Alkofahi A. The Use of Medicinal Herbs by Diabetic Jordanian Patients. J Herb Pharmacother. 2006;6:31–41. [PubMed] [Google Scholar]
- 4.Afifi FU, Wazaify M, Jabr M, Treish E. The use of herbal preparations as complementary and alternative medicine (CAM) in a sample of patients with cancer in Jordan. Complement Ther Clin Pract. 2010;16:208–12. doi: 10.1016/j.ctcp.2010.05.001. [DOI] [PubMed] [Google Scholar]
- 5.Gözüm S, Tezel A, Koc M. Complementary Alternative treatments used by patients with cancer in Eastern Turkey. Cancer Nurs. 2003;26:230–6. doi: 10.1097/00002820-200306000-00010. [DOI] [PubMed] [Google Scholar]
- 6.Barnes PM, Bloom B, Nahin RL. Hyattsville, MD: National Center for Health Statistics, 2008; Complementary and alternative medicine use among adults and children: United States, 2007. Report No.:12. [PubMed] [Google Scholar]
- 7.Al-Faris E, Al-Rowais N, Mohamed AG, Al-Rukban MO, Al-Kurdi A, Al-Noor MA, et al. Prevalence and pattern of alternative medicine use: The results of a household survey. Ann Saudi Med. 2008;28:4–10. doi: 10.5144/0256-4947.2008.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fashir B, Sivasubramaniam V, Al Momen S, Assaf H. Pattern of liver disease in a Saudi patient population: A decade of experience at security forces hospital, Riyadh, KSA. Saudi J Gastroenterol. 1996;2:50–2. [PubMed] [Google Scholar]
- 9.Abdel-Moneim AS, Bamaga MS, Shehab GM, Abu-Elsaad AA, Farahat FM. HCV Infection among Saudi Population: High Prevalence of Genotype 4 and Increased Viral Clearance Rate. PLoS ONE. 2012;7:e29781. doi: 10.1371/journal.pone.0029781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Al Faleh F. Hepatitis B infection in Saudi Arabia. Ann Saudi Med. 1988;8:474–98. [Google Scholar]
- 11.Strader DB, Bacon BR, Lindsay KL, Brecque DR, Morgan T, Wright EC, et al. Use of complementary and alternative medicine in patients with liver disease. Am J Gastroenterol. 2002;97:2391–7. doi: 10.1111/j.1572-0241.2002.05993.x. [DOI] [PubMed] [Google Scholar]