

International guidelines on hypertension recommend maintaining blood pressure (BP) below 140 mmHg systolic and 90 mmHg diastolic in the general hypertensive population up to the age of 80 years. A more aggressive BP target is recommended when the hypertensive patient has an additional risk for cardiovascular disease, such as if the patient has diabetes, renal disease, or a prior history of cardiovascular disease. In these situations, guidelines encourage decreasing BP below 130/80 mmHg to grant additional cardiovascular protection (1–3).
In the last 2 years, the target BP values recommended by guidelines have been the object of some dissenting views (4,5), based on the argument that these targets are often not supported by evidence from prospective randomized trials (4) and that lowering BP too aggressively may do harm rather than ensuring protection. This article addresses this issue by examining three sets of relevant studies: randomized trials, post hoc analysis of prospective studies, and studies on organ damage. Because of space limitations, the References do not include all single trials mentioned; the reader can refer to a recent document of the European Society of Hypertension for this information (5). This is the case also for the acronym of the trials quoted in Fig. 1.
Figure 1.
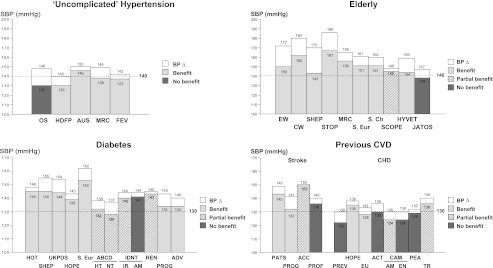
Systolic BP (SBP) values achieved in patients randomized to more active (filled rectangles) or less active (open rectangles) treatment in trials on uncomplicated hypertension, in hypertension of the elderly, and in patients with diabetes or previous cardiovascular disease (CVD). Light gray rectangles indicate trials with significant benefits of more active treatment; deep gray rectangles indicate trials without significant benefits; striped rectangles indicate trials with significant benefits of more active treatment limited to some secondary outcomes. Abbreviations at the bottom indicate trials. Modified from Zanchetti et al. (4).
RANDOMIZED TRIALS
As shown in Fig. 1 (4,5), there is little question that the target BP values recommended by guidelines are not consistently based on trials that compared an actively treated group with placebo or patients treated with less aggressive target BP. To-date trial evidence supports the recommendation to lower systolic BP below 140 mmHg in grade I uncomplicated low cardiovascular risk hypertensive patients, based on the fact that in most trials that involved these patients (although often their “uncomplicated low-risk hypertension category” was questionable [4]), a reduction in cardiovascular events was associated with systolic BP <140 mmHg. In elderly hypertensive patients, on the other hand, there is no consistent support for this target systolic BP, because even though a greater BP reduction in the actively treated group was associated with a reduction in cardiovascular events, in all trials, except for one, the in-treatment systolic BP values remained >140 mmHg. The exception was the Japanese Trial to Assess Optimal Systolic Blood Pressure in Elderly Hypertensive Patients (JATOS), which failed to show a significant difference in the cardiovascular event incidence between treated and placebo patients (6). In patients with diabetes, a large number of placebo-controlled trials also showed the beneficial effects of BP reductions, but in-treatment systolic BP values remained >130 mmHg. The only exception is a small trial, the Appropriate Blood Pressure Control in Diabetes Normotensives (ABCD Normotensives), which had as primary end point the treatment-induced changes in creatinine clearance and was clearly underpowered for detecting differences in cardiovascular event incidence (7). Finally, randomized trial evidence in favor of the protective effect of reducing systolic BP <130 mmHg is limited and inconsistent also for other categories of high–cardiovascular risk individuals, such as patients with a history of stroke or coronary artery disease. In the latter category, several trials succeeded in lowering systolic BP <130 mmHg, often, however, with no cardiovascular benefit compared with the group in which in-treatment systolic BP remained >130 mmHg.
Two more recent randomized trials further question the recommendation that BP should be lowered to <130 mmHg in patients with diabetes. In the Nateglinide and Valsartan Impaired Glucose Tolerance Outcomes Research (NAVIGATOR) trial on prediabetic patients (8), systolic BP was reduced in the actively treated group to ∼133 mmHg without evidence of a reduction in cardiovascular events compared with the group remaining at a somewhat higher systolic BP value (∼37 mmHg). In the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial on diabetic patients (9), reducing systolic BP to <120 mmHg did not show any reduction in the incidence of cardiovascular events compared with the group with a systolic BP of ∼130 mmHg.
POST HOC ANALYSIS OF RANDOMIZED TRIALS
Several randomized trials on hypertensive patients analyzed the cardiovascular event data in relation to the BP values achieved during treatment. The results have usually shown that, regardless of the type of treatment, patients in whom systolic BP was reduced to <140 mmHg showed a decreased incidence of cardiovascular events compared with patients with in-treatment values >140 mmHg (10–13). This is exemplified in Fig. 2, which shows the incidence of cardiovascular events, myocardial infarction, and stroke in the large number of patients with hypertension and coronary disease recruited in the International Verapamil SR-Trandolapril (INVEST) trial (11). For all events, the incidence decreased progressively as the number of in-treatment visits in which BP was reduced to <140/90 mmHg increased, suggesting that consistent BP control at values recommended by guidelines had a protective effect.
Figure 2.

Unadjusted incidence of cardiovascular events in relation to the proportion of visits with BP control in the INVEST trial. Full bars: primary outcomes of the study (all-cause deaths, nonfatal myocardial infarction, and stroke); open bars: fatal and nonfatal myocardial infarction; shaded bars: fatal and nonfatal stroke. Data are shown as percent values. Modified from Mancia et al. (11).
On the other hand, achieving BP values <130 mmHg has shown less consistent beneficial effects. The Irbesartan Type 2 Diabetic Nephropathy Trial (IDNT) and the Perindopril Protection Against Recurrent Stroke Study (PROGRESS) in high cardiovascular risk patients (14,15) showed that in-treatment systolic BP values <130 mmHg (and even 120 mmHg) were associated with a reduced incidence of heart failure and stroke recurrence, (particularly hemorrhagic stroke). However, in other trials, such low achieved systolic BP values were not associated with substantial benefits. Indeed, in large-scale trials on high cardiovascular risk patients, such as the Ongoing Telmisartan Alone and In Combination with Ramipril Global End Point Trial (ONTARGET), INVEST trial, and the Valsartan Antihypertensive Long-Term Use Evaluation (VALUE) trial (10,16–18), in-treatment systolic BP values between 130 and 120 mmHg were associated with an increase rather than a reduction in the overall incidence of cardiovascular events, suggesting the possibility of a “J-curve” phenomenon for BP values close to those recommended as target for people at high cardiovascular risk. This is in line with the results of an analysis of the INVEST trial limited to diabetic patients (19). In these patients, an in-treatment systolic BP between 130 and 140 mmHg was associated with a reduction of cardiovascular events compared with an in-treatment systolic BP >140 mmHg. However, a tighter BP control, i.e, an achieved systolic BP <130 mmHg, was not associated with further benefit. On the contrary, the cardiovascular events rate increased toward the level of the uncontrolled group, with the rise being particularly evident for achieved systolic BP values around or <120 mmHg.
In conclusion, post hoc analysis of randomized trials provide data in favor of the beneficial effects of lowering systolic BP to <140 mmHg, whereas it does not appear to consistently support the guidelines’ recommendation to go below 130 mmHg in high-risk individuals. It should be emphasized that post hoc analysis has limitations, the most important of which is that comparisons are done in nonrandomized groups that may differ for demographic and clinical characteristics. Although minimized by statistical adjustment procedures, one cannot rule out the possibility that the between-group differences in the incidence of cardiovascular events depend on differences in the initial risk profile rather than on the achieved BP.
DATA ON ORGAN DAMAGE
Both prospective and post hoc evidence indicate that, in nephropathic patients, systolic BP reduction to values <130 mmHg is associated with renal benefits, i.e., a decreased progression to end-stage renal disease (5). The evidence is particularly striking for diabetic nephropathy, based on old and new studies that documented that tight BP control may represent the most important therapeutic approach against the appearance and progression of renal disease. A recent example comes from the results of the Action in Diabetes and Vascular Disease Preterax and Diamicron-MR Controlled Evaluation (ADVANCE) trial on >11,000 diabetic patients (20), in which 1) renal events were progressively less common as systolic BP was reduced by treatment to values as low as 110 mmHg and 2) the benefit was seen also in patients in whom initial systolic BP was <140 mmHg and even <120 mmHg. Interestingly, low BP values were also associated with a greater antiproteinuric effect and a reduction in the incidence of new-onset micro or macroalbuminuria. This is clinically relevant because changes in urinary protein excretion by treatment have been shown to reflect the incidence of both renal and cardiovascular events (21–23).
IS OPTIMAL ON-TREATMENT BP TARGET DIFFERENT FOR THE BRAIN, THE KIDNEY, AND THE HEART?
Both prospective evidence and post hoc analysis of prospective trials suggest that lowering BP below 130/80 mmHg may provide cerebrovascular protection, with no further reduction, and perhaps even an increase, in the incidence of coronary events. In the ACCORD trial on diabetic patients (9), for example, the incidence of stroke was significantly less in the group in which systolic BP was reduced to ∼119 mmHg compared with the group in which it remained at ∼133 mmHg, whereas the incidence of myocardial infarction showed no between-group difference. In the INVEST trial (16) on high cardiovascular risk patients, a progressive reduction of achieved systolic BP to ∼120 mmHg was associated with a progressive reduction in stroke, whereas below 130 mmHg, the incidence of myocardial infarction showed a J-curve phenomenon. This was also the case in ONTARGET (16), in which high-risk patients starting with a systolic BP 130 mmHg showed an increase of coronary events when treatment brought about a further BP reduction. In contrast, decreases in stroke events continued to be observed for systolic BP values as low as 115 mmHg (Fig. 3) (16). It is possible that the differential effect of low achieved BP on the brain compared with the heart originates from a more effective cerebral autoregulation, i.e., a better ability to preserve blood flow and tissue perfusion when BP is markedly reduced by treatment, a feature that the brain may share with the kidney. However, because trials have shown that a J curve for cardiac events was conducted in patients with a prevailing history of coronary disease, an alternative explanation is that coronary autoregulation was selectively impaired, that is that the between-organ difference depended on the study population characteristics.
Figure 3.
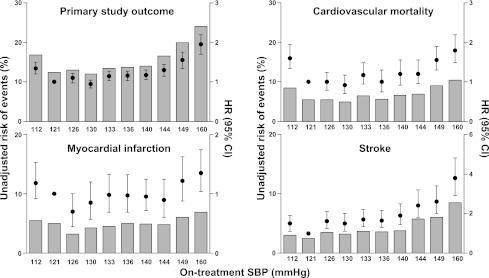
Unadjusted risk of cardiovascular events, cardiovascular mortality, myocardial infarction, and stroke in relation to on-treatment systolic BP (SBP) deciles. Hazard ratio values are also shown for each variable. Data from ONTARGET are shown. Modified from Sleight et al. (16).
CONCLUSIONS
If the data so far available reflect a differential behavior of the brain and the heart with tight BP control by treatment, the question arises as to what could be the practical recommendations. We may speculate that tight BP control may be recommended whenever patients are at higher risk of developing a cerebrovascular event rather than a coronary event. This would apply to patients with a history of cerebrovascular events, since it has been observed that in these patients the recurrence of stroke is much greater than the recurrence of coronary events (24,25).
Acknowledgments
No potential conflicts of interest relevant to this article were reported.
Footnotes
This publication is based on the presentations at the 3rd World Congress on Controversies to Consensus in Diabetes, Obesity and Hypertension (CODHy). The Congress and the publication of this supplement were made possible in part by unrestricted educational grants from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Eli Lilly, Ethicon Endo-Surgery, Generex Biotechnology, F. Hoffmann-La Roche, Janssen-Cilag, Johnson & Johnson, Novo Nordisk, Medtronic, and Pfizer.
References
- 1.Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2007;25:1105–1187 [DOI] [PubMed] [Google Scholar]
- 2.Rydén L, Standl E, Bartnik M, et al. Guidelines on diabetes, pre-diabetes, and cardiovascular diseases: executive summary. Eur Heart J 2007;28:88–136 [DOI] [PubMed] [Google Scholar]
- 3.Graham I, Atar D, Borch-Johnsen K, et al. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Eur Heart J 2007;28:2375–2414 [DOI] [PubMed] [Google Scholar]
- 4.Zanchetti A, Grassi G, Mancia G. When should antihypertensive drug treatment be initiated and to what levels should systolic blood pressure be lowered? A critical reappraisal. J Hypertens 2009;27:923–934 [DOI] [PubMed] [Google Scholar]
- 5.Mancia G, Laurent S, Agabiti-Rosei E, et al. Reappraisal of European guidelines on hypertension management: a European Society of Hypertension Task Force document. J Hypertens 2009;27:2121–2158 [DOI] [PubMed] [Google Scholar]
- 6.JATOS Study Group Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res 2008;31:2115–2127 [DOI] [PubMed] [Google Scholar]
- 7.Schrier RW, Estacio RO, Esler A, Mehler P. Effects of aggressive blood pressure control in normotensive type 2 diabetic patients on albuminuria, retinopathy and strokes. Kidney Int 2002;61:1086–1097 [DOI] [PubMed] [Google Scholar]
- 8.McMurray JJ, Holman RR, Haffner SM, et al. Effect of valsartan on the incidence of diabetes and cardiovascular events. N Engl J Med 2010;362:1477–1490 [DOI] [PubMed] [Google Scholar]
- 9.Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575–1585 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Julius S, Kjeldsen SE, Weber M, et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet 2004;363:2022–2031 [DOI] [PubMed] [Google Scholar]
- 11.Mancia G, Messerli F, Bakris G, Zhou Q, Champion A, Pepine CJ. Blood pressure control and improved cardiovascular outcomes in the International Verapamil SR-Trandolapril Study. Hypertension 2007;50:299–305 [DOI] [PubMed] [Google Scholar]
- 12.Bavry AA, Anderson RD, Gong Y, et al. Outcomes among hypertensive patients with concomitant peripheral and coronary artery disease: findings from the INternational VErapamil-SR/Trandolapril STudy. Hypertension 2010;55:48–53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mancia G, Messerli FH, Weber MA, et al. Association between the proportion of time under blood pressure (BP) control and cardiovascular (CV) morbidity and mortality in the VALUE trial. J Hypertens 2009;27(Suppl. 4):S327 [Google Scholar]
- 14.Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 2001;345:851–860 [DOI] [PubMed] [Google Scholar]
- 15.Arima H, Chalmers J, Woodward M, et al. Lower target blood pressures are safe and effective for the prevention of recurrent stroke: the PROGRESS trial. J Hypertens 2006;24:1201–1208 [DOI] [PubMed] [Google Scholar]
- 16.Sleight P, Redon J, Verdecchia P, et al. Prognostic value of blood pressure in patients with high vascular risk in the Ongoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial study. J Hypertens 2009;27:1360–1369 [DOI] [PubMed] [Google Scholar]
- 17.Messerli FH, Mancia G, Conti CR, et al. Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann Intern Med 2006;144:884–893 [DOI] [PubMed] [Google Scholar]
- 18.Messerli F, Mancia G, Weber MA, et al. Low blood pressure is associated with increased cardiovascular morbidity (J-shape curve) in treated hypertensive patients with increased cardiovascular risk: the VALUE randomized trial. J Hypertens 2009;27:S314. [DOI] [PubMed] [Google Scholar]
- 19.Cooper-DeHoff RM, Handberg EM, Mancia G, et al. Blood pressure goals and cardiovascular outcome in the diabetic population of the INVEST. J Am Coll Cardiol 2010;55:A60 [Google Scholar]
- 20.de Galan BE, Perkovic V, Ninomiya T, et al. Lowering blood pressure reduces renal events in type 2 diabetes. J Am Soc Nephrol 2009;20:883–892 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ninomiya T, Perkovic V, de Galan BE, et al. Albuminuria and kidney function independently predict cardiovascular and renal outcomes in diabetes. J Am Soc Nephrol 2009;20:1813–1821 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ibsen H, Olsen MH, Wachtell K, et al. Reduction in albuminuria translates to reduction in cardiovascular events in hypertensive patients: losartan intervention for endpoint reduction in hypertension study. Hypertension 2005;45:198–202 [DOI] [PubMed] [Google Scholar]
- 23.Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001;345:861–869 [DOI] [PubMed] [Google Scholar]
- 24.PATS Collaborating Group Post-stroke antihypertensive treatment study: a preliminary result. Chin Med J (Engl) 1995;108:710–717 [PubMed] [Google Scholar]
- 25.PROGRESS Collaborative Group Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358:1033–1041 [DOI] [PubMed] [Google Scholar]