

Abstract
Objective
To document the findings of a newborn eye examination programme for detecting ocular pathology in the healthy full-term newborn.
Methods
This is a cross-sectional study of the majority of newborns born in the Kunming Maternal and Child Healthcare Hospital, China, between May 2010 and June 2011. Infants underwent ocular examination within 42 days after birth using a flashlight, retinoscope, hand-held slit lamp microscope and wide-angle digital retinal image acquisition system. The retinal fundus examination utilised the RetCam wide-field digital imaging system (Clarity Medical Systems, Pleasanton, California, USA). The external eye, pupillary light reflex, red reflex, opacity of refractive media, anterior chamber and posterior segments were also examined.
Results
A total of 3573 healthy full-term newborns were enrolled and examined in the programme. There was detection of 871 abnormal cases (24.4%). The majority of abnormal exams were 769 (21.52%) retinal haemorrhages. Of these, there were 215 cases of significant retinal haemorrhage, possible sight threatening or amblyogenic, representing 6.02% of the total. In addition, 67 cases (1.88%) involved macular haemorrhage. The other 107 cases (2.99%) with abnormal ocular findings included subconjunctival haemorrhage, congenital microphthalmos, congenital corneal leukoma, posterior synechia, persistent pupillary membrane, congenital cataract, enlarged C/D ratio, retinal hamartoma versus retinoblastoma, optic nerve defects, macular pigment disorder and non-specific peripheral retinopathy.
Conclusion
Ocular examination of healthy newborns leads to the detection of a significant number of ocular pathologies. The most commonly discovered ocular abnormality during examination of the newborns in this study is retinal haemorrhage. The long-term impact of these findings is unknown. Although presumed by some to benign, neonatal retinal haemorrhages due to birth trauma could be involved in altering visual development. Further work, including prospective examination of newborns with long-term follow-up, is needed and supported by our findings.
Keywords: Child Health (Paediatrics), Retina, Public Health
Introduction
The American Academy of Paediatrics recommends red reflex testing (RRT) shortly after birth.1 Thereafter, children should have their eyes examined by their primary care physician on all well visits. Formal testing of recognition visual acuity will typically commence around 3 years of age. With this schedule, it is assumed that the vast majority of ocular health issues will be discovered. Nonetheless, there remain a significant number of children who despite screening go undetected with respect to vision and eye disorders. A careful review of Pubmed revealed no published literature on the universality, much less the sensitivity and false-negative rate of RRT of normal newborns. Further, this age group has not been studied extensively and the actual prevalence of ocular abnormalities, transient and permanent, is largely unknown. There are few previous studies looking at the incidence of retinal haemorrhages in healthy full-term newborns. Smaller series have been published2 3 previously and one study looked at fundus findings only in critically ill children.4
In the People's Republic of China, there is a move towards a national health standard for children. Neonatal eye examination may play a significant role in this process. The Ministry of Health as part of its National Children's Health Standard encourages newborn examination in detail. This standard has the goal of discovering serious congenital, hereditary and acquired diseases in the neonatal period of healthy newborns. The present study is, to the authors’ knowledge, the first to publish results of a large neonatal eye examination programme.
Materials and methods
Under the umbrella of the Chinese Ministry of Health requirements for general neonatal assessment, the authors devised specifications for neonatal eye examination. These exams were optional for the families. The Ministry of Health funded the eye examinations with occasional funding received from the patient and their insurers. Interested families were educated about the programme and signed an informed consent prior to ophthalmic evaluation. The consent form was reviewed by the hospital and the Ministry of Health ethics and institutional review boards and included statements of the benefits and modest risks of undergoing the eye examination.
From the start of the project, maternal health-related lectures regarding neonatal eye disease were held on a monthly basis for healthcare workers as well as for parents. Lectures covering the paediatric ophthalmology, including anatomy, basic pathology and disease treatment, were held as continuing medical education courses for training of physicians, nurses and allied personnel involved in the programme. This approach was designed to raise participants’ awareness of neonatal ophthalmic disorders. For the first 7 months, the ocular examination rate was 75.54% (1881 examined out of 2490 live births). For the 7 months following, examination rates increased to 93.90% (2126 examined out of 2264 live births).
Between May 2010 and June 2011, there were 4754 live births in the Kunming Maternal and Child Healthcare Hospital, Kunming, Yunnan Province, China. Of those, 4007 (84.29%) infants received a neonatal eye examination either at the hospital or returned after discharge within 42 days of birth.
This work focuses the analysis on the 3573 healthy full-term infants who underwent an eye examination within 1 week of birth (mean 2.35 days). In our study, a normal newborn is defined as having ≥37 weeks’ gestational age, weighing ≥2500 g. Further, the normal newborn has no evidence of systemic disease and an Apgar score of 7 or more. The male to female ratio was 1785 : 1788. Infants whose mothers had known transmitted diseases (eg, STDs, hepatitis B, HIV positive) were excluded. Infants who were premature or were examined after discharge at 42 days of birth with other follow-up were not included in this series.
The examinations were performed by a team consisting of an ophthalmologist and assisted, at times, by a nurse. An external examination of the eyes was performed first, which included the anterior segment and pupillary light reflex using a standard flashlight. Infants were then dilated with two drops of 1% tropicamide administered 10 min apart. After mydriasis, the RRT, retinoscopy and hand-held slit lamp examinations were performed to evaluate the clarity of ocular media. Topical anaesthetic was instilled. The anterior segment was examined using the non-contact wide-angle portrait camera lens.
Next a sterile eyelid speculum was placed in the eye to be examined. The anterior chamber angle was then evaluated with the 130° lens, tilted appropriately to image the angle in at least four quadrants. Using the RetCam, a wide-angle digital fundus camera examination was then performed in first one eye and then the other. Photos were taken of the posterior pole, including the optic nerve and macula. The superior, inferior, nasal and temporal retinal fields were imaged when possible. For patients in whom the eye exam revealed an abnormal finding, repeat examination or referral to the ophthalmology clinic was performed at a later date.
Data from the examinations were logged onto a spreadsheet and the Pems 3.3 (Package for Encyclopaedia of Medical Statistics) package was used for analysis.
Results
Of the 3573 healthy full-term newborns who underwent newborn eye examination, 871 (24.4%) cases were found to be abnormal. Of the total examined, 769 (21.53%) had retinal haemorrhages (figures 1 and 2). There were no statistically significant differences based on gender. Of these, 215 cases (6%) were Grade 3 (table 1) retinal haemorrhage and 67 cases (1.9%) involved macular haemorrhage. There were visually threatening ocular abnormalities in 107 cases (2.99%), of whom 28 were associated with retinal haemorrhage. These cases are summarised in table 2 below.
Figure 1.
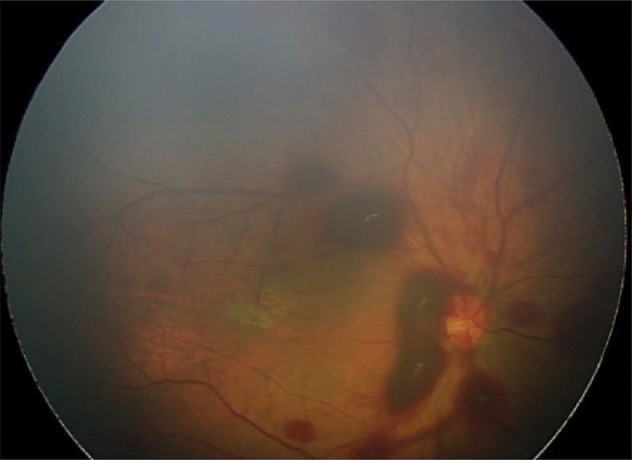
Retinal haemorrhages discovered on newborn digital eye examination.
Figure 2.
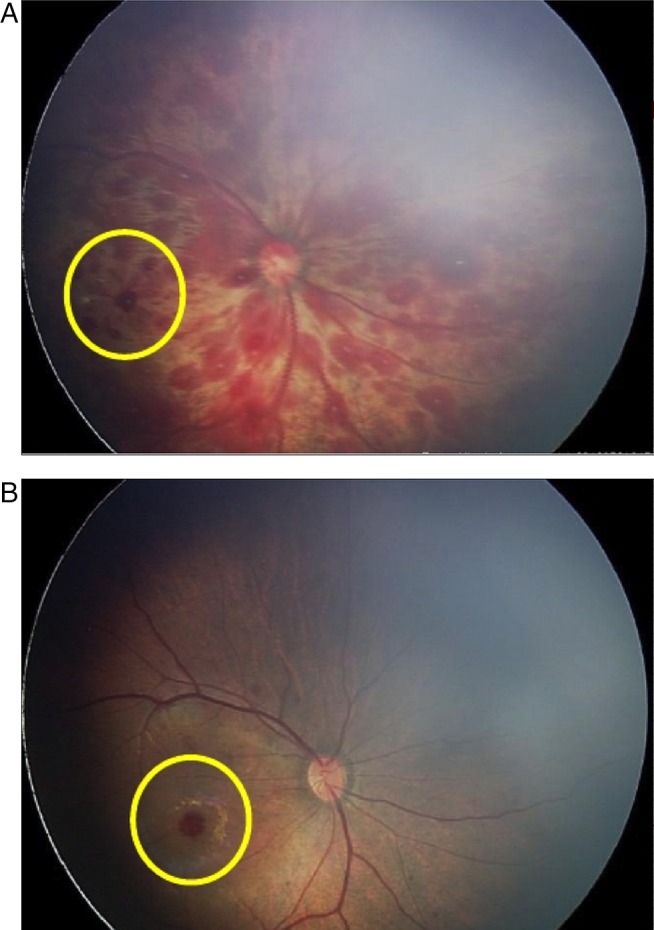
(A) Above: oculus dexter (OD) with Grade 3 retinal and macular haemorrhage; (B) Bottom: Review after 3 weeks shows persistent macular haemorrhage OD; retinal haemorrhage OS completely absorbed.
Table 1.
| Grade | Description |
|---|---|
| Grade 1 | Small retinal haemorrhage confined to the area around the optic nerve, associated with dot or fine linear bleeding. |
| Grade 2 | Slightly larger amount of retinal haemorrhage than Grade 1; patchy, dot, blot or flame-shaped aemorrhage, size does not exceed the optic disc diameter. |
| Grade 3 | Retinal haemorrhage more than the diameter of the optic disc area, a line of flame-shaped haemorrhage along vessels, macular haemorrhage (alone constitutes Grade 3). |
Table 2.
Results of abnormal eye screening of healthy newborns with the RetCam Digital Imaging System
| Abnormality found on newborn screening | Number of patients | Percentage out of 3573 infants |
|---|---|---|
| Retinal haemorrhage | 769 | 21.52 |
| Subconjucntival haemorrhage | 50 | 1.40 |
| Vitreoretinopathy (likely retinopathy of prematurity vs FEVR) | 15 | 0.42 |
| Abnormal fundus pigmentation (ex. CHRPE) | 9 | 0.25 |
| Optic nerve dysplasia/MGDA | 7 | 0.20 |
| Idiopathic retinal venous tortuosity | 4 | 0.11 |
| Severe optic nerve cupping | 3 | 0.08 |
| Congenital cataract | 2 | 0.06 |
| Persistent foetal vasculature | 2 | 0.06 |
| Retinal mass—retinoblastoma versus hamartoma | 2 | 0.06 |
| Optic nerve coloboma | 1 | 0.03 |
| Corneal leukoma | 1 | 0.03 |
| Microphthalmos | 1 | 0.03 |
| Fundus lesions without firm diagnosis—presumed infectious aetiology | 5 | 0.14 |
| Total | 871 | 24.39 |
Retinal haemorrhages are excluded and are reported separately within.
FEVR, familial exudative vitreoretinopathy; MGDA, morning glory disk anomaly.
Additionally, the examinations revealed multiple other ocular pathology of visual and possibly systemic significance. Findings include retinal hamartoma versus retinoblastoma discovered on day 3 of life. Figure 3 demonstrates familial exudative vitreoretinopathy (FEVR). Other pathology discovered on neonatal eye examination includes examples of retinopathy due to infectious causes such as cytomegalovirus, optic nerve anomalies, C/D enlargement and dysplasia versus morning glory disk anomaly. In the latter disorder, there exists a high risk of CNS comorbidity such as encephalocoele and moyamoya disease.5
Figure 3.
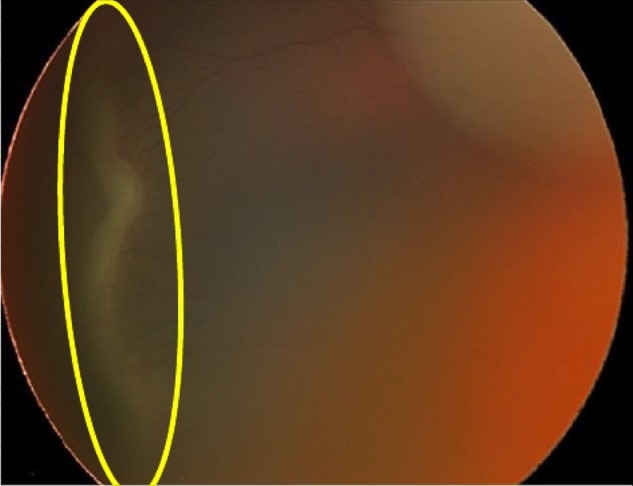
Presumed familial exudative vitreoretinopathy discovered on digital newborn examination in a full-term newborn.
Discussion
Our data reveals, for the first time, that a significant number of healthy newborns exhibit ocular abnormalities on digital ocular examination. Further, the highest proportion of abnormal findings during the study period was retinal haemorrhages, accounting for 92% of abnormalities. Results of a study of ocular screening of preschool children report that refractive errors account for 73.5% of ocular abnormalities.6 Of course, the incidence of newborn eye disease is not the same as reported in routine paediatric ophthalmology clinics.7 In the vast majority of cases, as we have always suspected, the eyes develop normally and most infants are unaffected by ocular disease in the neonatal period. Furthermore, it is postulated that the majority of ocular abnormalities found on the newborn examination will have resolved without sequelae before preschool screening. In fact, it is an unsupported assumption that disorders of the neonatal fundus, particularly retinal haemorrhages due to birth trauma, are at best very rare and at worst transient and benign. This is, however, speculation and our data point to the need for further study in this area. Is it possible that some visual disturbances seen later in childhood (ie, anisometropia, amblyopia) have their genesis or are manifest in the neonatal period? There are several theories being postulated that retinal blur may have a profound impact on normal optical development and emmetropisation of the eye.
In normal neonatal retinal development, macular cone cells are generally mature at 4–6 months of age. The congenital causes of amblyopia have been speculated by retrospective analysis in the past, leading to the consideration that some forms of ocular and visual disturbance may have developed during the perinatal period. Retinal haemorrhages, for example, could limit the function of the visual pathway and thus affect the normal development of visual function.6 7 It is generally understood that Grade 1 and 2 retinal haemorrhages can dissipate quickly and be absorbed without leaving a trace, causing no discernible effect on visual development. Third-degree macular haemorrhage however, can leave a long-term impact on vision.8 9 In this study, Grade 3 haemorrhages accounted for 27.82% of the total retinal haemorrhages. In addition, macular haemorrhages accounted for 1.88% of the total incidence of abnormalities or 8.71% of the retinal haemorrhages. This group of children, particularly those with macular haemorrhages detected during the ocular examination, as in figure 2, requires a long-term observational study in order to understand the significance, if any, of retinal haemorrhages on future ocular growth and development. Most neonatal retinopathy is neither discovered nor reported, as normal newborn ocular examination is not widely carried out. However, the authors believe that it is necessary to understand, recognise and monitor the incidence and variation of ocular disease in newborns in order to understand and, perhaps, minimise its impact on the development of normal visual function.
Some neonatal eye disease is time sensitive, and if found late, the best opportunity for effective treatment is missed, leading to irreversible visual impairment. In rare cases, such as retinoblastoma, late detection can be life threatening. Figure 4 shows retinoblastoma versus retinal hamartoma found in an infant 3 days of age that was detected during the digital fundus examination. This child had no family history of retinoblastoma and was otherwise normal systemically. This is by far the youngest age reported for detection of this disease, giving this infant the great advantage of early intervention. The child was treated with laser and after 8 weeks of follow-up, results showed that the tumour had shrunk, retaining vision in the eye and, perhaps, saving a young life.
Figure 4.
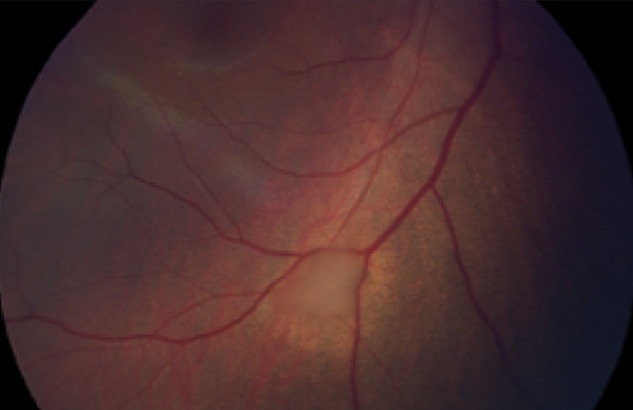
Retinal hamartoma versus retinoblastoma found in an infant 3 days of age.
Newborns are unable to express ocular or visual disorders as adults do and only through an examination, the neonatal eye diseases can be detected. RRT, when done and done properly, will pick up some disorders of the visual system at birth; examples include obvious leucocoria, strabismus and external masses. The true sensitivity of RRT cannot be elucidated due to the variability of its use. Our study shows that many cases of ocular abnormalities would likely be missed on RRT alone, especially discrete abnormalities of the optic nerve or peripheral ocular pathology.
This study has limitations: (1) foremost, an ocular examination programme such as described could not be mandated for each normal newborn, and it is not the authors’ intention to in any way suggest this. (2) The potential financial, personnel and logistic issues are far beyond the scope of this report to discuss but are important to the overall discussion nonetheless. In the current study, some participant families contributed financially and the programme is self-supporting. Analogously, newborns will routinely undergo hearing and metabolic screening in an effort to catch rare disorders that can impact the infant's health; the patient, insurance companies, the hospital and the state variably cover these examinations. The authors have found a relatively high percentage of pathology, primarily retinal haemorrhages, although the final impact of these findings on paediatric ocular disease is largely unknown. The data presented here must be augmented and, more importantly, carried forward. It will be very useful to perform a prospective study and carry the examinations of these and subsequent infants forward in order to correlate early fundus findings with eventual ocular and visual disease. It will be fascinating to follow patients with early, severe retinal haemorrhages to see whether there is indeed a long-term impact on the visual system. Until then, the authors strongly support work aimed at increasing the diagnosis of ocular disease at a young age through early examinations, such as in this report. The examinations should be done at the discretion of the treating obstetrician, paediatrician, neonatologist and indeed the parents.
Neonatal ocular examination may play a positive role in promoting paediatric eye health to paediatricians and parents. As part of the comprehensive newborn health examination process, it may prove invaluable in discovering pathology at an early stage. The RetCam exam can be taught to nurses and physician extenders with formal examinations being reserved for those infants’ abnormal findings. Through community outreach, we have been successful in educating pregnant women about this screening project through large interactive classroom sessions taught with illustrated, easy to understand training materials. Additionally, health booklets, magazine prescriptions and general health education material have been produced and distributed. Parents who participate in these active sessions facilitate adherence to the programme, making our neonatal eye screening initiative sustainable and more effective.
The authors present the results of ocular examination on the largest group of normal, healthy newborns to date. The data show a high percentage of retinal pathology, chiefly haemorrhages. It has been assumed that retinal haemorrhages due to birth trauma are typically benign. This supposition has not been based on large-scale studies of normal newborns. With more data, our view of the influence of birth haemorrhages upon normal ocular development may shift. This initiative may provide impetus for further scientific work on the importance, if any, of early retinal haemorrhages on visual development. Our investigative group has shown through the examination of over 3000 newborns that the use of advanced digital imaging technologies, such as the RetCam, is safe, convenient, fast and objective. Further, the programme provides a way to comprehensively evaluate and document an infant's eye. It remains to be seen if early discovery of pathological findings can indeed lead to the decrease in visual morbidity. A protocol is currently being developed for the prospective examination of the newborn fundus along with sustained follow-up in order to track resolution and the possible sequelae of abnormalities discovered on digital examination.
Footnotes
Contributors: Each author listed has participated in this work and can take public responsibility for appropriate portions of the content. The authors listed have substantial contributions, including conception and design, data acquisition, analysis and interpretation. All authors approved the final submitted version of this article.
Competing interests: None.
Ethics approval: Kunming Maternal and Child Healthcare Hospital Ethics Board and Cleveland Clinic IRB.
Provenance and peer review: Not commissioned; externally peer reviewed.
Open Access: This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
References
- 1.American Academy of Pediatrics; Section on Ophthalmology; American Association for Pediatric Ophthalmology And Strabismus, et al. Red reflex examination in neonates, infants, and children Pediatrics 2008;122:1401–4 [DOI] [PubMed] [Google Scholar]
- 2.Hughes LA, May K, Talbot JF, et al. Incidence, distribution, and duration of birth-related retinal hemorrhages: a prospective study. J AAPOS 2006;10:102–6 [DOI] [PubMed] [Google Scholar]
- 3.Ju RH, Ke XY, Zhang JQ, et al. Outcomes of 957 preterm neonatal fundus examinations in a Guangzhou NICU through 2008 to 2011. Int J Ophthalmol 2012;5:469–72 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Agrawal S, Peters MJ, Adams GG, et al. Prevalence of retinal hemorrhages in critically ill children. Pediatrics 2012;129:1388–96 [DOI] [PubMed] [Google Scholar]
- 5.Traboulsi EI. Morning glory disk anomaly—more than meets the eye. J AAPOS 2009;13:333–4 [DOI] [PubMed] [Google Scholar]
- 6.Egge K, Lyng G, Maltau JM. Retinal hemorrhages in the newborn. Acta Ophthalmol (Copenh) 1980;58:231–6 [DOI] [PubMed] [Google Scholar]
- 7.Egge K, Lyng G, Maltau JM. Effect of instrumental delivery on the frequency and severity of retinal hemorrhages in the newborn. Acta Obstet Gyneco Scand 1981;60:153–5 [PubMed] [Google Scholar]
- 8.Von Noorden GK. Classification of amblyopia. Am J Ophthalmol 1967;63:238–44 [DOI] [PubMed] [Google Scholar]
- 9.Von Noorden GK. Factors involved in the production of amblyopia. Br J Ophthalmol 1974;58:158. [DOI] [PMC free article] [PubMed] [Google Scholar]