

Abstract
The tobacco-free generation proposal advocates legislation precluding the sale and supply of tobacco to individuals born after a certain year. The measure is aimed at overcoming defects with current youth access laws that suffer from rite-of-passage and mixed signalling effects. Since its introduction in 2010, the proposal has attracted international attention, highlighting a number of matters that the present short article discusses. Efficacy issues, including retailer compliance, supply by surrogates and illicit sales, are addressed in the broader setting of community adherence to legislation. Encouragement for the likelihood of successful implementation is provided by historical precedents. In principle objections, relating to choice and generational fairness, are considered against the criteria of consistency and proportionality. It is concluded that the measure's emphasis on the welfare of future generations and its regard for the interests of existing stakeholders provide a feasible opportunity for the ultimate eradication of tobacco supply in appropriate jurisdictions.
Keywords: End game, Public policy, Tobacco industry, Addiction, Denormalization
Introduction
More than 80% of smokers start by age 18, and virtually all by 26.1 Therefore, preventing youth initiation may be the key to ending the tobacco epidemic.2 3 The preventive measure considered here is the tobacco-free generation proposal: In addition to existing laws, prevent supply of tobacco to those born in or after a specified year, such as the year 2000.4
This article first addresses the logic of existing youth access laws, the arguments that led to their introduction and the less evident reasons for their shortcomings. To appreciate why such laws have failed to ‘put the problem in the rear-view mirror’,5 it is necessary to consider the issue of compliance with a law (including not inciting disobedience in others) rather than simply enforcement. This provides a lens through which to observe the anomalous treatment of tobacco, how this treatment undermines underage laws and how the tobacco-free generation approach overcomes these problems. Historical precedents for this approach are also referenced.
Considerable international public discussion has been generated by the measure and subsequent developments, including its unanimous support in August 2012 by the Upper House of the Parliament of Tasmania,6–9 a jurisdiction aligned with the Framework Convention on Tobacco Control (FCTC). It is therefore timely to provide brief comment on issues raised in such debate.
Rationale for existing laws
In recognising both the difficulty of forcing addicts to quit10–13 and the importance of preventing initiation among teenagers, many jurisdictions have introduced restrictions on supply (including sale) of tobacco to those under a certain age. Although many people adhere to these laws, evidence supporting their effectiveness is limited.14–16 To understand why, it is useful to reflect on what makes a law effective.
Efficacy of laws
Figure 1 highlights factors influencing public adherence to a law.17 It is important to attend to personal and social influences in designing statutes, rather than assume that instrumental factors (deterrents) alone suffice.
Figure 1.

Typology of determinants of adherence to a law.
Current deficiencies
Both large-scale questionnaire surveys18–20 and intensive interviewing21 indicate that the primary initiators of teenage consumption are:
peer influence: predominantly among same-age friends/acquaintances
the desire to appear grown-up/look cool.
For example, 62% of European women smokers surveyed cite (1) and another 26% (2) as a reason for smoking initiation (tables 3 and 6 in the cited article);18 ‘the most proximal factor associated with smoking behaviour in these schools is the prevalence of the behaviour among an adolescent's peers’;22 89% of school-going daily smokers questioned had ever given tobacco to an underage teen, and 85% of that group had given to a same-age friend or acquaintance.23
There are two important drawbacks to an ‘underage’ restriction. First, it creates a rite-of-passage effect: 16- or 17-year-olds may think that by smoking they appear 18, as reflected in the tobacco industry's ‘Kids don't smoke’ campaigns.24 25
Second, it has an adverse signalling effect: If the government says that smoking is acceptable for an 18-year-old, then can it really be dangerous for a 16- or 17-year-old?26 Thus, the tobacco industry's frequent boast is: ‘It's a legal product.’27 Moreover, its counterintuitive position undermines governmental authority.
In the above typology, underage laws (as specified by FCTC)28 attempt to rely on the instrumental and legitimacy aspects of compliance, but overlook countervailing influences that they establish with regard to the personal empirical, social descriptive and legitimacy modes.29
Compare the anomalous current legal status of tobacco with other age-restricted activities and addictive harm-causing substances. Tobacco is the outlier: its legal status conforms neither to associated social norms nor to its empirical dependence hazard (tables 1 and 2).30–32
Table 1.
Age-restricted activities and their adult social norms
| Activity | Social norm (for adults) |
|---|---|
| Driving | Encouraged |
| Movie-going | Encouraged |
| Voting | Encouraged |
| Sex | Broadly encouraged |
| Alcohol consumption | Encouraged in moderation |
| Tobacco consumption | Discouraged |
Table 2.
Hazardous addictive substances and their current legal status for availability to adults
| Substance | Addictiveness | Legal status |
|---|---|---|
| Alcohol | Low | Slightly restricted |
| Marijuana | Low | Banned |
| Heroin | High | Banned |
| Cocaine | High | Banned |
| Methamphetamine | High | Banned |
| Tobacco | High | Unrestricted |
Table 3 compares the present legal permissions with actual choices being made, by age of first purchase, in Australia where adult tobacco prevalence is 16%,33 and the current smokers’ juvenile commencement rate of 80% is used.1
Table 3.
Permission versus reality for current tobacco initiation, by age at first purchase
| <18 | 18+ | |
|---|---|---|
| Current legal permission | 0% | 100% |
| Current actual initiation | 13% | 3% |
The tobacco-free generation proposal
The following pattern by which schoolchildren are introduced to cigarette consumption23 explains how reduction in retail sales induced only by instrumental measures (such as from FCTC Article 16)28 reduces cigarette consumption but not initiation,34 as, although packets are purchased less frequently, peer-sharing of individual cigarettes continues (figure 2).35
Figure 2.
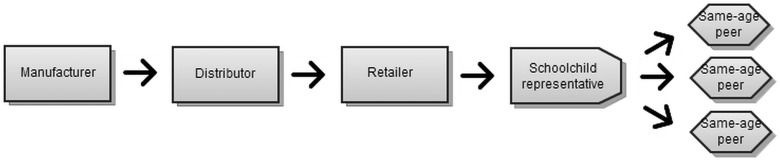
Dominant model for cigarette supply to experimental phase consumers.
This pattern is vulnerable to a normative change within the peer group. If there are insufficiently many same-age peers willing to share and buy cigarettes from each other, then the purchase of a packet is more difficult for the novice smoker to justify, prompting a ‘tipping point’36 37 in the group's behaviour. Such a normative change can be achieved by addressing the rite-of-passage and signalling defects of current policy.
Therefore, avoiding expecting existing smokers to quit, and denying that smoking is acceptable from a particular age, the tobacco-free generation proposal names a future date (the effective date) after which there are to be no new recipients of tobacco products. In a country with an existing under-18 law, a suitable effective date is 1/1/2018 (corresponding to a birth date of 1/1/2000).
People born before the birth date are still able to be supplied with tobacco. For them, existing laws apply. However, people born subsequently may never be supplied with tobacco. For maximum social acceptance, and to minimise the number of teenagers becoming addicted prior to the effective date, the announcement of the measure should occur as many years in advance of the effective date as possible.38
Impact on supply is obvious, but demand impact (removing personal empirical, social descriptive and legitimacy drawbacks of underage legislation) is also important. It addresses the rite-of-passage effect and enables peer influence to work in its favour: public health campaigns (especially where tobacco marketing is prohibited) are able to present smoking as a ‘last-century’ phenomenon. Over time, the age gap between teenagers and the visible smoking population steadily widens, facilitating a favourable ‘norm cascade’37 of ever-lower smoking prevalence among late-teenage cohorts benignly influencing subsequent cohorts. Thus, enforcement becomes progressively easier: ‘the best law is one that so shapes social norms that it becomes self-enforcing’.16
The measure's wording can be tailored so that eventually regulation of all dangerous addictive substances more properly reflects their relative hazards (see table 2).
Issues raised: efficacy
Although widely accepted that the proposal would result in an improvement on the present situation, the following issues concern how large that improvement would be.
Retailer compliance
Because retailers can be important enablers of the proposal's success, supporting policies should recognise their motivations. They are often apprehensive of losing a higher margin product line, and despite personal ethical inclinations may be fearful of losing customers to non-complying competitors (a social descriptive effect39).40 Policies should both be instrumental and maximise awareness of competitors’ compliance.41 42 This ‘norm transformation’39 can occur (in a vending-machine-free environment) with all tobacco retailers both licensed and counselled (see Precedents section below), numerous spot checks (until the new norm becomes established),43 a single infraction leading to license revocation (emphasising frequency of checking) and initial license revocations heavily publicised. Even with underage laws, similar policies have led to significant reductions in youth smoking.44–46 Stakeholder concerns (not necessarily realised47) can also be allayed by pointing to the availability of emerging product lines (clothing, cosmetics, IT, entertainment tickets) that attract teenage purchasing power released by the decline in tobacco sales. The measure's gradual effect on adult tobacco prevalence allows economic stakeholders considerable time for adjustment, as does an early announcement date.
The new measure also makes compliance easier for retailers compared with current underage laws. Instead of checking an identity card and then calculating age as at present required (but often omitted48), only date-of-birth need be checked: no calculation is needed.
Alternative supply
The concern is sometimes expressed that parents, older siblings or older friends will introduce tobacco consumption to the tobacco-free generation's children. However, there are two grounds for reassurance. First, smoking initiation predominantly occurs in the company of same-age peers.23 49 Second, whereas currently many people act on an expectation that youth will eventually smoke, the proposed legislation will change that social descriptor, freeing people to align to personal ethical motives: one professional survey revealed 98.8% of respondents regarding it as important to protect children from ever taking up smoking.4 Compare laws mandating car seats for infants, and prohibiting smoking in vehicles in the presence of children, that, although difficult to enforce, succeed by virtue of their expressive function that clarifies the role of a ‘good parent’ when driving a car occupied by a child.50
Regarding potential induction of adults by friends or colleagues, recall that currently, even with mixed legislative signals about the acceptability of smoking, only a small percentage of the adult population commences the practice of smoking (see table 3).
By avoiding forced cessation among existing users (another important class of stakeholders), the measure creates no new denied addicts needed to fuel a black market (despite likely tobacco industry supply efforts51). Sales to the unaddicted depend on the desire for experimentation, the next topic.
‘The whole smoking process is part of the illicit pleasure category. This illicit pleasure will lose its illicitness once they grow older... The cigarette is the entrance ticket to the hall of the adult society.’52 ‘Before I turned 21, the attraction of the whole bootleg culture of underage drinking was irresistible. It was the last frontier of the forbidden grown-up privileges.’53 Evidently, it is the temporal nature of the forbiddance that makes forbidden fruit attractive. By contrast vandalism (perpetually forbidden) is relatively rare;54 this is despite the low likelihood of apprehension and its possibilities as a peer-group activity.
Precedents
Two well-established precedents for the proposal's generational method for phasing out smoking concern opium smoking. The first was introduced in Formosa in 1900 (effective date, 1908): ‘first, to place the opium commodity under Governmental monopoly; second, to prohibit nonsmokers from acquiring the habit; third, to require the registration of all habitual smokers, who thereafter would be allowed to purchase the drug only upon presentation of a license, this in turn being shielded by legislative rule; fourth, to encourage smokers to abandon the habit; and, finally, to impress upon non-smokers the baneful influences on morals and on all progress which so surely follow in the wake of the habit.’55 At the 1924 Geneva Conferences on Opium, statistics were produced to show a more than 80% reduction in opium smokers from 1908 to 1923.56
The second instance occurred in British Ceylon in 1910 (effective date, 1911). In 1957 an independent commission reported that within 35 years opium use had been eradicated, and recommended the method as a model for dealing with then-current alcohol concerns.57
In both cases, additional initiatives were introduced to enhance the effectiveness of the generational measure, in the areas of supply control, registration/licensing of addicts, cessation programmes and education, some along similar lines to proposals elsewhere in this Supplement.56 58
Issues raised: principles
Objections to the measure based on philosophical principles tend to fail two key practical criteria: proportionality and consistency. For proportionality: how many deaths are acceptable to maintain the principle? (Noting the Willingness to Accept–Willingness to Pay (WTA-WTP) disparity59 60 and framing effects,61 one could more bluntly ask: how many deaths would one be willing to induce to enforce the principle?) How does that number of deaths compare with the number who die annually from tobacco?
Consistency arguments require clarity about the principle concerned (which claims of ‘nanny states’ and ‘slippery slopes’ usually lack).62 Advocates of a principle often overlook past breaches of it that are now so widely accepted as to be unnoticed.
Denial of choice
Concerning consistency, there are numerous constraints on consumer choice, including sale of various toxic food and pharmaceutical substances, lead-based paints and asbestos insulation. Although tobacco industry spokespersons like to refer to ‘adult choice’, a more accurate depiction of the present situation is ‘child choice, adult addiction’; hence the description of tobacco as a ‘pediatric disease’.63 The reality (table 3) is that only 3% of future adult cohorts would have their desire for purchase instrumentally restrained by the proposal; the proposal's major impact comes from its effect, both instrumental and normative, on the 13% who currently suffer underage initiation. Moreover, with the wording of the measure directed only to provision and sale, then even this 3% will remain able to grow tobacco for their own consumption.
For the proportionality test, compare this 3% with the approximately 20% of US adults who die prematurely from tobacco (including 2% from passive smoking).1 64
The addictiveness of tobacco is important in relation to the issue of choice. As ethicist Peter Singer notes: ‘Even setting aside the harm that smokers inflict on non-smokers, the free-to-choose argument is unconvincing with a drug as highly addictive as tobacco, and it becomes even more dubious when we consider that most smokers take up the habit as teenagers and later want to quit.’65 Well-known benchmarks for intervention versus choice include the Nuffield Intervention Ladder.66 67
Age discrimination
Cohort discrimination has already occurred widely, with examples such as introduction of compulsory education, compulsory immunisation and conscription, whether universal or non-universal determined by birthdate.68
As a further gauge of the applicability of the above principles of choice and age fairness, consider the following. If there becomes available a vaccine that is both safe and effective only if administered to children, is it responsible conduct to withhold free universal access on the grounds either that:
the children are not able to exercise adult choice whether or not to be vaccinated, or
the introduction of the vaccine would unfairly discriminate against those who are no longer young enough to be vaccinated?
Sometimes authorities have to make decisions on behalf of future generations; in the case of tobacco, former Australian Health Minister Roxon observes ‘We are killing people by not acting’.69
Conclusions
The observation that successful laws are those that generate popular compliance focuses attention on two main reasons why existing underage restraints on tobacco access have not achieved their objectives: the rite-of-passage effect and confusing health signalling. These problems may be overcome by the tobacco-free generation measure—ending the legal provision of tobacco to the generations that have not yet commenced consumption. Careful attention to the determinants of efficacy of legislation shows how issues aired in public discussion of the proposal may be addressed. In-principle concerns are allayed by consideration of consistency and proportionality criteria.
The emphasis of this measure on future generations, and its regard for the interests of existing stakeholders, makes it worthy of consideration as a surer path to the ultimate eradication of tobacco supply in jurisdictions where the social climate is conducive. In combination with supporting initiatives, it presents the opportunity finally to consign the tobacco problem to its rightful place in the grimy ashtray of history.
Acknowledgments
It is a pleasure to thank M Assunta, A Berrick, M Saunders and anonymous reviewers for critiques of earlier drafts of this article. Research assistance of S Shatenstein has been invaluable.
Footnotes
Competing interests: None.
Provenance and peer review: Not commissioned; internally peer reviewed.
References
- 1.Frieden TA. Foreword, preventing tobacco use among youth and young adults: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2012 [Google Scholar]
- 2.Sebelius K. Message from the Secretary for Health and Human Services, preventing tobacco use among youth and young adults: a report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2012 [Google Scholar]
- 3.Koh H. Message from the under-secretary for health, preventing tobacco use among youth and young adults: a report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2012 [Google Scholar]
- 4.Khoo D, Chiam Y, Ng P, et al. Phasing-out tobacco: proposal to deny access to tobacco for those born from 2000. Tobacco Control 2010;19:355–60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Summers L. Interview by BBC 7 June, 2012. http://www.bbc.co.uk/news/world-us-canada-18360140 (accessed Mar 2013).
- 6.Tasmania Legislative Council. Hansard: 21 August, 2012 at 3.53pm. http://www.parliament.tas.gov.au/ParliamentSearch/isysquery/a3403013-3861-493d-8b1e-7aca93dc1c7d/6/doc/ (accessed Aug 2012). [Google Scholar]
- 7.Siegel M. Australia mulls further restrictions on cigarette sales. New York Times 22 August, 2012. http://www.nytimes.com/2012/08/23/business/global/23iht-tobacco23.html (accessed Aug 2012).
- 8.Scotsman.com. Scots smoking stats led to professor's idea to ban smoking for anyone born after 2000. The Scotsman 7 September, 2012. http://www.scotsman.com/news/health/scots-smoking-stats-led-to-professor-s-idea-to-bansmoking-for-anyone-born-after-2000-1-2513188 (accessed Aug 2012).
- 9.Daynard R. Stubbing our cigarettes for good. New York Times 3 March, 2013.http://www.nytimes.com/2013/03/04/opinion/two-paths-to-the-gradual-abolition-of-smoking.html (accessed Mar 2013). [Google Scholar]
- 10.Jarvik ME. The major evidence for nicotine's addictiveness. Psychopharmacology 1995;117:18–20 [Google Scholar]
- 11.Tobacco Advisory Group of the Royal College of Physicians Nicotine addiction in Britain. London: Royal College of Physicians, 2000 [Google Scholar]
- 12.Evolution of the Tobacco Industry Positions on Addiction to Nicotine: A report prepared for the Tobacco Free Initiative, World Health Organization. WHO Tobacco Control Papers, Univ. Calif., San Francisco, 2008.
- 13. Lawson H. One Hundred and Three. In: A Fantasy of Man: Henry Lawson Complete Works 1901–1922 (ed. Cronin L). Sydney: Lansdowne 1984:371–4. [Google Scholar]
- 14.Stead LF, Lancaster T. A systematic review of interventions for preventing tobacco sales to minors. Tobacco Control 2000;9:169–76 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Crawford MA, Balch GI, Mermelstein R, et al. Responses to tobacco control policies among youth. Tobacco Control 2002;11:14–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Blanke DD, da Costa e Silva V. Tobacco Control Legislation: an introductory guide. 2nd edn Geneva: World Health Organization, 2004 [Google Scholar]
- 17.Berrick AJ. Determinants of adherence to a statute—a typology. Submitted for publication, 2013
- 18.Oh DL, Heck JE, Dresler C, et al. Determinants of smoking initiation among women in five European countries: a crosssectional survey. BMC Public Health 2010;10:74–84 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chang H-Y, Wu W-C, Cheng JY, et al. The incidence of experimental smoking in school children: an 8-year follow-up of the Child and Adolescent Behaviors in Long-term Evolution (CABLE) study. BMC Public Health 2011;11:844–52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. doi: 10.1080/1081073049050413. Evans WD, Price S, Blahut S, et al. Social imagery, tobacco independence, and the TruthSM campaign. J Health Comm 2004;9:425–41. [DOI] [PubMed] [Google Scholar]
- 21. Cpy5. 18 Oct 1977. Brown & Williamson. http://legacy.library.ucsf.edu/tid/jyj51f00 (accessed 4 Apr 2013)
- 22.Green HD, Horta M, de la Haye K, et al. Peer influence and selection processes in adolescent smoking behavior: a comparative study. Nicotine Tob Res 2013;15:534–41 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Forster J, Chen V, Blaine T, et al. Social exchange of cigarettes by youth. Tob Control 2003;12:148–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. The Tobacco Institute of Hong Kong Media Release (May 29, 1990) Bates 2501109205.
- 25.Wakefield M, McLeod K, Perry CL. “Stay away from them until you're old enough to make a decision”: tobacco company testimony about youth smoking initiation. Tob Control 2006;15:iv44–53 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Clark PI, Factors associated with tobacco sales to minors: lessons learned from the FDA compliance checks. J Am Med Assoc 2000;284:729–34 [DOI] [PubMed] [Google Scholar]
- 27.Imperial Tobacco New Zealand spokesperson Brendan Walker (May 24, 2012) http://www.nzherald.co.nz/business/news/article.cfm?c_id=3&objectid=10808246 (accessed Mar 2013).
- 28.WHO Framework Convention on Tobacco Control. Geneva: World Health Organization 2005. 29 Tobacco Institute of Australia Limited. Submission on the advertising of tobacco products presented to the West Australian Committee on the monitoring of tobacco advertising. n.d. Brown & Williamson. http://legacy.library.ucsf.edu/tid/cyc30f00 (accessed Mar 2013). [Google Scholar]
- 29.Tobacco Institute of Australia Limited. Submission on the advertising of tobacco products presented to the West Australian Committee on the monitoring of tobacco advertising. n.d. Brown & Williamson. http://legacy.library.ucsf.edu/tid/cyc30f00
- 30.Woody GE, Cottler LB, Cacciola J. Severity of dependence: data from the DSM-IV field trials. Addiction 1993;88:1573–9 [DOI] [PubMed] [Google Scholar]
- 31.United Nations International Drug Control Programme (UNDCP) World Drug Report. Oxford: Oxford University Press, 1997. Regulation–Legalization Debate pp.198–9 [Google Scholar]
- 32.Nutt D, King LA, Saulsbury W, et al. Development of a rational scale to assess the harm of drugs of potential misuse. Lancet 2007;369:1047–53 [DOI] [PubMed] [Google Scholar]
- 33.Intergovernmental Committee on Drugs National Tobacco Strategy 2012–2018: Draft for Consultation. Canberra: Department of Health and Ageing, 2012 [Google Scholar]
- 34.Gruber J, Zinman J. Youth smoking in the United States: evidence and implications. In: Gruber J. Risky behavior among youths: an economic analysis. Chicago: Univ Chicago Press, 2001: 69–120 [Google Scholar]
- 35.Gruber J. Private communication 2013.
- 36.Schelling TC. Micromotives and Macrobehavior 1978.
- 37.Sunstein CR. Social norms and social roles. Columbia Law Review 1996;96:903–68 [Google Scholar]
- 38.http://www.tobaccofreegeneration.info
- 39.Posner EA. Law, economics and efficient norms. Univ PA Law Rev 1996;144:1697–744 [Google Scholar]
- 40.Tobacco Retailers Alliance. The future of tobacco policy in Scotland. http://www.tobaccoretailersalliance.org.uk/index.php?option=com_content&view=article&id=75:the-future-of-tobacco-policy-in-scotland&catid=18:blog (accessed Mar 2013).
- 41.Nolan JM, Schultz PW, Cialdini RB, et al. Normative social influence is underdetected. Pers Soc Psychol Bull 2008;34:913–23 [DOI] [PubMed] [Google Scholar]
- 42.Cialdini RB, Demaine L, Sagarin BJ, et al. Managing social norms for persuasive impact. Soc Influence 2006;1:3–15 [Google Scholar]
- 43.O'Byrne M. Fewer tobacco retailers selling to children. Ministry of Health press release, Hobart Tasmania: 24 December 2010
- 44. Jason LA, Ji PY, Anes MD, et al. Active enforcement of cigarette control laws in the prevention of cigarette sales to minors. J Amer Med Assoc 1991;266:3159–61. [PubMed] [Google Scholar]
- 45.Altman DG, Foster V, Rasenick-Douss L, et al. Reducing the illegal sale of cigarettes to minors. J Am Med Assoc 1989;261:80–3 [PubMed] [Google Scholar]
- 46.DiFranza JR. Which interventions against the sale of tobacco to minors can be expected to reduce smoking? Tob Control 2012;21:436–42 [DOI] [PubMed] [Google Scholar]
- 47.Woodward AC, Henley PP, Wilson DJ. Banning tobacco sales in Massachusetts’ pharmacies. J Am Coll Nutr 2012;31:145–8 [DOI] [PubMed] [Google Scholar]
- 48.Levinson AH, Hendershott S, Byers TE. The ID effect on youth access to cigarettes. Tob Control 2002;11:296–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Cummings KM, Sciandra E, Pechacek TF, et al. Where teenagers get their cigarettes: a survey of the purchasing habits of 13–16 year olds in 12 US communities. Tob Control 1992;1:264–7 [Google Scholar]
- 50.McAdams RH. The origin, development, and regulation of norms. Mich Law Rev 1997;96:338–433 [Google Scholar]
- 51.Organized Crime and Corruption Reporting Project. Big trouble at big tobacco. 4 November 2011. https://reportingproject.net/troubles_with_big_tobacco/ (accessed Mar 2013).
- 52.Smoking-Cigarettes and Advertising. 00 1975. Brown & Williamson. http://legacy.library.ucsf.edu/tid/ubh04f00 (accessed 4 Apr 2013).
- 53.Pei N. Yale in denial. Yale Daily News 2012; September 28. http://www.yaledailynews.com/news/2012/sep/28/pei-yale-in-denial/ (accessed Mar 2013).
- 54.Arnett JJ. Sensation seeking, aggressiveness, and adolescent reckless behavior. Pers Individual Differences 1996;20:693–702 [Google Scholar]
- 55.Midzuno, K. Japan's crusade on the use of opium in Formosa. North Am Rev 1909;189:274–9 [Google Scholar]
- 56.Willoughby WW. Opium As an International Problem. Johns Hopkins,1925. p.118 [Google Scholar]
- 57.Report of the Prohibition Commission. Ceylon: 1957
- 58.Chapman S. The case for a smoker's license. PLoS Med 2012. 9:e1001342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Brown TC, Gregory R. Why the WTA-WTP disparity matters. Ecol Econ 1999;28:323–335 [Google Scholar]
- 60.Horowitz JK, McConnell A review of WTA/WTP Studies. J Environ Econ Manag 2002;44:426–47 [Google Scholar]
- 61.Kahneman D, Tversky A. Choices, values, and frames. Am Psychol 1984;39:341–50 [Google Scholar]
- 62.Enoch D. Once you start using slippery slope arguments, you're on a very slippery slope. Oxf J Leg Stud 2001;21:629–47 [Google Scholar]
- 63.Kessler D. Nicotine addiction: a pediatric disease. J Pediatrics 1997; 130:518–24 [DOI] [PubMed] [Google Scholar]
- 64.Schane RE, Glantz SA. Education on the dangers of passive smoking: a cessation strategy past due. Circulation 2008;118:1521–3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Singer P. Should we ban cigarettes? November 11, 2011. http://www.project-syndicate.org/commentary/should-we-ban-cigarettes- (accessed Mar 2013).
- 66.Nuffield Council on Bioethics. Public Health: Policy process and practice. London: Nuffield Council on Bioethics, 2007. http://www.nuffieldbioethics.org/public-health/public-health-policy-process-and-practice (accessed Mar 2013). [Google Scholar]
- 67.Walton M, Mengwasser E. An ethical evaluation of evidence: a stewardship approach to public health policy. Public Health Ethics 2012;5:16–21 [Google Scholar]
- 68.Levi M. Consent, dissent and patriotism. Cambridge: Cambridge University Press, 1997 [Google Scholar]
- 69.Kirby T. Australia considers string of preventive health measures. Lancet 2009;374:963. [DOI] [PubMed] [Google Scholar]