

Abstract
Background:
Cancer is one of the most common causes of mortality and morbidity today, with more than 10 million new cases and more than 6 million deaths each year worldwide. Globally Oral Cancer is the sixth most common cause of cancer related death. India accounts for 86% of the world's oral cancer cases. Often it proceeds by pre cancerous conditions and lesions. In search for biological markers with diagnostic value, we investigated serum glycoconjugates like protein bound hexoses, fucose and sialic acid in these diseases.
Materials and Methods:
For this Study 27 newly diagnosed Oral leukoplakia, 27 OSMF and 26 Oral Cancer patients, 40 healthy controls who are non tobacco users and 40 healthy controls who are tobacco users were selected. In all these groups we estimated serum glycoconjugates.
Results:
We observed no difference in serum glycoconjugates levels between tobacco and non tobacco controls (P > 0.05), but very high levels in oral cancer, Leukoplakia and oral sub mucous fibrosis (OSMF) patients (P < 0.001) when compared to control groups. Fucose levels were significant (P < 0.05) of all the glycoconjugates between OSMF and Leukoplakia.
Conclusion:
The serum glycoconjugates whose levels were very high in OSMF, Leukoplakia and Oral Cancer, do have a significant diagnostic and prognostic value in these diseases.
Keywords: Fucose and sialic acid, leukoplakia, oral sub mucous fibrosis, oral cancer, protein bound hexoses
INTRODUCTION
Cancer is one of the most common causes of mortality and morbidity today, with more than 10 million new cases and more than 6 million deaths each year worldwide.[1] It is projected that by 2020 there will be every year 15 million new cases and 10 million cancer deaths. It is estimated that around 43% of cancer deaths are due to tobacco use, unhealthy diets, alcohol consumption and infections.[2] Globally Oral Cancer is the sixth most common cause of cancer related death.[3] India accounts for 86% of the world's oral cancer cases, says the study conducted by the National Institute of Public Health in February 2011. Ninety percent of these cases are due to chewing tobacco, unlike in the west where smoking is the main reason. Oral cancer accounts for approximately 30-40% of all cancers in India.
Many properties of mammalian cells are expressed at, or mediated through the cell surface. Immense increase in knowledge of altered characteristic of malignant cells has shown that, altered cell surface is the hallmark of malignant cells.[4,5] Cell surface glycosylation changes are associated with diverse types of neoplastic transformation. Glycoproteins and glycolipids are the major constituents of cell membrane. Glycoproteins are usually defined as protein-carbohydrate complexes in which oligosaccharides and or polysaccharides are joined by covalent linkage to specific amino acids of proteins. The carbohydrate portion contains amino sugars (glucosamine, galactosamine and sialic acid) and hexoses (galactose, mannose) or fucose. These glycoconjugates especially the terminal epitopes of Glycoproteins are thought to play important role in cell-cell interactions, development of cell adhesion, malignant transformation and metastasis.[6–8] Sialic acid is thought to be important in determining surface properties of cells and has been implicated in cellular invasiveness, adhesiveness and immunogenicity.[9] Fucosylation of Glycoproteins at terminal ends is one of the most important features that mediate several specific biological functions. It has been documented that tumor cells modulate their surface by increasing fucosylation levels to escape recognition, thus contribute to decreased adhesion and uncontrolled tumor growth.[10] High serum glycoconjugates levels have been reported in many cancers including head neck and oral cancers indicating their usefulness in diagnosis and monitoring therapy.[11–15] Oral Cancer (OC) is preceded in many cases by pre cancerous conditions (PC) like OSMF and pre cancerous lesions (PL) like Leukoplakia.[16] The malignant transformation rate of OSMF is found to be 7.6%[17] and for leukoplakia it is 1 to 17% with highest transformation rate for the lesions on floor of the mouth, soft palate and tongue.[18] In search for biological markers, which can detect changes in oral tissue even at asymptomatic stage would be beneficial to monitor patients with high risk of malignancy, we investigated the serum levels of these glycoconjugates in PC, PL and OC to emphasize their diagnostic role in these diseases.
MATERIALS AND METHODS
This study was approved by Institutional Ethical Committee, and written consent was taken from every participant. The study comprises 5 groups. Group-I: 40 age and sex matched healthy individuals who are non tobacco and areca quid consumers (non tobacco control). Group-II: 40 age and sex matched healthy individuals who are tobacco and areca quid consumers (tobacco control), who were not suffering from any systemic illness. Group-III comprises 27 newly diagnosed both male and f emale Oral Leukoplakia patients, Group-IV: 27 OSMF patients and Group-V: 26 Oral Cancer patients of age between 23 to 50 years who have not received any previous treatment, and or on any antioxidant therapy and were conformed after the detailed case history and histopathological confirmation. Blood samples were collected from all the subjects and centrifuged at 4°C, serum was stored at -20°C for quantitative estimation of glycoconjugates.
Assays
Estimation of serum fucose levels
Serum fucose was estimated using Dische and Shettles method.[19] Briefly serum proteins were precipitated by 95% ethanol, and the pellet obtained from centrifugation was dissolved in 0.2 N NaOH. This was reacted with H2So4 followed by boiling to release fucose from proteins. The released fucose was reacted with cystein-HCl reagent, to form yellow colored chromospheres, whose intensity was read at 396 and 430 nm.
Estimation of protein bound hexoses
Serum protein bound hexoses were estimated by method adopted by Weimer and Moshin.[20] In brief serum proteins were precipitated by 95% ethanol and the pellet obtained from centrifugation was dissolved in 0.1 N NaOH. The hexoses of dissolved proteins were reacted with Orcinol- H2So4 reagent to form red colored chromospheres, whose intensity was read at 540 nm.
Estimation of serum total sialic acid
Serum sialic acid was estimated by slight modified method of Ayala et al.[21] In brief the protein bound sialic acid was released by treating serum with 5% TCA followed by boiling. The released sialic acid obtained by filtration with filter paper was treated with Diphenylamine reagent to get pinkish red colored chromospheres, whose intensity was read at 530 nm.
Statistics
All the results were expressed as mean + SD. Student t-test was used to assess statistical significance in serum glycoconjugates between non tobacco control, tobacco control, OSMF Leukoplakia and Oral Cancer. P value < 0.05 was considered significant and P value < 0.001 were considered as highly significant. One-way analysis of variance (ANOVA) was applied to study the statistical significance of the difference in the mean values of above said parameters in precancerous conditions, lesions and oral cancer patients.
RESULTS
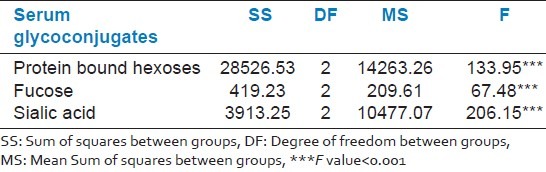
Table 1 shows the levels of serum glycoconjugates in all the five groups and we observed statistically highly significant levels in OSMF, Leukoplakia and OC when compared with control (P < 0.001) and shows no statistical difference in these serum glycoconjugates levels between non tobacco control and tobacco control (P > 0.05). Table 2 shows the mean difference in serum levels of above said glycoconjugates between OSMF, Leukoplakia and OC and we observed significant difference in them (P < 0.001).
Table 1.
The serum glycoconjugates levels in non tobacco control, tobacco consuming control, OSMF, leukoplakia and oral cancer
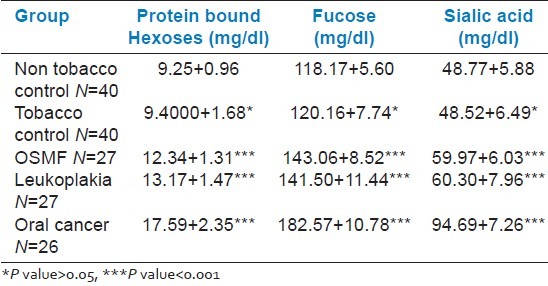
Table 2.
One-way ANOVA of serum glycoconjugates levels between OSMF, leukoplakia and oral cancer
DISCUSSION
Alterations in the cell surface glycosylation during transformation of a normal cell to a malignant cell have been suggested for many years. Measurements of protein bound carbohydrates have been used as an index to glycoprotein levels that may be valuable in establishing diagnosis, staging of disease, detecting metastasis, identifying patients at high risk for recurrence and evaluating therapeutic response. Many researchers[22–25] observed increased serum glycoproteins like fucose, sialic acid in different types of malignancies like melanoma, breast cancer, and carcinoma of cervix and brain tumor. The carbohydrate moiety of these glycoproteins can be released into circulation through increased turnover, secretion and or shedding and are considerable interest for their potential diagnostic and prognostic value. In our study we observed no significant difference in serum glycoconjugates levels between non tobacco control and tobacco consuming controls (P > 0.05), suggesting that the glycoconjugates are directly correlated with the disease activity, and they are not affected by dietary habits. The same was observed by Bina et al. in their study[26] indicating no effective role of dietary variation on serum glycoconjugates levels. In this study serum levels of protein bound hexoses were significantly higher in OSMF, Leukoplakia and Oral Cancer (P < 0.01) and was positively correlated with studies done by Neeraj Taneja et al.[27] Of the increasing pattern we observed very high levels in OC followed by leukoplakia and least raise in OSMF. The difference in serum protein bound hexoses between OSMF and Leukoplakia is insignificant (P > 0.05).
In this study we observed a very high serum fucose in OSMF, Leukoplakia and OC, when compared to controls (P < 0.001) as like that was observed by Parwani RN et al.28 in their study. According to Manisha Shah et al.[29] high fucosylation one of the characteristic feature of malignancies is mainly due to increased activity of fucosyl transferase activity in malignant tissue.
At the same time we observed an interesting and significant observation that there was a significant difference in serum fucose levels between OSMF and Leukoplakia, positively indicating the potential malignant transformation rate of leukoplakia in compare to OSMF and effective role of fucosylation and fuco-proteins in malignant transformation of normal cells.
Sialic acid is a major constituent of carbohydrate moiety of cell membrane glycoproteins and glycolipids. In this study we observed significantly higher serum levels of sialic acid in OSMF, Leukoplakia and OC (P < 0.01) and were positively correlated with findings of other studies.[30–32] Neoplasms often have increased concentration of sialic acid on tumor cell surface and sialoglycoproteins are shed or secreted by these cells increasing their concentration in blood. This increase in cancer is might also be due to selective increase in existing specific sialylated sequence or a tumor associated de-nova synthesis of specific sialylated sequence.
CONCLUSION
From this study we conclude that serum glycoconjugates like sialic acid, Fucose and protein bound hexoses can be used as routine markers in diagnosing oral pre malignant conditions, lesions and malignancies. More over in Oral Leukoplakia serum fucose can be better diagnostic and or prognostic marker of all the above glycoconjugates.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.The world health report 2004: Changing history. Geneva: WHO; 2004. World Health Organization. [Google Scholar]
- 2.Lopez AD, Mathers CD, Ezzati H, Jamison DT, Murray CJL. Global burden of disease and risk factors. New York: Oxford University Press; 2006. pp. 45–240. [Google Scholar]
- 3.Rizzolo D, Hanifin C, Chinado TA. Oral cancer. How to find this hidden killer in two minutes. JAAPA. 2007;20:42–7. doi: 10.1097/01720610-200710000-00021. [DOI] [PubMed] [Google Scholar]
- 4.Raval GN, Parekh LH, Patel DD, Jha FP, Sainger RN, Patel PS. Clinical usefulness of alterations in sialic acid.Sialyl transferase and sialoproteins in breast cancer. Ind J Clin Biochem. 2004;19:60–71. doi: 10.1007/BF02894259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rao VR, Krishnamoorthy L, Kumaraswamy SV, Ramaswamy G. Circulating levels in serum total sialic acid, lipid associated sialic acid and fucose in precancerous lesion and cancer of oral cavity. Cancer Detect Rev. 1998;22:237–40. doi: 10.1046/j.1525-1500.1998.0oa04.x. [DOI] [PubMed] [Google Scholar]
- 6.Yogeeswaran G. Cell surface glycolipids of the tumor cell surface. Biochem Biophys Acta. 1984;738:237–49. [Google Scholar]
- 7.Hakomori S, Barrant A. glycosylation in tumors and tumor associated carbohydrate antigens. Adv Cancer Res. 1989;52:257–331. doi: 10.1016/s0065-230x(08)60215-8. [DOI] [PubMed] [Google Scholar]
- 8.Warren L, Buck CA, Tuszynski GP. Glycopeptide changes and malignant transformation.A possible role of carbohydrate in malignant behaviors. Biochem Biophys Acta. 1978;516:97–127. doi: 10.1016/0304-419x(78)90005-7. [DOI] [PubMed] [Google Scholar]
- 9.Schirrmacher V, Altevogt P, Fogel M, Dennis J, Walker CA, Barz D, et al. Importance of cell surface carbohydrates in cancer cell adhesion, invasion and metastasis. Does sialic acid direct metastatic behavior? Invasion and Metastasis. 1982;2:313–60. [Google Scholar]
- 10.Mac Dougall SL, Schwarting GA, Parkinson D, Sulliman AK. Increased fucosylation of glycolipids in a human leukemia cell line (k562-clone I) with decreased sensitivity to NK-mediated lysis. Immunology. 1987;62:75–80. [PMC free article] [PubMed] [Google Scholar]
- 11.Joshi M, Patil R. Estimation and comparative study of serum total sialic acid levels as tumor markers in oral cancer and pre cancer. J Cancer Res Ther. 2010;6:263–6. doi: 10.4103/0973-1482.73339. [DOI] [PubMed] [Google Scholar]
- 12.Kadam CY, Katkam RV, Suryakar AN, Kashinath MK, Dipali PK, et al. Biochemical markers in oral cancer. Biomed Res. 2011;22:76–80. [Google Scholar]
- 13.Teneja N, Bathi RJ, Parveen S, Bhat K. Serum glycoproteins as prognosticator in oral cancer patients-A follow up study. Int J Oral Med Sci. 2009;8:74–82. [Google Scholar]
- 14.Wang JJ, Cao EH. Rapid kinetic rate assay of the serum α-L-fucosidase in patients with hepatocellular carcinoma by using a novel substrate. Clin Chim Acta. 2004;347:103–9. doi: 10.1016/j.cccn.2004.04.007. [DOI] [PubMed] [Google Scholar]
- 15.Deugnier Y. Serum α-fucosidase: A new marker for the diagnosis of primary hepatic carcinoma. Hepatol. 1984;4:889–92. doi: 10.1002/hep.1840040516. [DOI] [PubMed] [Google Scholar]
- 16.Mehta FS, Pindborg JJ, Gupta PC, Daftary DK. Epidemiologic and histologic study of oral cancer and leukoplakia among 50,915 villagers in India. Cancer. 1969;24:832–49. doi: 10.1002/1097-0142(196910)24:4<832::aid-cncr2820240427>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 17.Pillai KG, Burde KN. Increased copper levels in oral tissue of patients with sub mucous fibrosis and who chew areca nut products. West Indian Med J. 2005;54:270–1. doi: 10.1590/s0043-31442005000400014. [DOI] [PubMed] [Google Scholar]
- 18.Zhang L, Cheung Jr, Lam WL. Increased genetic damage in oral leukoplakia from high risk sites.Potential impact on staging and clinical malignant. Cancer. 2001;91:2148–55. doi: 10.1002/1097-0142(20010601)91:11<2148::aid-cncr1243>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 19.Dische Z, Shettles LB. A specific color reaction of methyl pentoses and a spectrophotometric micromethod for their determination. J Biol Chem. 1948;175:595–603. [PubMed] [Google Scholar]
- 20.Weimer HE, Moshin JR. Serum glycoprotein concentrations in experimental tuberculosis of guinea pigs. Am Rev Tuberc. 1952;68:594–602. doi: 10.1164/art.1953.68.4.594. [DOI] [PubMed] [Google Scholar]
- 21.Ayala W, Moore LV, Hess EL. The purple color reaction given by diphenylamine reagent.I. with normal and rheumatic fever sera. J Clin Invest. 1951;30:781–5. doi: 10.1172/JCI102492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Silver HK, Karim KA, Selinas FA. Relationship of total serum sialic acid to sialyl glycoprotein, acute phase reactants in malignant melanoma. Br J Cancer. 1980;41:745–50. doi: 10.1038/bjc.1980.136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ryan AH. Serum sialic acid and CEA concentrations in human breast cancer. Br J Cancer. 1980;41:587–92. doi: 10.1038/bjc.1980.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bandlish U, Prabhakar BR, Virmani U. Serum fucose levels in gynecological disorders including carcinoma of cervix. J Indian Med Assoc. 1991;89:250–1. [PubMed] [Google Scholar]
- 25.Manjula S, Monteiro F, Rao Aroor A, Rao S, Annaswamy R, Rao A. Assessment of serum L-Fucose in brain tumor cases. Ann Indian Acad Neurol. 2010;13:33–6. doi: 10.4103/0972-2327.61274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Baxi BR, Patel PS, Adhvaryu SG, Dayal PK. Usefulness of serum glycoconjugates in precancerous and cancerous diseases of oral cavity. Cancer. 1991;67:135–40. doi: 10.1002/1097-0142(19910101)67:1<135::aid-cncr2820670124>3.0.co;2-6. [DOI] [PubMed] [Google Scholar]
- 27.Taneja N, Bathi RJ, Parveen S, Bhat K. Serum glycoproteins as prognosticator in Oral Cancer Patients-A follow up study. Int J Oral Med Sci. 2009;8:74–82. [Google Scholar]
- 28.Parwani RN, Parwani SR. Quantitative evaluation of serum fucose in oral squamous cell carcinoma patients. J Can Res Ther. 2011;7:143–7. doi: 10.4103/0973-1482.82928. [DOI] [PubMed] [Google Scholar]
- 29.Shah M, Telang S, Raval G, Shah P, Patel PS. Serum fucosylation changes in oral cancer and oral precancerous conditions. Cancer. 2008;113:336–46. doi: 10.1002/cncr.23556. [DOI] [PubMed] [Google Scholar]
- 30.Chitra CS, Devi S. Effect of Vitamin E on protein bound carbohydrate complexes in radiation treated oral squamous cell carcinoma patients. Indian J Clin Biochem. 2008;23:92–4. doi: 10.1007/s12291-008-0022-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Silva CR, Vasudevan DM, Prabhu KS. Evaluation of serum glycoproteins in oral carcinoma. Indian J Clin Biochem. 2001;16:113–5. doi: 10.1007/BF02867579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kimura Y, Fujieda S, Takabayashi T, Tanaka T, Sugimoto C, Saito H. Conventional tumor markers and prognostic indicators in patients with head and neck squamous cell carcinoma. Cancer Lett. 2000;155:163–8. doi: 10.1016/s0304-3835(00)00423-7. [DOI] [PubMed] [Google Scholar]