

Abstract
Objective:
To describe profile of births occurring in teaching institution on selected parameters.
Materials and Methods:
Considering feasibility, four months were systematically chosen for two-year time frame over a decade to gather selected information of consecutive singleton intramural births from log books of labor room on structured pro-forma. Data management was done using software package and analysis carried out by computing descriptive statistics (%) and Chi-square test.
Results:
It was observed that there were a total of 2862 and 1527 singleton births (>28 weeks) recorded for the sampled time-frame of 2009 and 1999 respectively reflecting increased quantum of institutional deliveries over time-span. Out of 2862 births, monthly distribution was 21.8% (Jan), 20% (Apr), 37.2% (July) and 21.1% (Oct) with similar picture for 1999. The birth according to 8-hourly timeframe was computed to be 31.6% (12 am-8 am), 34.3% (8 am-4 pm) and 34.0% (4 pm to 12 am) for 2009 while it was 28.6%, 38.6% and 32.8% for 1999 (P < 0.05). Births took place through-out seven days of week; however, Sunday (12.0%) was the least popular day while Thursday (18.7%) recorded maximum proportion of births during 2009. Slightly higher proportion of pre-term births were recorded during 2009 (21.76%) in comparison to 1999 (18.53%). The caesarian section rose to 26.1% from 20.2% (P < 0.05) while M:F ratio at birth was 1.28 and 1.17 with similar proportion (92.3%; 93.0%) of newborns being discharged live during 2009 and 1999 respectively.
Conclusion:
It provides snapshots of birth occurring in a teaching hospital and within study constraints finding could be utilized for improving quality of care, health communication, better utilization of human resource and logistics.
Keywords: Birth, caesarian section, day, delivery, institution, month, outcome, perinatal mortality, record, retrospective, sex, time
INTRODUCTION
Birth has been described vividly with contrasting critiques and images by artist, anthropologist, demographer, sociologist and medical fraternity since time immemorial. Yet, topic offers freshness and depth, invites attention and attracts researcher to unfold different dimensions associated with the phenomenon. The path to discovery still continues. With this background, a cross-sectional record based retrospective study was undertaken to describe profile of births occurring in a medical college hospital of northern India on selected parameters.
MATERIALS AND METHODS
The study was conducted in one of the publically funded teaching institution of northern India which provides round the clock specialist's tertiary care services to patients largely belonging to lower/middle socio-economic strata of both rural and urban setting. University of Health Sciences, Rohtak (Haryana) has a current sanctioned seats of 200 (MBBS), 75 (Nursing) and 75 (Pharmacy) at undergraduate level, in addition to post-graduation and other paramedical courses. Currently, it caters to an avg. daily OPD attendance of more than 5000 patients and 80,000 annual admissions supported by 1750 in-patient beds.
Considering feasibility and resource constraints (lack of electronic database, skilled manpower for data collection, time etc.) it was envisaged to collect all pertinent information of births (beyond 28 weeks) by systematically selecting months of January, April, July and October for the year 2009. The same procedure was adopted for the year 1999 for comparison purpose. Preventive measures are taken for upkeep of records and assistance of staff was solicited in retrieving old records. Selected information (month, day, time of maternal hospital admission and birth, estimated period of gestation based on last menstrual cycle, type of delivery, sex of newborn, and outcome) of all consecutive singleton intramural births was extracted manually from the log books maintained in the labor room. The data collection was carried out by investigators using structured proforma from Feb to May 2010 after taking permission from authority. Atleast one of the investigators was available as supervisor during both the study time-frame. Nearly 3.1% [88 (2009) and 49 (1999)] case entries were incomplete/illegible, hence excluded from study. Time of day was divided into 3 intervals- 12 midnight to 8 am, 8 am to 4 pm and 4 pm to 12 midnight. Analysis was carried out by calculating proportion (%) and Chi-square test using software statistical package (SPSS ver. 16) and considered significant and reflected in the table at level P < 0.05 to assess change in trend overtime frame.
RESULTS
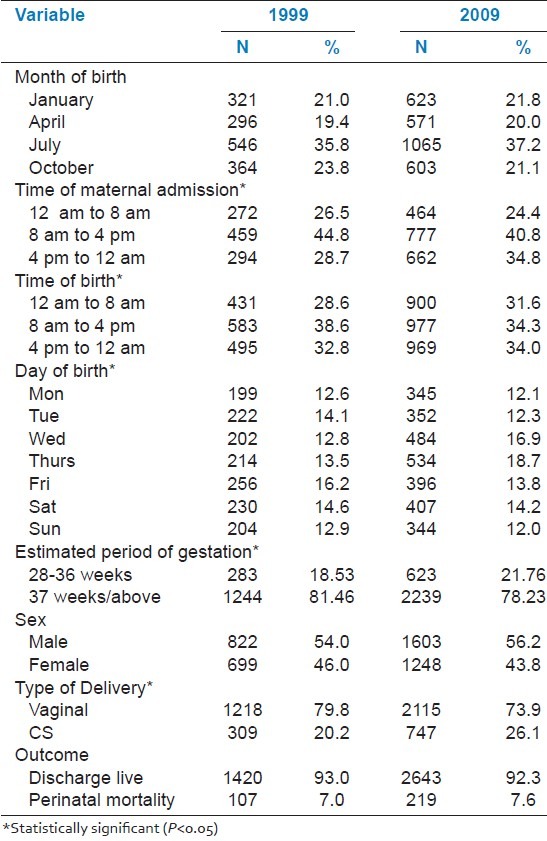
There were a total of 2862 and 1527 singleton births recorded for the sampled time-frame of 2009 and 1999 respectively reflecting increased (46.6%) quantum of institutional deliveries over the period. Out of 2862 births, monthly distribution was 21.8% (Jan), 20% (Apr), 37.2% (July) and 21.1% (Oct) with similar picture for 1999 [Table 1]. Majority of maternal admission was noticed during the time-interval of 8 am-4 pm, 44.8% (1999) and 40.8% (2009) respectively with a significant rise from 28.7% (1999) to 34.8 (2009) for 4 pm-12 am. The birth according to 8-hourly timeframe was computed to be 31.6% (12 am-8 am), 34.3% (8 am-4 pm) and 34.0% (4 pm to 12 am) for 2009 while it was 28.6%, 38.6% and 32.8% for 1999 (P < 0.05). Births took place through-out seven-days of week; however, Friday recorded highest proportion of births (16.2%) in 1999 and Thursday (18.7%) during 2009 (P < 0.05). The male: female ratio at birth was 1.28 (2009) and 1.17 (1999). Similar proportion (92.3%; 93.0%) of newborns was discharged live. The caesarian section (CS) recorded was higher in 2009 (26.1%) in comparison to 1999 (20.2%). The rise was found to be statistically significant (P < 0.5).
Table 1.
Profile of births in a teaching institution according to selected variables
DISCUSSION
A study was undertaken to describe births occurring in a government medical college hospital of northern India on selected parameters, a first of its kind in this region of country. The human beings in contrast to other species reproduce through-out the year but out of four systematically sampled (Jan, Apr, July, Oct) months, it was found out that the proportion of births were similar (19.0% to 23.0%) during all months except July (37.2% and 35.8%) corresponding to colloquial term of ‘birth seasons’ among obstetrician. India is the second most populous (1210 million persons, 2011) country in the world with nearly 25 million births taking place annually. The population control has been one of the greatest challenges with many policy interventions, strategies and measures in vogue since inception of National Family Planning Control program (1952) and current Reproductive Child Health (RCH) program of National Rural Health Mission (NRHM). Still a lot needs to be done in this direction using innovative strategies. Within study limitations as also there was no information on other co-variables, the finding technically indicates that maximum conception occurred during Nov-Dec. Public health implications e.g., family planning activities could be re-organized and specifically targeted during these winter months that may have a higher resultant yield.
Time of maternal admission followed a downward trend from highest during day time (8 am to 4 pm) followed by evening and least in early morning during both study period with variation noted in proportion. With doubling of deliveries in recent years due to improvement of socio-economic conditions, level of education, enhanced advocacy for institutional deliveries in India [34% (DLHS, 1998-99); 47% (DLHS, 2007-08); 60.5% (SRS, 2010)], easy access to communication and free transport facilities under National Rural Health Mission (NRHM), the other aspect of this scenario also points out at rising occupational burden, stress and sleep deprivation amongst health professionals especially if accompanied by staff shortage. It may also point towards poor communication, quality of care including adverse outcome and threat to physical security as large number of birth are taking place outside the working hours of institution which is accompanied by reduced staff strength in comparison to routine day shifts. Recently, electronic surveillance has been installed at this unit to strengthen security.
In a study from Tokyo hospital, proportion of deliveries have been reported for the same 8-hourly period as 38.5% (day), 33.37% (evening) and 28.0% (night) respectively.[1] Similar pattern was noted for 1999 study frame however for 2009 proportion of birth were similar for evening (34%) and night (34%) period. In our study, Sunday (12.0%) and Monday (12.1%) appeared to be least popular day while Thursday (18.7%) recorded maximum births during 2009 while Tuesday has been the most and Sunday the least popular day of all births in USA.[2] This could be suggestive of a evolving phenomenon but larger study sample is required to validate the findings. To the best of our efforts, we could not retrieve any recent study reflecting proportion of births according to time and week days in the national context. Previous studies generally agree that homo sapiens births without medical intervention occur mostly at night as a result of ancient evolutionary adaptive pattern. Various reasons have been suggested to explain the advantage of nocturnal deliveries among diurnal species (lower activity of predators, group protection, better conditions for delivery and higher mother-infant bonding).[3] Contractions most frequently start in the middle of the night with a peak just after midnight.[4] However, it has been suggested that natural adaptation is blurred in modern population because of cultural factors, institutional policies and procedures.
Overall adverse sex ratio is an area of concern in prosperous state of northern India with known female foeticide, infanticide and/or neglect. Globally, there are 105 baby boys to 100 girls at birth under natural circumstances. Sex ratio at birth (SRB) in India should be atleast 950 girls per 1000 boys for sustainability of society.[5] However according to sample registration system (2008-10) sex ratio at birth was 905 (India) and 848 (Haryana) girls per 1000 males. National figure of child (0-6 years) sex ratio accounted for 914 while the corresponding figure for Haryana was 830 (2011 Census)[6] that has improved from previous (Census 2001) figure of 819. The figure for Rohtak (Haryana) was grim with 807 girls/1000 boys. According to Civil Registration System (CRS) with 96% birth registration in the state of Haryana during 2011(total births: 563,556), SRB stood at 833 girls/1000 boys (personal communication). In this study also higher male births were reported (sex ratio being 778 (2009) and 850 (1999) girls to 1000 boys). But the finding was not statistically significant. The female to male recorded a decline in 2009, probably suggesting human intervention. However it has been documented that sample size of birth observations should be more than 100,000 to obtain robust SRB within narrow 95% confidence range[7] while our sample size was very small. As large number of un-booked case directly present to tertiary care hospital for delivery, it may be argued that if the sex of foetus was known during anti-natal period, there were greater chances of male foetus being brought to hospital for delivery.
From a sociological dimension, father of male foetus have a more active lifestyle and considered to have risk taking attributes in comparison to ‘philosophical/lazy’ father of female foetus. This may be one of the reasons for shifting their spouse for delivery in health institution in comparison to comfortable home environment of delivery in rural areas under the supervision of traditional birth attendant (dai). However, exact reason cannot be elucidated. In the neighboring state of Delhi, out of all births, males were 52.3% and female (47.7%)[8] while another study carried out in Delhi hospital also recorded a decline with 865 (2005) and 806 (2009) girls to 1000 boys at birth.[9] National Neo-natal Perinatal Database (NNPD) in India reported 52.9% (male) to 47% (female) at birth.[10]
Surgical interventions during pregnancy are usually performed to ensure safety of the mother and child under conditions of obstetric risk. They are justified under certain circumstances but rise of caesarian section (CS) rate in last three decade has been an area of acute concern, attention and debate across globe. Out of all births occurring in USA, CS rate was 31.8%.[2] In 2001 an estimated 21.4% of all deliveries in England and Wales were by CS, a five-fold increase since 1971.[11] In 1985, WHO had recommended that CS rate could be upto 15% of all deliveries while the most recent (2007-08) survey carried out by the international agency in Asian countries indicated CS rate of 46.2% (China), 35.6% (Vietnam), 34.1% (Thailand), 30.6% (Sri Lanka), 20.3% (Nepal), 19.8% (Japan), 18.8% (Philippines), 17.8% (India) and 14.7% (Cambodia).[12] While Indian literature reported the hospital CS rate of 26.2% in Raipur, 23.2% (Mangalore), 19-35% (Delhi teaching hospitals).[13–15] NNPD (2002-03) reported CS rate of 28.7%. Our study suggests a similar picture with rise of CS rate to 26.1% from 20.2% during last decade.
Teaching hospital attracts high risk patients and usually without antenatal registration as 56.9% mothers were not booked with the institution during antenatal period (2009). Our study revealed 92.3% newborns were discharge-live while NNPD (2002-03) reported 96.5%. Perinatal mortality rate in this study was 76.51 (2009) and 70.07 (1999) while a hospital in West Bengal (98.65) and Mexico reported as 20.5 per 1000 live and still births.[16,17] Stillbirth in India are under-recorded however according to available estimates perinatal mortality rate was 70 per 1000 live and still births.[18] On a corollary, an institutional study from neighboring Pakistan reported slightly higher (9.72%) perinatal mortality.[19]
In 2010, Caughey et al.[20] reported that neonatal outcomes do not differ between the daytime, evening and night time shifts in an institution with anesthesiology and obstetric staff on duty in-house 24 hours per day as also observed in present study. In addition, Bailit et al.[21] have found in their large multicenter study of teaching hospitals in United States that there were no important differences in maternal or neonatal morbidity rates according to work shift after unscheduled cesarean delivery. However, these studies are in sharp contrast to the Gould[22] and Suzuki[1] study which found that neonatal outcomes were worse at night in California and Tokyo respectively. This could be attributed to patient related factors, health care practices or reporting bias. Pre-term births constituted 9.6% (5%-18%) of all birth globally[23], 12.7% (USA)[1] , India (13%) while a hospital study from Lucknow[24] reported 20.3% similar to our findings of 21.76% and 18.53%.
CONCLUSIONS
To conclude, study provides a snapshot of births occurring in a teaching institution of northern India on selected parameters and findings could be utilized for improving quality of care, health communication, better utilization of human resource and logistics.
ACKNOWLEDGMENT
Vice-Chancellor, Director and Staff from Dept. of O.B.G. and Pediatrics, Pt. B.D. Sharma, PGIMS, Rohtak, India.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Suzuki S, Nakai M, Hiraizumi Y, Satomi M. Time of delivery and perinatal outcome. J Nippon Med Sch. 2010;77:277–81. doi: 10.1272/jnms.77.277. [DOI] [PubMed] [Google Scholar]
- 2.National Vital Statistics Reports, USA. Atlanta: CDC; 2010. Births: Final Data for 2007. [PubMed] [Google Scholar]
- 3.Bernis C, Varea C. Hour of birth and birth assistance: From a primate to a medicalized pattern? Am J Hum Biol. 2012;24:14–21. doi: 10.1002/ajhb.21228. [DOI] [PubMed] [Google Scholar]
- 4.Backe BA. Circadian variation in the observed duration of labor: Possible causes and implications. Acta Obstet Gynecol Scand. 1991;70:465–68. doi: 10.3109/00016349109007161. [DOI] [PubMed] [Google Scholar]
- 5.Sharma OP, Haub C. Washington, DC: Population Reference Bureau; 2008. [Last accessed on 2011 Jun 10]. Sex ratio at birth begins to improve in India. Available from: http://www.prb.org/Articles/2008/indiasexratio.aspx . [Google Scholar]
- 6.Directorate of Census Operations, Haryana, Ministry of Home Affairs, Government of India, Chandigarh. 2011. Census 2011, India: Haryana (Provisional) [Google Scholar]
- 7.Visaria PM. Sex ratio at birth in territories with a relatively complete registration. Eugenics Quarterly. 1967. [Last accessed on 2012 Feb 20]. pp. 132–142. Historical trends in the sex ratio at birth. Available from: https://jscholarship.library.jhu.edu/…/1774…/WP90-01_Sex_Ratio.pdf . [DOI] [PubMed]
- 8.Annual report on registration of births and death in Delhi: 2008. Directorate of economics and statistics and office of chief registrar, Delhi. 2009 [Google Scholar]
- 9.Manchanda S, Saikia B, Gupta N, Chowdhary S, Puliyel JM. Sex Ratio at Birth in India, Its Relation to Birth Order, Sex of Previous Children and Use of Indigenous Medicine. PLoS One. 2011;6:e20097. doi: 10.1371/journal.pone.0020097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Report: 2002-03. New Delhi: AIIMS; 2005. National Neonatal-Perinatal Database. [Google Scholar]
- 11.Sur S, Mackenzie IZ. Does discussion of possible scar influence preferred mode of delivery after cesarean section? J Obstet Gynecol. 2005;25:338–41. doi: 10.1080/01443610500119697. [DOI] [PubMed] [Google Scholar]
- 12.Lumbiganon P, Laopaiboon M, Gülmezoglu AM, Souza JP, Taneepanichskul S, Ruyan P, et al. Method of delivery and pregnancy outcomes in Asia: The WHO global survey on maternal and perinatal health 2007-08. Lancet. 2010;375:490–9. doi: 10.1016/S0140-6736(09)61870-5. [DOI] [PubMed] [Google Scholar]
- 13.Singh A, Channawar R. A recent way of evaluating cesarean birth. J Obstet Gynecol India. 2009;59:547–51. [Google Scholar]
- 14.Unnikrishnan B, Rakshith P, Aishwarya A, Nithin K, Rekha T, Prasanna P, et al. Trends and indications for caesarean section in a tertiary care obstetric hospital in coastal south India. Australasian Med J. 2010;12:821–5. [Google Scholar]
- 15.Mukherjee SN. Rising cesarean section rate. J Obstet Gynecol India. 2006;56:298–300. [Google Scholar]
- 16.Bhattacharya S, Mukhopadhyay G, Mistry P, Pati S, Saha S. Stillbirth in a tertiary care referral hospital in north Bengal-A review of causes, risk factors and prevention strategies. Online J Health Allied Sci. 2010;9:1–4. [Google Scholar]
- 17.Hernandez HR, Alcala GL, Castillo MN, Flores SR, Cortes FR, Buenrostro LA. A 35 year period review of the perinatal mortality in a gynecology-obstetric unit. Rev Med Inst Mex Seguro Soc. 2009;47:353–56. [PubMed] [Google Scholar]
- 18.Geneva: WHO; 2006. Neonatal and perinatal mortality: Country, regional and global estimates. [Google Scholar]
- 19.Karejo R, Bhutta S, Noorani KJ, Bhutta ZA. An audit and trends of perinatal mortality at the Jinnah Postgraduate Medical Centre, Karachi. J Pak Med Assoc. 2007;57:168–71. [PubMed] [Google Scholar]
- 20.Caughey AB, Urato AC, Lee KA, Thiet MP, Washington AE, Laros RK., Jr Time of delivery and neonatal morbidity and mortality. Am J Obstet Gynecol. 2008;199:496.e1–5. doi: 10.1016/j.ajog.2008.03.046. [DOI] [PubMed] [Google Scholar]
- 21.Bailit JL, Landon MB, Thom E, Rouse DJ, Spong CY, Varner MW, et al. The MFMU Cesarean registry: Impact of time of day on cesarean complications. Am J Obstet Gynecol. 2006;195:1132–37. doi: 10.1016/j.ajog.2006.06.009. [DOI] [PubMed] [Google Scholar]
- 22.Gould JB, Qin C, Chavez G. Time of birth and the risk of neonatal death. Obstet Gynecol. 2005;106:352–58. doi: 10.1097/01.AOG.0000168627.33566.3c. [DOI] [PubMed] [Google Scholar]
- 23.Beck S, Wojdyla D, Say L, Betran AP, Merialdi M, Requejo JH, et al. The worldwide incidence of preterm birth: A systematic review of maternal mortality and morbidity. Bull World Health Organ. 2010;88:31–38. doi: 10.2471/BLT.08.062554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Uma S, Nisha S, Shikha S. A prospective analysis of etiology and outcome of preterm labor. J Obstet Gynecol India. 2007;57:48–52. [Google Scholar]