

Abstract
Objective
Vitamin D deficiency is common and associated with dyslipidemia. However, it is unclear if oral vitamin D supplementation improves the lipid profile. Therefore, we conducted a randomized, placebo-controlled trial to determine the short-term effects of vitamin D repletion on the lipid profile.
Methods
151 vitamin D deficient (25-hydroxyvitamin D [25(OH)D] <20ng/ml) adults with elevated risk for cardiovascular disease were randomized to receive either 50,000 IU of vitamin D3 weekly for 8 weeks or placebo. The primary outcome was the change in small LDL particle number. Secondary outcomes included changes in other NMR-based and chemical lipid fractions.
Results
Vitamin D failed to improve the lipid profile. Compared to placebo, vitamin D repletion did not change small LDL particle number (mean change +18 nmol/l, 95% confidence interval (CI) [−80 to +116 nmol/L], P = 0.63). There were also no changes in the chemical lipid profile: total cholesterol (+5.8 mg/dl, 95%CI [−1.4 to +13.0 mg/dl], P =0.14); LDL cholesterol (+3.8 mg/dl, 95% CI [−2.5 to +10.2 mg/dl], P = 0.13); HDL cholesterol (+0.4 mg/dl 95% CI [−1.6 to +2.6 mg/dl], P = 0.71); triglycerides (+7.9 mg/dl 95%CI [−6.5 to +22.3 mg/dl]). In the vitamin D repletion group, exploratory multivariate regression analysis demonstrates that changes in LDL cholesterol were positively correlated with changes in serum calcium (P < .001) and inversely with changes in serum PTH (P = .02).
Conclusion
In contrast to the association between low 25(OH)D levels and dyslipidemia, correcting vitamin D deficiency in the short-term does not improve the lipid profile. Repletion of 25(OH)D levels raised serum calcium levels and decreased serum PTH levels. These expected physiologic responses to vitamin D therapy were correlated with a significant increase in LDL cholesterol.
Keywords: Vitamin D, cholesterol, NMR lipids, cardiovascular disease
Introduction
Vitamin D is primarily generated in the skin, in response to direct absorption of UVB radiation. Vitamin D can also be obtained through fortified foods and oral supplements. In the liver, vitamin D is hydroxylated to form 25(OH)D. The serum level of 25(OH)D is the standard criterion for determining whole body vitamin D status. Clinical strata of 25(OH)D levels are defined as: <20 ng/ml (deficient), 20–30 ng/ml (insufficient), >30 ng/ml (sufficient).1, 2 However, the optimal level of 25(OH)D remains to be defined. Indeed, a recent report from the Institute of Medicine concluded that higher 25(OH)D levels are “not consistently associated with greater benefit” and that levels ≥20 ng/ml may be sufficient.3
The classical actions of vitamin D influence mineral metabolism: suppressing parathyroid hormone (PTH) production and increasing gut calcium absorption.4, 5 In addition, vitamin D has pleiotropic actions, and vitamin D signaling is operational in many tissues, including the cardiovascular system.6, 7 Epidemiologic studies have shown an association between 25(OH)D deficiency and worse cardiovascular health.8–10 However, whether 25(OH)D is a mere biomarker of health or if 25(OH)D deficiency has a causal role in disease remains unclear. This distinction is especially important when deciding whether or not to target low 25(OH)D levels for repletion.
Blood cholesterol levels are strong predictors of cardiovascular risk.11 Elevated low density lipoprotein (LDL) cholesterol and decreased high density lipoprotein (HDL) cholesterol levels are independent risk factors for adverse cardiovascular events. LDL cholesterol levels are typically not measured directly, but rather calculated from the Friedewald equation and reflect cholesterol that is neither HDL cholesterol nor very low density lipoprotein (VLDL) cholesterol. An alternate way of measuring LDL is through NMR lipoprotein analysis. In some populations, the concentration of small, dense LDL particles can add to the prognostic value of the standard, chemical lipid profile.12
While there is epidemiologic evidence associating high 25(OH)D levels with a healthier lipid profile, there are no randomized placebo-controlled trials that have tested the effect of correcting vitamin D deficiency on the lipid profile.13 We previously conducted an analysis of a large, national, community-based laboratory database to infer how changes in 25(OH)D levels may affect the lipid profile.14 We established strong cross-sectional associations between higher 25(OH)D levels and lower total cholesterol, lower LDL cholesterol, higher HDL cholesterol and lower triglycerides. However, longitudinal analysis showed that increasing 25(OH)D levels from the deficient to sufficient range had a neutral effect on the lipid profile: increased total and HDL cholesterol, but no change in LDL cholesterol and triglycerides. While we could not determine the precise source of repletion, >80% of the increase in 25(OH)D levels was in the form of 25(OH)D2, and thus exogenous. We have extended these findings by performing, a randomized, double-blind, placebo-controlled trial to determine the short-term effect of vitamin D3 repletion on the lipid profile.
Methods
Subjects
Men and women between the ages of 18–85 were recruited and underwent a screening visit, at which non-fasting lipid profiles, 25(OH)D, high sensitivity C-reactive protein (hsCRP), serum creatinine, and glucose values were measured. A medical history, including current medications and tobacco use, as well as height and weight measurements were also performed. Estimated glomerular filtration rate (eGFR) was calculated using the 4-variable modification of diet in renal disease (MDRD) equation.15 Inclusion criteria were 25(OH)D level ≤ 20ng/ml and at least one of the following cardiovascular risk factors: BMI >30 kg/m2, HDL < 40 mg/dl for men or <50 mg/dl for women, hsCRP >2 mg/L, eGFR 30–59 ml/min/m2, a history of coronary artery disease, diabetes mellitus, or a 10-year Framingham risk score >10%. We excluded subjects who were taking > 400 IU of ergocalciferol or cholecalciferol, or any dose of activated vitamin D (1,25-dihydroxyvitamin D or its analogues) within 1 month, as well as subjects with triglycerides > 400 mg/dl, serum calcium > 10.5 mg/dl, serum phosphorus > 5.5 mg/dl, a change in any lipid therapy within 1 month, or an eGFR <30 ml/min/m2. All visits took place at the Rockefeller University Hospital (RUH). The research protocol was approved by Rockefeller University’s Institutional Review Board. This study was listed on ClinicalTrials.gov (Identifier NCT01008384).
Study Visits and Intervention
Subjects were required to fast for 8 hours prior to study visits. At the first study visit, a medical history was taken and subjects underwent venipuncture to determine 25(OH)D, calcium, PTH, lipid and hsCRP levels. After blood was drawn subjects ingested the first dose of study drug under direct observation and were given a study diary to record days/times of study drug doses. The study drug was either vitamin D3 10000 units or placebo (The BTR Group, Pittsfield, IL). Subjects were provided with an 8-week supply of medication and were instructed to take 5 pills each Monday, without specifying a time of day or in relation to meals. After 1 week, subjects were contacted by phone to determine if any adverse events had occurred. Subjects returned to RUH 4 weeks after the first study visit and underwent venipuncture to determine 25(OH)D, calcium, phosphorus, PTH and lipid levels. Interim compliance was assessed through pill counts and review of the study diary. The final study visit took place 8 weeks after the first study visit, where 25(OH)D, calcium, phosphorus, PTH, lipid and hsCRP levels were measured and pill counts and study diaries were reviewed.
Randomization
Eligible participants were assigned to the two study groups such that for every 6 subjects, 3 were randomly assigned to vitamin D repletion and the other 3 were assigned to placebo. Thus, subjects were grouped in blocks of 6 with random 1:1 allocation. Randomization and intervention assignment was performed by the RUH pharmacist. Study personnel remained blinded to subject allocation until results for the endpoints were available and entered into a composite database for analysis.
Endpoints
The primary endpoint was a change in small LDL particle number, determined by NMR lipid profiling (Liposcience, Raleigh, NC). Pilot studies (n = 22) conducted by our group showed that vitamin D repletion raised small LDL particle number by 13% (P = .04), whereas LDL cholesterol levels only increased by 5.8% (P = NS). Therefore, we chose the change in small LDL particle number as the primary endpoint. Based on the pilot data for this metric, we estimated a sample size of 150 subjects to achieve a power of 80% to demonstrate a difference in the primary endpoint between the groups with a two-tailed α< .05.
NMR lipid profiles were determined after all subjects had completed the study. Secondary endpoints included changes in other NMR lipid parameters, the standard lipid profile and hsCRP levels. Aside from the NMR-based measurements, all testing was performed by the Memorial Sloan Kettering Cancer Center clinical laboratory concurrent with study visits. 25(OH)D levels were determined using the Diasorin LIASON automated chemiluminescent immunoassay. Lipid profiles were measured using an enzyme-based Siemens platform, where LDL was calculated in accordance with the Friedewald equation.16
Statistical Analysis
Comparisons between the vitamin D repletion and placebo groups were made using the Mann-Whitney U test. Comparisons for within group changes were made using paired Student’s t-tests. Correlations were assessed by calculating Pearson correlation coefficients. Multivariate analysis was performed using stepwise linear regression models using the following inputs: [Baseline] age, 25(OH)D, calcium, PTH, LDL and HDL cholesterol, triglycerides, phosphorus, hsCRP, glucose [Response] Δ25(OH)D, ΔHDL, Δtriglycerides, Δcalcium, ΔPTH, Δphosphorus, ΔhsCRP, Δglucose. χ-square analysis was used for non-continuous variables. P-values < 0.05 were considered to be significant, except for assessing univariate correlation coefficients. For these, the Bonferroni correction was applied for testing 7 parameters associated with ΔLDL cholesterol, with a resultant significance threshold of P <.007. For the 2 parameters associated with the change in LDL particle number, a significance threshold of < .025 was used. Statistical analyses were conducted using Tibco S+ software (version 8.2).
Results
Baseline characteristics of the 151 subjects who completed the study are shown in Table 1. Subjects were recruited between October 2009 and May 2011. The subjects were well-matched with respect to age, gender, race, 25(OH)D and lipid levels. Consistent with the physiologic response of increased parathyroid hormone (PTH) to vitamin D deficiency, mean baseline PTH levels (approximately 60 pg/ml) were at the high end of the normal range (12–65 pg/ml) for both groups.
Table 1.
Baseline Characteristics.
| Vitamin D Repletion Group (n=76) | Placebo Group (n = 75) | P value | |
|---|---|---|---|
| Age (years) | 48.4±11.3 | 47.4±12.8 | 0.45 |
| % Women | 45% | 45% | 0.94 |
| % Black | 45% | 47% | 0.80 |
| 25(OH)D (ng/ml) | 13.4±5.3 | 14.1±5.7 | 0.45 |
| Calcium (mg/dl) | 9.0±0.3 | 9.1±0.4 | 0.06 |
| PTH (pg/ml) | 61±32 | 60±35 | 0.72 |
| Total Cholesterol (mg/dl) | 189.3±33.4 | 184.2±38.0 | 0.31 |
| HDL Cholesterol (mg/dl) | 50.8±14.9 | 49.3±12.7 | 0.94 |
| LDL Cholesterol (mg/dl) | 116.6±29.0 | 111.8±34.0 | 0.18 |
| Triglycerides (mg/dl) | 109.5±62.8 | 115.8±54.2 | 0.15 |
| Small LDL particles (nmol/l) | 780±487 | 816±421 | 0.49 |
| Total LDL particles (nmol/l) | 1267±425 | 1267±387 | 0.89 |
| Total HDL Particles (nmol/l) | 30836±6837 | 31884±5992 | 0.18 |
| Total VLDL Particles (nmol/l) | 57.7±34.4 | 57.4±29.9 | 0.91 |
| hs-CRP (mg/L) | 6.0±6.3 | 6.0±6.8 | 0.60 |
| Fasting Glucose (mg/dl) | 105.6±32.3 | 105.3±28.8 | 0.81 |
| Creatinine (mg/dl) | 1.0±0.2 | 1.0±0.2 | 0.47 |
Data is shown as mean values ± SD.
After 4 and 8 weeks of therapy, mean 25(OH)D levels were significantly higher than baseline in the vitamin D repletion group (37.0±9.5 and 43.0±12.3 ng/ml, respectively; P <0.0001 vs. baseline for both; Figure 1). In contrast, the 25(OH)D levels remained unchanged in the placebo group (14.5±5.8 and 14.6±6.2 ng/ml, 4 and 8 weeks respectively; P = NS for both vs. baseline). After 4 weeks, 79% of the subjects in the vitamin D repletion group had 25(OH)D levels ≥ 30 ng/ml and this proportion increased to 88% at the final study visit 8 weeks later. Therefore, most subjects who received vitamin D had sufficient 25(OH)D levels for the majority of the treatment period. Serum calcium levels increased by 0.12 mg/dl in the vitamin D group relative to the placebo group (P = .04), but remained below the upper limit of normal (10.5 mg/dl) for all subjects throughout the study, ranging between 8.0–10.1 mg/dl. PTH values decreased by an average 18±25 pg/ml in the vitamin D repletion group (P < .0001 vs. baseline), but were unchanged in the placebo group (−3±24 pg/ml, P = 0.28; ΔPTH for vitamin D vs. placebo P < .001).
Figure 1.
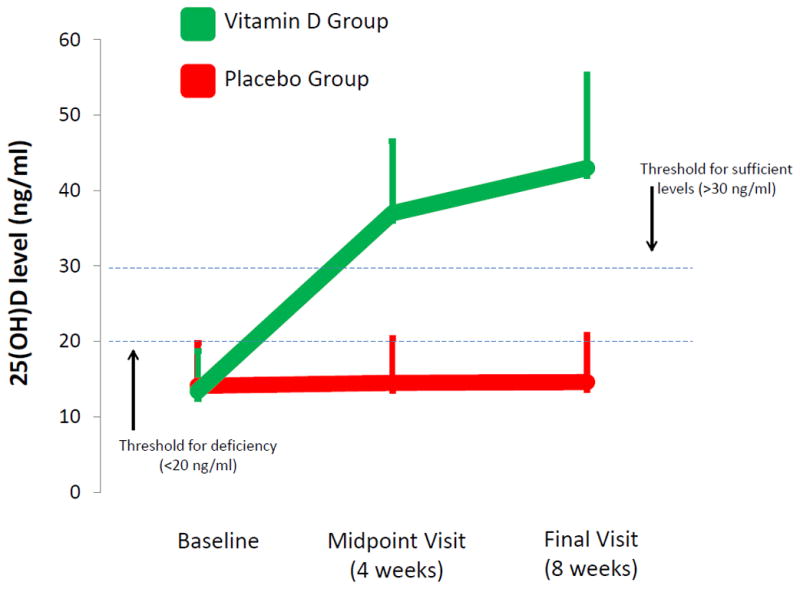
Changes in 25(OH)D levels
There were no significant differences in the changes in lipid parameters either within or between groups after 8 weeks of treatment for standard, chemical-based (Table 2) and NMR-based (Table S1) lipid measurements. There were also no changes in the chemical lipid profile after 4 weeks of treatment (Table S2).
Table 2.
Changes in the standard, chemical lipid profile (mg/dl). Data is shown as mean values ± SD and (% change).
| Change in Vitamin D Repletion Group (n=75) | P value | Change in Placebo Group (n = 76) | P value | Intergroup Difference [95%CI] | P value | |
|---|---|---|---|---|---|---|
| Total Cholesterol | +1.2±21.0 (+0.6) | 0.63 | −4.6±23.9 (−2.5) | 0.10 | +5.8 [−1.4 to +13.0] | 0.14 |
| LDL Cholesterol | −0.3±18.6 (−0.3) | 0.88 | −4.1±20.8 (−3.7) | 0.09 | +3.8 [−2.5 to +10.2] | 0.13 |
| HDL Cholesterol | +0.3±6.4 (+0.6) | 0.71 | −0.2±6.6 (−0.4) | 0.84 | +0.4 [−1.6 to +2.6] | 0.71 |
| Triglycerides | +6.1±50.0 (+5.3) | 0.29 | −1.8±39.0 (−1.6) | 0.70 | +7.9 [−6.5 to +22.3] | 0.43 |
Because there was a strong response of vitamin D repletion on the biomarkers of calcium and PTH, we determined through exploratory analyses, if this physiologic response to vitamin D was associated with changes in LDL cholesterol (Table 3a). Indeed, increases in serum calcium and decreases in PTH levels were significantly correlated with increases in LDL cholesterol. These relationships were absent in the placebo group (Figure 2). To account for potential confounding factors, we constructed a stepwise multivariate regression model for changes in LDL cholesterol in the vitamin D group (Table 3b). Consistent with the strong univariate relationships, changes in calcium and PTH remained significant, independent predictors of changes in LDL cholesterol (P < .001 and .016 for Δcalcium and ΔPTH, respectively; ANOVA F-statistic P < 1 × 10−6). In addition, the model explained 44% of the variability in LDL cholesterol levels. Increases in serum calcium and decreases in PTH were also significantly correlated with increases in LDL particle number: r = .33 for Δcalcium and r = −.40 for ΔPTH; P < .01 for both. Similarly, these relationships remained significant on multivariate analysis (P = .026 and .006 for Δcalcium and ΔPTH, respectively; ANOVA F-statistic P < 1 × 10−5; Table S3).
Table 3a.
Univariate Associations of Changes in Biomarkers with Changes in LDL Cholesterol in Response to Vitamin D Repletion
| Response Variables | r | P value |
|---|---|---|
| ΔCalcium | 0.522 | <.0001 |
| ΔPTH | −0.348 | 0.002 |
| ΔTG | −0.268 | 0.02 |
| Δ25(OH)D | 0.210 | 0.07 |
| ΔHDL Cholesterol | 0.198 | 0.09 |
| ΔPhosphorus | 0.098 | 0.40 |
| ΔhsCRP | 0.075 | 0.50 |
Figure 2.


Figure 2a. Changes in LDL vs. changes in calcium in response to placebo or vitamin D repletion.
Figure 2b. Changes in LDL vs. changes in PTH in response to placebo or vitamin D repletion.
Table 3b.
Multivariate Regression Model for the Change in LDL Cholesterol with Vitamin D therapy
| Regression Statistics | |
|---|---|
| Multiple R | 0.662 |
| R Square | 0.438 |
| Observations | 75 |
| Significance F | <.000001 |
| Coefficients | P-value | |
|---|---|---|
| ΔCalcium (per mg/dl) | 19.855 | <.001 |
| ΔPTH (per pg/ml) | −0.201 | 0.016 |
| ΔTG (per mg/dl) | −0.090 | 0.011 |
| Baseline LDL Cholesterol | −0.101 | 0.075 |
| ΔHDL | 0.513 | 0.083 |
| ΔGlucose | −0.116 | 0.127 |
Because vitamin D therapy has also been suggested to be anti-inflammatory, we measured serial hsCRP levels.17 Relative to the control group, there was no change in the mean hsCRP level with vitamin D repletion after 8 weeks (+1.5 mg/L, 95% CI [−0.5 to +3.5 mg/L]; P = 0.48).
Discussion
We conducted a randomized, double-blind, placebo-controlled trial to determine if vitamin D repletion exerts an effect on the lipid profile. Over an 8-week period, despite effective vitamin D repletion, there was a failure to improve either the standard or NMR-based lipid profile. As measured by a decrease in serum PTH and an increase in serum calcium, the vitamin D repletion group did show significant end-organ responses to vitamin D therapy. These physiologic responses were also significantly associated with an increase in LDL cholesterol. Therefore, high-dose oral supplementation in an at-risk population may have an adverse effect on cardiovascular risk for those individuals who have the strongest biologic response to vitamin D. Likewise, the benefit inferred from cross-sectional associations of higher 25(OH)D levels and a healthier lipid profile is not replicated by short-term vitamin D repletion.
Vitamin D deficiency is highly prevalent in the general population, and even more so in patients with cardiovascular disease.8, 9 Further, low 25(OH)D levels are associated with worse cardiovascular outcomes.10 However, adequately controlled, prospective studies of vitamin D repletion to determine an effect on cardiovascular morbidity and mortality are lacking.18 Even for surrogate cardiovascular biomarkers, such as blood lipids, few clinical trials have studied the effect of vitamin D supplementation, and these trials were inconclusive.19–28 We had previously reported on the incongruence of the vitamin D/lipid relationship when contrasting cross-sectional to longitudinal data.14 By analyzing a community-based laboratory data repository in a cross-sectional manner, we found that 25(OH)D levels >30 ng/ml compared to <20 ng/ml were associated with a markedly healthier lipid profile. However, in the same population of patients assessed longitudinally, raising 25(OH)D levels in the short-term had no effect on lipids. However, no randomized, placebo-controlled trial has studied the effect of vitamin D repletion, targeting 25(OH)D deficiency, with an adequate dose of vitamin D to achieve sufficient 25(OH)D levels. While large trials of vitamin D supplementation are underway that use higher doses of vitamin D than prior studies, they still do not specifically target vitamin D deficiency.30
Vitamin D deficiency is clinically defined by the serum level of 25(OH)D and low levels correlate with biomarkers of mineral metabolism, such as elevations in PTH. However, there is considerable variation in the end-organ response to vitamin D and there is still significant controversy over the definition of “normal” 25(OH)D levels.3, 31 We found that the biological effects of vitamin D repletion, namely a decrease in PTH and increase in serum calcium, were strongly and independently associated with a rise in LDL cholesterol and LDL particle number. Indeed, stratifying subjects by change in serum calcium with vitamin D therapy shows that those with an above-median response compared to those with a below-median response had an increase in LDL cholesterol of 15.4mg/dl. A similar subgroup analysis of the placebo group shows no relationship.
Our trial presents new data to guide clinical practice. In stark contrast to the strong cross-sectional associations between higher 25(OH)D levels each component of the lipid profile, our clinical trial failed to show any effect of vitamin D repletion on lipids.14 Further, the effect estimate for changes in LDL cholesterol was opposite that predicted by association. Indeed, qualitatively, there was a higher frequency of subjects in the vitamin D group who had an increase in LDL cholesterol levels compared to placebo at both 4 weeks (52% vs. 36%) and 8 weeks (55% vs. 37%). Though, the optimal timeframe for achieving repletion is unknown, and the long-term effects of vitamin D repletion on the lipid profile are unclear. However, the uncoupling between our randomized clinical trial data and the cross-sectional associations of higher 25(OH)D levels should spark caution towards inferred benefits of vitamin D supplementation on the lipid profile.
Epidemiologic and observational studies suggest that vitamin D may play a role in cardiovascular health and disease distinct from calcium and PTH homeostasis. However, definitive data from large, prospective clinical trials are lacking. Previous studies of other nutritional supplements have shown that such trials may be necessary prior to accepting supplementation as universal practice to avoid potential harm. Without the availability of outcomes data, an important step prior to embracing supplementation is to confirm that biomarkers of cardiovascular risk associated with vitamin D deficiency that were identified in cross-sectional studies do in fact respond to vitamin D therapy. Our study challenges the notion that vitamin D repletion ameliorates dyslipidemia and raises the possibility that vitamin D supplements may worsen the lipid profile for some patients.
Supplementary Material
Acknowledgments
“Supported in part by grant # 8 UL1 TR000043 from the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health.”
Footnotes
The authors do not have any conflicts of interest.
References
- 1.Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, Murad MH, Weaver CM. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–1930. doi: 10.1210/jc.2011-0385. [DOI] [PubMed] [Google Scholar]
- 2.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–281. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 3.Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, Clinton SK, Durazo-Arvizu RA, Gallagher JC, Gallo RL, Jones G, Kovacs CS, Mayne ST, Rosen CJ, Shapses SA. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab. 96:53–58. doi: 10.1210/jc.2010-2704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Heaney RP, Dowell MS, Hale CA, Bendich A. Calcium absorption varies within the reference range for serum 25-hydroxyvitamin D. J Am Coll Nutr. 2003;22:142–146. doi: 10.1080/07315724.2003.10719287. [DOI] [PubMed] [Google Scholar]
- 5.DeLuca HF. Overview of general physiologic features and functions of vitamin D. Am J Clin Nutr. 2004;80:1689S–1696S. doi: 10.1093/ajcn/80.6.1689S. [DOI] [PubMed] [Google Scholar]
- 6.Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25-Dihydroxyvitamin D(3) is a negative endocrine regulator of the renin-angiotensin system. J Clin Invest. 2002;110:229–238. doi: 10.1172/JCI15219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Merke J, Milde P, Lewicka S, Hugel U, Klaus G, Mangelsdorf DJ, Haussler MR, Rauterberg EW, Ritz E. Identification and regulation of 1,25-dihydroxyvitamin D3 receptor activity and biosynthesis of 1,25-dihydroxyvitamin D3. Studies in cultured bovine aortic endothelial cells and human dermal capillaries. J Clin Invest. 1989;83:1903–1915. doi: 10.1172/JCI114097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim DH, Sabour S, Sagar UN, Adams S, Whellan DJ. Prevalence of hypovitaminosis D in cardiovascular diseases (from the National Health and Nutrition Examination Survey 2001 to 2004) Am J Cardiol. 2008;102:1540–1544. doi: 10.1016/j.amjcard.2008.06.067. [DOI] [PubMed] [Google Scholar]
- 9.Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K, Benjamin EJ, D’Agostino RB, Wolf M, Vasan RS. Vitamin D deficiency and risk of cardiovascular disease. Circulation. 2008;117:503–511. doi: 10.1161/CIRCULATIONAHA.107.706127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Forman JP, Giovannucci E, Holmes MD, Bischoff-Ferrari HA, Tworoger SS, Willett WC, Curhan GC. Plasma 25-hydroxyvitamin D levels and risk of incident hypertension. Hypertension. 2007;49:1063–1069. doi: 10.1161/HYPERTENSIONAHA.107.087288. [DOI] [PubMed] [Google Scholar]
- 11.Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. The Expert Panel. Arch Intern Med. 1988;148:36–69. [PubMed] [Google Scholar]
- 12.Superko HR. Advanced lipoprotein testing and subfractionation are clinically useful. Circulation. 2009;119:2383–2395. doi: 10.1161/CIRCULATIONAHA.108.809582. [DOI] [PubMed] [Google Scholar]
- 13.Martins D, Wolf M, Pan D, Zadshir A, Tareen N, Thadhani R, Felsenfeld A, Levine B, Mehrotra R, Norris K. Prevalence of cardiovascular risk factors and the serum levels of 25-hydroxyvitamin D in the United States: data from the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2007;167:1159–1165. doi: 10.1001/archinte.167.11.1159. [DOI] [PubMed] [Google Scholar]
- 14.Ponda MP, Huang XX, Odeh MA, Breslow JL, Kaufman HW. Serial Clinical Laboratory Data Predict Vitamin D Repletion May Not Improve Lipid Levels. Circulation. 2012 doi: 10.1161/CIRCULATIONAHA.111.077875. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130:461–470. doi: 10.7326/0003-4819-130-6-199903160-00002. [DOI] [PubMed] [Google Scholar]
- 16.Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502. [PubMed] [Google Scholar]
- 17.Guillot X, Semerano L, Saidenberg-Kermanac’h N, Falgarone G, Boissier MC. Vitamin D and inflammation. Joint Bone Spine. 77:552–557. doi: 10.1016/j.jbspin.2010.09.018. [DOI] [PubMed] [Google Scholar]
- 18.Shapses SA, Manson JE. Vitamin D and prevention of cardiovascular disease and diabetes: why the evidence falls short. Jama. 305:2565–2566. doi: 10.1001/jama.2011.881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Andersen R, Brot C, Mejborn H, Molgaard C, Skovgaard LT, Trolle E, Ovesen L. Vitamin D supplementation does not affect serum lipids and lipoproteins in Pakistani immigrants. Eur J Clin Nutr. 2009;63:1150–1153. doi: 10.1038/ejcn.2009.18. [DOI] [PubMed] [Google Scholar]
- 20.Gannage-Yared MH, Azoury M, Mansour I, Baddoura R, Halaby G, Naaman R. Effects of a short-term calcium and vitamin D treatment on serum cytokines, bone markers, insulin and lipid concentrations in healthy post-menopausal women. J Endocrinol Invest. 2003;26:748–753. doi: 10.1007/BF03347358. [DOI] [PubMed] [Google Scholar]
- 21.Heikkinen AM, Tuppurainen MT, Niskanen L, Komulainen M, Penttila I, Saarikoski S. Long-term vitamin D3 supplementation may have adverse effects on serum lipids during postmenopausal hormone replacement therapy. Eur J Endocrinol. 1997;137:495–502. doi: 10.1530/eje.0.1370495. [DOI] [PubMed] [Google Scholar]
- 22.Maki KC, Rubin MR, Wong LG, McManus JF, Jensen CD, Lawless A. Effects of vitamin D supplementation on 25-hydroxyvitamin D, high-density lipoprotein cholesterol, and other cardiovascular disease risk markers in subjects with elevated waist circumference. Int J Food Sci Nutr. 62:318–327. doi: 10.3109/09637486.2010.536146. [DOI] [PubMed] [Google Scholar]
- 23.Nagpal J, Pande JN, Bhartia A. A double-blind, randomized, placebo-controlled trial of the short-term effect of vitamin D3 supplementation on insulin sensitivity in apparently healthy, middle-aged, centrally obese men. Diabet Med. 2009;26:19–27. doi: 10.1111/j.1464-5491.2008.02636.x. [DOI] [PubMed] [Google Scholar]
- 24.Rajpathak SN, Xue X, Wassertheil-Smoller S, VanHorn L, Robinson JG, Liu S, Allison M, Martin LW, Ho GY, Rohan TE. Effect of 5 y of calcium plus vitamin D supplementation on change in circulating lipids: results from the Women’s Health Initiative. Am J Clin Nutr. 91:894–899. doi: 10.3945/ajcn.2009.28579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Scragg R, Khaw KT, Murphy S. Effect of winter oral vitamin D3 supplementation on cardiovascular risk factors in elderly adults. Eur J Clin Nutr. 1995;49:640–646. [PubMed] [Google Scholar]
- 26.Tuppurainen M, Heikkinen AM, Penttila I, Saarikoski S. Does vitamin D3 have negative effects on serum levels of lipids? A follow-up study with a sequential combination of estradiol valerate and cyproterone acetate and/or vitamin D3. Maturitas. 1995;22:55–61. doi: 10.1016/0378-5122(95)00909-5. [DOI] [PubMed] [Google Scholar]
- 27.Witham MD, Nadir MA, Struthers AD. Effect of vitamin D on blood pressure: a systematic review and meta-analysis. J Hypertens. 2009;27:1948–1954. doi: 10.1097/HJH.0b013e32832f075b. [DOI] [PubMed] [Google Scholar]
- 28.Carbone LD, Rosenberg EW, Tolley EA, Holick MF, Hughes TA, Watsky MA, Barrow KD, Chen TC, Wilkin NK, Bhattacharya SK, Dowdy JC, Sayre RM, Weber KT. 25-Hydroxyvitamin D, cholesterol, and ultraviolet irradiation. Metabolism. 2008;57:741–748. doi: 10.1016/j.metabol.2008.01.011. [DOI] [PubMed] [Google Scholar]
- 29.Bolland MJ, Bacon CJ, Horne AM, Mason BH, Ames RW, Wang TK, Grey AB, Gamble GD, Reid IR. Vitamin D insufficiency and health outcomes over 5 y in older women. Am J Clin Nutr. 91:82–89. doi: 10.3945/ajcn.2009.28424. [DOI] [PubMed] [Google Scholar]
- 30.Manson JE. Vitamin D and the heart: why we need large-scale clinical trials. Cleve Clin J Med. 77:903–910. doi: 10.3949/ccjm.77gr.10004. [DOI] [PubMed] [Google Scholar]
- 31.Maxmen A. Nutrition advice: the vitamin D-lemma. Nature. 475:23–25. doi: 10.1038/475023a. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.