

Abstract
Background:
Breast cancer is the most common female malignancy and commonly associated with high levels of morbidity and mortality in developing countries due to late presentation. Breast self-examination (BSE) can help in early detection of the disease.
Aims:
This study aims to determine the awareness and practice of BSE among market women in Abakailiki, Southeast Nigeria.
Subjects and Methods:
This cross-sectional descriptive study involved the use of questionnaire among market women in Abakaliki. Inclusion criteria were women from the age of 18 years and above who own or sell in a shop, while females less than 18 years of age and women who came to the market to buy products were excluded. Questionnaires were distributed randomly among women who met the criteria in every shop visited based on willingness to participate. Analysis was done using Epi info version 3:5:3 (Atlanta Geogia USA.2008). The association between variables was tested using Chi square for trend statistics. Significance was set at P < 0.05. Binomial logistic regression analysis was used to test for relationship between the age group categories against ever heard of BSE.
Results:
The age range of participants was between 20 and 65 years, with a mean age of 34.3 (10.8) years. The age range between 20 and 29 years constituted the highest age group 35.3% (84/238). Majority 54.2% (129/238) had a maximum of secondary education. Of the 238 participants, 77.7% have heard of breast cancer, of which 73.9% thought that early detection would aid treatment. Only 38.9% (6/195), 13% and 13.4% have heard of BSE, clinical breast examination and mammography, respectively. Just 23.9% have been taught how to perform BSE, while 21.8% had done it in the past. One person 0.4% knew the correct frequency of BSE, and also did it regularly. There was a statistically significant difference between the level of education and awareness of BSE. However, there was no statistical significant difference between participants age and awareness of BSE.
Conclusion:
There was a low level of awareness of BSE among market women in Abakiliki, and there is a need to increase the level of awareness through campaigns.
Keywords: Awareness, Breast self-examination, Market women, Nigeria
Introduction
Breast cancer has increasingly become an issue of public health importance. In the year 2000, there were 10 million new cases of cancer and 6 million cancer deaths worldwide.[1,2] Each year, in the United States, almost 1.5 million individuals learn that they have some form of cancer.[3] Breast cancer is by far the most commonly diagnosed cancer in women, and, in the US in 2007, 202,964 women were diagnosed with breast cancer and 40,598 died from the disease.[4] Its incidence is becoming more common worldwide.[5] Studies have shown an increased incidence from African countries, where low rates have previously been reported, and an estimated world total incidence of 1.45 million was expected by the year 2010.[6–8] It is estimated that a woman who lives to the age of 90 years has a one in eight chance of developing breast cancer.[9] The peak age incidence of breast cancer in Nigeria is reported to be between 45 and 50 years, in contrast to Europe and America, where it was reported to be 65-75 years.[6,10,11] Some cases have been reported below 30 years in Nigeria.[12] Breast cancer reduces the life expectancy of the population at risk, especially those between 31 and 50 years.
The high incidence and fatality rate of breast cancer as well as the high cost of treatment require that it should be of a focus of high attention for health authorities and policy makers. The knowledge and care-seeking attitude for breast cancer management is so low that majority of the affected patients present late in the hospital when little or nothing can be done again. Studies have shown that most patients with breast cancer in developing countries like Nigeria present for the first time at stages 2 and 3. This indicates a need for increased community awareness of methods for early detection of the disease. Although breast cancer cannot be prevented, the risks of developing breast cancer can be minimized. Diagnosis of breast cancer during the early stage of the disease has been positively linked to a decrease in mortality, morbidity and effective cost of management of the illness. There are various methods of early detection of breast cancer. These include: Breast self examination (BSE), clinical breast examination (CBE) and mammography screening.
BSE involves visualization and palpation of the breast by oneself for lumps, shape, texture, size and contour. The purpose of this is for a woman to learn the topography of her breasts, know how her normal breasts feel and be able to identify changes in them should they occur in the future. Studies have shown that BSE has a positive effect on the early detection of breast cancer.[13] Despite that, there is no scientific evidence supporting the role of BSE in the early detection of breast cancer,[14] and some authors have argued that the declining practice of BSE dramatically decreases the probability of early detection of breast cancer.[15] The recommendations by the American College of Obstetricians and Gynaecologist (ACOG) and the American Cancer Society are for BSE to be performed monthly beginning at the age of 20 years and CBE annually beginning at the age of 18 years.[13] Although the role of regular BSE has been debated,[16] recent studies have suggested that BSE is a reliable screening tool when used as an adjunct to CBE and imaging study.[17] Again, it can nevertheless be utilised in enhancing breast cancer awareness among women.[18] In fact, regular BSE has been suggested as part of an overall health promotion concept.[19] It is important therefore to adequately motivate women to regularly carry out BSE so as to curtail the increasing mortality rate from breast cancer.
Although a lot has been done on the awareness and practice of BSE, not much has been done among the relatively less-educated group, like women that work in the market, as most of the studies have been directed toward relatively more educated and privileged group like nurses, doctors, university students, school teachers, etc., Again, the late presentation of many women with breast cancer to the hospitals in Abakiliki, Ebonyi State Southeast Nigeria, has continually become a major issue of great concern. In view of the importance of BSE in the early detection of breast cancer and the fact that it is cost effective and more readily available than any other method of early detection of breast cancer in our environment, this study was designed to assess the level of awareness and practice of regular BSE among market women in Abakaliki Southeast Nigeria.
Subjects and Methods
This study involved women in the Abakpa main market, which is the major market in Abakiliki LGA of Ebonyi state. Market women in this context refer to all women 18 years and above who own or sell in a shop within the market. The market is located in the heart of the town, and it attracts many buyers and sellers from peripheral communities and markets. It is a daily market that usually starts by 8:00 am and closes at 5:00 pm. The market is structured in lines according to the kind of trade one is dealing on. There are over 50 different lines in the market. Abakiliki is the capital city of Ebonyi state, housing the highest population and largest market in the State. It lies at the intersection between the Enugu, Afikpo and Ogoja roads. The city is a very young one and relatively on the developing sides compared with other neighboring state capitals. The estimated population of Abakaliki according to the 2006 census is 141,438. The inhabitants of the city are majorly of the Igbo tribe, Christians, and their predominant occupation is farming. Others are civil servants, quarry workers and business men and women.
The study population included women from the age of 18 years and above who own or sell in a shop. Exclusion criteria include females less than 18 years of age, women who came to the market to buy products and women who met the criteria but opted out. A questionnaire-based cross-sectional study of 238 women in the Abakpa main market of Abakiliki was done. The questionnaire was structured in three sections, which assessed the demographic characteristics of the study population, participant's awareness and practice of BSE. The participant level of awareness were assessed by asking questions like have you heard of breast cancer? have you heard of BSE? have you heard of clinical breast examination? etc.; the practice of BSE was equally assessed by asking questions like have you done BSE before? when last did you do BSE?. The questionnaire was validated and pre-tested among women in another market. The Egwuatu–Aneziokoro Medical Research Club members were trained as interviewers/research assistants to carry out the interview. The questionnaire was administered to participants on a one-on-one basis. The interviewers interpreted the questions to the language understood by the subjects. In the market, each line was located and one shop in every three shops that is manned by a woman was located. Questionnaires were distributed among women that met the criteria in every shop visited based on willingness to participate. Informed consent was obtained. This study was approved by the Research and Ethical Committee of the defunct Ebonyi State University Teaching Hospital, Abakaliki.
Data collected were analyzed using Epi info version 3:5:3 of the CDC Atlanta, USA, and presented in frequency table and simple chart distribution. The association between variables was tested using Chi square for trend statistics. Significance was set at P < 0.05. Binomial logistic regression analysis was used to test for relationship between the age group categories against ever heard of BSE [Table 1].
Table 1.
Using regression analysis for age against ever heard of BSE

Results
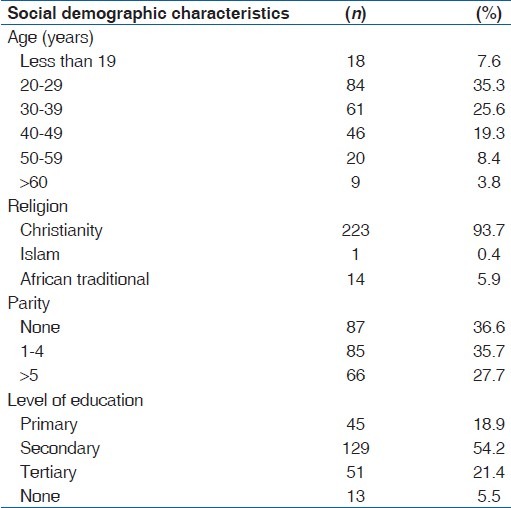
Two hundred and thirty-eight market women were recruited. The participants were aged between 18 and 65 years, with a mean age of 34.3 (10.8) years. The age range between 20 and 29 years constituted the highest age group (35.3%). Majority (93.7%) were Christians. More than half of the participants 129 (54.2%) had a maximum of secondary education, while only 13 participants (5.5%) had no formal education at all. Participants’ parity was evenly distributed as follows: None (36.6%), 1-4 (35.5%), greater than or equal to 5 (27.7%) [Table 2].
Table 2.
Frequency table of social demographic characteristics of the participants
On assessment of participants’ level of awareness of breast cancer, 185 participants (77.7%) agreed that they had heard of breast cancer, of which 176 (73.9%) thought that cancer could be treated if detected early. Participants’ perception of people at higher risk of having breast cancer is given in Table 3. Concerning the participants awareness of methods of early detection of breast cancer, 38.9 (76/195) participants had heard of BSE, 31 participants (13%) had heard of CBE while 32 participants (13.4%) had heard of mammography. Just 57 participants (23.9%) had been taught how to perform BSE, while 52 of them (21.8%) had done it in the past. Just one person (0.4%) practiced BSE monthly [Figure 1]. On comparing participants’ awareness of BSE and their educational attainment, results showed that there was a statistical association between the level of education and the awareness of BSE [Table 4]. However, there was no statistical association between participants age and awareness of BSE, as shown in Table 5.
Table 3.
Frequency table of participants’ perception of people at higher risk of having breast cancer
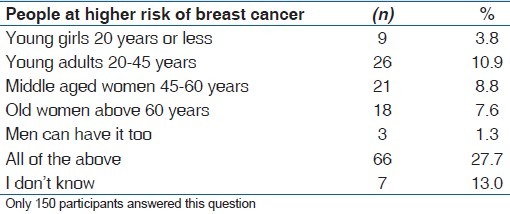
Figure 1.
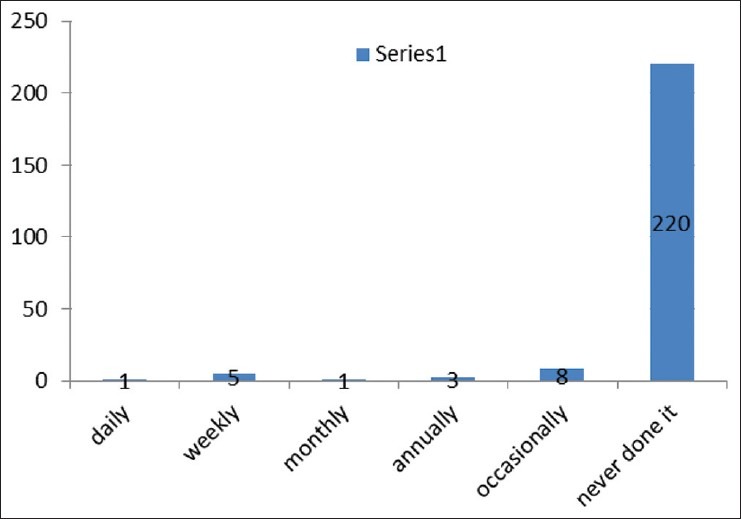
How often do you do breast self-examination?
Table 4.
Relationship between participants’ level of education and awareness of BSE

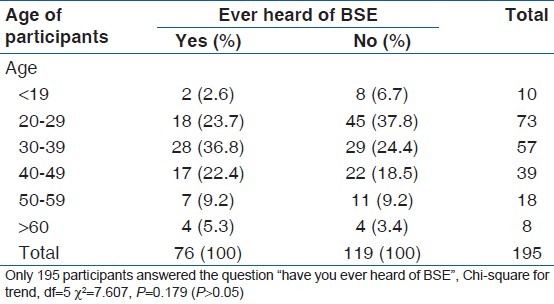
Table 5.
The relationship between participants’ age and awareness of BSE
There was a statistically significant difference between level of education and awareness of BSE.
Discussion
The participants’ level of awareness of breast cancer was significantly high (77.7%), implying that the market women in Abakiliki were very much aware of the disease, although only 73.9% believed that breast cancer could be treated if detected early. The reason for this high awareness level could be attributed to the several awareness campaigns about breast cancer directed to the market by the Medical Women Association and Medical Students Association in Abakailiki. The above results correlate with a similar study done in Abakaliki among nurses in Ebonyi State University Teaching Hospital, where Agwu et al., noted 98% awareness of the disease, and 59.2% believed that early detection could help save life.[20] It is also comparable to the 93.7% awareness noted in a study among nursing students in Lagos University Teaching Hospital. In the same study, it was reported that 99.3% of those aware of breast cancer agreed that early detection could improve the chances of survival.[21] The much higher level of awareness in these other studies is not surprising as the study was done among people in the health profession, and they are more likely to have heard of breast cancer than market women. Salaudeen et al., also recorded a high level of awareness of breast cancer (97.2%) among female undergraduates in Illorin, Nigeria.[22] Respondent's ideas of people predisposed to breast cancer is very diverse, and reveals very poor knowledge about breast cancer although there is high level of awareness. Awareness and level of knowledge are two different levels of education aims, and it is easier to gain awareness but not knowledge, which requires one to systematically be ‘taught’ or systematically look for info. Thus, the implication is to perform more structured educational campaigns targeting at knowledge now, and to follow-up on skills with practical sessions if needed as the study does show that educational intervention can improves skills. The study also found that 70% of the women maintained that lack of knowledge/skill on the proper practice of BSE was the key barrier to a more regular BSE practice.[23] In the study done by Rosemary et al., she recorded that 51.1% of her participants thought that only females could have breast cancer, while 48.9% thought that both males and females could have breast cancer.[21] This study was done among nurses, and that explains why her subjects had a better knowledge about the sort of people that do have breast cancer. The implication of this is that adequate health education programmes on breast cancer among the market women can greatly improve their level of knowledge of the disease.
Assessment of the participants’ awareness about various methods of early detection of breast cancer showed that more people were aware of BSE 38.9% than CBE and mammography (13% and 13.4%, respectively), although there is a generally low level of awareness of BSE. This is inconsistent with the 94.0% awareness of BSE and 30% awareness of other methods of early detection of breast cancer noted among female health practitioners at the Federal Medical Centre Owo, Ondo State.[24] This is probably because of the study group involved; health practitioners are more likely to have heard of BSE than market women. The awareness of CBE in this study, even though low, is higher than what was noted in Aba, Nigeria, where only 1% and 2% of the participants were aware that breast examination can be performed by doctors and nurses, respectively.[25] Another study among female teachers in Ilorin, Nigeria, also revealed 95.6% awareness of BSE.[26] These agreed with other studies done in Enugu and Lagos, both in Nigeria, which reported that 92% of the participants were aware of the procedure.[27,28] There was no statistically significant difference between participant's age and hearing of BSE in this study. However, there is a statistically significant difference between the participants’ level of education and hearing BSE. Although the more likely source of information about BSE to market women are churches and hospitals, which do not necessarily have to do with participants’ age or level of education, it is not surprising that education increases awareness of BSE, as it further exposes an individual to other possible sources like schools, newspapers, radios and televisions.
Concerning the knowledge of BSE, only 23.9% of the participants had been taught on how to perform BSE. This implies that even a lesser percentage will have good knowledge about BSE. This is very low compared with the 85.6% noted by Rosemary among female nurses in Lagos University Teaching Hospital;[21] although the study populations are different, it does not justify such low knowledge. However, another study reported among undergraduates in Ahmadu Bello University Zaria, Nigeria, showed a similar result in which only 37.3% of his participants could correctly describe BSE.[29] This seriously calls for urgent attention by the government, public and private health institutions and other non-governmental agencies to join hands in promoting awareness and proper knowledge about BSE as a method of early detection of breast cancer.
Concerning the practice of BSE, only 21.8% of our respondents have practiced it in the past, while only one respondent (0.4%) knows the correct frequency of BSE practice and also performs it religiously. The finding of this study corroborates similar Iranian and Egyptian studies, in which only 6% and 2.65% of the study population, respectively, practiced BSE monthly.[30] Gwarzor et al., also noted in their study that 57% of the participants have practiced BSE in the past, but only 32.1% of them currently practice it, while only 19.0% of the participants practice it every month.[28] In another study, although among health workers, Mbanaso et al., and Omolase found that 47.9% and 56% of their participants, respectively, performed BSE monthly.[17,31] Another study done in America revealed that 31% of the study population practiced BSE monthly.[32] The reason for the poor practice of BSE by these market women is not known. This area will be an interesting area to look at in subsequent studies.
In this study, Chi square was preferred for analysis over Fisher exact t test. The Fisher exact test is a statistically significant test for categorical data, measuring the association between two variables in a 2 × 2 contingency table. It is best when a cell has a value less than 5. However, in many cases, the Chi-square is preferred because the Fisher exact test is difficult to calculate. Although a package that can calculate Fisher exact for 2 × 3 has been developed, it was not possible to get a package to calculate the Fisher exact test for tables with more than three rolls. Indeed, it is recommended that if the table has two columns and three or more rows (or two rows and three or more columns), and the categories can be quantified, the Chi-square test for trend can be performed irrespective of the value in a cell.[33,34]
This study therefore reveals that most participants have heard of breast cancer as a disease entity; however, adequate knowledge and understanding of the disease is still lacking. Furthermore, the awareness, knowledge and practice of BSE and other methods of early detection of breast cancer among market women in Abakiliki is very much on the low side. We therefore recommend that more awareness campaigns about BSE should be carried out and directed to the market women by health organizations and students in Abakaliki; bill boards and hand tracts on BSE and its practice should be mounted and/or distributed within and around the market; government and non-governmental organizations should sponsor more campaigns about BSE in the market; health workers should intensify health education on BSE when they come in contact with these women during antenatal visits or other visits, encouraging and funding universal basic education is also advocated.
Further studies to explore reasons for such low levels of knowledge and practice of BSE, and the best methods of improving results, should be carried out.
Acknowledgment
The authors wish to appreciate the participants for their time and invaluable information. They also thank the members of the Egwuatu-Anieziokoro Medical Research Club for their effort in data collection. The supervisors are also highly appreciated.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol. 2001;2:533–43. doi: 10.1016/S1470-2045(01)00486-7. [DOI] [PubMed] [Google Scholar]
- 2.Pisani P, Bray F, Parkin DM. Estimates of the world wide prevalence of cancer for 25 sites in the adult population. Int J Cancer. 2002;97:72–81. doi: 10.1002/ijc.1571. [DOI] [PubMed] [Google Scholar]
- 3.Thomas P, Neoplasia . In: Robbins and Cotran, pathologic basis of diseases. 7th ed. Kumar V, Abbas K. A, Fausto N, editors. Singapore: Elsevier; 2006. p. 270. [Google Scholar]
- 4.US cancer statistics working group. Atlanta (GA): Department of health and human services, Centre for Disease Control and prevention and National cancer institute; 2010. [Last accessed on 2012 May 24]. United state cancer statistics: 1999-2007. Incidence and mortality web based report. Available from: http://www.CDC.gov/uscs . [Google Scholar]
- 5.Adebamowo CA, Adekunle OO. Case controlled study of the epidemiology risk factors for breast cancer in Nigeria. Br J Surg. 1999;86:665–8. doi: 10.1046/j.1365-2168.1999.01117.x. [DOI] [PubMed] [Google Scholar]
- 6.Parkin MD, Pisani P, Ferlay J. Global cancer statistics. CA Cancer J Clin. 1999;49:33–64. doi: 10.3322/canjclin.49.1.33. [DOI] [PubMed] [Google Scholar]
- 7.Adebamowo CA, Ajayi A. Breast cancer in Nigeria. West Afr J Med. 2000;19:179–91. [PubMed] [Google Scholar]
- 8.Salaudeen AG, Musa OI, Oluwale A. Effect of health education on breast cancer and practice of breast self examination among female students of the tertiary institution a Nigerian state. [Last accessed on 30th September, 2012];Res J Soc Sci. 2009 4:61–8. Available from: http://www.aensiweb.com/./61.68.pdf . [Google Scholar]
- 9.Susan CL. The breast. In: Kumar V, Abbas KA, Fausto N, editors. Robbins and Cotran, pathologic basis of diseases. 7th ed. Singapore: Elsevier; 2006. pp. 1129–49. [Google Scholar]
- 10.Abudu EK, Banjo AA, Izegbu MC, Agboola AO, Anunobi CC, Musa A. Malignant breast lesions at Olabisi Onabanjo University Teaching Hospital (OOUTH) Sagamu-a histopathological review. Niger Postgrad Med J. 2007;14:57–9. [PubMed] [Google Scholar]
- 11.Anyanwu SN. Breast cancer in eastern Nigeria: A ten year review. West Afr J Med. 2000;19:120–5. [PubMed] [Google Scholar]
- 12.Okobia MN, Osime U. Clinicopathological study of carcinoma of the breast in Benin City. Afr J Reprod Health. 2001;5:56–62. [PubMed] [Google Scholar]
- 13.Baines CJ. Breast self examination. Cancer. 1992;69:1942–6. doi: 10.1002/1097-0142(19920401)69:7+<1942::aid-cncr2820691712>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 14.Kösters JP, Gøtzsche PC. Regular self-examination or clinical examination for early detection of breast cancer. Cochrane Database Syst Rev. 2003;(2):CD003373. doi: 10.1002/14651858.CD003373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wagl A, Komorita NI, Lu ZJ. Social support and breast self examination. Cancer Nurs. 1997;20:42–8. doi: 10.1097/00002820-199702000-00006. [DOI] [PubMed] [Google Scholar]
- 16.Hackshaw AK, Paulo EA. Breast self examination and death from breast cancer a meta analysis. Br J Cancer. 2003;88:1047–53. doi: 10.1038/sj.bjc.6600847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Smith RA, Cokkinder V, Eyer HJ. American cancer society guideline for early detection of cancer, 2005. CA Cancer J Clin. 2005;55:31–44. doi: 10.3322/canjclin.55.1.31. [DOI] [PubMed] [Google Scholar]
- 18.Rao RS, Nair S, Nair NS, Kamath VG. Acceptability and effectiveness of breast health awareness programme for rural women in India. Indian J Med Sci. 2005;59:398–402. [PubMed] [Google Scholar]
- 19.Plesnicar A, Kovac V, Kralj B. Breast cancer and breast health awareness as an evolving health promotion concept. Radiol Oncol. 2004;38:27–34. [Google Scholar]
- 20.Agwu UM, Ajaero EP, Ezenwelu CM, Agbo CJ, Ejikeme BN. Knowledge, attitude and practice of breast self examination among nurses in Ebonyi State University Teaching Hospital, Abakiliki. EMJ J. 2007;6:44–7. [Google Scholar]
- 21.Rosemary BB, Nicholas KI, Modele AO, Adekunle AA, Adebayo TO. Knowledge, attitude and practice of breast self examination among nursing students in Lagos university teaching hospital. Acad J Cancer Res. 2010;3:11–5. [Google Scholar]
- 22.Salaudeen AG, Akande TM, Musa OI. Knowledge and attitude to Breast cancer and Breast Self Examination among Female Undergraduate in a state in Nigeria. [Last accessed on 2012 Sep 30];Euro J Soc Sci. 2009 7:157–65. Available from: http://www.eurojournals.com/ejss_7_3_15.pdf . [Google Scholar]
- 23.Loh SY, Chew SL. Awareness and practice of breast self examination among Malaysian women with breast cancer. [Last accessed on 2012 Jul 31];Asia Pac J Cancer Prev. 2011 12:199–202. Available from: http://www.apocp.org/cancer_download/Volume12_No1/199202%20c%2012.18%20Loh%20%20Siew%20Yim.pdf . [PubMed] [Google Scholar]
- 24.Omolase CO. Awareness, knowledge and practice of breast-self examination amongst female health workers in a Nigerian community. Ann Afr Med. 2009;8:55–8. [Google Scholar]
- 25.Onwere S, Okoro O, Chigbu B, Onwere A. Practice of antenatal clinical breast examination as a method of early detection of breast cancer by health care providers in a low resource setting. Arch Gynecol Obstet. 2007;10:7–10. doi: 10.1007/s00404-007-0533-z. [DOI] [PubMed] [Google Scholar]
- 26.Kayode FO, Akande TM, Osagbemi GK. Knowledge, attitude and practice of breast self examination among female secondary school teachers in Ilorin, Nigeria. European Journal of Scientific Research. 2005;10:42–7. [Google Scholar]
- 27.Nwagbo DF, Akpala CO. Awareness of breast cancer and breast self-examination among women in Enugu Urban, Eastern Nigeria. J Coll Med. 1996;1:34–6. [Google Scholar]
- 28.Odeyemi KA, Oyediran MA. Effects of a breast cancer screening community intervention in Oke-Ira, Lagos State, Nigeria. Nigerian Journal of Comm Med and Prry Health Care. 2002;14:66–77. [Google Scholar]
- 29.Gwarzo UM, Sabitu K, Idris SH. Knowledge and practice of breast-self examination among female undergraduate students of Ahmadu Bello University Zaria, north western Nigeria. Ann Afr Med. 2009;8:55–8. doi: 10.4103/1596-3519.55766. [DOI] [PubMed] [Google Scholar]
- 30.Haji-Mahmoodi M, Montazeri A, Jarvandi S, Ebrahimi M, Haghighat S, Harirchi I. Breast self –examination: Knowledge, attitudes and practices among female health care workers in Tehran Iran. Breast J. 2002;8:222–5. doi: 10.1046/j.1524-4741.2002.08406.x. [DOI] [PubMed] [Google Scholar]
- 31.Mbanaso AU, Adisa AC, Onuoha C. Status of breast self examination among health professional of Abia State University Teaching Hospital. J Experimental Clin Anat. 2005;4:55–7. [Google Scholar]
- 32.Sadler GR, Ko CM, Cohn JA, White M, Weldon RN, Wu P. Breast cancer knowledge, attitudes and screening behaviors among African American women the Black cosmetologists promoting health program. BMC Public Health. 2007;7:57. doi: 10.1186/1471-2458-7-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Chi-square test. [Last accessed on 2012 Aug 8]. Available from: http://ww/en.wikipedia.org/wiki/Pearson%27s_Chi-square_test .
- 34.Fisher Exact. [Last accessed on 2012 Aug 8]. Available from: http://en.wikipedia.org/wiki/Fisher's_exact_test .