

Abstract
Holt-Oram syndrome is a rare inherited disorder that causes abnormalities of the hands, arms, and the heart. Most commonly, there are defects in the carpal bones of the wrist and in the bones of the thumb along with cardiac defects such as atrial or ventricular septal defects. We report a case of Holt-Oram syndrome with a rare association of double outlet right ventricle.
Keywords: Complex congenital heart disease, double outlet right ventricle, heart-hand syndrome
INTRODUCTION
Congenital cardiac and upper-limb malformations frequently occur together and are classified as heart-hand syndromes. The most common amongst the heart-hand disorders is the Holt-Oram syndrome (HOS), which is characterized by the cardiac septation defects and pre-axial radial ray abnormalities. One out of 100,000 live births is affected.[1] Approximately 75% of HOS patients have some cardiac abnormality with common associations being either an atrial septal defect (ASD) or atrioventricular septal defect (VSD).[2] Herein, we report a rare sporadic case of Holt-Oram syndrome with double outlet right ventricle (DORV), and persistent left superior vena cava (SVC).
CASE REPORT
A seven month old baby was referred because of feeding difficulties and failure to thrive since 3 months of age. There was history of bluish discolouration of the body while excessive crying. The antenatal history was unremarkable and the baby was delivered at term normally by a 22 year old primigravida.
Physical examination revealed an active baby with weight of 5.5 Kgs, length of 63 cm, heart rate of 120 beats/min, blood pressure of 92/58 mm of Hg, respiratory rate of 40/min and systemic oxygen saturation was 85% at ambient room air. On musculoskeletal examination, left upper limb had foreshortened mid segment associated with flexion deformity at the elbow and wrist joints, rudimentary thumb and clinodactyly [Figure 1a]. Right upper limb had hypoplastic thumb, clinodactyly and flexion deformity of wrist [Figure 1a]. No obvious deformities were observed in lower limbs or elsewhere. Cardiovascular examination revealed ejection systolic murmur of grade III/VI at left parasternal area. Electrocardiogram [Figure 2] showed normal sinus rhythm with right ventricular hypertrophy with right axis deviation. Chest roentogram [Figure 2] showed levocardia, cardiomegaly mainly of right ventricle, pulmonary oligemia and normal thoracic situs. Plain radiograph of both upper limbs revealed absent radius, underdeveloped ulna of left upper limb and absent first metacarpal, hypoplastic thumb pahalanges in both upper limbs [Figure 1b]. Two dimensional echocardiography showed double outlet right ventricle (DORV) with large subaortic ventricular septal defect (VSD) with more than 50% over riding by aorta along with severe valvular pulmonary stenosis with normal pulmonary venous drainage [Figure 3]. There was evidence of aorto-mitral discountinuity. It also revealed persistent left superior vena cava draining into dilated coronary sinus. Complete blood count was normal (no thrombocytopenia). Renal ultrasound and kidney function tests were normal. The baby underwent the complete intracardiac repair. On follow up the baby is thriving well and asymptomatic regarding his cardiac symptoms. He is being followed up in paediatric, cardiology and orthopedic clinics.
Figure 1.

Photograph (a) depicting foreshortened midsegment of the left upper limb along with flexion deformity at the elbow and wrist joints and rudimentary thumb. Right upper limb has hypoplastic thumb. Clinodactyly is seen in both limbs. Plain radiograph (b) of the left upper limb (left side) showing absent radius and hypoplastic ulna with both upper limbs showing absent first metacarpal and hypoplastic thumb phalanges
Figure 2.
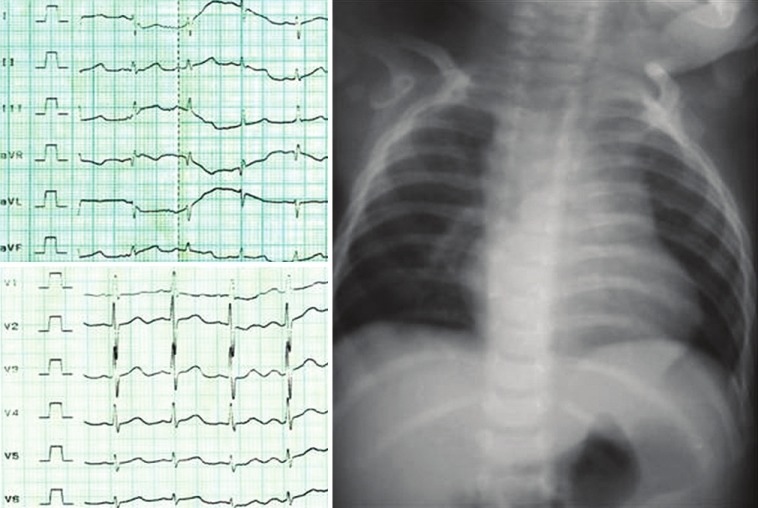
Electrocardiogram (left side) showed normal sinus rhythm with right ventricular hypertrophy with right axis deviation. Chest roentogram (right side) showed levocardia, oligemia, cardiomegaly (cardiothoracic ratio of 60%) mainly of right ventricle, normal thoracic situs
Figure 3.
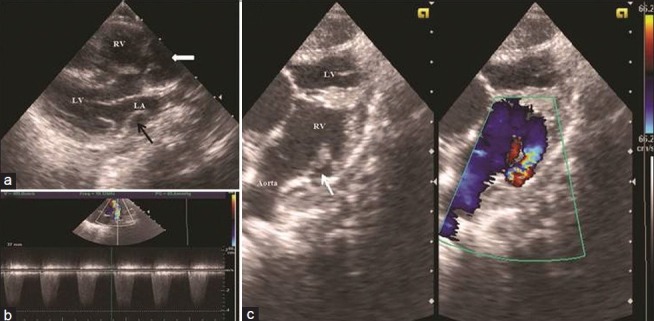
Parasternal long axis view (a) demonstrating large subaortic ventricular septal defect with more than 50% over riding by aorta (thick white arrow) and dilated coronary sinus (black arrow). Subcostal view (c) demonstrating both great vessel committed to right ventricle with Doppler evidence of severe right ventricular outflow tract obstruction (thin white arrow) having peak gradient of 65 mm of mercury (b) (LV = Left ventricle;RV = Right ventricle;LA = Left atrium)
DISCUSSION
HOS is an autosomal dominant disorder characterized by distinctive malformation of bones of the upper limbs and abnormalities of heart. Holt and Oram first described this syndrome in 1960.[3] The cardinal manifestations of HOS are dysplasia of upper limb that ranges from minor findings including hypoplasia of thumb, clinodactyly, brachydactyly, triphalangeal thumbs, carpal bone dysmorphism, shortness of ulna, shortness of humerus, aplasia of radius (as in our case) to phocomelia[4] and cardiac abnormalities. Although bilateral, left side often is affected more significantly (as in our case). In a study of 98 subjects with hypoplastic thumbs 16% proved to be the cases of HOS.[5] There are many well described heart-hand syndromes characterized by deformities of the radial ray and congenital heart defects like thrombocytopenia absent radius (TAR) syndrome, Roberts syndrome, thalidomide embryopathy and Fanconi anaemia. The unique feature that helps to differentiate these from HOS is that the radial aplasia is associated with hypoplasia/absence of the thumb without any haematological abnormalities and there is often a family history of heart and limb defects.
The associated congenital heart defects are the most important determining factors in morbidity and mortality in these patients. More than 85% of affected individuals have cardiac malformations particularly atrial septal or ventricular septal defects.[6] Other cardiac associations include pulmonary stenosis, mitral valve prolapse and arrhythmias in the form of atrio-ventricular blocks. More complex cardiac lesions such as tetralogy of Fallot, endocardial cushion defects and total anomalous pulmonary venous return are observed in 18% of subjects with HOS.[7] The association with DORV is very rare. As per best of our knowledge, till date there are very few cases reported in literature having description of HOS with DORV.[8,9] The electrocardiographic abnormalities such as variable degree of atrioventricular blocks have also been reported. In their first paper Holt and Oram described “bizarre atrial arrhythmias”.[10]
In conclusion, we reported a case of Holt-Oram syndrome with a rare association of double outlet right ventricle with valvular pulmonary stenosis with persistent left superior vena cava and right sided aortic arch.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Basson CT, Cowley GS, Solomon SD, Weissman B, Poznanski AK, Traill TA, et al. The clinical and gentic spectrum of the Holt-oram syndrome (heart-hand syndrome) N Engl J Med. 1994;330:885–91. doi: 10.1056/NEJM199403313301302. [DOI] [PubMed] [Google Scholar]
- 2.Basson CT, Solomon SD, Weissman B, MacRae CA, Poznanski AK, Prieto F, et al. Genetic heterogeneity of heart-hand syndromes. Circulation. 1995;91:1326–9. doi: 10.1161/01.cir.91.5.1326. [DOI] [PubMed] [Google Scholar]
- 3.Holt M, Oram S. Familial heart disease with skeletal malformations. Br Heart J. 1960;22:236–42. doi: 10.1136/hrt.22.2.236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Alizad A, Seward JB. Echocardiographic features of genetic diseases. J Am Soc Echocardiogr. 2000;13:248–53. doi: 10.1067/mje.2000.102345. [DOI] [PubMed] [Google Scholar]
- 5.James MA, Mc Carroll HR, Jr, Manske PR. Characteristics of patients with hypoplastic thumbs. J Hand Surg Am. 1996;21:104–13. doi: 10.1016/s0363-5023(96)80162-6. [DOI] [PubMed] [Google Scholar]
- 6.Lin AE, Perloff JK. Upper limb malformations associated with congenital heart disease. Am J Cardiol. 1985;55:1576–83. doi: 10.1016/0002-9149(85)90976-2. [DOI] [PubMed] [Google Scholar]
- 7.Sletten LJ, Pierpont ME. Variation in severity of cardiac disease in Holt-oram syndrome. Am J Med Genet. 1996;65:128–32. doi: 10.1002/(SICI)1096-8628(19961016)65:2<128::AID-AJMG9>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- 8.Awni Al-Madani. The Holt-oram syndrome with double outlet right ventricle with valvular and subvalvular pulmonary stenosis. Kuwait Med J. 2008;40:315–7. [Google Scholar]
- 9.Kumar A, Van Mierop LH, Epstein ML. Pathogenetic implications of muscular ventricular septal defect in Holt-Oram syndrome. Am J Cardiol. 1994;73:993–5. doi: 10.1016/0002-9149(94)90153-8. [DOI] [PubMed] [Google Scholar]
- 10.Bosset T, Walther T, Gummert J, Gummert J, Hubald R, Kostelka M, Mohr WF. Holt-Oram syndrome. Orphanet. 2003. Available from: https://www.orpha.net/data/patho/GB/uk-HOS.pdf . [DOI] [PubMed]