

Abstract
Background:
Intra operative cytology (IC), including touch imprint (TI) and crash preparations (CP), in general has been demonstrated to be a diagnostic tool for many organs but its validity and reliability for diagnosis of thyroid nodules remain controversial. We evaluate the diagnostic value of frozen section, touch imprint, crash preparation and the combination of touch imprint and crash preparation and the combination of frozen section, touch imprint and crash preparation.
Materials ans Methods:
55 intra operative specimens from patients with thyroid nodules who underwent thyroidectomy were evaluated at Alzahra and vali-Asr hospital laboratories. For all of the patients frozen section (FS), touch imprint (TI) and crash preparation (CP) was obtained and reviewed by two pathologists at the same time. Serial TI and CP, and FS, TI and CP were reviewed by the same pathologists. Sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, negative likelihood ratio and accuracy were calculated according to the permanent section as the gold standard test.
Results:
In our study sensitivity, specificity and accuracy for FS was 100%, 97.6% and 98.1% respectively; for TI they were 78.6%, 95% and 92.4%; for CP they were 78.6%, 92.7% and 89.9%; for serial TI and CP they were 85.7%, 92.7% and 90.9%; and for the combination of FS and TI and CP they were 100%, 97.6% and 98.18% respectively.
Conclusions:
Intra operative cytology (including TI and CP) seems to be a useful, valuable and inexpensive method in clinics, which do not have equipment for frozen sections. Intra operative cytology combined with FS increased the overall accuracy of diagnosis. Further studies are needed to validate the obtained results of this study.
Keywords: Crash Preparation, Frozen Section, Thyroid Nodule, Touch Imprint
INTRODUCTION
Thyroid nodules are very common, while thyroid cancer is a rare condition.[1] Estimated prevalence of thyroid nodule ranges from 4% by palpation to 67% by ultra sonography.[2] On the other hand, thyroid cancer accounts for less than 1% of all malignancies, with an incidence of 0.004% per year.[1,3]
Although thyroid nodules are common, only malignant nodules or large symptomatic nodules need surgery, a systemic approach evaluation is necessary to avoid erroneous surgical treatment.[4] Often these nodules can be managed conservatively. The clinical problem is to identify malignant lesions that require surgical operation. The most cost-effective method for evaluating thyroid nodules is fine needle aspiration (FNA); its accuracy exceeds 80% in most series.[3–5]
To avoid unnecessary surgical treatment intra operative frozen section (FS) is usually performed. FS has been in use since 1818, but it became routine after the introduction of cryostat in 1960.[6]
The role of FS has been criticized by some authors who have found no or little difference in the accuracy of FS and FNA methods, and some have recommended against the routine use of FS due to its cost-effectiveness and validity.[5,7,8]
Intra operative cytology (IC), including touch imprint (TI) and crash preparations (CP), has been demonstrated to be a diagnostic tool for breast, parathyroid, salivary gland and thyroid specimen.[9,10,11]
The performance of intra operative cytology is very rapid and easy but its validity and reliability for diagnosis of thyroid nodules remain controversial; there are different sensitivity, specificity and accuracy in literature for these techniques in the diagnosis of different histopathology statuses for example papillary carcinoma, colloid nodules and follicular neoplasm.[8–13]
The purpose of our study was to assess the value of FS, TI, CP, TI and CP, and FS, TI and CP techniques in predicting malignancy in patients with nodular thyroid disease.
MATERIALS AND METHODS
In this cross-sectional study 55 fresh, unfixed intra operative specimens submitted during thyroidectomy were reviewed in Alzahra (Isfahan, Iran) and Vali-asr (Arak, Iran) hospital laboratories during 2010-2011. Thyroglossal duct, cyst excision, incidental thyroid resections as part of laryngectomy or during another neck surgery for the other indication and metastatic lesions were excluded.
All specimens were sectioned by the pathologist in the abnormal area, then frozen and cut in cryostat (MICROM). The number of blocks depends on the size of the nodule: 2 blocks if the diameter of nodule was <= 2 cm, 3 blocks if it was greater than 2 cm. Three or more sections of each block were stained with the haematoxylin-eosin method.
The area of indicated lesion was touched by the surface of the glass slide in a small area before freezing, to prepare touch imprint slides. For preparation of crash slides, a piece of specimen was crushed between two glassy slides with a little force, so that the tissue would not be destroyed.
All smears were air dried and then stained with the fast Hematoxylin-Eosin method. The main difference of this method with the routine method is in the duration of eosin staining (3 minute versus 7 minute in routine H & E method).
The remaining tissue was fixed with formalin and then processed to prepared paraffin embedding and permanent sectioning (3 microns). The final diagnosis based on permanent H & E section (PS) was considered as a gold standard.
All FS, TI, CP and permanent slides were reviewed separately by two pathologists at the same time, and then TI and CP, and FS, TI and CP were reviewed together by the same pathologists retrospectively. These pathologists were blinded to the final and other techniques’ reports. All of these slides were reviewed after surgery and surgeons did not use this information to change the approach of surgery in this stage of the survey.
In FS and intra operative cytology (TI and CP), separately or together, the pathologic diagnoses were coded as malignant or suspicious nodule. All remaining diagnoses were coded as benign, including: goiter, adenoma, Hurtle cell adenoma, hyperplasia and thyroiditis.
Permanent, suspicious nodules could be categorized as malignant (follicular carcinoma) or benign (follicular adenoma)
Results of FS, TI, CP, combination of TI and CP, and the combination of FS, TI and CP were compared to permanent histological examinations for the determination of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (PLR), negative likelihood ratio (NLR) and accuracy for each technique. Sensitivity was based on the equation: true positive / (true positive + false negative); specificity was calculated by the equation: true negative / (true negative + false positive); PPV was defined as: true positive / (true and false positive); NPV was defined as: true negative / (true and false negative); and PLR and NLR represented the combination of sensitivity and specificity respectively: sensitivity / (1- specificity) and (1- sensitivity) / specificity. Accuracy was calculated by the equation: (true positive and negative) / total cases).
RESULTS
The studied patients were comprised of 46(83.6%) female and 9(16.4%) male. The mean (and standard deviation) age was 43.83(17.35) years, ranging from 21 to 76 years.
Permanent histological examination
Out of 55 patients with final pathological diagnosis by permanent section, 14 (25.5%) of the nodules were malignant and 41 (75.5%) were benign (Table 1). The results of FS, TI, CP, combination of TI and CP, and the combination of FS, TI and CP are compared with PS in table 2. We have no cases of follicular carcinoma because this diagnosis is very rare in our region; however, cytological techniques have limitations in the diagnosis of follicular carcinomas.
Table 1.
Final Histopathological Diagnosis in 55 Patients with Thyroid Nodules
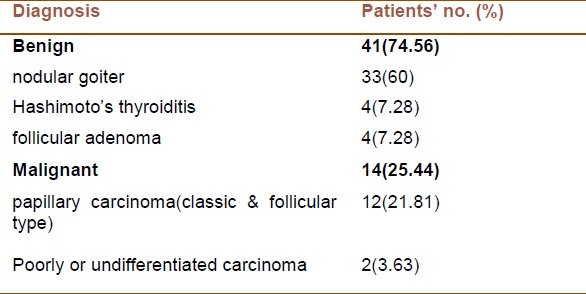
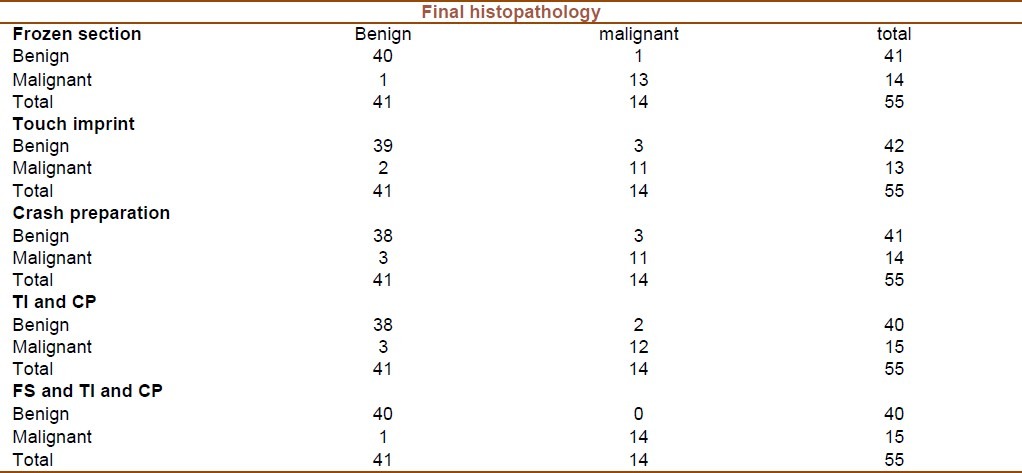
Table 2.
Results of each diagnostic method versus final histopatologic result
Frozen section
FS examinations revealed malignant nodules in 14 patients (25.5%), one of which was benign as compared with PS. The FS were diagnosed benign lesions in 41 cases (74.5%) but 1 specimen was malignant as compared with PS.
Touch imprint
Imprint examination showed malignant lesion in 13 patients (23.6%), but PS revealed that only eleven of them were malignant. Thus, the findings of malignancy were correct in 11 of 13 cases (84.6%) when showing 2 false positive findings. Benign imprint lesions were found in 42 (76.4%) patients, but PS revealed that 3 of them were malignant thus being false negative results. Imprint diagnosis of benign conditions was correct in 39 of 41 (95.1%) patients.
Crash preparation
Crash method found malignant nodules in 14 patients (25.5%), 3of which were diagnosed benign in PS; thus there were 3 false positive results. Out of 41 benign crash lesions, 3 lesions were malignant in PS, which means there were 3 false negative results.
Combination of touch imprint and Crash preparation
Combination of TI and CP examination showed 15 malignant (27.3%) and 40 benign (72.7%) nodules. 3 of 15 malignant lesions were benign in PS and 2 of 40 benign lesions were malignant compared with PS. Thus there were 3 false positive and 2 false negative results.
Combination of frozen section, touch imprint and crash preparation
Among the 15 cases diagnosed as malignant by the combination of the three techniques, 14 were confirmed by permanent pathology. Therefore, there were no false negative results. However, one case of those diagnosed as malignant was revealed to be benign in permanent pathology and considered as a false positive result.
Overall sensitivities, specificity, positive and negative predictive value, positive and negative likelihood ratio for FS, TI, CP, combination of TI and CP, and the combination of FS, TI and CP are presented in table 3, 4 and 5. Total accuracy was 96.36, 92.45, 89.9 and 98.18 respectively for each of these examinations.
Table 3.
Sensitivity and Specificity of each method

Table 4.
Positive predictive value (PPV) and negative predictive value (NPV) of each method
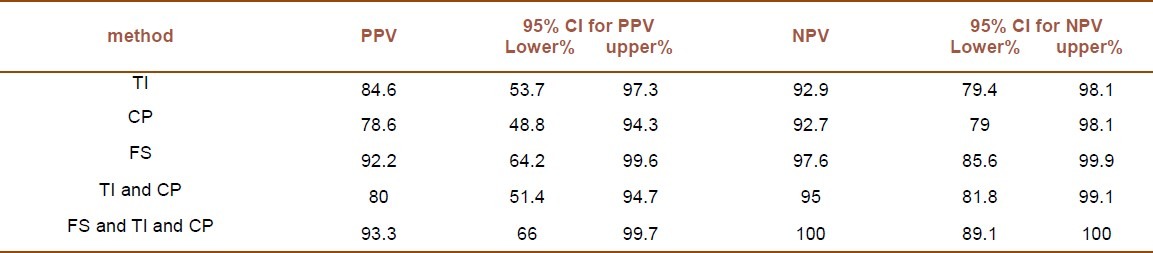
Table 5.
Positive likelihood ratio (PLR) and Negative likelihood ratio (NLR) and total accuracy for each technique

DISCUSSION
Although physical examination, scintigraphy and ultrasound give some preoperative information about the nature of nodules, they fail in the discrimination between benign and malignant nodules. Therefore, preoperative FNA biopsy, intra operative FS and cytology including imprint and crash preparation are required for this purpose. At present, preoperative FNA and intra operative FS are used routinely in both the diagnosis and management of the thyroid nodules.[7,8,13]
Fine-needle aspiration (FNA) is currently considered to be the single most accurate and cost-effective diagnostic method in the preoperative evaluation, with an accuracy rate exceeding 80% according to most studies,[5,14,15] but it has some limitations in non-diagnostic results and follicular lesions. In these cases many authors suggest the use of intra operative FS to increase the sensitivity for detecting a thyroid malignancy.[10,11,16]
Intra operative imprint cytology is rich for cells and thus has been assumed a more suitable cytological examination technique by pathologists, in spite of its limitation for detection of vascular and capsular invasion.[13]
Masuda et al. showed that imprint cytology may be useful in the prompt intra-operative evaluation.[17]
In another study Novik et al. evaluated patients with thyroid nodules and found the sensitivity of FNA biopsy and/or imprint cytology to be 92.3% and the specificity to be 75 % in regard to demonstrating malignancy. These results suggested an important role of cytological examinations in the management of thyroid nodules by showing that imprint cytology is more efficient and reliable because of its cellularity.[18]
On the other hand, Faroux et al. compared patients with thyroid nodules examined by intra-operative imprint cytology with patients evaluated by preoperative FNA with regard to 31 cytological criteria to distinguish benign from malignant lesions. They could not find any significant differences between the two methods.[19]
Ferit et al. in their study on patients with thyroid nodules reported the accuracy of FS and imprint to be 95% and 96% respectively. They suggested that imprint cytology can provide a useful adjunct to the frozen-section diagnosis and cytopathology and may be used safely in the diagnosis and management of thyroid nodules, especially in the case when the FS cannot be performed.[13]
Basolo et al. reported the value of intra operative consultations with FS examinations and tumor scrape preparation stained with ultrafast papanicolaou and they demonstrated that FS agreed with the final diagnosis in 29 cases out of 41 and that the diagnostic accuracy of FS increased up to 98% with the association of intra operative cytology(IC).[20]
In another study done by Basolo et al., FNA results and FS separately or in combination with IC were compared. In this study the diagnostic accuracy of FNA and FS was 88.8%, whereas combination of FS and IC had an accuracy of 95.7%.[12]
As found in our study, intra operative cytology showed the results comparable to FS. Although sensitivity of TI and CP were lower than FS separately, these sensitivities were valuable; specificity and overall accuracy of these methods were approximately equal to FS. It should be added that TI and CP need less instrumentation, do not have expensive equipments and are also less time consuming. Intra operative cytology can be managed properly because many of the nodules were not palpable and slides of preoperative FNA were insufficient, but during the surgical operation nodules were also easily seen. Moreover even when results of intra operative cytology (including TI and CP) combined with the findings obtained by FS, the overall accuracy, sensitivity, specificity, PPV, NPV and PLR were increased and NLR was decreased.
According to our observations, in TI and CP which were stained by fast haematoxylin-eosin some criteria such as overlapping or folding of nuclear contour, nuclear groove and clearing have been accepted to be features of malignancy versus large size and powdery appearance of nucleus in slide which were prepared by ultrafast papanicolaou staining.
One of the limitations of our study was that there were no cases of medullary carcinoma in the malignant group, so our results can only be applied to those lesions arising from follicular cells. This study does not give us any information about the diagnostic efficacy of intra operative cytology and frozen section for medullary carcinoma which arises from Para follicular cells.
CONCLUSION
Intra operative cytology (including TI and CP) seems to be a useful, valuable and inexpensive method in the management of thyroid nodules for clinics, which do not have expensive equipment. Intra operative cytology combined with FS increased the overall accuracy of the diagnosis. Further studies are needed to validate the obtained results of this study.
ACKNOWLEDGMENT
AC and MHS contributed in all stages of the article design, performing and manuscript preparation. We would like to thank other authors, who were also involved in design and data collection.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Greenspan FS. The thyroid gland. In: Greenspan FS, Gardner DG, editors. Basic and clinical endocrinology. 6th ed. New York: McGraw-Hill; 2001. pp. 201–72. [Google Scholar]
- 2.Ezzat S, Sarti DA, Cain DR, Braunstein GD. Thyroid incidentalomas. Prevalence by palpation and ultrasonography. Arch Intern Med. 1994;154(16):1838–40. doi: 10.1001/archinte.154.16.1838. [DOI] [PubMed] [Google Scholar]
- 3.Lumachi F, Borsato S, Tregnaghi A, Marino F, Poletti A, Iacobone M, et al. Accuracy of fine-needle aspiration cytology and frozen-section examination in patients with thyroid cancer. Biomed Pharmacother. 2004;58(1):56–60. doi: 10.1016/j.biopha.2003.08.025. [DOI] [PubMed] [Google Scholar]
- 4.Castro MR, Gharib H. Continuing controversies in the management of thyroid nodules. Ann Intern Med. 2005;142(11):926–31. doi: 10.7326/0003-4819-142-11-200506070-00011. [DOI] [PubMed] [Google Scholar]
- 5.Cetin B, Aslan S, Hatiboglu C, Babacan B, Onder A, Celik A, et al. Frozen section in thyroid surgery: is it a necessity? Can J Surg. 2004;47(1):29–33. [PMC free article] [PubMed] [Google Scholar]
- 6.Ibanez ML, Russell WO, Chang JP, Speece AJ. Cold chamber frozen sections for operating room diagnosis and routine surgical pathology. Lab Invest. 1960;9:98–109. [PubMed] [Google Scholar]
- 7.Mandell DL, Genden EM, Mechanick JI, Bergman DA, Biller HF, Urken ML. Diagnostic accuracy of fine-needle aspiration and frozen section in nodular thyroid disease. Otolaryngol Head Neck Surg. 2001;124(5):531–6. doi: 10.1067/mhn.2001.115372. [DOI] [PubMed] [Google Scholar]
- 8.Brooks AD, Shaha AR, DuMornay W, Huvos AG, Zakowski M, Brennan MF, et al. Role of fine-needle aspiration biopsy and frozen section analysis in the surgical management of thyroid tumors. Ann Surg Oncol. 2001;8(2):92–100. doi: 10.1007/s10434-001-0092-7. [DOI] [PubMed] [Google Scholar]
- 9.Shidham VB, Asma Z, Rao RN, Chavan A, Machhi J, Almagro U, et al. Intraoperative cytology increases the diagnostic accuracy of frozen sections for the confirmation of various tissues in the parathyroid region. Am J Clin Pathol. 2002;118(6):895–902. doi: 10.1309/N46X-JW4D-DYXF-DB4Y. [DOI] [PubMed] [Google Scholar]
- 10.Paessler M, LiVolsi VA, Baloch ZW. Role of ultrafast Papanicolaou-stained scrape preparations as an adjunct to frozen sections in the surgical management of thyroid lesions. Endocr Pract. 2001;7(2):89–94. doi: 10.4158/EP.7.2.89. [DOI] [PubMed] [Google Scholar]
- 11.Tworek JA, Giordano TJ, Michael CW. Comparison of intraoperative cytology with frozen sections in the diagnosis of thyroid lesions. Am J Clin Pathol. 1998;110(4):456–61. doi: 10.1093/ajcp/110.4.456. [DOI] [PubMed] [Google Scholar]
- 12.Basolo F, Ugolini C, Proietti A, Iacconi P, Berti P, Miccoli P. Role of frozen section associated with intraoperative cytology in comparison to FNA and FS alone in the management of thyroid nodules. Eur J Surg Oncol. 2007;33(6):769–75. doi: 10.1016/j.ejso.2006.12.004. [DOI] [PubMed] [Google Scholar]
- 13.Taneri F, Poyraz A, Salman B, Tekin E, Akyuerek N, Bayram O, et al. Using imprint and frozen sections in determining the surgical strategies for thyroid pathologies. Endocr Regul. 2001;35(2):71–4. [PubMed] [Google Scholar]
- 14.Bugis SP, Young JE, Archibald SD, Chen VS. Diagnostic accuracy of fine-needle aspiration biopsy versus frozen section in solitary thyroid nodules. Am J Surg. 1986;152(4):411–6. doi: 10.1016/0002-9610(86)90314-4. [DOI] [PubMed] [Google Scholar]
- 15.Boyd LA, Earnhardt RC, Dunn JT, Frierson HF, Hanks JB. Preoperative evaluation and predictive value of fine-needle aspiration and frozen section of thyroid nodules. J Am Coll Surg. 1998;187(5):494–502. doi: 10.1016/s1072-7515(98)00221-x. [DOI] [PubMed] [Google Scholar]
- 16.Richards ML, Chisholm R, Bruder JM, Strodel WE. Is thyroid frozen section too much for too little? Am J Surg. 2002;184(6):510–4. doi: 10.1016/s0002-9610(02)01074-7. [DOI] [PubMed] [Google Scholar]
- 17.Masuda T, Tezuka F, Konno H, Togashi A, Itoh Y, Sugawara T. Intraoperative imprint cytology of the thyroid gland with computer-assisted morphometric analysis of cell clusters. Anal Quant Cytol Histol. 1988;10(4):294–8. [PubMed] [Google Scholar]
- 18.Novik VI, Krasil’nikova LA, Iudkovskaia IL. The results of cytologic diagnosis of thyroid diseases (20 years experience) Vopr Onkol. 1997;43(2):202–5. [PubMed] [Google Scholar]
- 19.Faroux MJ, Pluot M, Delisle MJ, Coninx P. Evaluation of morphological criteria in the cytological diagnosis of thyroid cold nodules. A preliminary study. Pathol Res Pract. 1990;186(3):330–5. doi: 10.1016/S0344-0338(11)80291-8. [DOI] [PubMed] [Google Scholar]
- 20.Basolo F, Baloch ZW, Baldanzi A, Miccoli P, LiVolsi VA. Usefulness of Ultrafast Papanicolaou-stained scrape preparations in intraoperative management of thyroid lesions. Mod Pathol. 1999;12(6):653–7. [PubMed] [Google Scholar]