

Abstract
Background:
Extranodal lymphoma may arise anywhere outside lymph nodes mostly in the gastrointestinal (GI) tract as non-Hodgkin's disease. We reviewed the clinicopathological features and treatment results of patients with primary GI lymphoma.
Materials and Methods:
A total number of 30 cases with primary GI lymphoma were included in this study. Patients referred to the Radiation Oncology Department of Omid Hospital (Mashhad, Iran) during a 5-year period (2006-11). Clinical, paraclinical, and radiological data was collected from medical records of the patients.
Results:
Out of the 30 patients with primary GI lymphoma in the study, 12 were female (40%) and 18 were male (60%) (male to female ratio: 3/2). B symptoms were present in 27 patients (90%). Antidiuretic hormone (LDH) levels were elevated in 9 patients (32.1%). The most common primary site was stomach in 14 cases (46.7%). Other common sites included small intestine and colon each in 8 patients (26.7%). All patients had histopathologically proven non-Hodgkin's lymphoma. The most common histologic subtype was diffuse large B-cell lymphoma (DLBL) in 16 patients (53.3%). In addition, 28 patients (93.3%) received chemotherapy with cyclophosphamide, vincristine, doxorubicin, prednisolone (CHOP regimen). The median course of chemotherapy was 6 cources. Moreover, 8 patients (26.7%) received radiotherapy with cobalt 60. The median follow-up time was 26 months. The overall 5-year survival rate was 53% and the median survival time was 60 months.
Conclusion:
Primary GI lymphoma is commonly seen in stomach and small intestine and mostly is DLBCL or mucosa-associated lymphoid tissue (MALT) lymphoma.
Keywords: Primary Gastrointestinal Lymphoma, Diffuse Large B-Cell Lymphoma, Extranodal Lymphoma
INTRODUCTION
While extranodal lymphoma may arise anywhere outside lymph nodes, gastrointestinal (GI) tract is the most frequent site of extranodal involvement by non-Hodgkin's lymphoma.[1] Stomach is the most commonly involved organ followed by the small intestine, pharynx, colon, and rarely, esophagus.[2]
Primary lymphoma of the GI tract, as a single site, should be limited to the tract with no palpable peripheral lymphadenopathy. In addition, chest X-ray and white blood cell count would not reveal any abnormalities. Nodal involvement, if observed, should be limited to the drainage area of the involved segment of the GI tract while liver and spleen remain intact.[3]
Secondary involvement of the GI tract with lymphoma is common since mesenteric or retroperitoneal lymph nodes are common origins of lymphoma that may share their lymphatic drainage with lymphoid tissue in the GI tract.[4] According to Iranian Cancer Registry, lymphoma comprises 0.78% of total gastric cancers and 0.48% of colon cancers in the country.[5]
Several risk factors such as human immunodeficiency virus (HIV), Helicobacter pylori infection, celiac disease, inflammatory bowel disease, and immunosuppression after solid organ transplantation have been identified for GI tract lymphoma.[6] In this study, we reviewed demographic, clinical, and paraclinical characteristics of patients with primary GI tract lymphoma who were referred to our center. We also evaluated their outcome after therapy and during follow up.
MATERIALS AND METHODS
Patients:
Over a 5-year period (2006-11), 30 cases of primary GI tract lymphoma were in the oncology department of Omid Hospital (affiliated to Mashhad University of Medical Sciences, Mashhad, Iran) were evaluated. Clinical, paraclinical, and radiological data was collected from the patients’ medical records.
Clinical staging:
The patients’ clinical staging was determined according to the Ann Arbor classification. Diagnostic work-up and staging procedures at the presentation time included patient medical history and complete physical examination, complete blood count, serum biochemistry, erythrocyte sedimentation rate, bone marrow aspiration and biopsy, chest X-ray, computed tomography (CT) scan of the chest, CT or ultrasonography of the abdomen and the pelvis, and multiple biopsies of the lesion in the GI tract.
Histology and immunohistochemistry:
All pathology blocks and slides were reviewed by pathologists of the center. Moreover, immunohistochemical studies such as leucocytes common antigen (LCA), cluster of differentiation (CD)3, CD15, CD20, and other markers, were performed to determine the subtype of non-Hodgkin's lymphoma. Classification by the Revised European-American Lymphoma (REAL)/the World Health Organization (WHO) was used for histopathologic subclassification. Finally, data was analyzed by SPSS16.
RESULTS
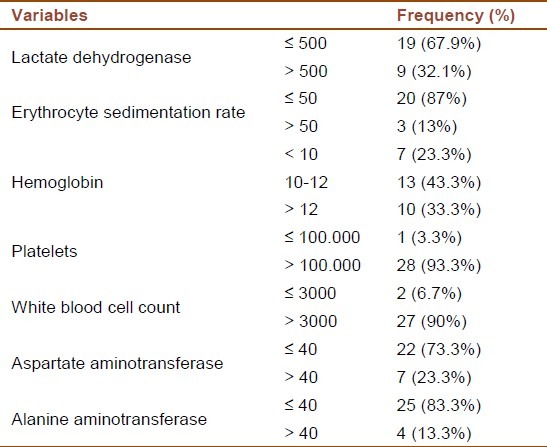
During 2006-11, epidemiologic data of 30 patients (12 females and 18 males; male to female ratio: 3:2) with primary GI lymphoma was assessed. The mean age of patients was 50 ± 16.9 years (range: 15-79 years). Dyspepsia and obstruction were the most common presenting symptoms. The characteristics of the patients and results of laboratory tests are summarized in Tables 1 and 2, respectively. B symptoms were present in 27 patients (90%). Lactate dehydrogenase (LDH), as an important prognostic factor in non-Hodgkin's lymphoma, was elevated in 9 patients (32.1%). Anemia was seen in 20 patients (66.6%). In the majority of patients, other laboratory tests such as platelets, white blood cell count and liver enzymes were normal.
Table 1.
Characteristics of patients with primary gastrointestinal tract lymphoma
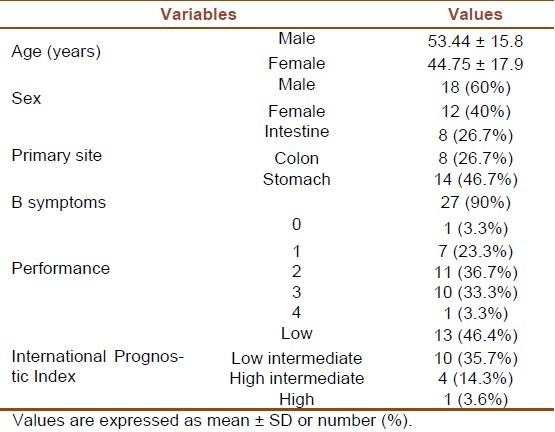
Table 2.
Results of laboratory tests of patients with primary gastrointestinal tract lymphoma
The most common primary site of lymphoma was stomach which was involved in 14 cases (46.7%). Other common sites were small intestine and colon which were each involved in 8 (26.7%) patients. (Figure 1)
Figure 1.
The primary involved site of GI lymphoma
All patients had proven non-Hodgkin's lymphoma. Spleen was intact in all cases. According to Ann Arbor staging system, 43.3% of patients were in stage I, 36.6% in stage II, 6.6 % in stage III, and 13.3% in stage IV. The International Prognostic Index (IPI) score and final condition of patients are presented in Figures 2 and 3, respectively.
Figure 2.
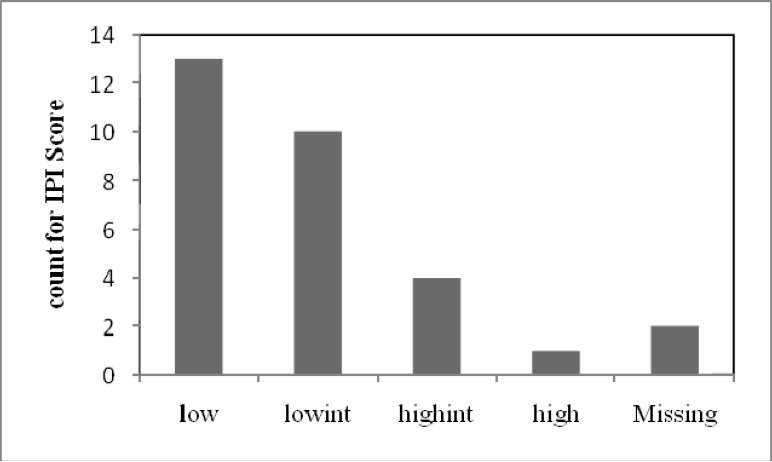
The International Prognostic Index (IPI) score of patients with gastrointestinal tract lymphoma in Omid Hospital (Mashhad, Iran)
Figure 3.
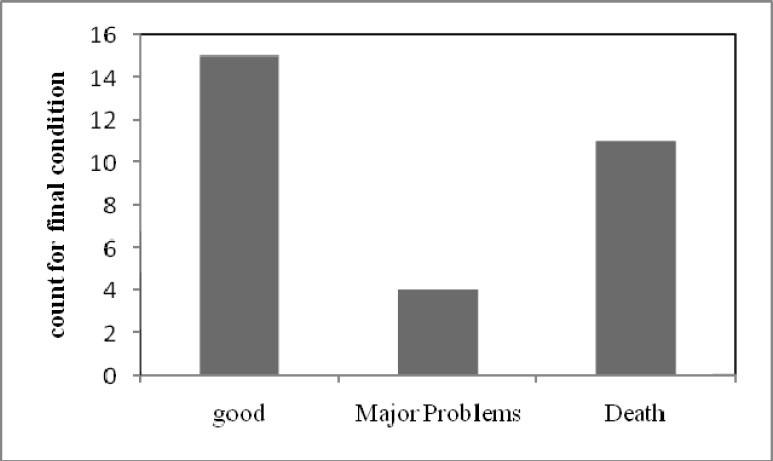
Final condition of patients with primary gastrointestinal tract lymphoma
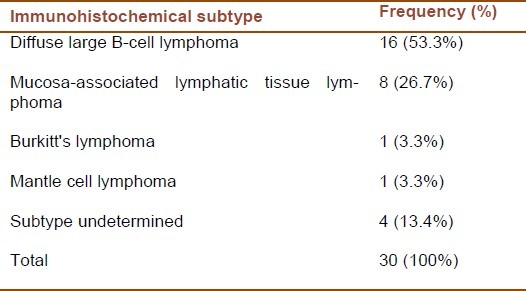
The most common histologic subtype was diffuse large B-cell lymphoma in 16 patients (53.3%). In addition, mucosa-associated lymphatic tissue (MALT) lymphoma, Burkitt's lymphoma, and mantle cell lymphoma (MCL) were observed in 8 patients (26.7%), 1 patient (3.3%), and 1 patient (3.3%), respectively. In 4 cases however, the subtype remained undetermined (Table 3).
Table 3.
Subtypes of non-Hodgkin's lymphoma
Moreover, 28 patients (93.3%) received chemotherapy with cyclophosphamide, vincristine, doxorubicin, and prednisolone (CHOP regimen). The median course of chemotherapy was 6 cources. Radiotherapy with cobalt 60 was also performed for 8 patients (26.7%).
Median follow-up time was 26 months. The overall 5-year survival was 53% and median survival was 60 months. (Figure 4)
Figure 4.
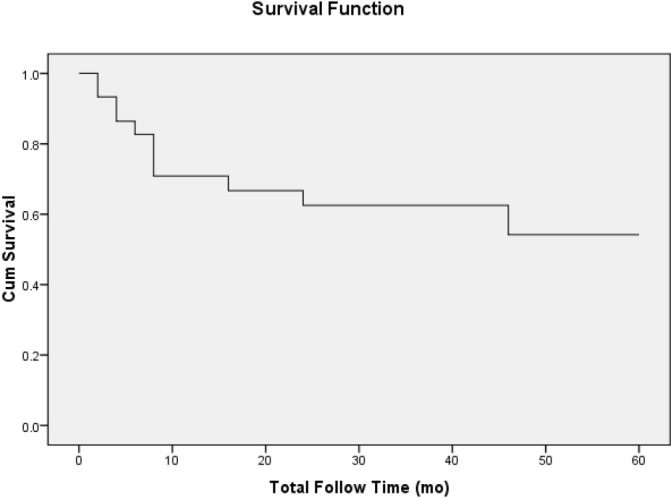
Median follow-up and median survival time
DISCUSSION
Primary GI tract lymphoma, with an incidence about 11-34% in all non-Hodgkin's lymphomas, is not a very common disease.[7,8] Lymphomas in the GI tract are usually of the B-cell phenotype and mostly diffuse large cell subtype.[9] Histological subtype of lymphoma may be different according to the site of involvement. Primary lymphoma of the stomach is common and is mostly of MALT type.[9,10] Primary follicular lymphoma of the GI tract is very rare and accounts for less than 7% of all non-Hodgkin's lymphomas.[2]
A clinical index of prognosis, i.e. IPI, has been used to assess and estimate the outcome of lymphoma patients. This indicator is based on the patient's age, performance status, and location and extent of disease. Low IPI scores (0-2) have been identified to be associated with better overall survival as compared to high IPI scores (3-5).
In our study, 28 out of 30 patients had favorable prognosis according to IPI scoring. Final condition was good in almost half of our patients. In the review of pathologic findings and final diagnosis, most of the studied GI tract lymphomas were diffuse large B-cell lymphoma and low grade MALT lymphoma. Similarly, Hans et al. reported diffuse large B-cell lymphoma to be the most common type of non-Hodgkin's lymphoma which accounted for 30-40% of all new cases. However, it was found heterogeneous both clinically and morphologically.[12] Shukla et al. evaluated 25 cases of primary GI tract lymphoma and detected 9 cases of gastric lymphoma, 9 cases of small intestinal lymphoma, and 7 cases of large intestinal lymphoma. Male to female ratio was 2.6:1 and age range was 4-63 years. Abdominal pain or mass were the most common presenting symptoms. Diffuse large B-cell type and Burkitt's lymphoma were the most common types of GI tract lymphoma, each of which accounted for 36% of the cases.[13] In another study by Al-Sayes, among 23 patients with primary GI non-Hodgkin's lymphoma, male to female ratio was 1.3:1 and the mean age was 61.3 years. Abdominal pain was the most common presenting symptom (78.3%), and the most common primary site was the stomach (73.9%) followed by the small bowel (13%). The most frequent histologic subtype was diffuse large B-cell lymphoma, accounting for 60.9% of all cases, followed by the marginal-zone cell lymphoma (MALT type).[14] Review of similar articles showed almost the same epidemiologic distribution and general specifications for primary GI tract lymphoma in different populations.
CONCLUSIONS
Primary GI tract lymphoma is commonly seen in stomach and small intestine and mostly is diffuse large B-cell lymphoma or MALT type.
ACKNOWLEDGMENTS
Authors would like to thank Mrs. Ahmadi Simab for her valuable contribution in statistical analysis process in this study.
Footnotes
Source of Support: This work was supported by Cancer Research Center (Omid Hospital), Mashhad University of Medical Sciences (MUMS), Mashhad, Iran.
Conflict of Interest: None declared.
REFERENCES
- 1.Yoo CC, Levine MS, McLarney JK, Rubesin SE, Herlinger H. Value of barium studies for predicting primary versus secondary non-Hodgkin's gastrointestinal lymphoma. Abdom Imaging. 2000;25(4):368–72. doi: 10.1007/s002610000055. [DOI] [PubMed] [Google Scholar]
- 2.Crump M, Gospodarowicz M, Shepherd FA. Lymphoma of the gastrointestinal tract. Semin Oncol. 1999;26(3):324–37. [PubMed] [Google Scholar]
- 3.Johnston MR, de Perrot M. Lymphoma. In: Devita VT, Lawrence TS, Rosenberg SA, Weinberg RA, editors. Cancer: Principles and practice of oncology. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2008. pp. 2476–92. [Google Scholar]
- 4.Clarke CA, Glaser SL. Changing incidence of non-Hodgkin lymphomas in the United States. Cancer. 2002;94(7):2015–23. doi: 10.1002/cncr.10403. [DOI] [PubMed] [Google Scholar]
- 5.Tehran: Ministry of Health and Medical education, Deputy of Health; 2006. Iran canser Report 2005. [Online]. Available from: URL: http://www.emro.who.int/ncd/pdf/cancer_registry_iran.pdf . [Google Scholar]
- 6.Card TR, West J, Holmes GK. Risk of malignancy in diagnosed coeliac disease: a 24-year prospective, population-based, cohort study. Aliment Pharmacol Ther. 2004;20(7):769–75. doi: 10.1111/j.1365-2036.2004.02177.x. [DOI] [PubMed] [Google Scholar]
- 7.Gou HF, Zang J, Jiang M, Yang Y, Cao D, Chen XC. Clinical prognostic analysis of 116 patients with primary intestinal non-Hodgkin lymphoma. Med Oncol. 2012;29(1):227–34. doi: 10.1007/s12032-010-9783-x. [DOI] [PubMed] [Google Scholar]
- 8.Radic-Kristo D, Planinc-Peraica A, Ostojic S, Vrhovac R, Kardum-Skelin I, Jaksic B. Primary gastrointestinal non-Hodgkin lymphoma in adults: clinicopathologic and survival characteristics. Coll Antropol. 2010;34(2):413–7. [PubMed] [Google Scholar]
- 9.Koch P, del VF, Berdel WE, Willich NA, Reers B, Hiddemann W, et al. Primary gastrointestinal non-Hodgkin's lymphoma: I.Anatomic and histologic distribution, clinical features, and survival data of 371 patients registered in the German Multicenter Study GIT NHL 01/92. J Clin Oncol. 2001;19(18):3861–73. doi: 10.1200/JCO.2001.19.18.3861. [DOI] [PubMed] [Google Scholar]
- 10.Gandhi JS, Mehta A, Sharma A, Kamboj M. Primary Hodgkin lymphoma of the ileum. J Cancer Res Ther. 2010;6(3):342–3. doi: 10.4103/0973-1482.73354. [DOI] [PubMed] [Google Scholar]
- 11.LeBrun DP, Kamel OW, Cleary ML, Dorfman RF, Warnke RA. Follicular lymphomas of the gastrointestinal tract. Pathologic features in 31 cases and bcl-2 oncogenic protein expression. Am J Pathol. 1992;140(6):1327–35. [PMC free article] [PubMed] [Google Scholar]
- 12.Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103(1):275–82. doi: 10.1182/blood-2003-05-1545. [DOI] [PubMed] [Google Scholar]
- 13.Shukla K, Patel T, Shukla J, Palanki S. Primary gastrointestinal lymphoma--a clinicopathologic study. Indian J Pathol Microbiol. 2007;50(2):296–9. [PubMed] [Google Scholar]
- 14.Al-Sayes FM. Gastrointestinal Non-Hodgkin's lymphoma: a clinico-pathological study. Saudi J Gastroenterol. 2006;12(3):118–22. doi: 10.4103/1319-3767.29751. [DOI] [PubMed] [Google Scholar]