

Abstract
Background:
Fetus in fetu is a rare congenital anomaly in which malformed fetus grows within the body of its twin. It is almost always detected as an abdominal mass in infancy. It is a parasitic twin of a diamniotic, monozygotic twin. It should be differentiated from teratoma which has no axial arrangement and has got definite malignant potential. Herein, we present a case of a two-month old female infant and review the literature. Although fetus in fetu is a rare condition, correct diagnosis using imaging can be made before surgery. It should be considered as a differential diagnosis for lump abdomen especially in infants. Complete excision is curative.
Keywords: Fetus in Fetu, Teratoma, Twin
INTRODUCTION
Fetus in fetu is a rare disorder. Its pathogenesis and differentiation from teratoma have been well established. We present the diagnosis and management of a case of fetus in fetu in a two-month old female infant.
A fetus in fetu is monochorionic-diamniotic, monozygotic twin of its bearer. It is usually intraperitoneal or retroperitoneal but may also present in scrotum, or in cranial cavity.[1] It is usually surrounded by a membrane analogous to amniotic sac and supplied by a single feeding vessel. A true placenta is usually absent. Absence of an independent circulatory system explains the subsequent growth retardation. Developmentally speaking, it has gone through the stage of primitive streak which is why it has vertebral body and organ arranged around axis. This differentiates it from fetiform teratoma. Fetus in fetu is usually malformed because of pressure exerted by the host organ.[2] This pathology is rare and the incidence is 1 per 500,000 births.[3] Fetus in fetu is a rare condition with less than 200 cases reported in the world to the best of our knowledge.[4] The present study is an effort to present a rare case of fetus in fetu with review of the available literature.
CASE REPORT
A two month-old girl was admitted to New Medical College Hospital, Kota, India in January 2011. Her parents complained about a gradually increasing lump in her right upper abdomen since birth which was extending up to the right iliac fossa. There was no history of maternal illness, exposure to radiation, or drug intake during pregnancy. There was no family history of multiple pregnancies. There was no other gastrointestinal or genitourinary symptom. At clinical examination, a bulky, firm, rounded mass of 10×12 cm2 was palpated in the right hypochondrium. The plain abdominal radiograph revealed a right-upper quadrant mass containing calcified densities identifiable as fetal parts (Figure 1). Intravenous urography showed a retroperitoneal extra renal mass. Ultrasound examination and abdominal computed tomography revealed a large mass with cystic and solid calcified components in the retroperitoneum.
Figure 1.
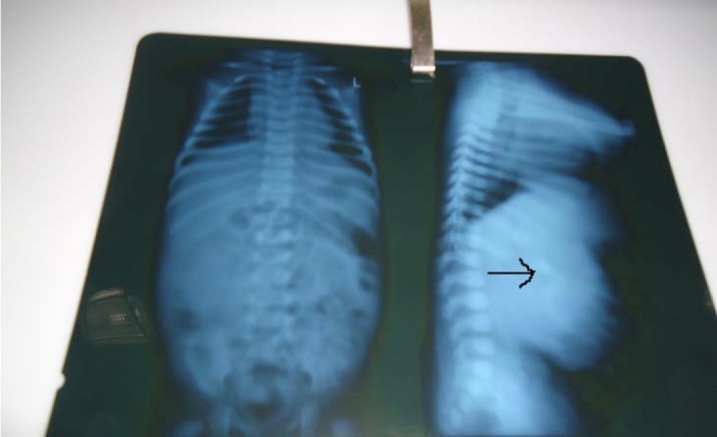
Radiograph showing fetus skeleton inside the abdomen of a 2-month old infant
Laparotomy was performed through a transverse supraumbilical incision. At surgery, a thin-walled cystic mass was found in the retroperitoneal region which compressed the inferior vena cava and medially displaced the duodenum. The tumor was entirely enveloped by a saclike capsule with an umbilical cord (Figure 2) which connected the mass to the branch of abdominal aorta. After ligation and section of the cord, the mass was easily and completely removed (Figure 3). By opening the capsule, a fetiform structure floating in yellowish fluid was observed. Symmetrical, well-developed lower limbs with structures resembling toes were present bilaterally. Upper limbs were also present, but were rudimentary in form. A further radiograph confirmed these observations. Histopathological examination revealed the presence of brain tissue, gut-like structures, fingers, and limbs. The mass was finally confirmed as fetus in fetu.
Figure 2.

Encapsulated fetus dissecting out of the abdomen of the infant
Figure 3.

Fetus in fetu
DISCUSSION
Fetus-in-fetu is a usually single, however possibly multiple, aberration of monozygotic diamniotic twinning in which unequal division of the totipotent inner cell mass of the developing blastocyst leads to the inclusion of a smaller cell mass within a maturing sister embryo.[5] Thakral et al.[6] reported equal male and female prevalence but Patankar et al.[7] and Federici et al.[8] noted a 2:1 male predominance. The common presentation of fetus in fetu is mass most commonly in the abdomen, almost 80% in the retroperitoneum.[9] The fetus in fetu produces symptoms due to mass effect leading to distention, difficulty in feeding, vomiting, jaundice, urinary retention.
In this study, during the surgery, the fetus was found to be surrounded by a capsule that grossly resembled a fetal membrane. It contained a variable amount of fluid and was connected by a peduncle to a vascular structure of the host twin. Preoperative diagnosis is possible with computed tomography and pre- or postnatal ultrasonography. Plain abdominal X-ray may be helpful in diagnosis. In half of the cases, X-ray shows the vertebral column and axial skeleton. Though a rare anomaly, fetus in fetu can be identified radiologically in the preoperative period.[10] Radiological differential diagnosis includes teratoma and meconium pseudocyst.[11] Maternal and host serum alpha fetoprotein levels may also be raised.
Pathological controversy arises during differentiation of fetus in fetu from a mature or well organized teratoma. According to Willis,[12] the presence of axial skeleton with vertebral axis and an appropriate arrangement of other limbs and organs goes more in favor of fetus in fetu. Consistent with the theory of Willis, in our case, the vertebral column was detected by the pathologist. It was radio-opaque as it was relatively calcified. However, review of literature showed that in about 9% of cases of fetus in fetu, no vertebral column was found even on pathological examination.[13] Therefore, Gonzalez-Crussi suggested fetus in fetu to be applied to any structure in which the fetal form has a highly developed organogenesis or to the presence of vertebral axis. Our case did not fall in the first category as we observed the vertebral column in our fetus in fetu. On the other hand, teratoma is an accumulation of pluripotent cells in which there is neither organogenesis nor vertebral segmentation.[14] Another important aspect of fetus in fetu is that they never become malignant whereas teratoma is known to become malignant.
Treatment of fetus in fetu is essentially surgical and excision gives complete recovery.[8] In our case, we completely resected the mass with no subsequent complication to the best of our knowledge. It is necessary to keep the child in follow-up and surveillance as malignant recurrence has also been described.
CONCLUSIONS
Fetus in fetu is a rare and interesting entity that typically presents as an abdominal mass in infancy or early childhood. It can be diagnosed in the preoperative period. Complete excision of mass is curative and confirmatory. Though a rare entity, it should be kept in mind as a differential diagnosis for lump abdomen in infancy and early childhood and should be well differentiated from teratoma which a common variant.
ACKNOWLEDGMENTS
We certify that this case report has not been previously published, nor is it under consideration by another journal. The authors have read this report thoroughly and to ensure honest work.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Sutthiwan P, Sutthiwan I, Tree-trakan T. Fetus in fetu. J Pediatr Surg. 1983;18(3):290–2. doi: 10.1016/s0022-3468(83)80105-5. [DOI] [PubMed] [Google Scholar]
- 2.Du Plessis JP, Winship WS, Kirstein JD. Fetus in fetu and teratoma. A case report and review. S Afr Med J. 1974;48(50):2119–22. [PubMed] [Google Scholar]
- 3.Hopkins KL, Dickson PK, Ball TI, Ricketts RR, O’Shea PA, Abramowsky CR. Fetus-in-fetu with malignant recurrence. J Pediatr Surg. 1997;32(10):1476–9. doi: 10.1016/s0022-3468(97)90567-4. [DOI] [PubMed] [Google Scholar]
- 4.Arlikar JD, Mane SB, Dhende NP, Sanghavi Y, Valand AG, Butale PR. Fetus in fetu: two case reports and review of literature. Pediatr Surg Int. 2009;25(3):289–92. doi: 10.1007/s00383-009-2328-8. [DOI] [PubMed] [Google Scholar]
- 5.Lewis RH. Fetus in fetu and retroperitoneal teratoma. Arch Dis Child. 1960;36:220–6. doi: 10.1136/adc.36.186.220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Thakral CL, Maji DC, Sajwani MJ. Fetus-in-fetu: a case report and review of the literature. J Pediatr Surg. 1998;33(9):1432–4. doi: 10.1016/s0022-3468(98)90029-x. [DOI] [PubMed] [Google Scholar]
- 7.Patankar T, Fatterpekar GM, Prasad S, Maniyar A, Mukherji SK. Fetus in fetu: CT appearance—report of two cases. Radiology. 2000;214(3):735–7. doi: 10.1148/radiology.214.3.r00mr32735. [DOI] [PubMed] [Google Scholar]
- 8.Federici S, Ceccarelli PL, Ferrari M, Galli G, Zanetti G, Domini R. Fetus in fetu: report of three cases and review of the literature. Pediatr Surg Int. 1991;6(1):60–5. [Google Scholar]
- 9.Tada S, Yasukochi H, Otaki C, Fukuta A, Takanashi R. Fetus in fetu. Br J Radiol. 1974;47(554):146–8. doi: 10.1259/0007-1285-47-554-146. [DOI] [PubMed] [Google Scholar]
- 10.Luzzatto C, Talenti E, Tregnaghi A, Fabris S, Scapinello A, Guglielmi M. Double fetus in fetu: diagnostic imaging. Pediatr Radiol. 1994;24(8):602–3. doi: 10.1007/BF02012747. [DOI] [PubMed] [Google Scholar]
- 11.Majhi AK, Saha K, Karmakar M, Sinha KK, Sen A, Das S. Fetus in fetu--a mystery in medicine. ScientificWorldJournal. 2007;7:252–7. doi: 10.1100/tsw.2007.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Willis RA. The borderland of embryology and pathology. 2nd ed. London: Butterworths Washington DC; 1962. pp. 442–46. [Google Scholar]
- 13.Gonzalez-Crussi F. Extragonadal teratomas (Atlas of tumor pathology) Washington, DC: Armed Forces Institute of Pathology; 1982. [Google Scholar]
- 14.Kim OH, Shinn KS. Postnatal growth of fetus-in-fetu. Pediatr Radiol. 1993;23(5):411–2. doi: 10.1007/BF02011978. [DOI] [PubMed] [Google Scholar]