

Abstract
The left eye of a 65-year-old male was blind due to optic atrophy and only seeing eye had also dry type age-related macular degeneration. An anterior ischemic optic neuropathy developed in the better seeing eye. Vision recovered in the blind eye in a short time after losing the better eye. Gaining some vision in a blind eye may be an adaptation of visual pathway in such patients.
Keywords: Optic atrophy, optic neuropathy, visual recovery
INTRODUCTION
Recovery from blindness is rare. A few cases have been reported who had significant visual improvement in the blind eye only after losing vision in the seeing better eye. These include age-related macular degeneration, amblyopia, and bilateral geographic atrophy.[1–6] Visual recovery of a blind eye from optic atrophy is very rare in the current literature.[7–9] Here we report on a case, to our knowledge for the first time, visual recovery of a blind eye with optic atrophy following sudden loss of vision in the seeing eye because of an acute anterior ischemic optic neuropathy.
CASE REPORT
The patient was a 65 years old man with hypertension who had been monitored for dry age-related macular degeneration for the last two years in ophthalmology department of University Hospital, Kırıkkale, Turkey, 2009. He also had optic atrophy due to anterior optic neuropathy in the left eye diagnosed two years previously. Visual acuities were 3/10 on the right and count fingers at 3 m on the left at his last visit. The patient presented with sudden onset of painless visual loss in the right eye. He did not complain of headache, scalp tenderness, jaw claudication, or any neurologic symptoms.
Best corrected visual acuities were hand movements and count fingers at 3 m right and left, respectively. Intraocular pressure measurements were normal. He was bilaterally pseudophakic. He had macular pigmentary disturbance predominantly in the right eye. On neuro-ophthalmic examination, the right eye had afferent pupillary defect with complete loss of color vision. The optic disc was swollen and hyperemic in the right eye and pale in the left [Figures 1a and b]. He had inferior altitudinal visual field defect on Goldmann visual field testing. Computed tomographies of orbit and brain revealed only age-related changes. Pattern visual evoked response demonstrated a conduction defect in the right eye. Hematological and biochemical investigations revealed no pathological findings.
Figure 1.
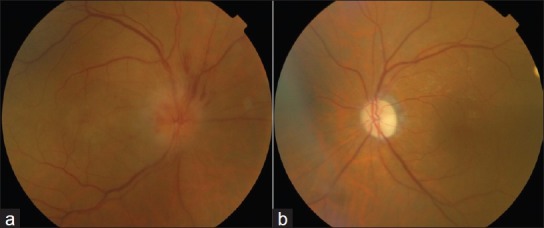
(a) Funduscopic examination revealed hyperemic and swollen optic disc with small hemorrhages in the right eye ( b ) Pale and atrophic optic disc in the left eye
The patient was decided to be followed with the diagnosis of anterior optic neuropathy in the light of these findings without any medications. At the one week's visit, the blind eye had visual acuity of 2/10. The right eye was the same. On examination, there was not any significant change when compared with the previous findings. Two weeks later, the left eye came to the same level as the right eye was before the visual loss (3/10). Optic disc oedema was minimal. Visual acuity at six months was 3/10.
DISCUSSION
It has been already known that eyes which suffered from optic neuropathies caused by trauma, neurological disorders, such as multiple sclerosis and Leber's hereditary optic neuropathy, may soon recover useful vision.[1–4] But it is not common to see such an improvement in a blind eye with optic atrophy caused by ischemic optic neuropathy.[1–5] The rare cases with visual recovery from optic atrophy include traumatic optic neuropathy, optic glioma, and tuberculum sellae meningioma.[7–9]
Indeed, no treatment has been shown to be efficacious for anterior ischemic optic neuropathy yet, while approximately half of the nonarteritic ischemic optic neuropathy patients gain three or more lines within six months of event.[2,4]
When optic disc loses its normal healthy fibers, it is relieved to as optic atrophy. This may result from injury to any portion of the visual pathway. It is the end stage appearance of an optic nerve damage for an eye. Observations in primates have suggested that signals including colors and forms are communicated to the visual cortex from the parvocellular geniculate subdivisions and these pathways are less prone to damage when optic atrophy is present.[10] Retinal ganglion cells subserving centrally located macular function may be spared even in the presence of significant optic atrophy.[11]
Bissell et al.[5] have noted visual recovery from macular geographic atrophy, this is the first case to report a visual recovery in an optic atrophy disease after losing the better seeing eye acutely. Recovery from macular disease has been explained by extrafoveal fixation, but it is not easy to find a relationship between visual improvement and optic atrophy. Animal studies have shown that monocular deprivation in adults may result in decreasing the acuity of the deprived pathway and improving the acuity of the nondeprived way.[12] In another study, unilaterally enucleated participants showed better letter recognition in comparison to normally sighted controls viewing monocularly.[13] In the light of these data, cortical response to monocular visual deprivation due to optic neuropathy may have resulted in with the reorganization of central and/or peripheral mechanisms including still viable cells or removal of binocular inhibitory interactions along the visual pathway on the blind side. Some aspects of visual ability in the remaining eye seem to be enhanced by the loss of binocularity as in this case.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Mashima Y, Sato EA, Ohde H, Oguchi Y. Macular nerve fibers temporal to fovea may have a greater potential to recover function in patients with Leber's hereditary optic neuropathy. Jpn J Ophthalmol. 2002;46:660–7. doi: 10.1016/s0021-5155(02)00562-2. [DOI] [PubMed] [Google Scholar]
- 2.Mathews MK. Nonarteritic anterior ischemic optic neuropathy. Curr Opin Ophthalmol. 2005;16:341–5. doi: 10.1097/01.icu.0000188361.52166.93. [DOI] [PubMed] [Google Scholar]
- 3.Buono LM, Foroozan R. Perioperative posterior ischemic optic neuropathy: Review of the literature. Surv Ophthalmol. 2005;50:15–26. doi: 10.1016/j.survophthal.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 4.Balcer LJ, Galetta SL. Treatment of acute demyelinating optic neuritis. Semin Ophthalmol. 2002;17:4–10. doi: 10.1076/soph.17.1.4.10287. [DOI] [PubMed] [Google Scholar]
- 5.Bissell AJ, Yalcinbayir O, Akduman L. Bilateral geographic atrophy: Spontaneous visual improvement after loss of vision in the fellow eye. Acta Ophthalmol Scand. 2005;83:514–5. doi: 10.1111/j.1600-0420.2005.00441.x. [DOI] [PubMed] [Google Scholar]
- 6.Fronius M, Bachert I. Spontaneous improvement of visual acuity in adult amblyopia after functional loss in the non-amblyopic eye? Klin Monbl Augenheilkd. 2009;226:634–9. doi: 10.1055/s-0028-1109374. [DOI] [PubMed] [Google Scholar]
- 7.Gall C, Fedorov AB, Ernst L, Borrmann A, Sabel BA. Repetitive transorbital alternating current stimulation in optic neuropathy. NeuroRehabilitation. 2010;27:335–41. doi: 10.3233/NRE-2010-0617. [DOI] [PubMed] [Google Scholar]
- 8.Chiaretti A, Falsini B, Servidei S, Marangoni D, Pierri F, Riccardi R. Nerve growth factor eye drop administration improves visual function in a patient with optic glioma. Neurorehabil Neural Repair. 2011;25:386–90. doi: 10.1177/1545968310395601. [DOI] [PubMed] [Google Scholar]
- 9.Oyama H, Kito A, Maki H, Hattori K, Noda T, Wada K. Postoperative recovery from unilateral blindness caused by tuberculum sellae meningioma. Nagoya J Med Sci. 2012;74:181–7. [PMC free article] [PubMed] [Google Scholar]
- 10.Livingstone M, Hubel D. Segregation of form, color, movement, and depth: Anatomy, physiology, and perception. Science. 1988;240:740–9. doi: 10.1126/science.3283936. [DOI] [PubMed] [Google Scholar]
- 11.Trobe JD, Glaser JS, Cassady JC. Optic atrophy.Differential diagnosis by fundus observation alone. Arch Ophthalmol. 1980;98:1040–5. doi: 10.1001/archopht.1980.01020031030003. [DOI] [PubMed] [Google Scholar]
- 12.Fischer QS, Graves A, Evans S, Lickey ME, Pham TA. Monocular deprivation in adult mice alters visual acuity and single-unit activity. Learn Mem. 2007;14:277–86. doi: 10.1101/lm.392107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Reed MJ, Steeves JK, Kraft SP, Gallie BL, Steinbach MJ. Contrast letter thresholds in the non-affected eye of strabismic and unilateral eye enucleated children. Vision Res. 1996;36:3011–8. doi: 10.1016/0042-6989(96)00019-3. [DOI] [PubMed] [Google Scholar]