

Abstract
Despite widespread intervention efforts to curtail the spread of HIV, heterosexual transmission of HIV continues to drive the HIV/AIDS epidemic in the United States, especially among women. Research has shown that knowledge about HIV and AIDS is relatively great, even among persons who engage in high rates of risky sexual behaviors. This begs the question: What characteristics underlie and are predictive of involvement in unprotected sex? The objective of this paper is to examine the factors that are associated with engaging in unprotected sex in a population of urban, at-risk, heterosexually-active women. Conceptually, the research is guided by the notion of understanding risk and, theoretically, by the Theory of Gender and Power.
Face-to-face structured interviews were conducted with 178 sexually active adult at-risk heterosexual women in Atlanta, Georgia. Street outreach efforts were used to identify potential study participants, and ethnographic mapping and targeted sampling procedures guided the recruitment process.
Using a multivariate path analysis approach, three factors–marital status, having two drug-abusing parents, and negative attitudes toward condom use–were identified as predictors of unsafe sex. Further exploration of the latter measure yielded two factors that were statistically-significant multivariate predictors of attitudes toward using condoms: age and self-esteem level. Structural equation modeling was used to assess the fit of a risk-prediction model containing all of these measures, and it was shown to be supported quite strongly by the data.
Keywords: HIV/AIDS, risk behaviors, women, unsafe sex, condom use, attitudes toward condom use
Overview
As time has elapsed, the “changing face” of the HIV/AIDS epidemic in the United States has led to substantial increases in the spread of HIV via heterosexual transmission. This route of transmission accounted for 13.7% of all new AIDS diagnoses in 1996–1997 but had increased to 15.6% of all AIDS diagnoses made between 1998 and 2001, and 18.9% of those made during 2005 and 2006, and 19.2% of those made during the most recent reporting period (Centers for Disease Control and Prevention [CDC], 2009, 2005, 2000, 1998). African American women (who comprised the large majority of the participants in the present study) in general and those residing in the southeastern region of the United States in particular have been affected especially significantly by the heterosexual transmission of HIV and other sexually transmitted infections in recent years (CDC, 2009). This is true despite extensive risk reduction interventions targeting risky sexual practices and extensive programs targeting African American women (Gilbert & Wright, 2003; Sterk, 2002). A number of programs have focused their efforts on changing risky sexual and/or drug-using behaviors, particularly among users of crack cocaine and/or injected drugs (Hoffman et al., 1999; Sterk, 2002). Although many of these intervention endeavors have yielded very positive results, researchers continue to discover high rates of unsafe sex among these populations.
In light of these findings, the present study aims to identify the factors that predict unsafe sexual practices in one specific population of at-risk heterosexual adult women. In this paper, the designation of women being at-risk is based on a variety of demographic and background characteristics (e.g., low socioeconomic status, low educational attainment, high rates of criminal involvement, substance abuse histories), neighborhood conditions (e.g., living in drug-infested neighborhoods), and access to resources (e.g., lacking adequate medical care, having no health insurance) that place them at an elevated risk for a variety of health-related problems. In these analyses, we consider a variety of demographic variables, background and experiences measures, childhood maltreatment experiences, psychosocial functioning variables, and substance use-related items as potential influences on women’s likelihood of engaging in unprotected sex.
Regarding demographic characteristics and condom use among women, a few studies have reported on a relationship between age and condom use (Cerwonka, Hansen, & Isbell, 2000; Crosby, Meyerson, & Yarber, 1999). Some research has suggested that Caucasians are less likely than other racial groups to use condoms (DiIorio, Soet, & Dudley, 1998; Graves & Hines, 1997). Married persons or those living with a partner tend to use condoms less than their peers whose marital status is something other than married (Booth, 1995; Crosby, Meyerson, & Yarber, 1999). Living in a rural area (versus an urban area) has also been associated with less condom use (Crosby, Meyerson, & Yarber, 1999). Finance-related considerations also appear to play a role in women’s use of sexual protection, with research showing that being financially dependent or interdependent upon one’s sexual partner relates to less condom use (Crosby, Meyerson, & Yarber, 1999; Sherman & Latkin, 2001).
On the subject of psychological and psychosocial factors and condom use, higher rates of sexual protection have been associated with having better coping skills and higher levels of self-esteem (Hobfall & Schroeder, 2001; McNair, Williams, & Carter, 1998). Conversely, depression has been shown to be linked with a decreased likelihood of using condoms (Urato et al., 2001). A number of studies have shown that greater condom use is associated with having positive attitudes toward using condoms (e.g., Bazargan et al., 2000; Organista et al., 2000) and higher levels of condom use self-efficacy (Longshore et al., 1998; Organista et al., 2000).
A variety of relationship characteristics have also been examined for their impact upon women’s condom use behaviors. Studies have shown that the use of sexual protection is greater among women who: have multiple sex partners (Bazargan et al., 2000), have better condom-related negotiation skills (Bazargan et al., 2000; Monahan, Rothspan, & Miller, 1997; Wingood & DiClemente, 1998), have been involved with a partner for a shorter period of time (Civic, 1999; Crosby, Meyerson, & Yarber, 1999), engage in more communication with their partners (Koch et al., 1999; Monahan, Rothspan, & Miller, 1997), and those who have a history of relationship infidelity (Cerwonka, Hansen, & Isbell, 2000). Women’s experiences dealing with HIV and HIV-related issues also may affect their decisions regarding condom use or nonuse. For example, researchers have reported that being HIV-positive and/or knowing people who have AIDS leads many women to use condoms more frequently (Organista et al., 2000; Sherman & Latkin, 2001).
Finally, a number of studies have reported a link between substance use and sexual protection. For example, the more women use alcohol, the less likely they are to use condoms (Graves & Hines, 1997; McNair, Williams, & Carter, 1998; Wingood & DiClemente, 1998). Similarly, crack use has been associated with diminished sexual protection, particularly as both the frequency and intensity of crack use increase (Hoffman et al., 1999). The severity of women’s drug-related problems has also been shown to be related to their use of condoms, with condom use declining as drug problem severity increased (Urato et al., 2001). Parental substance abuse during one’s formative years has also been linked with an increased risk for HIV risk taking among adult women (Dillon, De La Rosa, Schwartz, Rojas, Duan, & Malow, 2010; Mullings, Marquart, & Hartley, 2003).
In the present study, we focus on predictors of unsafe sexual practices in a population of at-risk women. We consider the relevance of a variety of demographic variables, background and experiences items, childhood maltreatment measures, psychosocial functioning variables, and substance use-related items. Multivariate analyses are undertaken in an effort to determine which factors predict women’s involvement in unprotected sex.
Guiding Conceptual Construct and Theoretical Approach
A guiding conceptual construct inherent in the present study is that of “risk.” Defining risk and understanding its multiple meanings poses challenges, especially as those definitions are likely to change over time (Lupton, 1999). Risk is related to threat and danger and, at times, the reduction of one risk may lead to increases in other risks. For example, a woman who proposes consistent condom use with a steady partner may be reducing her risk for HIV but she also may be increasing her risk for being abused or abandoned depending upon her partner’s reaction (Sterk, 1999a). People engaging in behaviors that are known to pose HIV-related risks may choose to weigh the potential perceived risks associated with risk involvement (e.g., becoming HIV-infected, contracting hepatitis) against the potential perceived risks associated with electing not to engage in a particular behavior (e.g., angering a sex partner, estranging and/or engendering a lack of trust among one’s drug-using friends), and on that basis opt to engage in the HIV-related risk behavior because its perceived level of risk or the immediacy of the risk to be taken is deemed lower than alternative behavioral choices. Frequently, outsiders, including many persons working in the HIV intervention and prevention fields, assume that risk levels will be diminished and unsafe behaviors will be prevented if persons being targeted have sufficient knowledge about the riskiness of their behaviors. Research on the relationship between knowledge and risk practices, however, has been mixed, often showing no relationship or only a weak relationship between level of knowledge and involvement in risky practices (Dancy, 1996; Harris & Kavanagh, 1995; Silbersiepe & Hardy, 1997). This is probably because both risk perceptions and risk taking oftentimes are moderated by competing concerns or life events. Drug use is one such concern; physical safety (as addressed in the Theory of Gender and Power; see below) is another such concern; personal economic circumstances are yet another such concern.
In addition to being guided by the notion of individualized understandings of risk, from a theoretical perspective, this paper is guided by the Theory of Gender and Power. This theoretical model helps to explain why heterosexual women place themselves at risk and engage in unsafe sex despite their awareness of possible risks. Given our focus on unsafe sex, we must recognize the importance of sexual dynamics in heterosexual relationships, thereby making the Theory of Gender and Power (Connell, 1987) applicable to this work. A main thesis of this theory is that women who are in heterosexual relationships tend to have less power and be less likely to be in decision-making roles than men due to gender role expectations in society-at-large. Such power disparities may result in unsafe sex when/if women’s male partner(s) exert their power regarding the type of sex in which the couple engages. Recently, this theory has been applied to studies on HIV, specifically those involving women (Alleyne & Gaston, 2010; Mallory, Harris, & Stampley, 2009; Wingood & DiClemente, 2000).
In this paper, we present an inquiry of predictors of unsafe sexual behaviors among at- risk women whose risk factors include a variety of demographic and background characteristics (e.g., low socioeconomic status, low educational attainment, high rates of criminal involvement, substance abuse histories), neighborhood conditions (e.g., living in drug-infested neighborhoods), and limited access to resources (e.g., lacking adequate medical care, having no health insurance). In addition, we hypothesize that involvement in HIV-related sexual behaviors is driven by attitudes toward condom use (both the women’s own attitudes and those of their partners), as numerous studies have shown the latter to be predictive of the former (Lindberg, 2000; Posner et al., 2001). Since we hypothesize condom-related attitudes to play a key role in determining involvement in unprotected sex, in this paper, we also examine the predictors of condom-related attitudes. We would like to point out that even condom-related attitudes may be construed as a type of risk vis-a-vis HIV if they are oppositional to reducing risky sexual behaviors.
Method
Overview and Sample
The data for this study are part of a larger project, the Female Atlanta Study (Project FAST), conducted in the Atlanta, Georgia metropolitan area. The objectives of the study were to examine life issues and challenges, substance use, psychological and psychosocial functioning, and a variety of HIV-related risk behaviors among adult at-risk women. Building upon our guiding conceptualization of risk, in the present study, labeling someone as being at-risk was operationalized as being based on the following seven dimensions: (1) living in areas known for high rates of drug abuse (characterizing 100% of the women), (2) being either active users of illegal drugs and/or having an immediate family member who was a substance abuser (characterizing 72% of the women), (3) being impoverished (affecting 66% of the study participants), (4) lacking adequate medical care and/or health insurance (characterizing 45% of the study participants), (5) having a low education level (true for 42% of the women), (6) being unemployed or unable to work due to disability (true for 52% of the women), and (7) having a criminal history (characterizing 52% of the sample). All of the women met at least one criterion of risk and most of them (70%) met at least four of the criteria.
As Table 1 shows, most of the study participants were African American (90%), with all other racial groups (primarily Caucasian) constituting the other 10%. The women comprising this research sample tended to be on the young side (median age = 33), with most of them being aged 18–29 (44%) or 30–39 (24%). Nearly half of the study participants (49%) had never been married, compared to 30% being married or living as married and 12% being separated or divorced. Overall, the women in this sample were not well-educated, with most of them either having not completed high school (42%) or having a high school graduation or a general equivalency diploma (35%) but no education beyond that point.
Table 1.
Description of the Sample
| % of Women | |
|---|---|
| Race | |
| African American | 90.4 |
| All others | 9.6 |
| Age | |
| 18–29 | 43.8 |
| 30–39 | 24.2 |
| 40–49 | 24.7 |
| 50 or older | 7.3 |
| Marital Status | |
| Single | 49.4 |
| Married / Living as Married | 29.8 |
| Separated / Divorced | 12.4 |
| All others | 8.4 |
| Educational Attainment | |
| Less than High School | 41.6 |
| High School Graduate | 34.8 |
| At Least Some College | 23.6 |
| At-Risk Criteria | |
| Living in Drug-Infested Area | 100.0 |
| Drug User or Close Relative Who Abuses Drugs | 71.5 |
| Income at/below Poverty Level | 66.1 |
| Less than High School Education | 41.6 |
| Lacking Needed Medical Care or Having No Medical Insurance | 45.1 |
| Unemployed or Disabled | 52.4 |
| Criminal History | 51.8 |
| Met 2–3 At-Risk Criteria | 30.1 |
| Met 4–5 At-Risk Criteria | 43.0 |
| Met 6–7 At-Risk Criteria | 26.9 |
Eligibility
In order to participate in the study, in addition to being considered an at-risk woman, several other eligibility criteria also had to be met. Each woman had to live in one of the study’s catchment areas. She had to be aged 18 or older and be able to conduct her interview in English. In addition, in order to ensure that a noninstitutionalized sample was obtained, women could not be enrolled in a substance abuse treatment program, incarcerated in a prison or jail, or be living in any other institutional setting at the time of their participation. In the present study, because the focus was on unprotected sex, only sexually-active heterosexual adult women were included in the analyses reported herein. Sixty-five women were excluded because they had not had any type of sex during the 90 days prior to interview, and seven others were excluded because they self-identified as bisexual or lesbian, leaving us with a sample size of 178 at-risk women for this particular paper.
Recruitment
Using centrally-located field sites in the Atlanta area, women were recruited into the study by outreach workers who were trained in ethnographic mapping, targeted sampling, and chain referral sampling procedures (Sterk, 1999b; Watters & Biernacki, 1989). The targeted neighborhoods were chosen because of their concentration of at-risk women. These communities were “hot spots” of local drug activity characterized by frequent drug sales and widespread drug use. Within these community “hot spots,” the outreach workers targeted places where at-risk women were known to gather (e.g., laundromats, stores, playgrounds, churches, and activity centers), so as to maximize their recruitment efforts. Informed consent procedures were approved by the institutional review boards at both Georgia State University and Emory University, from which the co-investigators conducted this study. Eligible women were given the option to complete their interviews at a project field site or at a place of their choosing. Trained interviewers conducted face-to-face interviews which, on average, took two hours to complete. At the completion of the interview, each woman was paid $15 for her participation and offered referrals to local health/social service agencies, as appropriate.
Measures Used
All of the data in Project FAST were based on self-reports. The survey instrument used for the face-to-face interviews included questions assessing numerous sociodemographic characteristics, a variety of high-risk sexual behaviors, attitudes toward condom use, childhood maltreatment experiences, several measures assessing psychological and psychosocial functioning, drug use (current and past use), exposure to substance abusers in one’s family and friendship networks, relationship attributes, and HIV risk perception. The items chosen for initial consideration in the analyses were based on the findings of numerous studies indicating the relevance of these factors to understanding differences in HIV risk perceptions and HIV risk behavior practices, particularly among women.
In these analyses, the number of times having unprotected sexual relations during the 90 days prior to interview served as the main dependent variable. This measure included responses to nine questions indicating the number of times women had oral or vaginal or anal sex with a main or casual or paying partner (3 sex types × 3 partner types = 9 questions), and then multiplying each of these numbers by the proportion of times that each type of sex involved the use of a condom or another type of barrier protection. These nine values were summed to form a single measure indicating the number of times women had unprotected sex during the 90 days prior to interview (range = 0–230, mean = 21.2, s.d. = 34.9). For the sake of simplicity and clarity in the presentation of the study’s main results, we elected to combine the oral sex, anal sex, and vaginal sex measures with different partner types into a single measure assessing overall risk associated with unprotected sex. Had the different types of sex and/or the different types of sex partners (casual, main, paying) been examined and reported separately, the presentation of the analytical results would have become extremely laborious and there would have been a considerable loss of statistical power for the analyses. Therefore, we deemed it appropriate to combine these measures as has been done in this paper.
The endogenous/mediating variable, attitudes toward condom use (Brown, 1984), included nine items that were scored using a five-point Likert scale: (1) dislike using condoms due to reduced sexual pleasure, (2) partner dislikes using condoms due to reduced sexual pleasure, (3) would permit partner to use a condom if he wanted to, (4) partner would use condoms if asked to do so, (5) condoms ruin the mood, (6) condoms do not seem natural, (7) using condoms is embarrassing, (8) condoms delay orgasm and help a man last longer, and (9) partner would think person was cheating on him if asked to use a condom. Responses to these items were summed to form a single scale measure (Cronbach’s alpha = .78) that was used in the analyses done for this paper.
As alluded to above, four types of independent variables were used in these analyses: demographic variables, background and experiences measures, childhood maltreatment experiences, assessments of psychosocial functioning, and substance use-related measures. Demographic variables used included age (coded as a continuous variable), race (coded as African American or other-than-African American), educational attainment (coded as less than high school graduate, high school graduate or equivalent, and at least some college education), marital status (coded as married or living as married versus all other marital status groups), and religiosity (coded as a continuous variable based on the interaction of frequency of religious service attendance and perceived importance of religion upon one’s behaviors). These measures were included because a number of studies have shown that HIV risk behaviors differ, often quite dramatically, based on demographic characteristics such as race/ethnicity, age, marital status, homelessness, and so forth (Newcomb et al., 1998; Smereck & Hockman, 1998; Wayment et al., 2003). Childhood maltreatment variables were based on experiences prior to age 18 and were coded as “happened” or “did not happen.” Constructs examined here were assessed using items from Bernstein et al.’s (1994) Childhood Trauma Questionnaire and included sexual abuse, physical abuse, emotional abuse, neglect, and one additional measure that indicated whether or not the person had been victimized in all four of these ways. These items were included because childhood maltreatment has been shown to be relevant to HIV risk in adulthood (Bensley, Eenwyk, & Simmons, 2000; Morrill et al., 2001), especially among women. Psychological and psychosocial functioning (e.g., self-esteem, depression, anxiety, impulsivity) have also been shown in many studies to be predictive of HIV risk practices (Schroeder et al., 2001; Somlai et al., 2000; Stoskopf, Kim, & Glover, 2001) and, accordingly, are included in this study. Five such measures were examined in the present study, including self-esteem (a continuous scale measure based on Rosenberg’s (1965) self-esteem scale)(Cronbach alpha = .85), depression (a continuous scale measure based on the Depression and Anxiety Stress Scale 42 [DASS 42] developed by Lovibond & Lovibond [1995])(Cronbach alpha = .87), level of coping with everyday stresses (a continuous scale measure derived from the Ways of Coping Questionnaire [Folkman & Lazarus, 1988] (Cronbach alpha = .65), optimism about the future (a continuous scale measure derived from five items)(Cronbach alpha = .67), and assertiveness (a continuous measure derived from 13 items)(Cronbach alpha =.78). Similarly, numerous studies have shown that different types of drug use or abuse are risk factors for HIV (Broome, Joe, & Simpson, 1999; Deren et al., 2001; Roberts et al., 2003). Accordingly, five substance use or exposure to substance abusers measures were also used in the analyses. These included measures examining living with any person(s) using illegal drugs (coded yes/no), having two drug-abusing parents (coded as yes/no), the amount of alcohol used (a continuous measure constructed by multiplying the average number of drinks consumed per occasion by the number of days using alcohol during the preceding month), the amount of illegal drugs used (a continuous measure constructed by summing the quantity-frequency amount of nine different drug types), and the number of drug problems experienced (a continuous scale measure based on responses to 11 items indicating substance abuse and substance dependency, as specified in the DSM-IV [American Psychiatric Association, 1994])(Kuder-Richardson20 = .92).
Analysis
Initially, the bivariate relationships between the predictor variables and the outcome measure in question (i.e., number of times having unprotected sex or overall attitudes toward using condoms) were tested, and all variables found to be related significantly (p<.05) or marginally (.10>p>.05) to the dependent measure in question were chosen for entry into separate multivariate equations (one for the condom attitudes measure and one for the unprotected sex outcome measure). Only items that were found to contribute significantly to the overall prediction of the dependent variables were retained in the final equations. Forward selection and backward elimination approaches were used to make sure that the order of entering variables into the equations did not affect the results obtained; it did not.
As a final step in the analytical process, the findings of the multivariate analyses were subjected to a structural equation analysis. SAS’s PROC CALIS procedure was used to assess the overall fit of the model to the data. When we use this type of structural equation analysis, we look for several specific outcomes: (1) a goodness-of-fit index as close to 1.00 as possible, but no less than 0.90, (2) a Bentler-Bonett normed fit index value as close to 1.00 as possible, but no less than 0.90, (3) an overall chi-square value for the model that is statistically nonsignificant, preferably as far from attaining statistical significance as possible, and (4) a root mean square error approximation value as close to 0.00 as possible, but no greater than 0.05. If these conditions are met, then the relationships depicted are considered to indicate a good fit with the data.
In the presentation of findings below, results are reported as significant whenever p<.05.
Results
Predictors of Unprotected Sex
Table 2 presents the findings for the bivariate analyses, examining which measures were/not related to unprotected sex. Two of the demographic variables were found to be predictive of the number of times that women reported having unprotected sex. Women who were married or involved in a marital-type relationship had more than twice as much unsafe sex as their counterparts who were not married or involved in a marital-type relationship (p<.001). Also, the greater their level of religiosity, the fewer the number of times that women reported having unprotected sex (p<.10). One of the childhood maltreatment experiences measures was found to be related to the number of times women reported having unsafe sex: Those who had been neglected during their formative years reported about 50% more unprotected sex as their non-neglected peers (p<.10). Two of the psychosocial measures were identified as predictive of unprotected sex. The better women coped with everyday stresses, the fewer the number of times they engaged in unsafe sex (p<.10). Also, the more they disliked using condoms, the more unprotected sex they reported having had (p<.05). Finally, one of the substance use-related items was identified as a meaningful predictor of unprotected sex in the bivariate analyses: Women who said that both of their parents were substance abusers reported nearly three times as much unsafe sex as their counterparts who had zero or one parent abusing drugs (p<.001).
Table 2.
Bivariate Analyses for Factors Associated with Unprotected Sex
| Independent Variable | Unprotected Sex Acts | Statistical Significance |
|---|---|---|
| Demographic Measures | ||
| Age | (continuous measure) | n.s. |
| Race | ||
| African American | 20.6 | |
| All others | 19.4 | n.s. |
| Educational Attainment | ||
| Less than high school | 17.3 | |
| High school graduate | 22.4 | |
| At least some college | 23.1 | n.s. |
| Marital Status | ||
| Married or equivalent | 34.1 | |
| Not married or equivalent | 14.9 | .0003 |
| Religiosity | (continuous measure) | .06 |
| Childhood Maltreatment Experiences | ||
| Sexual Abuse | ||
| No | 19.0 | |
| Yes | 24.0 | n.s. |
| Physical Abuse | ||
| No | 15.6 | |
| Yes | 22.0 | n.s. |
| Emotional Abuse | ||
| No | 14.6 | |
| Yes | 22.5 | n.s. |
| Neglect | ||
| No | 17.2 | |
| Yes | 27.0 | .07 |
| Abused All Four Ways | ||
| No | 19.2 | |
| Yes | 24.3 | n.s. |
| Psychological / Psychosocial Functioning | ||
| Self-Esteem | (continuous measure) | n.s. |
| Depression | (continuous measure) | n.s. |
| Coping | (continuous measure) | .08 |
| Optimism about the Future | (continuous measure) | n.s. |
| Assertiveness | (continuous measure) | n.s. |
| Condom-Related Attitudes | (continuous measure) | .04 |
| Substance Use-Related Measures | ||
| Living with Substance Abuser(s) | ||
| No | 18.3 | |
| Yes | 24.8 | n.s. |
| Having Two Substance-Abusing Parents | ||
| No | 17.8 | |
| Yes | 42.7 | .0006 |
| Amount of Alcohol Use | (continuous measure) | n.s. |
| Amount of Illegal Drug Use | (continuous measure) | n.s. |
| Number of Drug Problems | (continuous measure) | n.s. |
When the items listed above were entered into a multivariate equation, three variables were found to be significant predictors of the number of times that women engaged in unprotected sex. Predictive of more unsafe sex were: (1) marital status (specifically, being married) (β = 0.29, p<.001), (2) having two drug-abusing parents (β = 0.30, p<.001), and (3) condom-related attitudes (specifically, having more negative attitudes toward condom use) (β = 0.15, p<.05). Together, these three variables explained 18.4% of the total variance in the number of times that women reported having unsafe sex.
Predictors of Condom-Related Attitudes
Table 3 presents the findings of the bivariate analyses for the factors associated with women’s attitudes toward using condoms. Of the demographic variables examined, only one, age, was found to be related to women’s condom-related attitudes. The older women were, the more opposed they tended to be toward the use of condoms (p<.001). Two of the childhood maltreatment experiences measures were linked with attitudes toward condom use. Women who had been emotionally abused (p<.10) and those who had been neglected (p<.10) during their formative years reported somewhat more negative attitudes toward using condoms than their peers who had not been emotionally abused or neglected. Four of the psychological/psychosocial measures examined were found to be related to women’s attitudes toward using condoms. More positive attitudes regarding condom use were associated with higher levels of self-esteem (p<.001), lower levels of depression (p<.05), greater levels of assertiveness (p<.01), and greater ability to cope with everyday stresses (p<.01). Finally, associations were found between condom-related attitudes and two of the substance use-related items. More negative attitudes toward using condoms were reported by women who lived with a substance abuser (p<.05) and those who experienced more problems as a result of their drug use (p<.10).
Table 3.
Bivariate Analyses for Factors Associated with Attitudes Toward Condom Use
| Independent Variable | Condom Attitude Score | Statistical Significance |
|---|---|---|
| Demographic Measures | ||
| Age | (continuous measure) | .009 |
| Race | ||
| African American | 2.55 | |
| All others | 2.50 | n.s. |
| Educational Attainment | ||
| Less than high school | 2.65 | |
| High school graduate | 2.59 | |
| At least some college | 2.29 | n.s. |
| Marital Status | ||
| Married or equivalent | 2.64 | |
| Not married or equivalent | 2.51 | n.s. |
| Religiosity | (continuous measure) | n.s. |
| Childhood Maltreatment Experiences | ||
| Sexual Abuse | ||
| No | 2.55 | |
| Yes | 2.57 | n.s. |
| Physical Abuse | ||
| No | 2.36 | |
| Yes | 2.61 | n.s. |
| Emotional Abuse | ||
| No | 2.30 | |
| Yes | 2.63 | .06 |
| Neglect | ||
| No | 2.45 | |
| Yes | 2.74 | .07 |
| Abused All Four Ways | ||
| No | 2.54 | |
| Yes | 2.59 | n.s. |
| Psychological / Psychosocial Functioning | ||
| Self-Esteem | (continuous measure) | .0001 |
| Depression | (continuous measure) | .02 |
| Coping | (continuous measure) | .003 |
| Optimism about the Future | (continuous measure) | n.s. |
| Assertiveness | (continuous measure) | .004 |
| Substance Use-Related Measures | ||
| Living with Substance Abuser(s) | ||
| No | ||
| Yes | 2.40 | |
| 2.78 | .02 | |
| Having Two Substance-Abusing Parents | ||
| No | ||
| Yes | 2.58 | |
| 2.44 | n.s. | |
| Amount of Alcohol Use | (continuous measure) | n.s. |
| Amount of Illegal Drug Use | (continuous measure) | n.s. |
| Number of Drug Problems | (continuous measure) | .08 |
These items were entered into a multivariate equation and two variables were found to be significant multivariate determinants of women’s attitudes toward condom use. Predictive of more positive attitudes toward using condoms were: younger age (β = 0.19, p<.01) and having a higher self-esteem (β = 0.30, p<.001). Combined, these variables explained 13.1% of the total variance in women’s condom-related attitude scores.
Structural Equation Analysis Results
The results obtained by the multivariate analyses just reported for unprotected sex and attitudes toward condom use were subjected to a structural equation analysis, to determine if the path model approach to studying these data is supported by the data. The results are presented in Figure 1. The structural equation analysis revealed that this way of depicting the data is an excellent representation of the interrelationships amongst the variables. The goodness-of-fit index for this model is 0.992, which is supported by the Bentler-Bonett normed fit index value of 0.961, indicating a strong overall “fit” for the data. The model’s chi-square value is 3.85 (4df), which, as hoped/strived for in structural equation analysis, is not statistically significant (p=.427) and does not approach attaining statistical significance. Finally, the root mean square error approximation has a value of 0.000.
Figure 1.
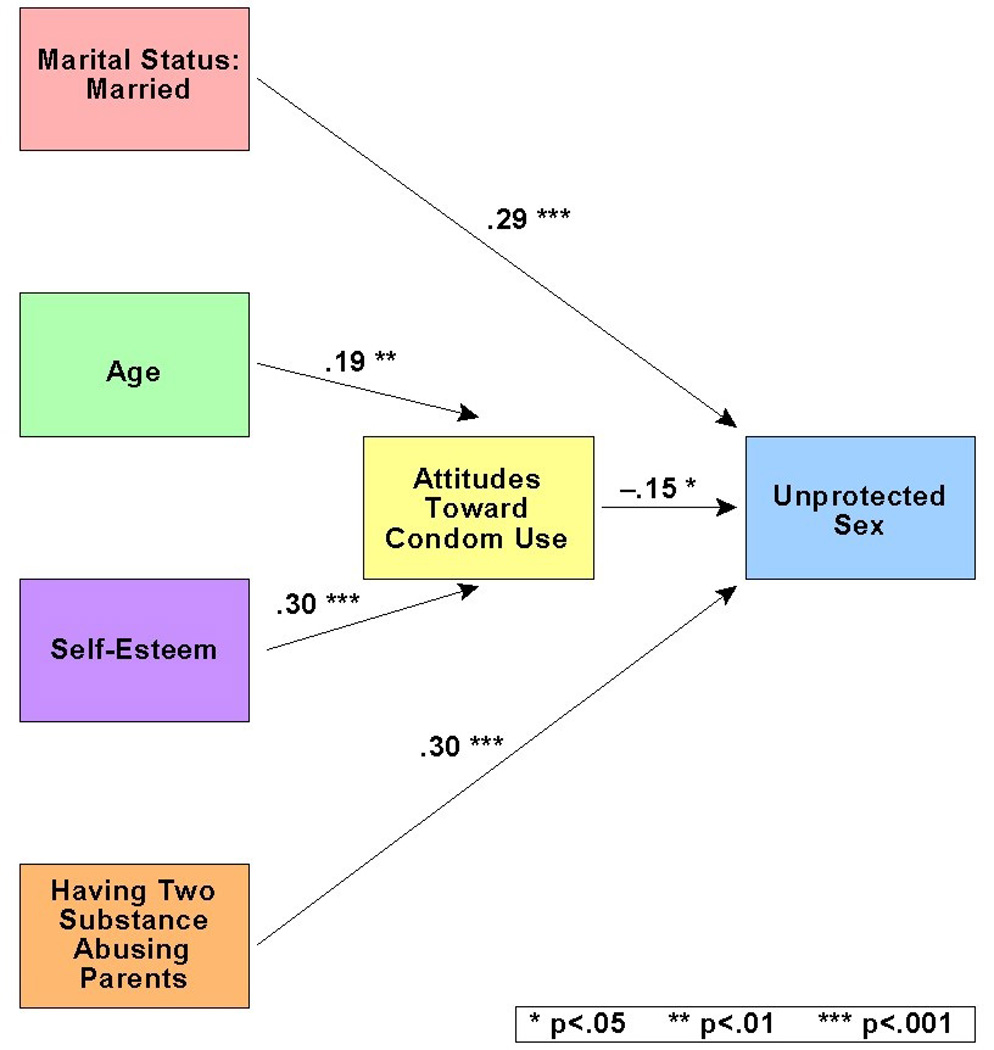
Path Model for Unprotected Sex
Discussion
This research has much to contribute to our understanding of unsafe sex practices among at-risk women. Overall, the data supported our research hypotheses and anticipated interitem relationships fairly well, with demographic variables, specific childhood maltreatment experiences, psychosocial functioning, substance use-related measures, and attitudes toward condom use all being relevant to understanding the extent to which women had unsafe sex. Ultimately, our data support the use of a multivariate model that included three statistically-significant predictors (marital status, having two drug-abusing parents, and attitudes toward condom use) that accounted for approximately one-fifth of the total variance in at-risk women’s unsafe sexual practices. We will discuss each of these predictor variables in turn.
First, our analyses revealed that married women engaged in nearly twice as much unprotected sex as their counterparts who were single, separated, divorced, widowed, or of some other marital status classification. This finding is consistent with those obtained by numerous previous research studies, showing that women are less likely to use condoms when having sex with steady partners than they are with other partner types (Lauby et al., 2000; Thomas et al., 1999). In all likelihood, this is due to issues pertaining to trust, intimacy, and power in their sexual relationships. Social exchange theorists, for example, conceptualize power as the extent to which one person’s resistance can be overcome by another person. They posit that the person with the greater amount of power in the relationship will be dominant when it comes to decision making, including decision making in the domain of sexual behaviors. The Theory of Gender and Power (Connell, 1987) expands upon this notion of power, extending its applicability to gender differences. Its supporters contend that men tend to be more powerful than women in American society, thereby leaving women in heterosexual couples with less decision-making power than their male counterparts. This lack of parity often results in decreased condom use and greater involvement in unsafe sex, because many men consider it unnecessary, undesirable, and less pleasurable to use condoms with women with whom they have on ongoing relationship (Sterk, 1999a). Interventions that can change how women feel about using condoms with their steady partners are important, as are interventions that can improve women’s comfort and ability to negotiate safer sexual practices with their steady partners. Even more important, though, are risk reduction interventions that recognize the central role that male dominance plays in many heterosexual relationships, and that can work with women and their partners to bring decision-making power and equity to both partners. Such initiatives will have the greatest chance of succeeding if they can enlist the cooperation and involvement of both partners in the couple, as published studies have shown that couples-oriented HIV interventions are quite successful when sexual risk-related matters are involved (El Bassel et al., 2001). A number of authors have discussed the potential benefits of couples-oriented HIV educational programs and the need for HIV interventions to target both members of sexually-involved couples (Polacsek et al., 1999; Sherman & Latkin, 2001; Wells et al., 1994).
Second, we discovered that more than twice as much unprotected sex was reported by women whose mothers and fathers were drug abusers compared to women who had either one parent or no parents who abused drugs. This measure was the single strongest predictor we obtained for unprotected sex, and as such, it merits considerable thought. Researchers have reported that parental drug use results in chaotic family processes and limited attention being devoted to important family matters (Conger, Patterson, & Ge, 1995; Brook et al., 2007; Dube et al., 2003; Hoffman & Cerbone, 2002), and may also entail the perpetration of various types of childhood maltreatment (Chapple, Hope, & Whiteford, 2005; Dunn et al., 2002). The impact of parental drug use/abuse has been shown to have long-lasting effects on people’s lives, lasting well into adulthood (Perkins, Elifson, & Sterk, 2010). In families in which one parent uses or abuses drugs but the other does not, the nonusing/nonabusing parent may be available to provide emotional support and structure to the family. Although having one drug using/abusing parent in the family increases the likelihood that familial chaos and dysfunction will occur, the damage may be diminished somewhat by the presence of one emotionally healthier, non-drug-using parent. But in families in which there are two drug-abusing parents, we believe that it is likely that people may suffer more psychologically and may be raised with lower senses of self-esteem and self-efficacy. In many ways, having two substance-using parents is tantamount to the effects of neglect and emotional abuse, not to mention any physical abuse that might occur during periods when one or both parents are high. Many studies have shown that people who were abused and/or neglected during childhood engage in higher rates of risky sexual behaviors in adulthood than their peers who were not abused (Bensley, Van Eenwyk, & Simmons, 2000; Hillis et al., 2001; Odonne-Paolucci, Genuis, & Violato, 2001). This finding highlights the need for HIV prevention and intervention efforts to consider not only women’s current life circumstances but also their actions and relationships in the context of their life course, including characteristics of their families-of-origin. Such an orientation recognizes the need to understand power dynamics throughout women’s lives, and how these power dynamics affect decision-making and risk behavior practices. Given the devastating effects of HIV/AIDS, it is tempting to develop intervention programs that can provide knowledge and skills to address immediate risk behavior practices (e.g., failure to use condoms consistently). It is important, however, to develop programs that adopt a more holistic approach–programs that can address factors underlying risk practices, so that the intervention effects can have a longer-lasting protective impact. In the case of women who grew up in households with two drug-abusing parents, this means not only addressing their current risk practices with specific prevention and risk-reduction information but also offering them individual mental health services to address any unresolved issues they may have as a result of growing up in dysfunctional families, family counseling services that can help them to strengthen bonds with their family members, substance abuse treatment information and recovery services to help any family members who continue to use or abuse drugs, and so forth.
Third, attitudes toward using condoms were a strong predictor of women’s use or nonuse of condoms. Women who held favorable attitudes toward condom use were far more likely than those who held negative attitudes toward condom use to engage in protected sexual relations. Not surprisingly, many scholars have obtained similar findings in their own research studies (Lindberg, 2000; Marin et al., 1998; Montoya, 1997; Posner et al., 2001; Santelli et al., 1995; Stark et al., 1998). The principal implication of this finding is that intervention programs targeting sexual risk behaviors among at-risk women need to discover ways to affect how women feel about using condoms. The more positive their feelings can be made to be with regard to using sexual protection, the greater the likelihood is that they will engage in lowered-risk practices.
Toward that end, we also identified two factors (age and self-esteem level) that were predictive of women’s attitudes toward using condoms. Each of these will be discussed briefly, in turn.
Our finding that older women were more opposed to the use of condoms than younger women were has clear implications for intervention: Older women require specialized educational and intervention efforts to alter how they think and feel about using condoms. Currently, knowledge is limited with regard to the social and cultural factors underlying older women’s attitudes toward using condoms. It is possible that, compared to their younger counterparts, older women may feel more uncomfortable talking about matters pertaining to sex, negotiating safer sex with their partners, and/or considering using condoms. Moreover, older women may not perceive themselves to be at risk for acquiring HIV (Theall et al., 2003), thereby rendering them feeling as if condoms are unnecessary for them. In addition to “traditional” HIV risk reduction interventions that enhance awareness about HIV-related safety and improve risk reduction skills, older women may benefit from woman-controlled methods of risk reduction, such as the female condom. Research needs to be done in this area. Many authors have commented on the benefits of and the continued need for HIV intervention projects to target specific age groups (Donisi et al., 1998; Richard, Bell, & Montoya, 2000; Strombeck & Levy, 1998). This is particularly important in light of research that has shown that older adults quite often do engage in risky sex (Catania et al., 1989; Feldman, 1994; Stall & Catania, 1994) and that they are less likely than their younger counterparts to use condoms (Newcomer, 1997; Schable, Chu, & Diaz, 1996).
Our data also suggest that women’s opposition to using condoms might be diminished by bolstering their self-esteem levels. In this study, it was the women with the lowest self-esteem levels who had the most antagonistic feelings about using condoms. Several researchers have found associations between self-esteem levels (or changes in self-esteem levels) and risk behavior involvement (or changes in risk behavior involvement) (Nyamathi & Stein, 1997; Paul, Stall, & Davis, 1993; St. Lawrence et al., 1997). Therefore, it seems likely that by improving women’s self-esteem levels, they will become more likely to engage in protected (rather than unprotected) sex, in great part because the elevated levels of self-esteem will correspond with more favorable attitudes toward the use of condoms.
Before concluding, we wish to acknowledge that this study has weaknesses. Whereas the quantitative data collection approach provided important insights into factors underlying women’s unsafe sex behaviors, the adoption of a qualitative orientation would have allowed for a more in-depth investigation, including an exploration of the meaning of the behaviors to the women themselves, their relationship dynamics, and the impact of the contexts in which their behaviors occurred (Sterk & Elifson, 2004). In addition, some of our quantitative measures had limitations. For example, the frequency of condom use was assessed via an ordinal scale, and a more precise measurement of condom use may have yielded somewhat different computations of the number/proportion of times engaging in unprotected sex. Another limitation is the potential of recall bias when asking about behaviors occurring during the past 30 days or the past 90 days. Likewise, the interview was lengthy and respondent fatigue/inattention may have affected responses provided to some questions asked later in the interview (which happens to be the measures of psychological and psychosocial functioning). Quantitative researchers might consider the sampling strategy to be a limitation and raise questions about the generalizability of the study findings. Additionally, in our main outcome measure of sexual risk, we have combined behaviors (oral sex, vaginal sex, anal sex) that, separately, pose quite different degrees of risk with regard to HIV transmission. It may have been preferable to examine these behaviors separately, but the relatively small sample size for this research precluded us from doing this due to statistical power-related concerns.
In summary, this study has shown that a number of factors elevate the likelihood that at- risk women will engage in unprotected sex. These are being married or involved in a marital-type relationship with someone, having two drug-abusing parents, and having negative attitudes toward condom use. Negative attitudes toward condom use, in turn, are shaped by women’s age and their self-esteem levels. All of these characteristics represent risk factors that warrant further attention by researchers, HIV educators, and HIV interventionists, and they all have direct implications for interventions aiming to reduce the chances that at-risk women will have sex without using condoms. Much of our current knowledge about women’s engagement in unsafe sex has been derived from research that has focused on individual-level characteristics. A more woman-focused approach to HIV prevention could prove useful and insightful, and would require that attention be paid to gender-specific influences, specifically relationship power and sexual inequality. The Theory of Gender and Power provides a framework that can be used to explore how women’s health is compromised by their limited power in some heterosexual relationships. The findings from the present study highlight the need for additional research in this area to be undertaken, particularly utilizing qualitative investigative approaches.
Acknowledgments
This research was supported by a grant from the National Institute on Drug Abuse (R01-DA09819).
Contributor Information
Kirk W. Elifson, Rollins School of Public Health, Emory University
Hugh Klein, Rollins School of Public Health, Emory University
Claire E. Sterk, Rollins School of Public Health, Emory University
References
- Alleyne B, Gaston G. Gender disparity and HIV risk among young Black women in college: A literature review. Journal of Women and Social Work. 2010;25:135–145. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (fourth edition) Washington DC: American Psychiatric Association; 1994. [Google Scholar]
- Bazargan M, Stein JA, Husaini BA, Bazargan SH, Kelly EM. Correlates of HIV risk-taking behaviors among African-American college students: The effect of HIV knowledge, motivation, and behavioral skills. Journal of the National Medical Association. 2000;92:391–404. [PMC free article] [PubMed] [Google Scholar]
- Bensley LS, Van Eenwyk J, Simmons KW. Self-reported childhood sexual and physical abuse and adult HIV-risk behaviors and heavy drinking. American Journal of Preventive Medicine. 2000;18:151–158. doi: 10.1016/s0749-3797(99)00084-7. [DOI] [PubMed] [Google Scholar]
- Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K, Sapareto E, Ruggiero J. Initial reliability and validity of a new retrospective measure of child abuse and neglect. American Journal of Psychiatry. 1994;151:1132–1136. doi: 10.1176/ajp.151.8.1132. [DOI] [PubMed] [Google Scholar]
- Booth RE. Gender differences in high-risk sex behaviors among heterosexual drug injectors and crack smokers. American Journal of Drug and Alcohol Abuse. 1995;21:419–432. doi: 10.3109/00952999509002708. [DOI] [PubMed] [Google Scholar]
- Broome KM, Joe GW, Simpson DD. HIV risk reduction in outpatient drug abuse treatment: Individual and geographic differences. AIDS Education and Prevention. 1999;11:293–306. [PubMed] [Google Scholar]
- Brown IS. Development of a scale to measure attitude toward the condom as a method of birth control. Journal of Sex Research. 1984;20:255–263. [Google Scholar]
- Catania JA, Stall R, Coates TJ, Pelham AO, Sacks C. Issues in AIDS primary prevention for late-middle-aged and elderly Americans. Generations: AIDS and an Aging Society. 1989 Fall;:50–54. [Google Scholar]
- Centers for Disease Control and Prevention. HIV/AIDS surveillance report. 2009;20(1):1–143. [Google Scholar]
- Centers for Disease Control and Prevention. HIV/AIDS surveillance report. 2005;16(1):1–46. [Google Scholar]
- Centers for Disease Control and Prevention. HIV/AIDS surveillance report. 2002;13(1):1–41. [Google Scholar]
- Centers for Disease Control and Prevention. HIV/AIDS surveillance report. 2000;11(1):1–45. [Google Scholar]
- Centers for Disease Control and Prevention. HIV/AIDS surveillance report. 1998;9(1):1–37. [Google Scholar]
- Cerwonka ER, Hansen CE, Isbell TR. Psychosocial factors as predictors of unsafe sexual practices among young adults. AIDS Education and Prevention. 2000;12:141–153. [PubMed] [Google Scholar]
- Chapple C, Hope T, Whiteford S. The direct and indirect effects of parental bonds, parental drug use, self-control on adolescent substance use. Journal of Child and Adolescent Substance Abuse. 2005;14:17–38. [Google Scholar]
- Civic D. The association between characteristics of dating relationships and condom use among heterosexual young adults. AIDS Education and Prevention. 1999;11:343–352. [PubMed] [Google Scholar]
- Conger R, Patterson G, Ge X. It takes two to replicate: A mediational model for the impact of parents’ stress on adolescent adjustment. Child Development. 1995;66:80–97. doi: 10.1111/j.1467-8624.1995.tb00857.x. [DOI] [PubMed] [Google Scholar]
- Connell RW. Gender and power: Society, the person and sexual politics. Stanford, CA: Stanford University Press; 1987. [Google Scholar]
- Crosby RA, Meyerson B, Yarber WL. Frequency and predictors of condom use and reasons for not using condoms among low-income women. Journal of Sex Education and Therapy. 1999;24:73–70. [Google Scholar]
- Dancy B. What African-American women know, do, feel about AIDS: A function of age and education. AIDS Education & Prevention. 1996;8:26–36. [PubMed] [Google Scholar]
- Deren S, Goldstein MF, DesJarlais DC, Richman BL, Kang SY, Flom PL. Drug use, HIV-related risk behaviors and dropout status of new admissions and re- admissions to methadone treatment. Journal of Substance Abuse Treatment. 2001;20:185–189. doi: 10.1016/s0740-5472(00)00153-7. [DOI] [PubMed] [Google Scholar]
- DiIorio C, Soet J, Dudley WN. Predictors of HIV risk among college students: A CHAID analysis. Journal of Applied Biobehavioral Research. 1998;3:119–134. [Google Scholar]
- Dillon FR, De La Rosa M, Schwartz SJ, Rojas P, Duan R, Malow RM. U.S. Latina age of sexual debut: Long-term associations and implications for HIV and drug use prevention. AIDS Care. 2010;22:431–440. doi: 10.1080/09540120903202871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donisi A, Tomasoni D, Ripamonti D, Milini P, Palvarini L, Cattane A, Paraninfo G, Casari S, Cadeo GP, Carosi G. Changing patterns of HIV transmission and better targeting for intervention strategies. International Journal of STD and AIDS. 1998;9:740–743. doi: 10.1258/0956462981921495. [DOI] [PubMed] [Google Scholar]
- Dube S, Felitti V, Dong M, Chapman D, Giles W, Anda RF. Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: The adverse childhood experiences study. Pediatrics. 2003;111:564–572. doi: 10.1542/peds.111.3.564. [DOI] [PubMed] [Google Scholar]
- Dunn M, Tarter R, Mezzich A, Vanyukov M, Kirisci L, Kirillova G. Origins and consequences of child neglect in substance abuse families. Clinical Psychology Review. 2002;22:1063–1090. doi: 10.1016/s0272-7358(02)00132-0. [DOI] [PubMed] [Google Scholar]
- Feldman MD. Sex, AIDS, and the elderly. Archives of Internal Medicine. 1994;154:19–20. [PubMed] [Google Scholar]
- Folkman S, Lazarus RS. Ways of Coping Questionnaire: Research edition. Palo Alto, CA: 1988. [Google Scholar]
- Gilbert DJ, Wright EM. Consulting Psychologists Press. African American women and HIV/AIDS: Critical responses. Westport, CT: Greenwood Publishing Group; 2003. [Google Scholar]
- Graves KL, Hines AM. Ethnic differences in the association between alcohol and risky sexual behavior with a new partner: An event-based analysis. AIDS Education and Prevention. 1997;9:219–237. [PubMed] [Google Scholar]
- Harris RM, Kavanagh KH. Perception of AIDS risk and high-risk behaviors in African-American methadone-dependent women. AIDS Education & Prevention. 1995;7:415–428. [PubMed] [Google Scholar]
- Hillis SD, Anda RF, Felitti VJ, Marchbanks PA. Adverse childhood experiences and sexual risk behaviors in women: A retrospective cohort study. Family Planning Perspectives. 2001;33:206–211. [PubMed] [Google Scholar]
- Hobfoll SE, Schroeder KEE. Distinguishing between passive and active prosocial coping: Bridging inner-city women’s mental health and AIDS risk behavior. Journal of Social and Personal Relationships. 2001;18:201–217. [Google Scholar]
- Hoffman J, Cerbone F. Parental substance use disorder and the risk of adolescent drug abuse: An event history analysis. Drug and Alcohol Dependence. 2002;66:255–264. doi: 10.1016/s0376-8716(02)00005-4. [DOI] [PubMed] [Google Scholar]
- Hoffman JA, Klein H, Crosby H, Clark D. Project Neighborhoods in Action: An HIV-related intervention project targeting drug abusers in Washington, DC. Journal of Urban Health. 1999;76:419–434. doi: 10.1007/BF02351500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koch PB, Vicary JR, Wood JM, Palmer RF. Mixing sex and alcohol in college: Female-male HIV risk model. Journal of Sex Education and Therapy. 1999;24:99–108. [Google Scholar]
- Lauby JL, Stark M, Person B, Adams J, Smith PJ. A community-level HIV prevention intervention for inner-city women: Results of the Women and Infants Demonstration Projects. American Journal of Public Health. 2000;90:216–222. doi: 10.2105/ajph.90.2.216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindberg CE. Knowledge, self-efficacy, coping, and condom use among urban women. Journal of the Association of Nurses in AIDS Care. 2000;11:80–90. doi: 10.1016/S1055-3290(06)60387-7. [DOI] [PubMed] [Google Scholar]
- Longshore D, Kowalewski M, Anglin MD, Stein JA. Psychosocial antecedents of unprotected sex by drug-using men and women. AIDS and Behavior. 1998;2:293–306. [Google Scholar]
- Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales (2nd. Ed.) Sydney, Australia: Psychology Foundation; 1995. [Google Scholar]
- Lupton D. Risk and sociocultural theory: New directions and perspectives. New York: Cambridge University Press; 1999. [Google Scholar]
- Mallory C, Harris G, Stampley C. Midlife African-American women’s protective and risky practices related to HIV. Journal of Advanced Nursing. 2009;65:1248–1258. doi: 10.1111/j.1365-2648.2009.04985.x. [DOI] [PubMed] [Google Scholar]
- Marin BV, Tschann JM, Gomez CA, Gregorich S. Self-efficacy to use condoms in unmarried Latino adults. American Journal of Community Psychology. 1998;26:53–71. doi: 10.1023/a:1021882107615. [DOI] [PubMed] [Google Scholar]
- McNair LD, Williams MK, Carter JA. Self-esteem, gender, and alcohol use: Relationships with HIV risk perception and behaviors in college students. Journal of Sex and Marital Therapy. 1998;24:29–36. doi: 10.1080/00926239808414666. [DOI] [PubMed] [Google Scholar]
- Monahan JL, Rothspan S, Miller LC. Power and intimacy: On the dynamics of risky sex. Health Communication. 1997;9:303–321. [Google Scholar]
- Montoya ID. Attitudes, norms, self-efficacy, and stage of change among out-of- treatment female crack cocaine users: A pilot study. AIDS Education and Prevention. 1997;9:424–441. [PubMed] [Google Scholar]
- Morrill AC, Kasten L, Urato M, Larson MJ. Abuse, addiction, and depression as pathways to sexual risk in women and men with a history of substance abuse. Journal of Substance Abuse. 2001;13:169–184. doi: 10.1016/s0899-3289(01)00065-7. [DOI] [PubMed] [Google Scholar]
- Mullings JL, Marquart JW, Hartley DJ. Exploring the effects of childhood sexual abuse and its impact on HIV/AIDS risk-taking behavior among women prisoners. The Prison Journal. 2003;83:442–463. [Google Scholar]
- Newcomb MD, Wyatt GE, Romero GJ, Tucker MB, Wayment HA, Carmona JV, Solis B, Mitchell-Kernan C. Acculturation, sexual risk taking, and HIV health promotion among Latinas. Journal of Counseling Psychology. 1998;45:454–467. [Google Scholar]
- Newcomer VD. Human immunodeficiency virus infection and acquired immunodeficiency syndrome in the elderly. Archives of Dermatology. 1997;133:1311–1312. [PubMed] [Google Scholar]
- Nyamathi AM, Stein JA. Assessing the impact of HIV risk reduction counseling in impoverished African American women: A structural equations approach. AIDS Education and Prevention. 1997;9:253–273. [PubMed] [Google Scholar]
- Odonne-Paolucci E, Genuis ML, Violato C. A meta-analysis of the published research on the effects of child sexual abuse. Journal of Psychology. 2001;135:17–36. doi: 10.1080/00223980109603677. [DOI] [PubMed] [Google Scholar]
- Organista KC, Bola JR, De Alba GJEG, Moran MAC, Organista PB. Predictors of condom use in Mexican migrant laborers. American Journal of Community Psychology. 2000;28:245–265. doi: 10.1023/a:1005191302428. [DOI] [PubMed] [Google Scholar]
- Paul JP, Stall R, Davis F. Sexual risk for HIV transmission among gay/bisexual men in substance-abuse treatment. AIDS Education and Prevention. 1993;5:11–24. [PubMed] [Google Scholar]
- Perkins M, Elifson K, Sterk C. Drug risk: A cross-sectional exploration of the influence of family-of-origin and current situational circumstances. Journal of Drug Issues. 2010;4:353–378. doi: 10.1177/002204261004000205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polacsek M, Celentano DD, O’Campo P, Santelli J. Correlates of condom use stage of change: Implications for intervention. AIDS Education and Prevention. 1999;11:38–52. [PubMed] [Google Scholar]
- Posner SF, Pulley LV, Artz L, Cabral R, Macaluso M. Psychosocial factors associated with self-reported male condom use among women attending public health clinics. Sexually Transmitted Diseases. 2001;28:387–393. doi: 10.1097/00007435-200107000-00005. [DOI] [PubMed] [Google Scholar]
- Richard AJ, Bell DC, Montoya ID. Age and HIV risk in a national sample of injecting drug and crack cocaine users. Substance Use and Misuse. 2000;35:1385–1404. doi: 10.3109/10826080009148221. [DOI] [PubMed] [Google Scholar]
- Roberts AC, Wechsberg WM, Zule W, Burroughs AR. Contextual factors and other correlates of sexual risk of HIV among African-American crack-abusing women. Addictive Behaviors. 2003;28:523–536. doi: 10.1016/s0306-4603(01)00255-6. [DOI] [PubMed] [Google Scholar]
- Rosenberg M. Society and the adolescent self-image. Princeton, NJ: Princeton University Press; 1965. [Google Scholar]
- Santelli JS, Davis M, Celentano DD, Crump AD, Burwell LG. Combined use of condoms with other contraceptive methods among inner-city Baltimore women. Family Planning Perspectives. 1995;27:74–78. [PubMed] [Google Scholar]
- Schable B, Chu SY, Diaz T. Characteristics of women 50 years of age or older with heterosexually acquired AIDS. American Journal of Public Health. 1996;86:1616–1618. doi: 10.2105/ajph.86.11.1616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schroeder KEE, Hobfoll SE, Jackson AP, Lavin J. Proximal and distal predictors of AIDS risk behaviors among inner-city African American and European American women. Journal of Health Psychology. 2001;6:169–190. doi: 10.1177/135910530100600207. [DOI] [PubMed] [Google Scholar]
- Sherman SG, Latkin CA. Intimate relationship characteristics associated with condom use among drug users and their sex partners: A multilevel analysis. Drug and Alcohol Dependence. 2001;64:97–104. doi: 10.1016/s0376-8716(00)00236-2. [DOI] [PubMed] [Google Scholar]
- Silbersiepe KA, Hardy AM. AIDS knowledge and risk perception of cocaine and crack users in a national household survey. AIDS Education & Prevention. 1997;9:460–471. [PubMed] [Google Scholar]
- Smereck GAD, Hockman EM. Prevalence of HIV infection and HIV risk behaviors associated with living place: On-the-street homeless drug users as a special target population for public health intervention. American Journal of Drug and Alcohol Abuse. 1998;24:299–319. doi: 10.3109/00952999809001714. [DOI] [PubMed] [Google Scholar]
- Somlai AM, Kelly JA, Heckman TG, Hackl K, Runge L, Wright C. Life optimism, substance use, AIDS-specific attitudes associated with HIV risk behavior among disadvantaged innercity women. Journal of Women’s Health and Gender-Based Medicine. 2000;9:1101–1111. doi: 10.1089/152460900446018. [DOI] [PubMed] [Google Scholar]
- St. Lawrence J, Eldridge GD, Shelby MC, Little CE, Brasfield TL, O’Bannon RE., III HIV risk reduction for incarcerated women: A comparison of brief interventions based on two theoretical models. Journal of Consulting and Clinical Psychology. 1997;65:504–509. doi: 10.1037//0022-006x.65.3.504. [DOI] [PubMed] [Google Scholar]
- Stall R, Catania J. AIDS risk behaviors among late middle-aged and elderly Americans. Archives of Internal Medicine. 1994;154:57–63. [PubMed] [Google Scholar]
- Stark MJ, Tesselaar HM, O’Connell AA, Person B, Galavotti C, Cohen A, Walls C. Psychosocial factors associated with the stages of change for condom use among women at risk for HIV and STDs: Implications for intervention development. Journal of Consulting and Clinical Psychology. 1998;66:967–978. doi: 10.1037//0022-006x.66.6.967. [DOI] [PubMed] [Google Scholar]
- Sterk C. Fast lives: Women and crack cocaine. Philadelphia: Temple University Press; 1999a. [Google Scholar]
- Sterk C. Building bridges: Community involvement in HIV and substance abuse research. Drugs and Society. 1999b;14:107–121. [Google Scholar]
- Sterk CE. The Health Intervention Project: HIV risk reduction among African American women drug users. Public Health Reports. 2002;117:s88–s95. [PMC free article] [PubMed] [Google Scholar]
- Sterk C, Elifson K. Qualitative methods in community-based research. In: Blumenthal D, DiClemente R, editors. Community based research: Issues and methods. New York: Springer; 2004. pp. 133–151. [Google Scholar]
- Stoskopf CH, Kim YK, Glover SH. Dual diagnosis: HIV and mental illness, a population-based study. Community Mental Health Journal. 2001;37:469–479. doi: 10.1023/a:1017577827658. [DOI] [PubMed] [Google Scholar]
- Strombeck R, Levy JA. Educational strategies and interventions targeting adults age 50 and older for HIV/AIDS prevention. Research on Aging. 1998;20:912–936. [Google Scholar]
- Theall K, Elifson K, Sterk C, Klein H. Perceived susceptibility to HIV among women: Differences according to age. Research on Aging. 2003;25:405–432. [Google Scholar]
- Thomas JC, Weiner DH, Earp JA, Schoenbach VS, Lansky A. Behaviors that facilitate sexual transmission of HIV and STDs in a rural community. AIDS and Behavior. 1999;3:257–267. [Google Scholar]
- Urato M, Larson MJ, Morrill AC, Kasten L. Abuse, addiction, and depression as pathways to sexual risk in women and men with a history of substance abuse. Journal of Substance Abuse. 2001;13:169–184. doi: 10.1016/s0899-3289(01)00065-7. [DOI] [PubMed] [Google Scholar]
- Watters J, Biernacki P. Targeted sampling: Options for the study of hidden populations. Social Problems. 1989;36:416–430. [Google Scholar]
- Wayment HA, Wyatt GE, Tucker MB, Romero GJ, Carmona JV, Newcomb M, Solis BM, Riederle M, Mitchell-Kernan C. Predictors of risky and precautionary sexual behaviors among single and married white women. Journal of Applied Social Psychology. 2003;33:791–816. [Google Scholar]
- Wells EA, Clark LL, Calsyn DA, Saxon AJ, Jackson TR, Wrede AF. Reporting of HIV risk behaviors by injection drug using heterosexual couples in methadone maintenance. Drug and Alcohol Dependence. 1994;36:33–38. doi: 10.1016/0376-8716(94)90007-8. [DOI] [PubMed] [Google Scholar]
- Wingood G, DiClemente R. Application of the theory of gender and power to examine HIV-related exposures, risk factors, and effective interventions for women. Health Education and Behavior. 2000;27:539–565. doi: 10.1177/109019810002700502. [DOI] [PubMed] [Google Scholar]
- Wingood GM, DiClemente RJ. The influence of psychosocial factors, alcohol, drug use on African-American women’s high-risk sexual behavior. American Journal of Preventive Medicine. 1998;15:54–59. doi: 10.1016/s0749-3797(98)00027-0. [DOI] [PubMed] [Google Scholar]