

Abstract
Pancreatic adenocarcinoma is the most common malignancy of the pancreas with high death rate. Preoperative imaging is crucial for the assessment of the disease and the planning of treatment. In this review, we discussed the common and unusual findings of pancreatic carcinoma. The common CT and MR findings include hypovascular mass, dilataion of upstream biliary and pancreatic ducts, invasion to adjacent structures and metastasis. The uncommon CT and MR findings include: a cystic mass, a mass without dilataion of upstream ducts, multiple masses or a lesion diffusively infiltrating most parts of the pancreas without distorting its configuration.
Key Words: CT, MRI, pancreatic adenocarcinoma, Magnetic resonance cholangiopancreatography (MRCP)
Introduction
Pancreatic adenocarcinoma is the most common malignancy of the pancreas with a high mortality, accounting for over 90% of all pancreatic tumors (1). Surgical resection is the only curative treatment option. However, the complication of pancreaticoduodenectomy can be as high as 40% (2,3). Therefore, the accurate characterization of pancreatic adenocarcinoma is very important for patients’ management. CT and MRI have been become the most important modalities for evaluating pancreatic lesions. However, precise diagnosis of pancreatic adenocarcinoma is not always straightforward because they frequently show atypical imaging features and many other diseases may mimic pancreatic adenocarcinoma (4). Understanding its common and uncommon CT and MRI manifestations may facilitate diagnosis and differential diagnosis of pancreatic adenocarcinoma.
CT and MRI protocols
CT and MR imaging protocol have been developed to highlight pancreas. Optimal protocol should obtain obvious contrast between pancreatic parenchyma and lesions. Oral abundant water to fill the gastrointestinal tract is routinely used at CT examination to improve the visualization of peripancreatic anatomic structures. Maximal enhancement can be obtained at pancreatic phase with 40-45 sec delay after intravenous administration of contrast agent at a rate of 3-4 mL/sec. Therefore, radiologists may prefer dual-phase protocol to get optimal enhancement of pancreas and liver due to hypo-vascular characteristics of pancreatic adenocarcinoma. Tri-phase dynamic enhanced CT had been used to characterize pancreas (Figure 1). At arterial dominated phase, most contrast materials are staying in the vascular, the enhancement of the pancreatic parenchyma is mild even though pancreas is a hyper-vascular organ. If neuroendocrine tumor is suspected or clinicians want to know whether arteries are invaded, arterial phase is necessary. Another advantage of pancreatic phase is that peripancreatic vessels, including veins, can be enhanced. This can facilitate assessment of vascular invasion. Conventional MR imaging protocol for pancreas should include T1-weighted images, T2-weighted images, Magnetic resonance cholangiopancreatography (MRCP), and dynamic enhancement with arterial phase, port vein phase, and delay phase using fast gradient recall sequence. Fat-suppress T1 weighted imaging is recommended because it can improve the dynamic contrast of pancreatic parenchyma (Figure 2). MRCP is routinely used in evaluating pancreatic adenocarcinoma to depicture morphological changes of biliary and pancreatic ducts, which has substituted diagnostic ERCP (Figure 3).
Figure 1.

Contras-enhanced CT images obtained at 25 (A), 40 (B) and 70 (C) sec delay after intravenous injection of contrast agency at a rate of 3 mL/sec and with a dose of 100 mL. Maximal contrast enhancement of pancreas is achieved at pancreatic parenchymal phase (40 sec)
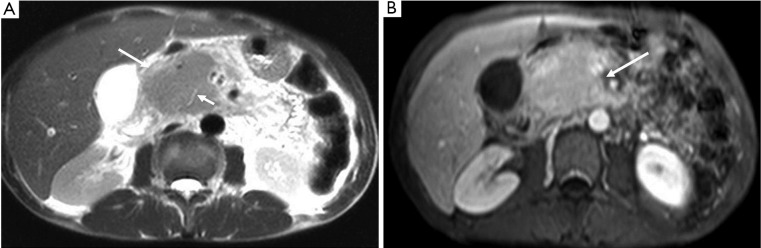
Figure 2.
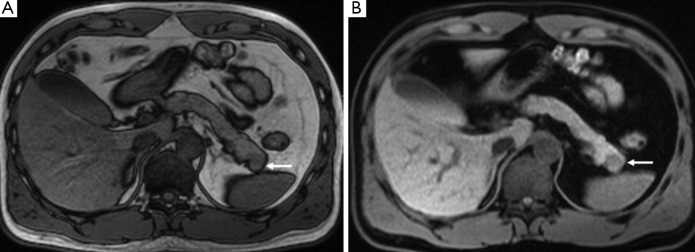
A small lesion (arrows) on the pancreatic tail is more obvious on fat-suppressed T1WI (B) than on conventional T1WI (A)
Figure 3.
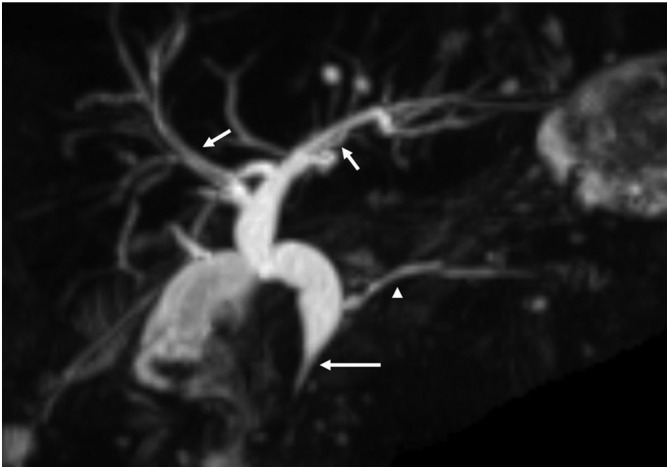
MRCP of a patient with chronic pancreatitis and pancreatic adenocarcinoma shows morphological changes of cholangiopancreatic ducts, which include a stricture (long arrow) of bile duct at the pancreatic head and dilatation of biliary ducts (short arrows) and pancreatic duct (arrowhead)
Common CT and MRI findings
Direct signs: pancreatic mass
Due to pancreatic duct origin, pancreatic adenocarcinoma often results in pancreatic duct stricture or obstruction, and forms a mass. Approximately 60% occur in the pancreatic head, with the classic clinical presentation of painless jaundice (5).
The typical CT and MRI features of pancreatic adenocarcinoma are a hypovascular infiltrative pancreatic mass, often with resultant obstruction of the pancreatic and/or common bile duct (CBD). On CT, it often manifests as a low-density mass on triple phase (arterial and portal) contrast enhanced CT. Maximal contrast between the tumor and the normal pancreas can be achieved in pancreatic and portal venous phase (Figure 4). Because pancreas is a soft organ without capsule and pancreatic adenocarcinoma is extremely invasive, pancreatic adenocarcinoma often had advanced local invasion when it was diagnosed (Figure 5).
Figure 4.
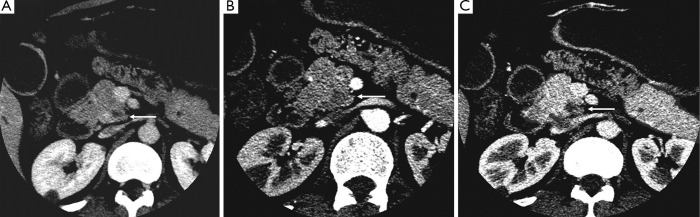
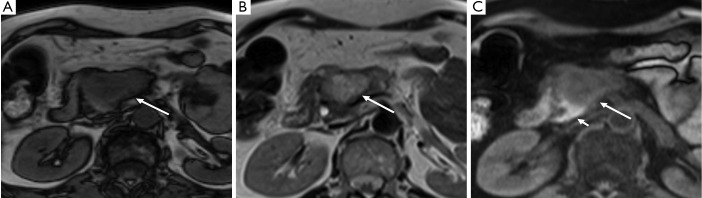
A case of pancreatic adenocarcinoma in pancreatic head. A small low enhancement nodule at the pancreatic head (arrows in A, B and C) is optimally shown on the pancreatic phase (B) and portal venous phase (C) without dilatation of the pancreatic duct, while the contrast between the tumor and the normal pancreatic parenchyma is poor in arterial phase (A)
Figure 5.
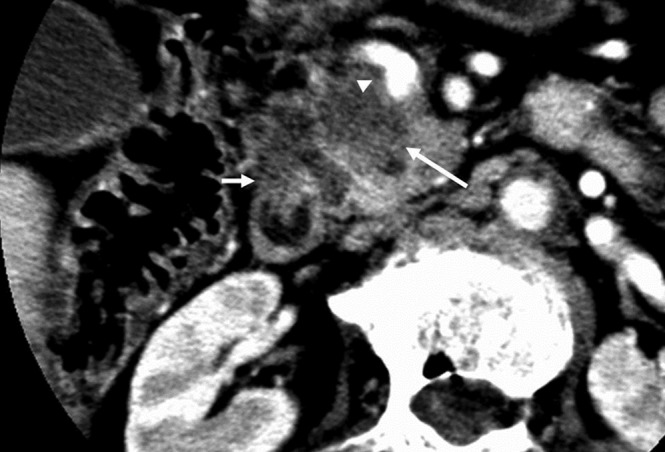
CT image at port vein phase shows a hypo-enhanced ill-demarcated mass (long arrow) at the pancreatic head in a patient with pancreatic adenocarcinoma. The mass invaded duodenum (short arrow) and superior mesenteric vein (arrowhead)
On MR, pancreatic adenocarcinoma shows a mass of hypointensity on T1-weighted image and slight hyperintensity on T2-weighted images, especially on fat-suppressed T1-weighted images (Figure 6). As with CT, dynamic-enhanced MR imaging reveals a low enhancement mass (Figure 7).
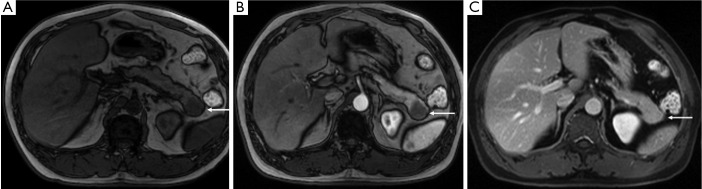
Figure 6.
Pancreatic adenocarcinoma at the pancreatic head. A. Transversal T1-weighted image shows a hypointensity mass (arrow); B. Transversal T2-weighted image shows the mass is of slight hyperintensity (arrow); C. Fat-suppressed T1-weighted image improves the contrast between tumor (long arrow) and normal pancreatic parenchyma (short arrow)
Figure 7.
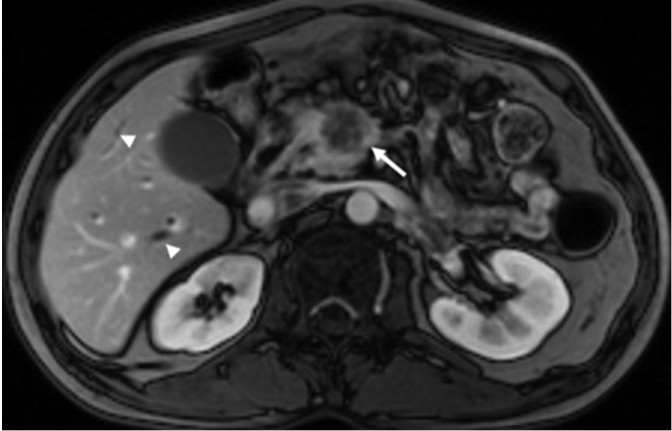
A low enhancement mass (arrow) in the pancreatic head is demonstrated at port vein phase of dynamic enhanced MR imaging. Dilatation of intrahepatic bile ducts (arrowheads) is also revealed
Indirect signs
Pancreatic adenocarcinoma frequently locates at the pancreatic head and cause dilatation of both the pancreatic and common bile duct which is called the “double duct sign” (Figures 8,9). Both CT and MR (esp. MRCP) can show “double duct sign” clearly. Rarely, the tumor in the pancreatic head stricts only CBD, and only the bile ducts are dilatated. When the tumor locates in the neck, body or tail, it causes only upstream pancreatic duct dilatation (Figure 10).
Figure 8.
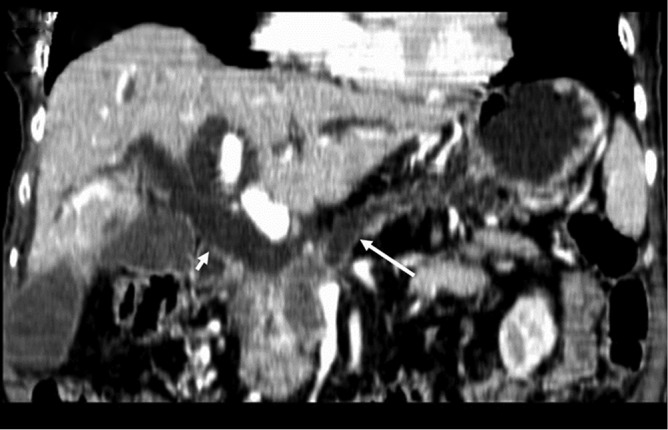
“Double duct sign” on MPR of CT. A pancreatic adenocarcinoma in the head of the pancreas results in dilatation of the pancreatic duct (long arrow) and the common bile duct (short arrow)
Figure 9.
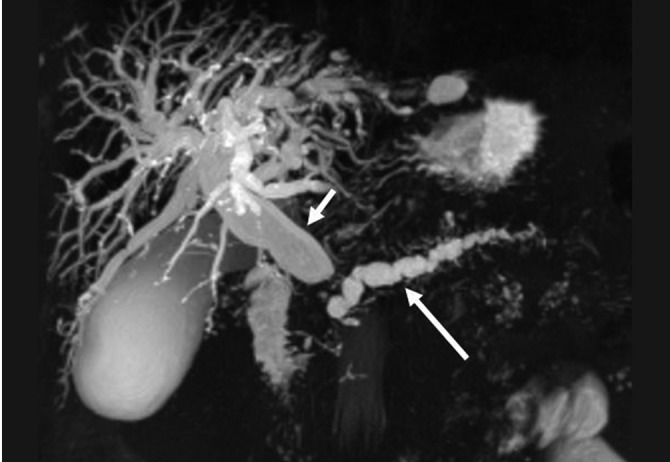
“Double duct sign” on MRCP. Both the pancreatic duct (long arrow) and the common bile duct (short arrow) are dilated due to pancreatic adenocarcinoma in the pancreatic head
Figure 10.
Upstream pancreatic duct dilatation (short arrow) due to a pancreatic adenocarcinoma (long arrow) in the body of the pancreas
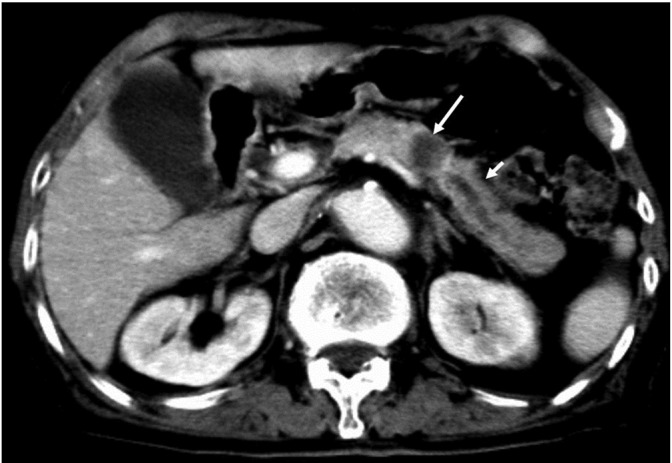
Unresectable disease is seen at presentation in 75% of patients, with metastases (mainly to the liver and peritoneum) presenting in 85% of these patients (6). Tumor invasion of adjacent organs and vessels is also common which makes the tumor unresectable (Figure 11).
Figure 11.
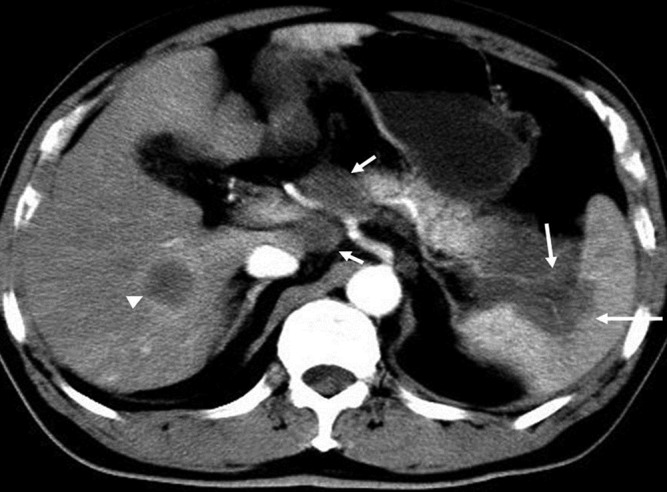
A pancreatic adenocarcinoma in the tail of the pancreas with splenic invasion and encasement of the splenic vessels (long arrows) and metastasis to the liver (arrowhead) and retroperitoneal lymph nodes (short arrows)
Uncommon radiological findings
Cystic change of pancreatic adenocarcinoma can present, which may be related to a cystic neoplastic component, necrosis, retention cysts from pancreatic ductal obstruction, or pseudocysts from pancreatitis (7) (Figure 12).
Figure 12.
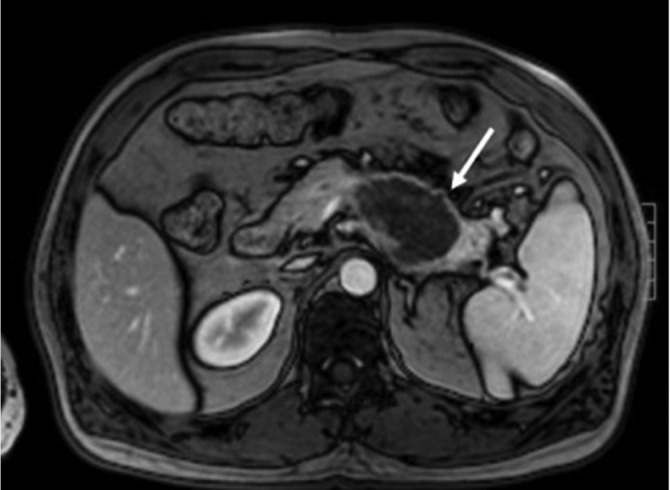
Cystic pancreatic adenocarcinoma. A unilocular cystic mass (arrow) locates in the body of the pancreas. It is difficult to be differentiated from cystic pancreatic tumors, such as mucinous cystadenoma
Sometimes, pancreatic adenocarcinoma can present as a focal mass without dilation of upstream pancreatic duct. This phenomenon can be contributed to anatomic variation of pancreatic or bile ducts. If the tumor locates in uncinate process of pancreas, it may not infiltrate bile duct and main pancreatic duct (Figure 13). Multiple lesions might be seen in pancreatic adenocarcinoma rarely (Figure 14). However, it should be differentiated from pancreatic metastasis. The history of primary tumor and the absence of pancreatic duct dilatation can help the differentiation (Figure 15). Occasionally, a pancreatic adenocarcinoma may infiltrate pancreatic parenchyma without distorting pancreatic figuration (Figure 16).
Figure 13.
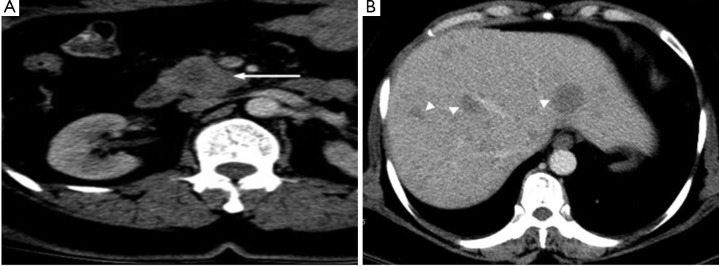
Pancreatic head adenocarcinoma (arrow) with hepatic metastasis (arrowheads) without dilation of pancreatic duct and bile duct
Figure 14.

Multifocal pancreatic adenocarcinoma. Two focal hypo-enhanced masses (arrows) are seen at the head and the tail of the pancreas respectively with sparing the body
Figure 15.

Pancreatic metastasis. A patient with known history of melanoma. Multiple hypoattenuating masses (arrow) in the pancreas without pancreatic duct dilatation. Retroperitoneal adenopathy (arrowheads) is also noted
Figure 16.

A case of diffusive infiltrative pancreatic adenocarcinoma. An infiltrative pancreatic mass (arrow) is noted in the body and the tail of the pancreas. Note the metastatic foci within the liver (arrowheads)
Pancreatic lesions mimics
Since pancreatic adenocarcinoma frequently presents as solid mass in the pancreas, it should be differentiated from solid masses in and adjacent to the pancreas. Common lesions mimic pancreatic adenocarcinoma include: chronic focal pancreatitis, solid pseudopapillary tumors, endocrine tumor of the pancreas, gastrointestinal stromal tumor (GIST) adjacent to the pancreas. Metastatic disease to the pancreas can sometimes be a diagnostic challenge.
(I) Chronic focal pancreatitis can manifest as a focal mass, often in the pancreatic head, thereby mimicking adenocarcinoma (Figure 17). The differential diagnosis between focal pancreatitis and adenocarcinoma may be difficult. Their density and signal intensity can be similar. However, nondilated or smoothly tapering pancreatic and bile ducts coursing through the mass [“duct penetrating sign” (8)], pancreatic duct irregularity, and the presence of pancreatic calcifications favor a diagnosis of focal pancreatitis (9).
Figure 17.
Chronic focal pancreatitis. A. Transversal T2-weighted image shows enlargement of the pancreatic head (long arrow). “Duct penetrating sign” is seen (short arrow); B. Transversal contrast enhanced T1-weighted image shows the enhancement of the enlarged pancreatic head being uniform
(II) Solid pseudopapillary tumors of the pancreas. This rare cystic low-grade malignancy can sometimes present as a solid mass when it is small making it mimics a small pancreatic adenocarcinoma on unenhanced CT and MR. When scanned at arterial phase, it manifests mild enhancement. However, it has gradual enhancement with time which is not seen in pancreatic adenocarcinoma (Figure 18).
Figure 18.
Solid pseudopapillary tumors of the pancreas (arrows in A, B, and C). A hypoinsensitive mass (A) in the tail of the pancreas shows little enhancement on arterial phase (B). However, it enhanced as an iso-intensitive mass on the delayed scan
(III) Neuroendocrine tumor of the pancreas frequently presents as a small mass of hypodensity on non-enhanced CT and hypointensity on non-enhanced T1WI. However, it enhances strongly on arterial phase and dilatation of the pancreas duct is usually absent (Figure19).
Figure 19.
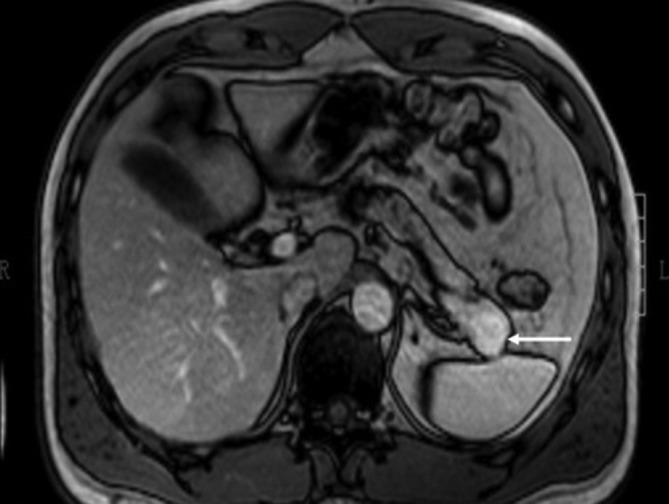
A case of neuroendocrine tumor of the pancreas. A small enhanced mass (arrow) in the pancreatic tail is demonstrated at the arterial phase of DCE-MRI
(IV) Sometimes a GIST adjacent to the pancreas can mimic a pancreatic mass (Figure 20). However, GIST has a stronger contrast enhancement than pancreatic adenocarcinoma and rarely has pancreatic duct dilatation.
Figure 20.

A duodenum GIST (arrow) mimics a pancreatic head adenocarcinoma. However, it manifests strong contrast enhancement without pancreatic duct dilatation
In conclusion, most of pancreatic adenocarcinoma shows typical manifestations on CT and MRI, which can be easy to identify and stage. However, pancreatic adenocarcinoma can demonstrate atypical appearances and several diseases may mimic pancreatic adenocarcinoma on CT and MRI. Familiarity of common and uncommon CT and MRI manifestations of pancreatic adenocarcinoma is essential to achieve the correct diagnose.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- 1.Mergo PJ, Helmberger TK, Buetow PC, et al. Pancreatic neoplasms: MR imaging and pathologic correlation. Radiographics 1997;17:281-301 [DOI] [PubMed] [Google Scholar]
- 2.Gouma DJ, van Geenen RC, van Gulik TM, et al. Rates of complications and death after pancreaticoduodenectomy: risk factors and the impact of hospital volume. Ann Surg 2000;232:786-95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Miedema BW, Sarr MG, van Heerden JA, et al. Complications following pancreaticoduodenectomy. Current management. Arch Surg 1992;127:945-9; discussion 949-50 [DOI] [PubMed] [Google Scholar]
- 4.Coakley FV, Hanley-Knutson K, Mongan J, et al. Pancreatic imaging mimics: part 1, imaging mimics of pancreatic adenocarcinoma. AJR Am J Roentgenol 2012;199:301-8 [DOI] [PubMed] [Google Scholar]
- 5.Martin DR, Semelka RC. MR imaging of pancreatic masses. Magn Reson Imaging Clin N Am 2000;8:787-812 [PubMed] [Google Scholar]
- 6.Ros PR, Mortelé KJ. Imaging features of pancreatic neoplasms. JBR-BTR 2001;84:239-49 [PubMed] [Google Scholar]
- 7.Kosmahl M, Pauser U, Anlauf M, et al. Pancreatic ductal adenocarcinomas with cystic features: neither rare nor uniform. Mod Pathol 2005;18:1157-64 [DOI] [PubMed] [Google Scholar]
- 8.Ichikawa T, Sou H, Araki T, et al. Duct-penetrating sign at MRCP: usefulness for differentiating inflammatory pancreatic mass from pancreatic carcinomas. Radiology 2001;221:107-16 [DOI] [PubMed] [Google Scholar]
- 9.Siddiqi AJ, Miller F. Chronic pancreatitis: ultrasound, computed tomography, and magnetic resonance imaging features. Semin Ultrasound CT MR 2007;28:384-94 [DOI] [PubMed] [Google Scholar]