

Abstract
Patients presenting with vague head and neck pain can lead to wide-ranging differential diagnosis. Elongation of styloid process (SP) should also be considered as one of the etiological factors for cervical pain radiating to jaws, pharyngodynia, and difficulty in swallowing. Symptomatic elongation of SP or mineralization of stylohyoid ligament is referred as Eagle's syndrome. It is a rare entity presenting with an array of symptoms like recurrent throat pain, dysphagia, otalgia, and neck pain. History and physical examination play a vital role in diagnosing this condition and further radiological investigation confirms the diagnosis. The preferred radiologic modality is 3D-computed tomography, which gives accurate information about length, angulation, type of elongation, and relation to vital structures and hence helps in execution of treatment planning. This paper describes clinical approach, imaging investigations, and management of a case of Eagle's syndrome.
Keywords: Cervical pain, computed tomography imaging, stylohyoid ligament calcification
Introduction
Watt W. Eagle first described the clinical findings of Eagle syndrome in 1937.[1] Eagle's syndrome encompasses multiple symptoms, which include pharyngodynia, dysphagia, foreign body sensation in pharynx, otalgia, headache, pain on neck rotation, and facial pain. These symptoms are produced due to elongated styloid process (SP) or calcified stylohyoid ligament exerting pressure symptoms on neurovascular structures in its vicinity. Normal length of SP varies from 2.5 cm to 3.0 cm and it is said to be elongated if its length exceeds 3.0 cm.[2] Estimated incidence shows that an average of 4% of population has elongated process, but only 4-10.3% of these individuals presents with symptoms.[3] However, the number of reported cases is underestimated because it is an incidental finding in radiographs and is usually asymptomatic. Diagnosis is supported by description of symptoms by patient, previous history of any cervical trauma and tonsillectomy, physical examination, and radiographs. Treatment includes both non-surgical and surgical approaches.
Case Report
A 24-year-old male patient referred to the department for opinion regarding radiating head and neck pain. Patient's complaints were on and off pain over neck region radiating to shoulders and arms for the past 5 years, headache and giddiness on the side to side neck movements, difficulty and pain while swallowing, and foreign body feeling in the throat. Previous history of any surgery and trauma was unremarkable. On examination, all third molars were completely erupted in proper occlusion and no abnormal finding was present on temporomandibular joint (TMJ) examination, but tenderness was present bilaterally in tonsillar fossae region on palpation. There was no evidence of any palpable mass in neck. Based on clinical findings, presumptive diagnosis of neuralgic pain and elongated SP (Eagle's syndrome) was made. Patient was preceded with a panoramic radiograph, which revealed bilateral elongated SP [Figure 1] and TMJ morphology was also normal. After evaluation of panoramic radiograph, patient was subjected to computed tomography (CT) scan to obtain accurate information about SP including its length and direction as superimposition of several anatomical structures, distortion, and magnification are the drawbacks of conventional radiographs. Coronal section of CT scans showed bilateral elongated SP reaching upto the hyoid bone [Figure 2]. Right lateral view showed segmentations present along the elongated SP and left lateral view showed uninterrupted elongated SP [Figures 3 and 4]. 3D-CT reformatted image better defined anatomy and measurements were done using a software tool which gave length of 6.8 cm on left side and 6.7 cm on the right side [Figure 5]. Serum calcium and phosphorus levels were within normal limits. So after seeing imaging findings, confirmative diagnosis of Eagle's syndrome was made. Since the patient had persistent pain and giddiness, however, possible causative factor for giddiness could be impingement on carotid arteries, surgical removal of bilateral elongated SP was planned and was done through extra-oral approach on left side and intraoral approach on the right side after performing tonsillectomy. Approximately, 4.5-5.0 cm of the segment was removed on both the sides [Figures 6]. Patient was observed and was relieved of the symptoms after 1 week. Post-operative CT scan was advised after 40 days [Figure 7]. Patient was completely symptom free after 2 months and is under regular follow-up.
Figure 1.
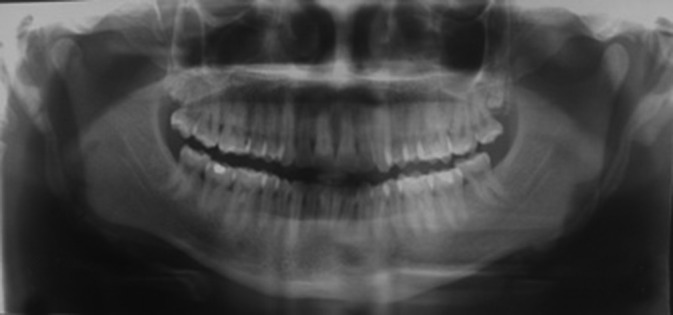
Panoramic radiograph showing bilaterally elongated styloid process
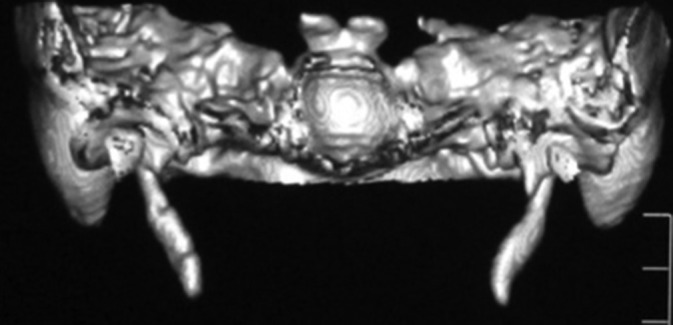
Figure 2.
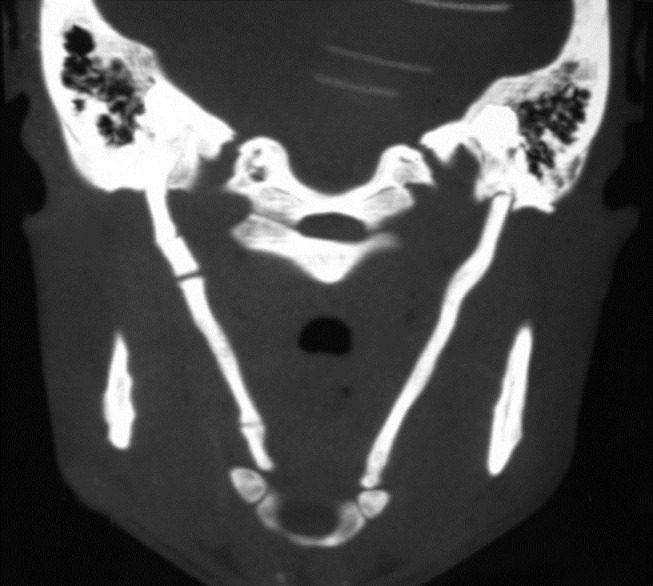
Coronal computed tomography image showing bilateral elongated styloid process reaching upto hyoid bone
Figure 3.

Right lateral view showing segmentations along elongated styloid process
Figure 4.
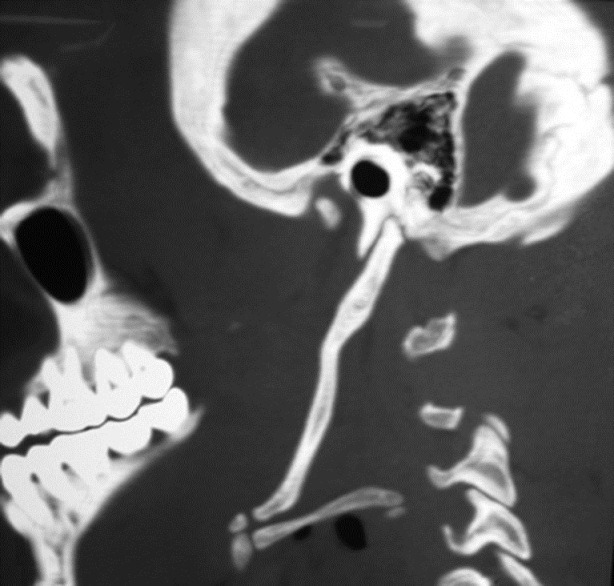
Left lateral view showing uninterrupted elongated styloid process
Figure 5.
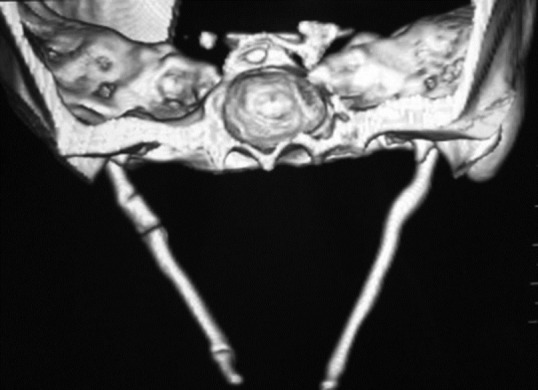
3D-computed tomography image showing bilateral elongated styloid process
Figure 6.

Photograph of surgically excised specimen
Figure 7.
Post-operative 3D-computed tomography image after 40 days
Discussion
SP is a small tapering projection from the base of temporal bone lying anteriorly to mastoid process. Muscles and ligaments attached to it play a role in mastication and swallowing. Vital structures lying in close proximity to it are internal and external carotid artery, internal jugular vein, glossopharyngeal, hypoglossal, and vagus nerve. Elongated SP giving rise to clinical symptoms of cervico-facial pain is known as Eagle's syndrome. Pain from elongated SP is due to “Constant mechanoreceptor discharge in area of V, VII, IX, X cranial nerve endings” initiated by mechanical irritation from SP.[4] The compression depends on the size, shape, and orientation of ossified the SP.[5] Eagle's syndrome presents with plethora of symptoms, which includes pain in throat, sensation of the foreign body in pharynx, dysphagia, otalgia, headache, pain on cervical rotation, pain along the distribution of external and internal carotid artery, and syncope. If the external carotid artery is affected, pain in the neck on turning head, or pain radiating to the eye, ear, angle of the mandible, soft palate and nose may be present, when the internal carotid artery is involved, pain over the entire head and larynx may be there.[6] Since the presentation of symptoms is highly variable, patients report to different specialties like otolaryngology, neurology, and dentistry for seeking treatment. In 1937, Eagle described two possible clinical presentations of elongated SP, which are classical Eagle syndrome and stylocarotid syndrome. Classical Eagle syndrome is typically seen after tonsillectomy or pharyngeal trauma, characterized by pharyngeal pain with swallowing, dysphagia, facial, and cervical pain. Stylocarotid syndrome is due to the pressure of the elongated SP on the internal or external carotid artery and sympathetic fibres in the wall of these vessels, characterized by pain and recurrent syncope provoked by cervical movements, particularly rotation. The exact cause of the elongated SP is not clear but various etiologies suggested are local chronic irritations, surgical trauma, endocrine disorders in female at menopause, persistence of mesenchymal elements, growth of the osseous tissue and mechanical stress or trauma during development of SP. Gokce et al.,[7] reported that ectopic calcification might have a role for elongation of SP, especially in patients with abnormal calcium, phosphorus, vitamin D metabolism as in end stage renal disease. There is progression in the length of calcification with advancing age.[8] The syndrome is reported more frequently in women than in men, with an age distribution greater than 40 years.[9] In this case, it was reported in young age. Differential diagnosis includes neuralgia (trigeminal, glossopharyngeal, and sphenopalatine), TMJ disorder, tonsillo-pharyngitis, cervical vertebra arthritis, otitis, impacted molar teeth, cluster headache, migraine, benign or malignant neoplasm, and salivary gland disease. While examination, palpable SP through tonsillar fossae is suggestive of elongated SP, which is not palpable in normal condition, also pain is exacerbated. Temporary relief from pain after infiltration of anesthetic solution in tonsillar fossae is highly suspicious for diagnosis of Eagle's syndrome. Radiographs are the confirmatory tool after examination. Conventional radiographs, which can be used are panoramic radiograph, posteroanterior skull view, lateral cephalogram, lateral oblique mandible view, Towne's view. However, moreover conventional radiographs have inherent drawback of superimposition of anatomical structures, and hence reducing the diagnostic information. CT imaging overcomes all drawbacks of conventional radiographs. However, no 2D-CT image provides exact value of length of SP because no plane of image is exactly parallel to the SP leading to underestimation of the length. Moreover 3D-CT is a valuable and preferred diagnostic tool, which facilitates in providing accurate information regarding length, angulation, and anatomical relationship. Langlais et al.,[10] classified elongated SP into; type I pattern, which is uninterrupted, elongated process, type II characterized by the SP apparently being joined to the stylohyoid ligament by a single pseudo-articulation giving the appearance of an articulated elongated SP, and type III consisting of interrupting segments of the mineralized ligament, sometimes creating the appearance of multiple pseudo-articulations. In this case, elongated SP on the right side was Langlais type III and left side was Langlais type I. Conservative modality of treatment includes local infiltration of anesthetics, (NSAIDS) non steroidal anti-inflammatory drugs, and steroids in tonsillar fossae region. Surgical treatment includes styloidectomy, for which both extra-oral and intraoral approach can be used. Advantages of intraoral approach are less time consuming, simple, no scarring and disadvantages are poor visualization of surgical field, possible injury of nearby neurovascular structures, and risk of deep neck space infection. Advantages of extra-oral approach are better visualization of surgical field and disadvantages are time consuming, neck scar, and risk of damage to facial nerve. In this case, the surgical intervention was adopted using an extra-oral approach on the left side and intraoral approach on right side without any post-operative complications. In conclusion, patients presenting with radiating cervico-facial pain detailed physical examination should be carried out and possibility of Eagle's syndrome should also be considered though it is rare. Clinicians should be well aware of this condition. In imaging, CT scan is the most preferred diagnostic tool.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
References
- 1.Eagle WW. Elongated styloid process: Report of two cases. Arch Otolaryngol. 1937;25:584–6. doi: 10.1001/archotol.1949.03760110046003. [DOI] [PubMed] [Google Scholar]
- 2.Raina D, Gothi R, Rajan S. Eagle syndrome. Indian J Radiol Imaging. 2009;19:107–8. doi: 10.4103/0971-3026.50826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rechtweg JS, Wax MK. Eagle's syndrome: A review. Am J Otolaryngol. 1998;19:316–21. doi: 10.1016/s0196-0709(98)90005-9. [DOI] [PubMed] [Google Scholar]
- 4.Naik SM, Naik SS. Tonsillo-styloidectomy for Eagle's syndrome: A review of 15 cases in KVG Medical College Sullia. Oman Med J. 2011;26:122–6. doi: 10.5001/omj.2011.30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ramadan SU, Gokharman D, Tunçbilek I, Kacar M, Koşar P, Kosar U. Assessment of the stylohoid chain by 3D-CT. Surg Radiol Anat. 2007;29:583–8. doi: 10.1007/s00276-007-0239-8. [DOI] [PubMed] [Google Scholar]
- 6.Feldman VB. Eagle's syndrome: A case of symptomatic calcification of the stylohyoid ligaments. J Can Chiropr Assoc. 2003;47:21–7. [Google Scholar]
- 7.Gokce C, Sisman Y, Sipahioglu M. Styloid process elongation or Eagle's syndrome: Is there any role for ectopic calcification? Eur J Dent. 2008;2:224–8. [PMC free article] [PubMed] [Google Scholar]
- 8.Jaju PP, Suvarna P, Parikh N. Eagles syndrome: An enigma to dentists. J Indian Acad Oral Med Radiol. 2007;19:424–9. [Google Scholar]
- 9.Öztaş B, Orhan K. Investigation of the incidence of stylohyoid ligament calcifications with panoramic radiographs. J Investig Clin Dent. 2012;3:30–5. doi: 10.1111/j.2041-1626.2011.00081.x. [DOI] [PubMed] [Google Scholar]
- 10.Langlais RP, Miles DA, Van Dis ML. Elongated and mineralized stylohyoid ligament complex: A proposed classification and report of a case of Eagle's syndrome. Oral Surg Oral Med Oral Pathol. 1986;61:527–32. doi: 10.1016/0030-4220(86)90400-7. [DOI] [PubMed] [Google Scholar]