

Abstract
Aims:
This study was aimed to determine the effectiveness of Papacárie® for caries removal as compared to the conventional method with respect to microbial flora, time, the amount of tissue removal, child's behavior, pain perception, and preference of treatment.
Materials and Methods:
Sixty primary molars of 30 children of age 4-9 years were selected randomly and divided into two groups of 30 teeth each: Group A treated by conventional method and group B with Papacárie® method.
Results:
Comparatively, no statistical difference was seen in microbial growth, total bacterial count, and lactobacilli count in both the groups (P = 0.36). The mean cavity entrance size with group A was 0.98133 mm and group B was 0.26083 mm (P < 0.001). The mean preparation time for group A was 4.7 Mins (minutes) and group B was 17.96 min s (P < 0.001). Majority of kids of both group A and B scored 3 (Frankl Behavior Rating Scale) before and after the treatment showing no statistical difference in their behavioral score (P = 1). In group A 50% of children experienced no pain as compared to 86.7% in group B (P = 0.01). There was no statistical difference in the preference of treatment (P = 0.12).
Conclusion:
Thus, the Chemo mechanical caries removal method can be considered as an effective method to control pain and preserve sound tooth structure during caries excavation.
Keywords: Behavior assessment, cariogenic flora, chemo-mechanical caries removal, mechanical method of caries removal, Papacárie®
Introduction
In the distant past due to the absence of adhesive restorative materials, it was necessary to remove sound tooth structure just to make room for the restoration. Now-a-days the main aim of restoring a decayed tooth is to reinforce by preserving as much tooth structure as possible by limiting the extent of cavity preparation by removing only affected dentin. Due to better understanding of caries process and improved knowledge of the function of fluoride, it is possible to retain some of the demineralized enamel and dentin and allowing it to heal through remineralization.
Even though the rotary method of caries removal is widely accepted and quick technique, it is often associated with excessive cutting of uninfected dentin, pain, discomfort, noise, and fear. Hence, the quest for removal of caries with minimal pain and more tissue preservation has given rise to various alternative caries removal techniques. This includes air abrasion, atraumatic restorative therapy, chemo-mechanical system, and lasers.[1–4]
Chemo mechanical caries removal (CMCR) method is a non-invasive technique which eliminates infected tissues, preserving healthy structures, avoiding pulp irritation and patient discomfort. Papacárie® introduced in 2003 has claimed to preserve healthy dental tissue with benefits of minimal discomfort, antibacterial, and anti-inflammatory effects.[5]
This study was carried out to compare the clinical efficacy of a CMCR product in reducing cariogenic flora, duration of caries removal, the amount of tooth loss, child's behavioral assessment before, during and after procedure, pain perception, and preference of treatment in comparison with the conventional method.
Materials and Methods
The study sample consisted of 60 primary molars from 30 children, 2 teeth in each, between 4 and 9 years of age with broad cavitated occlusal lesions not involving the pulp. All patients were treated in the Department of Pediatric Dentistry, SDM School of Dentistry, Dharwad, India. The study was approved by the Institutional Review Board and informed consent was obtained from the parents. The study samples were divided into group A and B having 30 teeth in each. Carious teeth in group A were treated by the conventional airotor method and group B were treated by Papacárie®.
Topical anesthetic gel was applied to reduce patient discomfort during rubber dam placement. After this, the patient was allowed to settle down for some time before starting the caries excavation to minimize its effect on change in the behavior of child during procedure. The administration of local anesthesia was not done as it would alter the pain perception of the patient.
Caries excavation in group A was done with help of airotor using a round bur (no. 008). In group B, caries excavation was done according to the manufacturer's instruction using Papacárie® gel (Formulae Acao, Sao Paulo, Brazil). Complete caries excavation was confirmed by the tactile and visual method.
After completion of caries removal in each method, healthy dentin samples were collected using a sharp spoon excavator and immediately transferred to thyoglycolate broth for microbiological investigations. The broth was transferred into culture media using microbiological sticks. The diluted samples were plated on two different agar plates, i.e., rogosa agar plates and chocolate agar plates to determine the lactobacilli counts (LBC) and total bacterial counts (TBC), respectively.
The border of the lesion was marked and the greatest diameter of the lesion entrance was measured with a sterile divider (Ceto diamond, Mumbai, India) and recorded before and after the caries removal in both methods. To minimize bias, inter-examination of the cavities on both occasions was done and the mean was calculated. All the sample teeth were finally restored with miracle mix restorative material (GC corporation Tokyo, Japan). Time taken was recorded for both the procedure with the help of a digital stop watch.
The degree of cooperation by the child before, during and after caries removal was evaluated and recorded according to Wright's modified Frankl's Behavior Rating Scale. After completion of the caries removal procedure by each method, the child was interviewed regarding pain or discomfort and the preferred caries removal method.
Results
Microbial growth was observed in 36.7% of group A samples and 56.7% of group B samples [Figure 1]. The mean TBC were 0.9 × 102, 1.15 × 102 and LBC were 0.35 × 102, 0.41 × 102, respectively, for group A and B [Figure 2]. Although the mean TBC and LBC in the Conventional method was less than the Papacárie® method the results were not statistically significant (P = 0.36).
Figure 1.
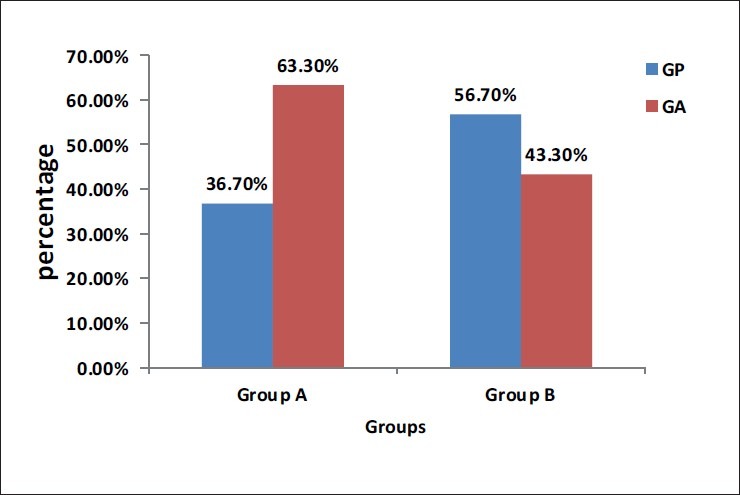
Microbial growth in both the groups. GP - Growth present, GA - Growth absent
Figure 2.
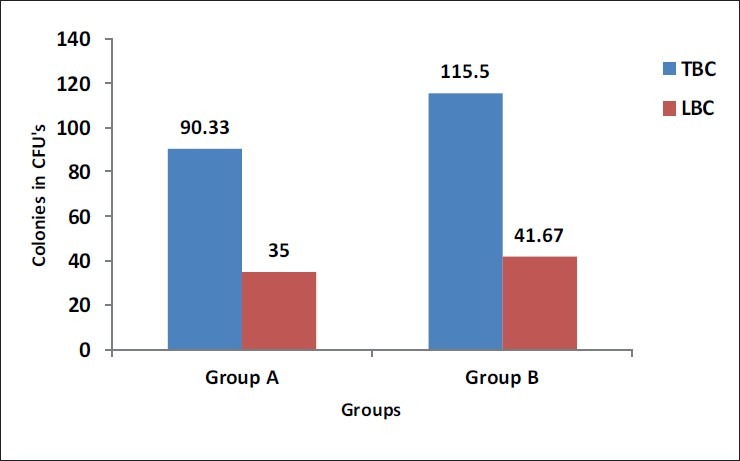
Mean total bacterial count and lactobacilli count in both the groups. TBC - Total bacterial count, LBC - Lactobacilli count
The mean cavity entrance size [Figure 3] with group A was 0.98133 mm, and group B was 0.26083 mm (P < 0.001). The mean preparation time [Figure 4] for group A was 280.89 s and group B was 1077.60 s (P < 0.001).
Figure 3.
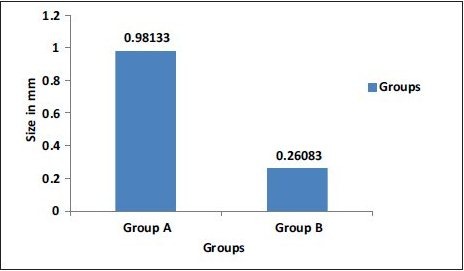
Mean difference in cavity entrance size in both the groups
Figure 4.
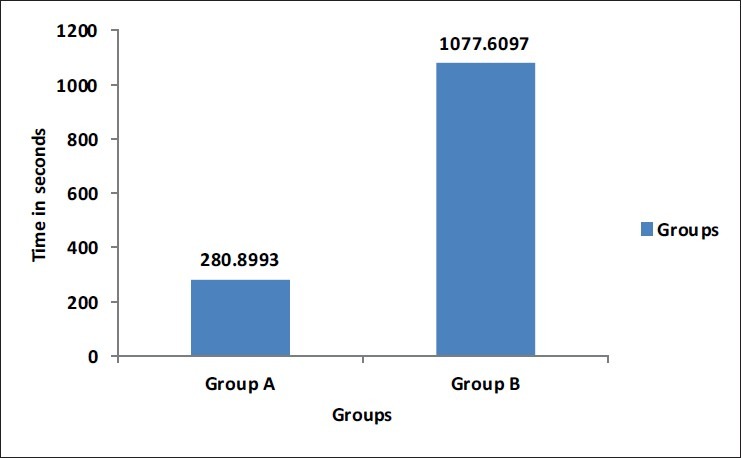
Mean preparation time for both the groups
Majority of kids of both group A and B scored 3 [Figure 5] before and after the treatment showing no statistical difference in their behavioral score (P = 1). In group A, 50% of children had no pain, 46.7% had slight, and 3.3% had unspecified pain. In group B, 86.7% of children had no pain, 10% had slight, and 3.3% had unspecified pain [Figure 6]. There was statistical significance in the number of children who had no pain among the two groups (P = 0.01). Considering the preference 36.7% of children preferred conventional method, 60% preferred Papacárie® , and 3.3% preferred both the methods [Figure 7]. There was no statistical difference in the preference of treatment (P = 0.12).
Figure 5.
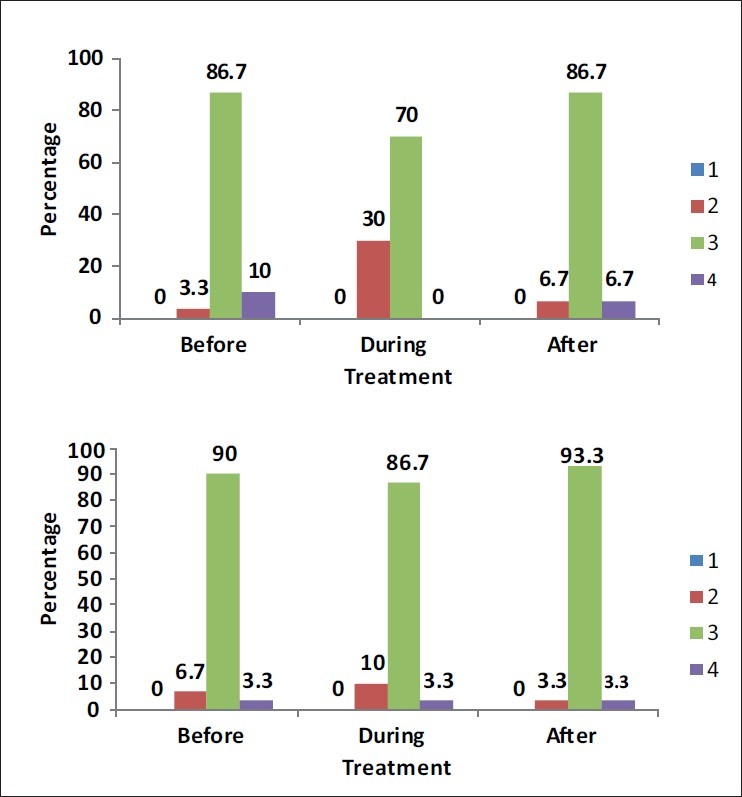
Percentage of children scoring the various behavioral scores before, during and after the treatment in both the groups. 1 - Definitely negative, 2 - Negative, 3 - Positive, 4 - Definitely positive
Figure 6.
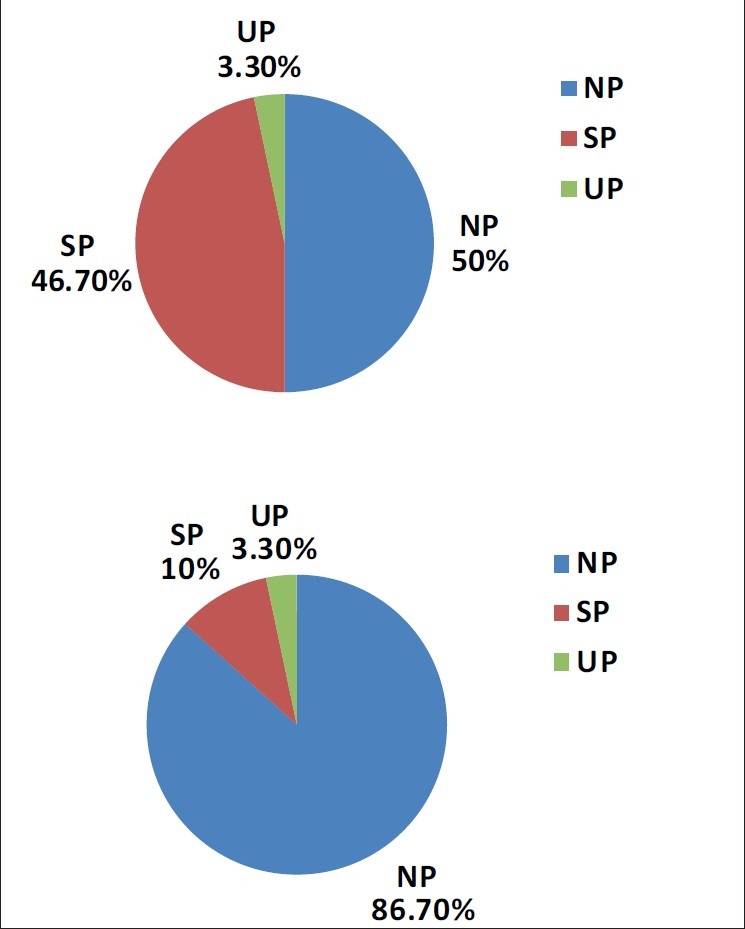
Percentage of children with different pain perception in both the groups
Figure 7.
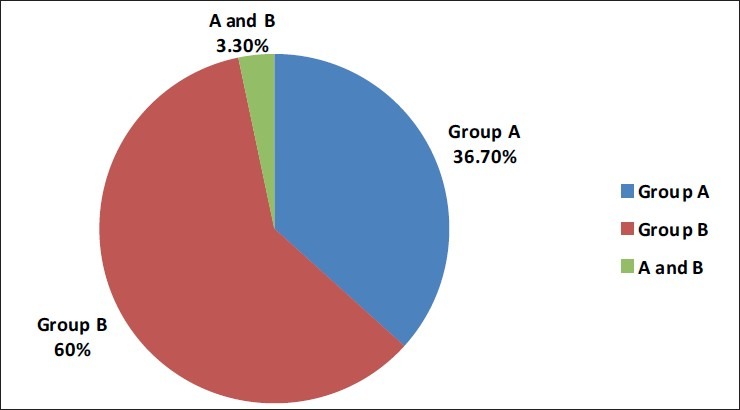
Percentage of children preferring each method of treatment
Discussion
New methods of caries removal have always been a major objective for dental researchers seeking possible alternative to existing conventional methods in the field of pediatric dentistry. Factors, including speed, pain-free preparation, cost-effectiveness, clinical application, safety and proper conservative cavity preparation for the placement of advanced chemically adhesive restorative material has encouraged research in this field thus inventing new devices for this purpose. Among most caries removal methods, the CMCR system has found to be easy, simple and economic, as well as being effective in removing caries. Researchers claim the use of this technique for children who are basically anxious for dental treatment is interesting based on its simplicity.[6,7]
In this study, all the cavities were found to be clinically caries-free in both conventional and Papacárie® methods when observed by the tactile and visual method. The one used by Kidd et al., wherein they reported satisfactory results in assessing the caries-free status of lesion.[8] Bussadori et al.,[9] found that after 1 year of clinical and radiographic follow-up; caries-free teeth with good retention of restoration were found with Papacárie® method. It indicates the reduction in occurrence of secondary caries and retention of restoration.
Kidd et al.,[10] used a procedure for taking samples from residual dentin, by round bur of a defined size. In this study, an excavator was chosen to reduce the risk of accidental pulpal exposure, especially when sampling hard dentin, similar to the study done by Azrak et al.[11] and Subramaniam et al.[12]
Several investigations have shown that often a low number of residual microorganisms (101-103 CFU) remains behind in clinically sound hard dentin in spite of a significant reduction in the bacterial count. However, this low level of bacteria is considered to be clinically acceptable by several authors.[10,13,14] Residual bacteria cannot be held solely responsible for occurrence of secondary caries, since individual factors like oral hygiene and dietary habits of the patients also have a profound influence on caries progression. The study results are comparable with studies of Kidd et al.[13] and Heinrich et al.[15] as bacterial values were below 102 CFU's for the streptococci and LBC in hard dentin.
According to the chart, Papacárie® takes about 4 times longer time than the conventional method. Reasons attributed for increased time taken in Papacárie® method could be multiple applications needed for complete caries removal, differences in type and size of the cavities, type of teeth and age of the patient. Similar results were seen in a study conducted by Ferrari et al.[16]
Bussadori et al.,[9] observed through scanning electron microscope that in Papacárie® method, there was more preservation of dentin structure. Though contrasting results have been put forth by Fure et al.,[17] In this study, the Papacárie® method was beneficial in preserving more amounts of healthy tooth tissue being minimally invasive.
Studies by Berggren et al. and Green et al., have revealed that the most feared events in dental treatment as ranked by the patients are cavity cutting, induction of anesthesia, and tooth extraction. Therefore, a CMCR method is more preferable for persons with dental anxiety.[18,19]
Wright's Modification of Frankl's Behavior Rating Scale[20] in this study were simple, sufficiently sensitive, and easy to record and widely accepted. According to Hosey and Blinkhorn,[21] Frankl's Behavior Rating Scale showed a significant correlation with the newer scales.
In this study, there was deterioration of the behavior from positive to negative during the treatment with the Conventional method and after the treatment, there was an improvement in the behavior. However, in Papacárie® method there was no change in the behavior of children before, during and after the treatment.
The study results are in correlation with many others; wherein they had concluded that CMCR is well suited for dental treatment of anxious patients.[6,22,23] But, contradicting to these studies Inglehart et al., found that the subject's fear of the dentists increased in the CMCR method, while it is slightly decreased in the conventional method. They have attributed this finding to the longer treatment time required for CMCR method.[24]
According to Ansari et al., the CMCR method not only prevents anxious patients losing their teeth at an early age, it can also be used successfully when the alternative treatment is under general anesthesia. It could also be beneficial to medically be compromised and immunosuppressed patients.[6]
Silva et al., demonstrated that caries removal using Papacarie® method is significantly less painful compared to the conventional method. It reduces the risk of pulpal exposure and thereby reduces the damage to healthy tissues, Silva et al., and Bussadori et al.,.[25,26] Anusavice and Kincheloe[27] demonstrated that cutting sound dentin often results in some level of pain. In this study, the age of participants limited the possibilities of obtaining a more complete description of the kind of pain felt during the caries excavation. However, the gel itself may have a thermal insulating function as it covers the cavity during the procedure.[28] In addition the method is expected not to open so many dentinal tubules as in drilling.[29]
Regarding preference, around 60% of the children preferred Papacárie® method [Figure 7]. Similar studies on Carisolv™ reported that most of the patients prefered CMCR method over the conventional method.[6,22,30] Contrasting results were reported by Maragakis et al., who claimed that only 31% of pediatric patients preferred CMCR method. The reasons for preferring conventional method was that “it was quicker,” “it tasted better,” and “they finished sooner.”[31] Another study by Zinck et al., reported that 93% preferred CMCR method more than conventional method. The reasons given were that they felt it decreased drilling time, did not cause pain and provided a general feeling of comfort and relaxation.[32] In this study, the children who did not prefer Papacárie® method gave the reason that it took a longer time than conventional method. Thus, the time factor may be crucial for the acceptance of the treatment by some patients, especially children, since it constitutes an important source of discouragement for them.
Conclusion
The results from this study indicate that the CMCR method is a safe and effective method for excavation of dentinal caries. As the efficacy of the active gel compared to traditional hand excavation has been documented in vitro, this study showed that the chemo-mechanical method may reduce patient discomfort and decrease unnecessary removal of sound dental tissue.
It can be successfully employed to treat medically compromised, bed-ridden patients and in school dental camps. Thus, this method seems to be a promising alternative for conventional method of cavity cutting in pediatric dental use.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
References
- 1.Black RB. Airabrasive: Some fundamentals. J Am Dent Assoc. 1950;41:701–10. doi: 10.14219/jada.archive.1950.0247. [DOI] [PubMed] [Google Scholar]
- 2.Frencken JE, Pilot T, Songpaisan Y, Phantumvanit P. Atraumatic restorative treatment (ART): Rationale, technique, and development. J Public Health Dent. 1996;56:135–40. doi: 10.1111/j.1752-7325.1996.tb02423.x. [DOI] [PubMed] [Google Scholar]
- 3.Goldman M, Kronman JH. A preliminary report on a chemo-mechanical means of removing caries. J Am Dent Assoc. 1976;93:1149–53. doi: 10.14219/jada.archive.1976.0249. [DOI] [PubMed] [Google Scholar]
- 4.Keller U, Hibst R, Geurtsen W, Schilke R, Heidemann D, Klaiber B, et al. Erbium: YAG laser application in caries therapy. Evaluation of patient perception and acceptance. J Dent. 1998;26:649–56. doi: 10.1016/s0300-5712(97)00036-5. [DOI] [PubMed] [Google Scholar]
- 5.Pereira SA, Silva LR, Motta LJ, Bussadori SK. Remocao quimico-mechanica da carie por meio do gel Papacarie. [Chemical-mechanical caries removal with Papacarie gel] Rev Inst Cienc Health. 2004;52(5):385–88. [Google Scholar]
- 6.Ansari G, Beeley JA, Fung DE. Chemomechanical caries removal in primary teeth in group of anxious children. J Oral Rehabil. 2003;30:773–9. doi: 10.1046/j.1365-2842.2003.01119.x. [DOI] [PubMed] [Google Scholar]
- 7.Banerjee A, Watson TF, Kidd EA. Dentine caries excavation: A review of current clinical techniques. Br Dent J. 2000;188:476–82. doi: 10.1038/sj.bdj.4800515. [DOI] [PubMed] [Google Scholar]
- 8.Kidd EA, Joyston-Bechal S, Beighton D. The use of a caries detector dye during cavity preparation: A microbiological assessment. Br Dent J. 1993;174:245–8. doi: 10.1038/sj.bdj.4808142. [DOI] [PubMed] [Google Scholar]
- 9.Bussadori SK, Guedes CC, Hermida Bruno ML, Ram D. Chemo-mechanical removal of caries in an adolescent patient using a papain gel: Case report. J Clin Pediatr Dent. 2008;32:177–80. doi: 10.17796/jcpd.32.3.1168770338617085. [DOI] [PubMed] [Google Scholar]
- 10.Kidd EA, Joyston-Bechal S, Beighton D. Microbiological validation of assessments of caries activity during cavity preparation. Caries Res. 1993;27:402–8. doi: 10.1159/000261571. [DOI] [PubMed] [Google Scholar]
- 11.Azrak B, Callaway A, Grundheber A, Stender E, Willershausen B. Comparison of the efficacy of chemomechanical caries removal (Carisolv) with that of conventional excavation in reducing the cariogenic flora. Int J Paediatr Dent. 2004;14:182–91. doi: 10.1111/j.1365-263X.2004.00535.x. [DOI] [PubMed] [Google Scholar]
- 12.Subramaniam P, Babu KL, Neeraja G. Comparison of the antimicrobial efficacy of chemomechanical caries removal (Carisolv) with that of conventional drilling in reducing cariogenic flora. J Clin Pediatr Dent. 2008;32:215–9. doi: 10.17796/jcpd.32.3.1r08w6k1478865u7. [DOI] [PubMed] [Google Scholar]
- 13.Kidd EA, Ricketts DN, Beighton D. Criteria for caries removal at the enamel-dentine junction: A clinical and microbiological study. Br Dent J. 1996;180:287–91. doi: 10.1038/sj.bdj.4809066. [DOI] [PubMed] [Google Scholar]
- 14.Bjørndal L, Larsen T, Thylstrup A. A clinical and microbiological study of deep carious lesions during stepwise excavation using long treatment intervals. Caries Res. 1997;31:411–7. doi: 10.1159/000262431. [DOI] [PubMed] [Google Scholar]
- 15.Heinrich R, Kneist S, Künzel W. Clinical controlled study on the treatment of deep carious lesions in deciduous molars. Dtsch Zahnarztl Z. 1991;46:581–4. [PubMed] [Google Scholar]
- 16.Ferrari JC, Motisuki C, Bortoletto CC, Santos-Pinto L. Efficiency of Papacárie® in the chemo-mechanical carious dentine removal. Rev bras odontol. 2005;62:209–11. [Google Scholar]
- 17.Fure S, Lingstrom P, Birkhed D. Chemo-mechanical removal of root caries compared to drilling. J Dent Res. 1999;78:108. [Google Scholar]
- 18.Berggren U, Meynert G. Dental fear and avoidance: Causes, symptoms, and consequences. J Am Dent Assoc. 1984;109:247–51. doi: 10.14219/jada.archive.1984.0328. [DOI] [PubMed] [Google Scholar]
- 19.Green RM, Green A. Adult attitudes to dentistry among dental attenders in South Wales. Br Dent J. 1985;159:157–60. doi: 10.1038/sj.bdj.4805662. [DOI] [PubMed] [Google Scholar]
- 20.Wright FA, Lange DE. Dental anxiety in children. N Z Dent J. 1976;72:80–3. [PubMed] [Google Scholar]
- 21.Hosey MT, Blinkhorn AS. An evaluation of four methods of assessing the behaviour of anxious child dental patients. Int J Paediatr Dent. 1995;5:87–95. doi: 10.1111/j.1365-263x.1995.tb00170.x. [DOI] [PubMed] [Google Scholar]
- 22.Lozano-Chourio MA, Zambrano O, González H, Quero M. Clinical randomized controlled trial of chemomechanical caries removal (Carisolv) Int J Paediatr Dent. 2006;16:161–7. doi: 10.1111/j.1365-263X.2006.00719.x. [DOI] [PubMed] [Google Scholar]
- 23.Bergmann J, Leitão J, Kultje C, Bergmann D, Clode MJ. Removing dentine caries in deciduous teeth with Carisolv: A randomised, controlled, prospective study with six-month follow-up, comparing chemomechanical treatment with drilling. Oral Health Prev Dent. 2005;3:105–11. [PubMed] [Google Scholar]
- 24.Inglehart MR, Peters MC, Flamenbaum MH, Eboda NN, Feigal RJ. Chemomechanical caries removal in children: An operator's and pediatric patients’ responses. J Am Dent Assoc. 2007;138:47–55. doi: 10.14219/jada.archive.2007.0020. [DOI] [PubMed] [Google Scholar]
- 25.Silva LR, Motta LJ, Reda SH, Facanha RA, Bussadori SK. Papacarie -um novo sistema para a remocao quimica e mechanica do tecido cariado – relato de caso clinico. [Papacárie: A new system for chemo-mechanical caries re- moval: A case report] Rev Paul Odontol. 2004;26(6):4–8. [Google Scholar]
- 26.Bussadori SK, Castro LC, Galvão AC. Papain gel: A new chemo-mechanical caries removal agent. J Clin Pediatr Dent. 2005;30:115–9. doi: 10.17796/jcpd.30.2.xq641w720u101048. [DOI] [PubMed] [Google Scholar]
- 27.Anusavice KJ, Kincheloe JE. Comparison of pain associated with mechanical and chemomechanical removal of caries. J Dent Res. 1987;66:1680–3. doi: 10.1177/00220345870660111501. [DOI] [PubMed] [Google Scholar]
- 28.Ericson D. In-vitro of a new gel for chemo-mechanical caries removal. J Dent Res. 1998;77:1252. [Google Scholar]
- 29.Lopes MC, Mascarini RC, da Silva BM, Flório FM, Basting RT. Effect of a papain-based gel for chemomechanical caries removal on dentin shear bond strength. J Dent Child (Chic) 2007;74:93–7. [PubMed] [Google Scholar]
- 30.Rafique S, Fiske J, Banerjee A. Clinical trial of an air-abrasion/chemomechanical operative procedure for the restorative treatment of dental patients. Caries Res. 2003;37:360–4. doi: 10.1159/000072168. [DOI] [PubMed] [Google Scholar]
- 31.Maragakis GM, Hahn P, Hellwig E. Clinical evaluation of chemomechanical caries removal in primary molars and its acceptance by patients. Caries Res. 2001;35:205–10. doi: 10.1159/000047457. [DOI] [PubMed] [Google Scholar]
- 32.Zinck JH, McInnes-Ledoux P, Capdeboscq C, Weinberg R. Chemomechanical caries removal – A clinical evaluation. J Oral Rehabil. 1988;15:23–33. doi: 10.1111/j.1365-2842.1988.tb00143.x. [DOI] [PubMed] [Google Scholar]