

Abstract
Purpose:
To evaluate the correlation between sagittal condylar guidance obtained by protrusive interocclusal records and panoramic radiograph tracing methods in human dentulous subjects.
Materials and Methods:
The sagittal condylar guidance was determined in 75 dentulous subjects by protrusive interocclusal records using Aluwax through a face bow transfer (HANAU™ Spring Bow, Whip Mix Corporation, USA) to a semi-adjustable articulator (HANAU™ Wide-Vue Articulator, Whip Mix Corporation, USA). In the same subjects, the sagittal outline of the articular eminence and glenoid fossa was traced in panoramic radiographs. The sagittal condylar path inclination was constructed by joining the heights of curvature in the glenoid fossa and the corresponding articular eminence. This was then related to the constructed Frankfurt's horizontal plane to determine the radiographic angle of sagittal condylar guidance.
Results:
A strong positive correlation existed between right and left condylar guidance by the protrusive interocclusal method (P 0.000) and similarly by the radiographic method (P 0.013). The mean difference between the condylar guidance obtained using both methods were 1.97° for the right side and 3.18° for the left side. This difference between the values by the two methods was found to be highly significant for the right (P 0.003) and left side (P 0.000), respectively. The sagittal condylar guidance obtained from both methods showed a significant positive correlation on right (P 0.000) and left side (P 0.015), respectively.
Conclusion:
Panoramic radiographic tracings of the sagittal condylar path guidance may be made relative to the Frankfurt's horizontal reference plane and the resulting condylar guidance angles used to set the condylar guide settings of semi-adjustable articulators.
Keywords: Articular eminence, panoramic radiographs, protrusive interocclusal registration, sagittal condylar guidance
Introduction
The goal of a prosthodontic rehabilitation is to fabricate a prosthesis, which is in harmony with the patient's stomatognathic system. The most essential consideration in the oral rehabilitation of any patient is the inclination of the condylar path. Condylar path is the path traversed by the condyle in relation to the articular eminence when the mandible is moved either protrusively or laterally from centric relation.[1] Condylar guidance is the mechanical form located in the upper posterior region of an articulator that controls movement of its mobile member.[2] The purpose of protrusive jaw relation is to set the condylar elements of the articulator so that they will reproduce inclinations, which are similar or comparable to that of the patient's temporomandibular articulation.[3]
However, many practitioners rely on average values of condylar guidance, which range from 22° to 65°.[1,4,5] If the individual inclination of the articular eminence is very steep or flat, guidance derived from the mean value settings may vary sufficiently leading to incorporation of inaccuracies while accomplishing a particular clinical objectives such as posterior disocclusion or balanced occlusion.[6,7] Various intra-oral and extra-oral methods have been used to register the path of the condyle and adjust the articulator accordingly. Centric and eccentric relations of the mandible can be recorded through intraoral or positional wax method, graphic recordings, functional recordings, and cephalometrics.[8] Despite accurate registration methods, sources of error arise in laboratory procedures as a result of instability of materials and changes during their setting or polymerization.[9] The reliability of wax records for protrusive jaw relation has been questioned as condylar guidance adjusted according to three separate records will yield three different results.[10] Moreover, if the patient moves the jaw laterally in protrusive movement, the registration of the condyle path will be changed.[11]
The use of supplementary aids such as imaging may help in resolving the above problems and establish accurate registration of sagittal condylar guidance. The outline of the articular eminence and the glenoid fossa of the temporal bone has been evaluated on panoramic radiographs and proposed to be of valuable aid in setting the condylar guidance in semi-adjustable articulators.[6] There are no studies in the dental literature, which compare condylar guidance obtained with protrusive interocclusal records using Aluwax and panoramic radiographic images. This study sought to evaluate the two techniques for recording and determining sagittal condylar guidance.
Materials and Methods
A total of 75 dentulous healthy subjects participated in the study after written informed consent was obtained. The study was given clearance by the Institutional Ethical Review Committee and was completed over a period of 8 months from January to August, 2011. Subjects within the age group of 20-40 years having a minimum of three teeth in each of the posterior quadrants were included, while subjects with less than three teeth in each of the posterior quadrant, facial or skeletal malformations, temporomandibular disorders, and poor neuromuscular co-ordination were excluded from the study.
Protrusive interocclusal records
Maxillary and mandibular impressions were made using irreversible hydrocolloid (Zelgan 2002; DENTSPLY, India) impression material and casts were immediately poured using Type III dental stone (Dental Stone, Kalabhai, India,). Using face bow (HANAU™ Spring Bow, Whip Mix Corporation, USA) transfer, the maxillary cast was mounted on the semi-adjustable articulator (HANAU™ Wide-Vue Articulator, Whip Mix Corporation, USA). Mandibular cast was mounted using the patient's maximum intercuspation record. The protrusive interocclusal record was made at 6 mm protrusion by using Aluwax [Figure 1]. This record was then transferred to articulator (HANAU™ Wide-Vue Articulator). Protrusive relation was evaluated and reconfirmed before the sagittal condylar inclinations were set and locknuts were tightened with hand pressure [Figure 2]. In all the cases, articulator was programmed by a single operator.
Figure 1.

Protrusive interocclusal record using Aluwax
Figure 2.
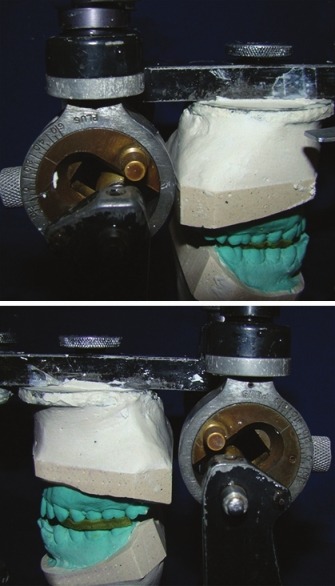
Condylar guidance obtained by programming of articulator using protrusive interocclusal registration
Panoramic radiography
The radiographic procedures were carried out in Department of Oral Radiology of the institute. All radiographs were made by the single operator in the same radiographic unit (Promaxtm Planmeca, Helsinki) with exposure factors of 68 kVp and 10 mA. The images were printed to 100% scale on Agfatm Films in an Agfa Drystartm 5302 printer. The sagittal outlines of the left and right articular eminence and glenoid fossae were traced on a transparent acetate tracing sheet by two examiners. The left and right “orbitale” (lowest point in the margin of the orbit) and “porion” highest point in the margin of the auditory meatus) were identified and the Frankfurt horizontal plane was constructed by joining the two landmarks on each side. The most superior point on the articular eminence and the most inferior point on the articular tubercle were identified and a second line to represent the mean condylar path inclination was constructed by joining the two points. The angle formed by the intersection of the two lines was determined to represent the angle of sagittal condylar inclination [Figures 3 and 4]. This was determined by the two examiners and the average taken as the true value.
Figure 3.
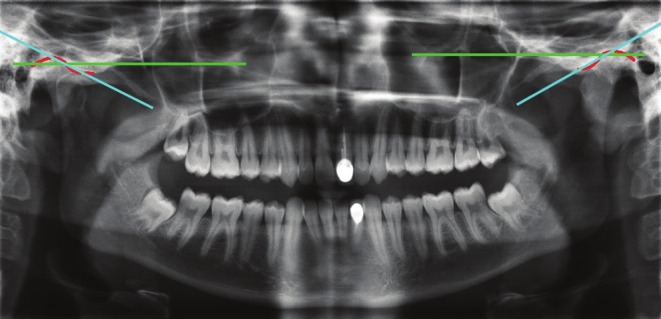
Panoramic radiograph of the patient showing the tracing of the angle of sagittal condylar guidance. Red line: Outline of articular fossa and eminence, green line: Frankfurt horizontal plane, blue line: Sagittal condylar path inclination
Figure 4.
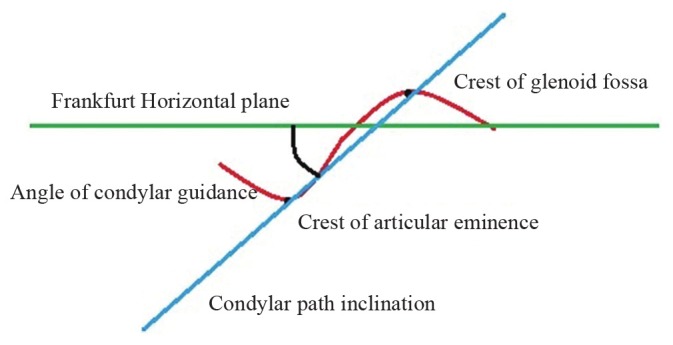
Line diagram of the panoramic tracing of the angle of sagittal condylar guidance
Statistical analysis
All statistical analysis was carried out in SPSS 16 software (Statistical Package for the Social Sciences, IBM Software Group, USA). Spearman-Rho's test was used to find the correlation between the sagittal condylar guidance between left and right sides and between the two methods on each side. Wilcoxon Sign Rank test was applied to check the difference between the right and left side condylar guidance determined by the two methods. Cronbach's alpha was used to identify the degree of reliability of the radiographic method.
Results
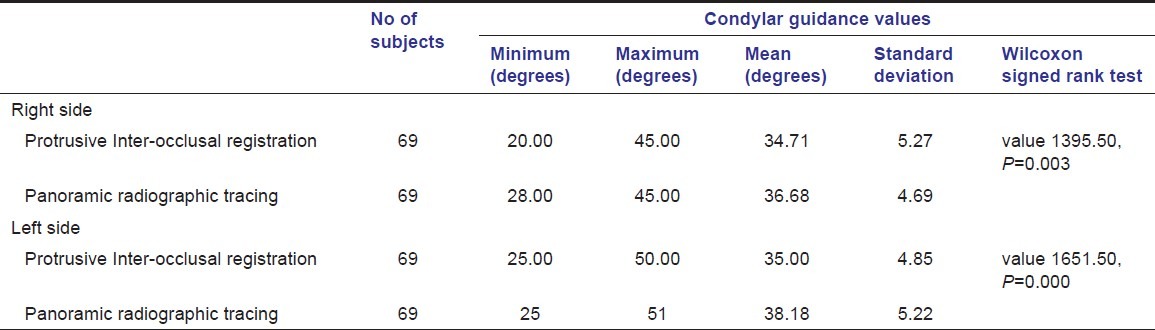
Although, 75 dentulous healthy subjects participated in the study six were excluded due to presence of radiographic artifacts. The sagittal condylar guidance values obtained by both methods from 69 subjects were analyzed. There were 30 male and 39 female subjects between 20 years and 42 years of age with a mean age of 26.76 years. Table 1 summarizes the range, mean, and standard deviation of condylar guidance values obtained using both the methods on the right and left side. The mean difference between the condylar guidance values obtained using both methods was 1.97° for the right side and 3.18° for the left side, with the radiographic values being higher. This difference between the values was found to be highly significant between the two methods for the right side (1395.50, P = 0.003) and left side (1651.50, P = 0.000), respectively. A significant positive correlation existed between the condylar guidance values of right and left sides in same subjects obtained using the protrusive interocclusal registration [Graph 1] and also by the panoramic radiograph separately [Graph 2]. The condylar guidance values obtained from protrusive interocclusal registration and a panoramic radiograph showed a significant positive correlation for the right and left sides separately [Graphs 3 and 4]. The inter-observer reliability in identification and determination of condylar guidance by the panoramic radiographic method using Cronbach's alpha showed a high degree of reliability with 0.911 on the right side and 0.933 on the left side, respectively.
Table 1.
Distribution of condylar guidance values obtained using both methods
Graph 1.
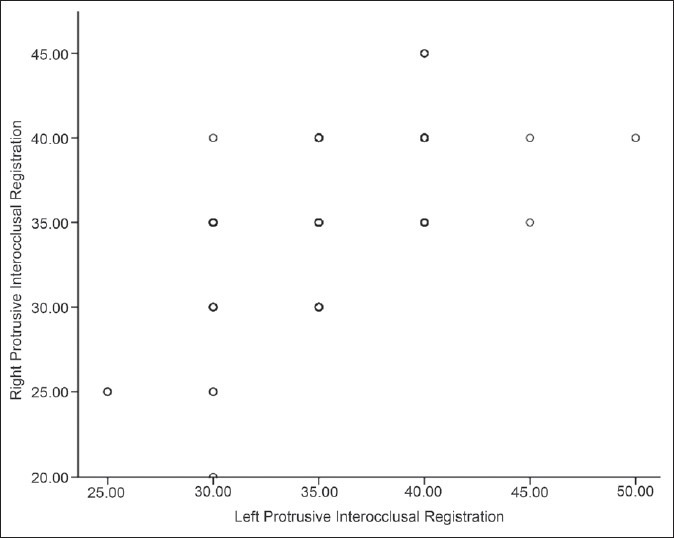
Correlation between condylar guidance values obtained using protrusive interocclusal registration on right and left side (r = 0.594, P = 0.000)
Graph 2.
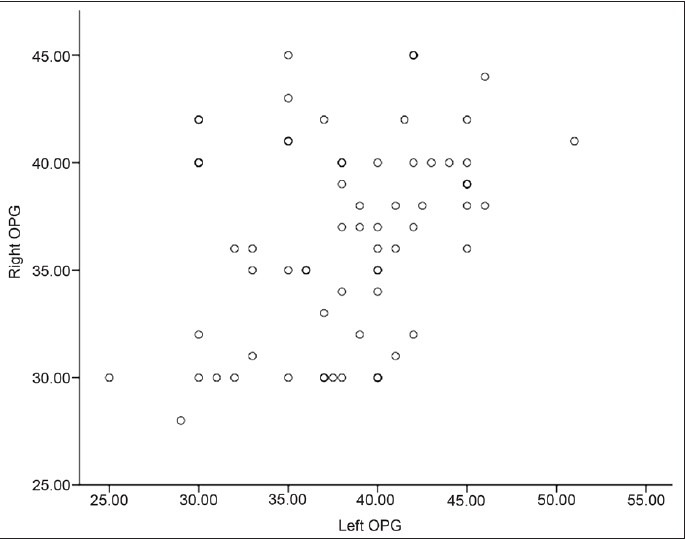
Correlation between condylar guidance values obtained using panoramic radiograph on right and left side (r = 0.299, P = 0.013)
Graph 3.
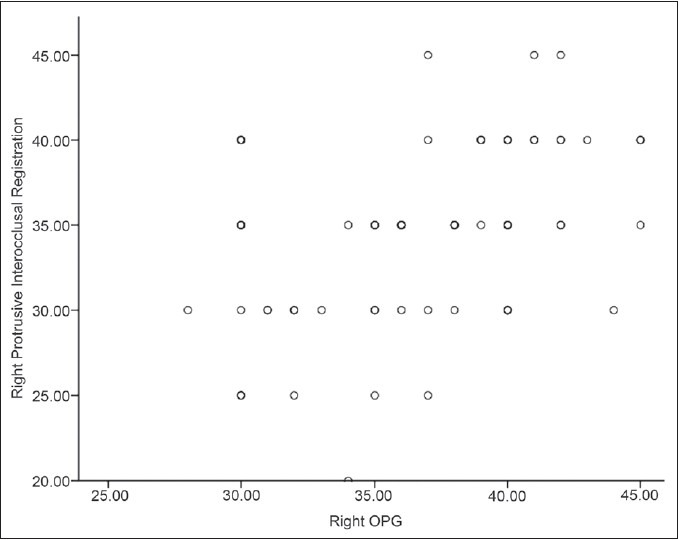
Correlation between condylar guidance values obtained using protrusive interocclusal registration and panoramic radiograph on right side (r = 0.413, P = 0.000)
Graph 4.
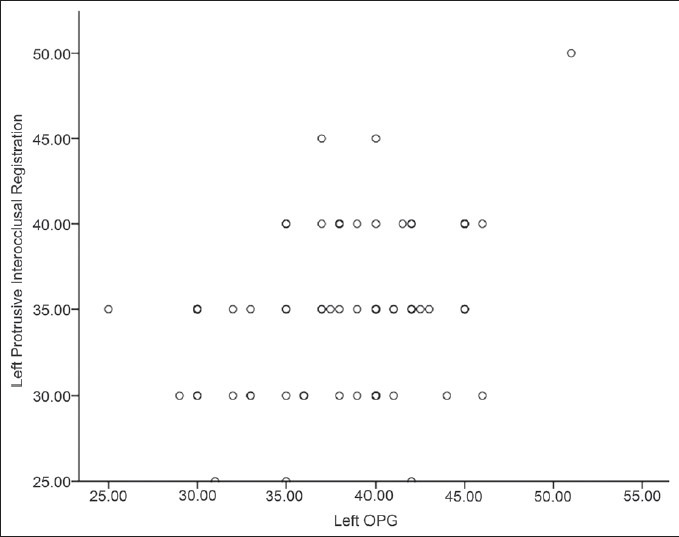
Correlation between condylar guidance values obtained using protrusive interocclusal registration and panoramic radiograph on left side (r = 0.291, P = 0.015)
A linear regression coefficient showed a strong degree of association between the two methods by the equation (y = a + bx), where y = dependent variable/condylar guidance set by interocclusal records, a = interceptor, 22.79 for left side and 18.44 for right side, b = coefficient, 0.34 for left side and 0.39 for right side, x = independent variable/condylar guidance set by the panoramic radiographic method.
Discussion
During any prosthodontic rehabilitation, it is of utmost importance to restore the patient's occlusion which coincides with centric relation and to provide an occlusion free of interference. Most articulators have condylar element glide-in-slots to provide a rectilinear stimulation of the curvilinear path of the condyle thus, producing a difference between the existing biological situation and the mechanical articulator.[9] Sometimes, frictional inhibition of movement of the condylar components of the articulator also introduces errors in the values of the condylar guidance.[12]
Radiographic determination of the condylar guidance has been attempted by the temporomandibular joint (TMJ) transpharyngeal view described by Mc Queen. The angle of condylar guidance was determined by relating the sagittal condylar path inclination to the Camper's plane (ala of the nose to the tragus).[11] However, the reproducibility of these TMJ specific views is suspect, as also the use of a reference plane which does not rely on stable bony landmarks can lead to further incorporation of errors. Condylar guidance on an articulator is adjusted utilizing either the patient's protrusive or lateral interocclusal registrations. The HANAU™ Wide-Vue Articulator with fixed intercondylar distance can be set using the protrusive interocclusal registration.[9] Following the protrusive interocclusal registration condylar guidance is measured in degrees relative to a plane of reference.[12] Condylar guidance inclination determined by two methods cannot be compared when obtained by different planes of reference. The present study utilized the (HANAU™ Spring Bow) which relies on the Frankfurt's horizontal plane to transfer the patient's relation to the articulator. The same plane is readily demonstrable on a panoramic radiograph by joining the porion and the orbitale landmarks [Figures 3 and 4].
The panoramic radiographic image of the sagittal outline of the articular eminence and glenoid fossae was clearly identified in 69 subjects. Six subjects were not considered in the final analysis because of radiographic artifacts. When viewing the region of the temporal bone on a panoramic radiograph two radio-opaque lines are apparent, the lighter and superior one depicting the articular eminence and fossa and the heavier, more inferior one representing the inferior border of the zygomatic arch. Inter-examiner reliability in identification of the radiographic outline of the articular eminence and determination of condylar guidance by the radiographic method showed suitable values of 0.911 on the right side and 0.933 on the left side.
The average condylar guidance by the interocclusal method was 34.71° on the right side and 35.00° on the left side. The mean condylar guidance values obtained using the radiographic method was 36.68° on the right side and 38.18° on the left side. Literature suggests that the right and left eminences seldom have exactly the same slants, contours, and declivities.[4] The average condyle path angle of left condyle reported using a gnathograph was 35.11°, and that of the right condyle was 36.02°.[1] In contrast, a bilateral symmetry of the right and left sagittal condylar guidance angle:31° on both sides has also been reported using protrusive interocclusal records.[13] Similarly, the present study showed a lesser mean difference of 0.29° between the right and left sides by the protrusive interocclusal record method than the 1.5° by the panoramic radiograph method, highlighting the inherent differences in the method of determination of condylar guidance.
A significant positive correlation was observed between the condylar guidance acquired using protrusive interocclusal records and panoramic images for both right (P 0.000) and left sides (P 0.015). A study comparing the radiographic image of the sagittal condylar path inclination and its actual anatomic outline in dry skulls and found that the radiographic values were on an average 7° greater than the skull values.[6] The present study found that the condylar guidance values by the radiographic method were greater by 1.97° and 3.18° than the protrusive interocclusal method for the right and left sides, respectively.
There are some limitations of the radiographic method concerning panoramic distortion, head and reference plane orientation, and difficulty in distinguishing the articular eminence outline from the zygomatic arch. The positions of these two lines relative to each other may vary if there is a change in beam direction due to positioning errors. Further, the articular eminence inclination in the radiographic image was traced by a line joining the heights of curvature in the glenoid fossa and the articular eminence to represent the mean sagittal condylar path inclination. This may be different from the guiding inclination with approximately 4-6 mm of protrusion, which is the clinically significant range of protrusion and condylar guidance.[13]
Despite these drawbacks, the panoramic radiograph is extremely useful for comparison between right and left sides since it shows both the TMJs with relatively same magnification errors (×1.2). It is a reproducible radiograph unlike the other TMJ specific radiographs which are subject to projection errors.[14] Although direct comparisons between a functional method and a radiographic method would seem improbable; the present study found a strong degree of correlation between the condylar guidance determined by the two methods. This was further demonstrated by the linear coefficient equation derived (y = a + bx) above.
Further studies on the variations in the sagittal condylar path inclination values in the panoramic radiographs are required to obtain normative data for our population
Conclusion
Considering the inaccuracies of the interocclusal record technique with inherent errors of up to 30°; the radiographic method may have clinical relevance. It suggests that such tracings may be made relative to a suitable horizontal reference plane like the Frankfurt horizontal and the resulting condylar guidance angles used to set the condylar guide settings of semi-adjustable articulators.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared
References
- 1.Isaacson D. A clinical study of the condyle path. J Prosthet Dent. 1959;9:927–35. [Google Scholar]
- 2.Academy of Prosthodontics. Glossary of prosthodontic terms. J Prosthet Dent. (8th ed) 2005;94:10–92. doi: 10.1016/j.prosdent.2005.03.013. [DOI] [PubMed] [Google Scholar]
- 3.Rothstein JR. Condylar guidance setting on articulators from protrusive records. J Prosthet Dent. 1972;28:334–5. doi: 10.1016/0022-3913(72)90228-4. [DOI] [PubMed] [Google Scholar]
- 4.Aull AE. Condylar determinants of occlusal patterns. J Prosthet Dent. 1965;15:826–49. doi: 10.1016/0022-3913(65)90122-8. [DOI] [PubMed] [Google Scholar]
- 5.Payne JA. Condylar determinants in a patient population: Electronic pantographic assessment. J Oral Rehabil. 1997;24:157–63. doi: 10.1046/j.1365-2842.1997.00452.x. [DOI] [PubMed] [Google Scholar]
- 6.Gilboa I, Cardash HS, Kaffe I, Gross MD. Condylar guidance: Correlation between articular morphology and panoramic radiographic images in dry human skulls. J Prosthet Dent. 2008;99:477–82. doi: 10.1016/S0022-3913(08)60112-2. [DOI] [PubMed] [Google Scholar]
- 7.Posselt U, Nevstedt P. Registration of the condyle path inclination by intra-oral wax records – Its practical value. J Prosthet Dent. 1961;1:43–7. [Google Scholar]
- 8.Preti G, Scotti R, Bruscagin C, Carossa S. A clinical study of graphic registration of the condylar path inclination. J Prosthet Dent. 1982;48:461–6. doi: 10.1016/0022-3913(82)90086-5. [DOI] [PubMed] [Google Scholar]
- 9.Harcourt JK. Accuracy in registration and transfer of prosthetic records. Aust Dent J. 1974;19:182–9. doi: 10.1111/j.1834-7819.1974.tb05036.x. [DOI] [PubMed] [Google Scholar]
- 10.Craddock FW. The accuracy and practical value of records of condyle path inclination. J Am Dent Assoc. 1949;38:697–710. doi: 10.14219/jada.archive.1949.0066. [DOI] [PubMed] [Google Scholar]
- 11.Boos RH. Condylar path by roentgenograph. J Prosthet Dent. 1951;1:387–92. doi: 10.1016/0022-3913(51)90022-4. [DOI] [PubMed] [Google Scholar]
- 12.dos Santos J, Jr, Nelson S, Nowlin T. Comparison of condylar guidance setting obtained from a wax record versus an extraoral tracing: A pilot study. J Prosthet Dent. 2003;89:54–9. doi: 10.1067/mpr.2003.11. [DOI] [PubMed] [Google Scholar]
- 13.Donegan SJ, Christensen LV. Sagittal condylar guidance as determined by protrusion records and wear facets of teeth. Int J Prosthodont. 1991;4:469–72. [PubMed] [Google Scholar]
- 14.Gray RJ, Quayle AA, Horner K, Al-Gorashi AJ. The effects of positioning variations in transcranial radiographs of the temporomandibular joint: A laboratory study. Br J Oral Maxillofac Surg. 1991;29:241–9. doi: 10.1016/0266-4356(91)90191-7. [DOI] [PubMed] [Google Scholar]