

Abstract
Appendicectomy for appendicitis is one of the commonest surgical procedures performed worldwide. The residual appendiceal stump left after an initial appendectomy risks the development of stump appendicitis. Stump appendicitis is a real recognized entity but not often considered when evaluating patients with right lower quadrant abdominal pain, especially those with past history of appendectomy. It remains a clinical challenge with the result that its diagnosis and effective treatment are often delayed with possible attendant morbidity or mortality. Stump appendicitis results from obstruction of the lumen of the remaining appendix stump, usually by a faecolith. This increases intraluminal pressure, impairing venous drainage and allowing subsequent bacterial infection. We present the case of a twenty-five (25)-year-old female who underwent laparoscopic appendicectomy and presented four and half (4(1/2)) months later with fever, right lower quadrant abdominal pain, and tenderness associated with repeated vomiting. Exploratory laparotomy was carried out after clinical and imaging studies which revealed big inflammatory mass with abscess at the right iliac fossa and recurrent appendicitis of the appendiceal stump. Surgical treatment is easy but recognition of this important entity but potentially dangerous condition should always be borne in mind in order to avoid delay in its diagnosis and treatment.
1. Introduction
Acute Appendicitis is one of the most common causes of abdominal pain, and it is one of the common surgical emergencies treated by general surgeons.
Most surgical personnel are quite familiar with the common complications after appendectomy such as wound infections and pelvic abscesses [1].
The postoperative development of stump appendicitis is an exceedingly rare entity with only 36 reported cases in the English language literature [2–4]. Stump appendicitis is an acute inflammation of the residual appendiceal stump and is an underreported complication that can occur after open or laparoscopic appendectomy [5–13].
The entity has been recorded as occurring from about three weeks to an interval of twenty-three (23) years after appendectomy, but our case presented only four and half (4(1/2)) months after laparoscopic appendectomy [14, 15].
With the introduction of laparoscopic appendectomy in the last fifteen to twenty (15–20) years; however, incidence of stump appendicitis has probably increased even though this was not supported by the findings of Liang et al. [3].
The fact that the diagnosis of stump appendicitis is usually not considered as the possible etiology for right lower quadrant abdominal pain in patients with prior appendectomy creates a delay in making the correct diagnosis and explains why the rate of perforation for stump appendicitis approaches 70% [16, 17].
We present this case of a twenty-five (25)-year-old female who presented in our emergency room (ER) department with right iliac fossa abdominal pain and repeated vomiting four and half (4(1/2)) months after laparoscopic appendectomy.
It is to draw attention to the fact that stump appendicitis with all its attendant complications such as perforation, abscess formation is real and should be borne in mind in the differential diagnosis of patients presented with right iliac fossa pain after appendectomy [18].
2. Case Report
A twenty-five (25)-year-old lady presented with a two-day history of stabbing abdominal pain located first in the epigastric area but later migrated to the right lower abdomen with associated repeated vomiting. This pain became more intense and continuous in the right lower abdomen.
Her last menstrual period was one week prior to presentation at the emergency room (ER).
Significant in her past medical history is the fact that she underwent laparoscopic appendectomy four and half (4(1/2)) months earlier.
On admission, the patient looked unwell with a fever of 38°C, BP = 90/60 mm Hg, and Pulse = 92/min RR = 28/min. Abdomen was tender all over but maximum in the right iliac fossa with guarding and rigidity. Bowel sounds were sluggish.
Plain abdominal X-ray and urinalysis were normal, but the total white cell count (WBC) was 19000 with 85% neutrophils.
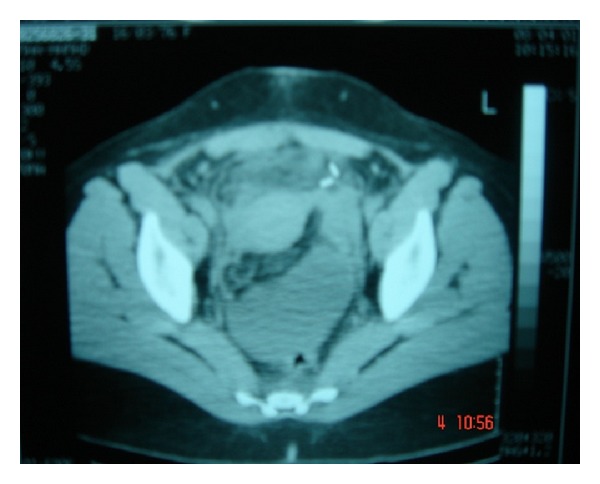
Abdominal ultrasound (U/S) (Figure 1) and abdominal computerized tomographic scan (CT) (Figure 2) revealed inflammatory, intraperitoneal collection at the right iliac fossa (RIF) which was diagnosed radiologically as an inflammatory mass with abscess.
Figure 1.

Figure 2.
IV fluid with parenteral antibiotics was commenced.
The patient underwent exploratory laparotomy through lower midline incision with a view to draining the abscess.
At laparotomy, a significant stump of the original appendix was left behind, inflamed with missed faecolith at the base of the appendix. It was perforated with abscess formation (Figures 3 and 4).
Figure 3.

Residual appendix.
Figure 4.

Suturing of base.
The appendiceal stump with the left-behind faecolith was ligated, abscess drained followed by peritoneal toilet and wound closed in layers with a drain left in situ.
Histopathological examination of the ligated appendix stump confirmed the presence of an appendix with inflammation of surrounding adjacent tissue and abscess (Figure 5).
Figure 5.
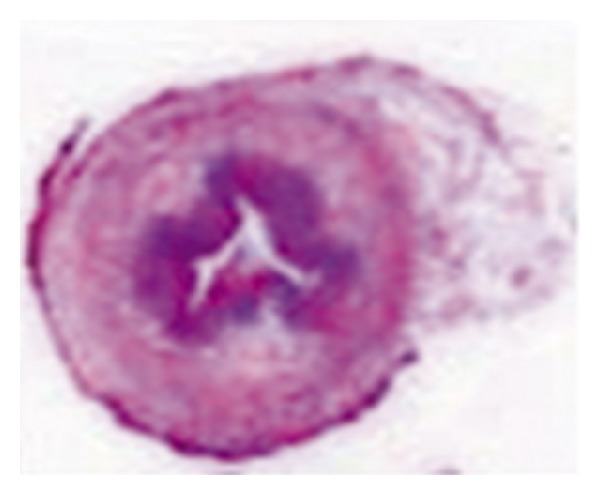
Slide of appendix.
Postoperatively, she did well and was discharged home after one week and has since been discharged from surgical outpatient followup.
3. Discussion and Conclusion
Baumgardner in 1949 [15] was the first to describe stump appendicitis, and since then a total of 36 cases have been reported in a comprehensive review of the English language literature [2, 3].
Some reports have suggested that laparoscopic appendectomy is associated with an increased incidence of stump appendicitis when compared with open appendectomy.
However, the most recent comprehensive review of the literature examining thirty-six (36) cases of stump appendicitis by Liang et al. [3] revealed that only 34% of cases were initially performed laparoscopically, and 66% were initially performed as open surgeries, thereby, supporting that it can occur after either laparoscopic or open appendectomy [19].
Stump appendicitis is a real entity not often considered when evaluating patients with right lower quadrant abdominal pain after appendectomy and may be probably an underreported problem [20, 21].
It can occur from about two (2) weeks to an interval of twenty-three (23) year after appendectomy but our case presented four and half (4(1/2)) months postlaparoscopic appendicectomy [14, 15].
Preoperative stump appendicitis diagnosis is still clinical because typically patients present with signs and symptoms similar to acute appendicitis.
Clinicians should have a high index of suspicion for stump appendicitis [22, 23] in patients with a history of previous appendectomy who presented with an acute appendicitis-like picture [24, 25].
Plain films, USD, and CT [26] may all play a role in its diagnosis especially in those associated with abscess formation or perforated cases with intraperitoneal fluid collection in the right lower abdomen or in the pelvis.
The surgical error commonly ascribed to either technique of open or laparoscopic method is the inability in not adequately identifying the base of the appendix, thereby resulting in failure to completely remove [21] the appendix during the initial operation of appendicetomy.
Some authors have suggested stump inversion routinely in all cases after removal of the appendix as a way of minimizing the incidence of stump appendicitis, but others think this is not necessary as long an appendiceal stump of not more than 3 mm in depth is left behind [27, 28].
Different methods of dealing with stump appendicitis include reappendectomy with or without stump inversion, or even limited right hemicolectomy [21, 29, 30].
In our case during exploratory laparotomy, the appendiceal stump with the left behind faecolith was ligated, its base sutured, and the accompanying abscess was drained, followed by peritoneal toilet, abdominal closure and a drain left in situ.
We, therefore, recommend early recognition of this clinical entity to decrease morbidity and high rate of perforation associated with delayed diagnosis [7, 18, 31, 32].
It has therefore been proposed that diagnosis of stump appendicitis should be borne in mind in the differential diagnosis of patients presented with right lower abdominal pain with past history of appendectomy.
References
- 1.Cama JK. Recurrent abdominal pain post appendectomy: a rare case. Pacific Health Dialog. 2010;16(2):78–81. [PubMed] [Google Scholar]
- 2.Subramanian A, Liang MK. A 60-year literature review of stump appendicitis: The need for a critical view. The American Journal of Surgery. 2012;203(4):503–507. doi: 10.1016/j.amjsurg.2011.04.009. [DOI] [PubMed] [Google Scholar]
- 3.Liang MK, Lo HG, Marks JL. Stump appendicitis: a comprehensive review of literature. The American Surgeon. 2006;72(2):162–166. [PubMed] [Google Scholar]
- 4.Watkins BP, Kothari SN, Landercasper J. Stump appendicitis: case report and review. Surgical Laparoscopy, Endoscopy and Percutaneous Techniques. 2004;14(3):167–171. doi: 10.1097/01.sle.0000129392.75673.97. [DOI] [PubMed] [Google Scholar]
- 5.Baek SK, Kim MS, Kim YH, Chung WJ, Kwon JH. A case of stump appendicitis after appendectomy. The Korean Journal of Gastroenterology. 2008;51(1):45–47. [PubMed] [Google Scholar]
- 6.Bosma E, Roukema JA, Verhofstad MHJ. Stump appendicitis after previous appendicectomy. Nederlands Tijdschrift voor Geneeskunde. 2008;152(19):1113–1116. [PubMed] [Google Scholar]
- 7.Uludag M, Isgor A, Basak M. Stump appendicitis is a rare delayed complication of appendectomy: a case report. World Journal of Gastroenterology. 2006;12(33):5401–5403. doi: 10.3748/wjg.v12.i33.5401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Burt BM, Javid PJ, Ferzoco SJ. Stump appendicitis in a patient with prior appendectomy. Digestive Diseases and Sciences. 2005;50(11):2163–2164. doi: 10.1007/s10620-005-3025-7. [DOI] [PubMed] [Google Scholar]
- 9.Truty MJ, Stulak JM, Utter PA, Solberg JJ, Degnim AC. Appendicitis after appendectomy. Archives of Surgery. 2008;143(4):413–415. doi: 10.1001/archsurg.143.4.413. [DOI] [PubMed] [Google Scholar]
- 10.Bu-Ali O, Al-Bashir M, Samir HA, Abu-Zidan FM. Stump appendicitis after laparoscopic appendectomy: case report. Ulusal Travma ve Acil Cerrahi Dergisi. 2011;17(3):267–268. doi: 10.5505/tjtes.2011.47123. [DOI] [PubMed] [Google Scholar]
- 11.Nielsen-Breining M, Nordentoft T. Stump appendicitis after laparoscopic appendectomy. Ugeskrift for Laeger. 2005;167(19):2067–2068. [PubMed] [Google Scholar]
- 12.Parameshwarappa S, Rodrigues G, Prabhu R, Sambhaji C. Stump appendicitis following laparoscopic appendectomy. Sultan Qaboos University Medical Journal. 2011;11(1):112–114. [PMC free article] [PubMed] [Google Scholar]
- 13.Walsh DCA, Roediger WEW. Stump appendicitis: a potential problem after laparoscopic appendicectomy. Surgical Laparoscopy, Endoscopy and Percutaneous Techniques. 1997;7(4):357–358. [PubMed] [Google Scholar]
- 14.Siegel SA. Appendiceal stump abscess: a report of stump abscess twenty-three years postappendectomy. The American Journal of Surgery. 1954;63(4):630–632. doi: 10.1016/0002-9610(54)90306-2. [DOI] [PubMed] [Google Scholar]
- 15.Baumgardner LO. Rupture of appendiceal stump three months after uneventful appendicectomy with repair and recovery. Ohio State Medical Journal. 1949;45:476–477. [PubMed] [Google Scholar]
- 16.Ismail I, Iusco D, Jannaci M, et al. Prompt recognition of stump appendicitis is important to avoid serious complications: a case report. Cases Journal. 2009;2(7, article 7415) doi: 10.4076/1757-1626-2-7415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roberts KE, Starker LF, Duffy AJ, Bell RL. Stump appendicitis: a surgeon's dilemma. Journal of the Society of Laparoendoscopic Surgeons. 2011;15(3):373–378. doi: 10.4293/108680811X13125733356954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Roche-Nagle G, Gallagher C, Kilgallen C, Caldwell M. Stump appendicitis: a rare but important entity. Surgeon. 2005;3(1):53–54. doi: 10.1016/s1479-666x(05)80015-0. [DOI] [PubMed] [Google Scholar]
- 19.Leff DR, Sait MR, Hanief M, Salakianathan S, Darzi AW, Vashisht R. Inflammation of the residual appendix stump: a systematic review. Colorectal Disease. 2010;(10):1463–1318. doi: 10.1111/j.1463-1318.2010.02487.x. [DOI] [PubMed] [Google Scholar]
- 20.Mangi AA, Berger DL. Stump appendicitis. The American Surgeon. 2000;66(8):739–741. [PubMed] [Google Scholar]
- 21.Werbin N. Unfinished surgery. Harefuah. 2005;144(12):894–908. [PubMed] [Google Scholar]
- 22.O’Leary DP, Myers E, Coyle J, Wilson I. Case report of recurrent acute appendicitis in a residual tip. Cases Journal. 2010;3(1, article 14) doi: 10.1186/1757-1626-3-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Rosón Rodríguez PJ, Victória Toscano Castilla E, Cotta Rebollo J, Lozano Lanagran M, Lopez Vega MC. Appendicitis of the appendicular stump: apropos of a case propósito de un caso. Gastroenterologia y Hepatologia. 2011;34(10):722–723. doi: 10.1016/j.gastrohep.2011.08.001. [DOI] [PubMed] [Google Scholar]
- 24.Al-Dabbagh AK, Thomas NB, Haboubi N. Stump appendicitis: a diagnostic dilemma. Techniques in Coloproctology. 2009;13(1):73–74. doi: 10.1007/s10151-008-0419-5. [DOI] [PubMed] [Google Scholar]
- 25.Robledo-Ogazón F, Bojalil-Durán L, Vargas-Rivas A, Torres-Vieyra L, Valle-Carmona Y. Appendiceal stump appendicitis: case report. Cirugia y Cirujanos. 2005;73(4):311–314. [PubMed] [Google Scholar]
- 26.Romesburg J, Imam K. Stump appendicitis. Applied Radiology. 2010;39(10):36–38. [Google Scholar]
- 27.Belli S, Yalçinkaya C, Ezer A, Bolat F, Çolakoğlu T, Şimşek E. Stump appendicitis and chorioamnionitis due to incomplete appendectomy: a case report. Turkish Journal of Gastroenterology. 2011;22(5):540–543. doi: 10.4318/tjg.2011.0265. [DOI] [PubMed] [Google Scholar]
- 28.Durgun AV, Baca B, Ersoy Y, Kapan M. Stump appendicitis and generalized peritonitis due to incomplete appendectomy. Techniques in Coloproctology. 2003;7(2):102–104. doi: 10.1007/s10151-003-0018-4. [DOI] [PubMed] [Google Scholar]
- 29.De U, De Krishna K. Stump appendicitis. Journal of the Indian Medical Association. 2004;102(6):p. 329. [PubMed] [Google Scholar]
- 30.Tang XB, Qu RB, Bai YZ, Wang WL. Stump appendicitis in children. Journal of Pediatric Surgery. 2011;46(1):233–236. doi: 10.1016/j.jpedsurg.2010.09.049. [DOI] [PubMed] [Google Scholar]
- 31.Erzurum VZ, Kasirajan K, Hashmi M. Stump appendicitis: a case report. Journal of Laparoendoscopic and Advanced Surgical Techniques A. 1997;7(6):389–391. doi: 10.1089/lap.1997.7.389. [DOI] [PubMed] [Google Scholar]
- 32.Aschkenasy MT, Rybicki FJ. Acute appendicitis of the appendiceal stump. Journal of Emergency Medicine. 2005;28(1):41–43. doi: 10.1016/j.jemermed.2004.07.007. [DOI] [PubMed] [Google Scholar]