

Abstract
Acute respiratory distress syndrome (ARDS) is common in critically ill patients admitted to intensive care units (ICU). ARDS results in increased use of critical care resources and healthcare costs, yet the overall mortality associated with these conditions remains high. Research focusing on preventing ARDS and identifying patients at risk of developing ARDS is necessary to develop strategies to alter the clinical course and progression of the disease. To date, few strategies have shown clear benefits. One of the most important obstacles to preventive interventions is the difficulty of identifying patients likely to develop ARDS. Identifying patients at risk and implementing prevention strategies in this group are key factors in preventing ARDS. This review will discuss early identification of at-risk patients and the current prevention strategies.
Review
Introduction
Acute respiratory distress syndrome (ARDS) is common in critically ill patients admitted to intensive care units (ICU).
Multiple hit model for ALI/ARDS development
Previous studies support a two-hit model of ARDS development in which exposure to pertinent risk factors modifies the development and expression of ARDS in a host with predisposing conditions [1-3]. However, beyond the development of ARDS in a susceptible host, theories of the pathogenesis of this condition should explain progression from an initial lung injury to mild ARDS or from mild or moderate to severe ARDS. To this end, a chain reaction based on multiple hits can be involved in the pathogenesis of ARDS development and/or the progression of severity [4]. Host predisposing conditions act as a first hit in healthy lungs, where multiple hit can induce ARDS. In the absence of these predisposing conditions, the probability that the other hits would result in ARDS is lower. Whether the disease progresses from an initial injury to ARDS or continues to progress from mild-moderate ARDS to severe ARDS probably depends on a chain reaction based on these multiple hits (Figure 1).
Figure 1.
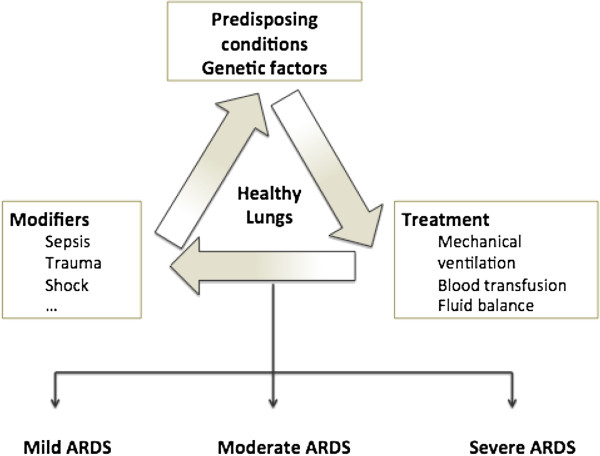
Multiple-hit model. A chain reaction of predisposing conditions and multiple hits (modifiers factors and treatments) in healthy lungs can develop mild, moderate or severe ARDS.
Hudson et al. [5] found the presence of one or more of eight clinical conditions (sepsis, aspiration, drug overdose, near-drowning, pulmonary contusion, multiple transfusions, multiple fractures, head trauma) predicted whether ARDS develops with 79% sensitivity but only 26% specificity. Fowler et al. [6] found pneumonia, aspiration, and disseminated intravascular coagulation were the strongest predictors but only 7% of the patients with one or more predisposing factors developed ALI. Gong et al. [7] showed the risk of ARDS increased with a pulmonary etiology of injury, hematologic failure, transfusion of eight or more units of packed red blood cells, respiratory rate > 33 breaths/min, hematocrit > 37.5%, arterial pH < 7.33, albumin ≤ 2.3 g/dL, and transfer from another hospital. In another study in non-ICU hospitalized patients, Ferguson et al. [8] found that pulmonary risk conditions had a higher rate of progression to ARDS than nonpulmonary conditions, but shock was the strongest predictor. Therefore, by halting this unvirtous circle might help to stop the progression to ARDS.
Towards prevention. Early recognition
Identification of patients at risk
The first obstacle to preventing ARDS is identifying patients at risk of developing ARDS [9]. Many authors have proposed clinically detectable predisposing factors and even scores to identify patients at risk early in the course of the disease. Implementing preventive measures requires an algorithm for early detection. Different algorithms have been proposed. Trillo-Alvarez et al. [10] developed an ALI prediction score, the lung injury prediction score (LIPS), that identifies patients at high risk for ALI before ICU admission. Risk factors are divided into predisposing conditions (sepsis, shock, pneumonia, aspiration, trauma, and high risk-surgery) and risk modifiers (obesity, alcohol abuse, diabetes, hypoalbuminemia, acidosis, tachypnea, and oxygen supplementation). Gajic et al. [11] validated this score in a prospective, multicenter, observational study, demonstrating that the LIPS model discriminates efficiently between patients who have a low risk of developing ARDS and those with high risk (AUC = 0.8), while maintaining an appropriate sensitivity for screening (negative predictive value (NPV) = 0.97).
In 2010, Thakur et al. [12] reported a cohort study designed to identify patients at risk early before ARDS develops, using an electronic medical record that facilitates early recognition of specific criteria, based on a previously validated ARDS sniffer (NPV = 0.99, 95% confidence interval (CI) 0.98-1.00) [13]. They identified patients at risk by the LIPS score and recorded hospital-acquired exposures that may modify the risk of ARDS and its impact on subgroups of high-risk patients. Levitt et al. [14] proposed the term “early ALI” (EALI). EALI identified patients progressing to ARDS with a sensitivity of 73% and a specificity of 79%. The combination of early clinical recognition and predictive scores could help in the detection of patients at-risk and in the early treatment or implementation of preventive strategies.
Biomarkers
Identifying a biomarker that predicts the development of ARDS or progression of severity could be helpful. The ideal biomarker would be easy and safe to collect, easily measured and reproducible, highly sensitive and specific in predicting clinical outcome, and have a defined role in the pathogenesis of ARDS [15]. Unfortunately, no single biomarker is currently specific or sensitive enough to be incorporated into routine clinical practice.
Volatile organic compounds in exhaled air may differ between diseases. Bos et al. [16,17] conducted two studies where they discriminated between mechanically ventilated patients with and without ARDS on the basis of a breathprint obtained by analyzing exhaled air through eNose technology. This breathprint distinguished between patients with ARDS and those without as accurately as PaO2/FiO2 assessment. Noninvasive analysis of exhaled air may help to identify a biomarker to detect ARDS in an early stage, before clinical signs; however, further studies are needed before this approach can be incorporated into routine clinical practice.
Other biomarkers in plasma or bronchoalveolar lavage fluid have been studied in patients with ARDS. A recent trial in critically ill patients demonstrated that higher levels in plasma of angiopoetin-2 were significantly associated with increased development of ALI (odds ratio (OR) 2.4; 95% CI 1.3-4.2) [18].
Furthermore, the association of angiopoetin-2 levels and the LIPS improved the AUC to 0.84. Because there is no ideal biomarker to help us in the early detection of ARDS, the association between biomarkers and different scoring systems based on clinical data or diagnostic tests could improve prediction scores [19,20].
Genetic predisposition
There is some evidence that genetic factors predispose to the development of ARDS and poor prognosis. Copland et al. [21] used an experimental model of acute ventilator-induced lung injury (VILI) to determine which genes changed their expression depending on inspiratory volumes, and they identified various genes with overexpression. One of the most important studies is from Grigoryev et al. [22], who identified 85 genes important in the pathogenesis and different biologic processes involved in the development of ARDS.
Nevertheless, at present, we cannot identify a single gene responsible for a high susceptibility to ARDS. Some studies are currently trying to evaluate the role of single nucleotide polymorphism (SNPs) and haplotypes in order to better detect patients at ARDS risk. These studies could help to define new therapeutic targets, new approaches to treatment, and individual indicators of predisposition to developing the disease that might enable the development of effective preventive strategies.
Pathogen virulence
Defining risk factors associated with the development of ARDS in patients with an infectious disease is challenging because virulence factors of different pathogens have been implicated in causing lung damage. Bacterial products are directly toxic to the lung epithelium, independent of host inflammatory responses and other factors [23]. Kojicic et al. [24] recently found that the risk of hospitalized patients with infectious pneumonia developing ALI varied with the pulmonary pathogens.
Preventive measures
Beyond the etiology, certain modifiable external factors can accelerate the development of ARDS.
Mechanical ventilation
Lung protective ventilation Lung-protective mechanical ventilation strategies are the only supportive therapy that clearly improve survival in patients with ARDS. However, mechanical ventilation can lead to lung injury by different mechanisms, with subsequent diffuse alveolar damage, pulmonary edema, and local production of inflammatory mediators. This circumstance is known as VILI.
Tremblay et al. [25] showed that mechanical ventilation with high volumes and without positive end-expiratory pressure (PEEP) could increase tumor necrosis factor (TNF-alpha) and interleukin-6 (IL-6) concentrations in bronchoalveolar lavage fluid, whereas cytokine levels are lower if protective mechanical ventilation is used. Amato et al. [26] demonstrated lower mortality in patients ventilated with a limited tidal volume to avoid overdistension. A prospective, multicenter trial (ARDS Network) published in 2000 confirmed that mechanical ventilation with lower tidal volume (6 mL/Kg predicted body weight (PBW)) resulted in an increase in the number of ventilator-free days and a reduction of in-hospital mortality [27].
Mechanical ventilation is an important factor in the treatment of ARDS, but is it important in prevention? Does mechanical ventilation work as a risk modifier in patients at risk? Could we help to prevent the development of ARDS by applying protective mechanical ventilation in patients at risk?
In a recent study, our group found that septic patients without ARDS ventilated with a protective strategy using a plateau pressure < 30 cmH20 had better outcomes and a lower incidence of ARDS than those ventilated without this limit on plateau pressure [28]. Thus, it may be beneficial to implement protective ventilation strategies from the start of mechanical ventilation, not only when ARDS appears. It remains to be determined whether only plateau pressure should be targeted or whether tidal volume should be targeted too. In our opinion, preventive strategies also should include protective ventilation with low tidal volume in patients at risk, and some studies support this approach. In 2004, Gajic et al. [29] reported that in ventilated patients without ARDS large tidal volumes (11.4 mL/kg PBW for women and 10.4 mL/kg PBW for men) were independently associated with the development of ARDS. In a prospective trial, Determann et al. [30] randomized patients who required mechanical ventilation to receive low tidal volume (6 mL/kg PBW) or conventional tidal volume (10 mL/kg PBW); the trial was stopped prematurely because more patients in the conventional tidal-volume group developed ARDS than in the lower tidal-volume group (13.5 vs. 2.6; p = 0.01).
Interestingly, the use of protective ventilation in “healthy lungs” seems to be a field for further research. A recently published meta-analysis, including eight trials that evaluated two types of mechanical ventilation in patients with uninjured lungs in the operating room, demonstrated a decrease in lung injury development, pulmonary infection, and atelectasis using lower tidal volumes and high PEEP [31]. These results support the previous meta-analysis that demonstrated only an attenuation of the development of lung injury, conducted with trials that included patients in operating room and ICU [32].
No concrete ventilation strategies have been established for patients without ARDS who require mechanical ventilation. We think that ventilation with low tidal volumes and plateau pressure < 30 cmH2O is a reasonable prevention strategy of ARDS. Side effects associated with low tidal volumes seem to be minimal. However, based on a review by Schultz et al. [33], most studies favoring low tidal volume ventilation in patients without ARDS measured inflammatory mediators instead of clinical outcomes, so prospective trials should be done to evaluate the clinical impact of this ventilatory strategy.
PEEP strategies
The use of prophylactic PEEP in patients without ARDS is controversial. Various authors have demonstrated that prophylactic PEEP decreases the incidence of ARDS and PEEP may protect the lung after different types of insults. In the 1970s it was demonstrated that intraoperative use of PEEP reduced ARDS development [34] and the use of early prophylactic PEEP reduced the incidence of ARDS [35]. Other studies demonstrated that the use of certain amount of PEEP reduced the intensity of lung injury from different aggressions, as Dreyfuss et al. showed in 1988 with the reduction of edema and preservation of the normal structural aspect of alveolar epithelium using high levels of PEEP [36,37]. However, other studies have refuted this effect. Pepe et al. conducted a trial where found that the early application of PEEP in high-risk patients had no effect on the incidence of ARDS [38]. Manzano et al. [39] conducted a randomized trial where nonhypoxemic patients without lung injury received 5 cmH2O or 8 cmH2O PEEP versus no PEEP. They found no differences between groups in the development of ARDS, but the proportion of patients who developed hypoxemia was significantly higher in the no-PEEP group and the PEEP group developed less ventilator-associated pneumonia (relative risk (RR) 0.37; 0.15-0.84).
The use of higher tidal volumes, based on older strategies, arose from a need to prevent atelectasis. PEEP strategies are now better understood and the risk of over distension better appreciated. So, this need has lessened.
Supportive treatments
Fluid balance
Fluid balance is an important risk modifier in the development of ARDS. Pulmonary edema is largely due to increased capillary permeability but is exacerbated by increased hydrostatic pressures and oncotic pressure falls [40]. The first reports about fluid strategies date from 1987, when Simmons et al. [41] observed that outcomes in ARDS patients were better if they lost body weight and had a lower fluid balance. Sakr et al. [42] in a cohort observational study showed that a higher mean fluid balance was independently associated with increased mortality in patients with ARDS. In 2006, the ARDS Network published the results of a prospective, randomized trial comparing conservative and liberal fluid strategies in patients with ARDS. The authors included patients after 48 hours of ICU admission and with systolic blood pressure > 60 mmHg. The primary outcome (60-day mortality) did not differ between groups, but the conservative group had better oxygenation index and lung injury scores, as well as more ventilator-free days [43]. A limitation of this study is the exclusion of hemodynamically unstable patients that difficult the generalization of the results to all patients with ARDS. On the other hand, Murphy et al. [44] showed in a retrospective analysis of patients with septic shock and ARDS that an adequate initial fluid resuscitation during the first 2 consecutive days coupled with conservative fluid management after that was associated with the lowest mortality. Despite the above, no randomized trials have been done evaluating a two-phase fluid management strategy that could confirm this strategy. Thus, in patients with established ARDS, it seems that a conservative fluid strategy should be used, but it is difficult to know the role of fluid balance in the absence of ARDS.
Sepsis management
Sepsis precipitates ARDS in 25% to 40% of cases, and the risk increases if a systemic inflammatory response, shock, or organ dysfunction is present. The most frequent etiology is pneumonia, followed by nonpulmonary infections [45]. There is no specific preventive treatment against the development of ARDS in patients with sepsis. Novel therapies are being studied, but no promising results have been reported. It seems that early detection of patients with sepsis who are at risk of developing ARDS is one way to achieve better results in the earliest phase. Indeed, one of the most important preventive strategies is to ensure adequate management of sepsis, including source control and early appropriate antibiotic therapy [46,47].
Restrictive transfusion
Several studies have demonstrated an association between the transfusion of blood products and ARDS. Zilberberg et al. [48] showed that more patients who developed ARDS had received red cell transfusions than those who did not develop ARDS; moreover, they found that transfusion of greater amounts increased the risk of developing ARDS. Many authors have since confirmed this association [7,45,49,50].
Transfusion-related acute lung injury (TRALI) is defined as new ARDS during or within 6 hours after an infusion of one or more plasma-containing or plasma-derived blood products [51].
The neutrophil has been postulated that is the responsible cell in the pathogenesis of TRALI. In 1985 Popovsky et al. published a sequence of patients who developed TRALI after blood transfusion and demonstrated the presence of leukocyte antibodies and antibodies anti-HLA in a high percentage of blood donators. It was thought that donors’ antibodies were responsible of TRALI, but some transfused patients did not develop TRALI despite the presence of leukocyte antibodies [52].
Silliman et al. proposed a nonimmune model based on two hits: first, a lung injury in the lung epithelium causes sequestration of neutrophils in the lungs, and second, the transfusion of blood storage causes liberation of cytotoxic factors and capillary damage. This concept is because blood storage products are correlated with a high development of transfusion reactions, and factors responsible of these reactions increase with time of storage [53].
The activated neutrophils release oxygen radicals and other elements that damage the lung endothelium. Despite this, there are clinical and experimental evidence of TRALI without neutrophil primo activation, but it is the underlying disease that activates the endothelium and after that neutrophils are recruited in lung capillaries.
These theories of pathogenesis suggest different preventive strategies. Several studies have demonstrated worse outcomes after donation from multiparous women, because the likelihood of HLA and HNA immunization increases with the number of pregnancies [54-56]. Because of this, many authors suggest the restriction of women donors [57-59]. Although it could seem disproportioned, the option of the screening of donors is expensive and not available in all sites.
The strategy of reduction the time of blood storage seems reasonable to prevent nonimmune TRALI. Another option is the leukoreduction, reducing the activity of preactivated neutrophils. It has been introduced in many countries [60]. An adequate policy of transfusion focused on less transfusion is perhaps the most important preventive strategy [61].
Specific strategies
Many trials are underway to test whether different pharmacologic treatments have beneficial effects, but many pharmacologic therapies that prove effective in animal models fail in human studies. To date, there is no specific pharmacologic treatment for the prevention of ALI/ARDS.
Activated protein C
Activated protein C (APC) has several anti-inflammatory effects that may reduce the likelihood and severity of lung injury. In ARDS, acute inflammation in pulmonary compartments is characterized by fibrin formation, cytokine production, and protein leakage into the alveolar space due to increased capillary barrier permeability and neutrophil migration. All of these are potential targets of recombinant human APC. Local administration of APC would be a good treatment strategy in ARDS, avoiding the bleeding complications associated with systemic administration.
It might be feasible to administer APC to ARDS patients by inhalation. Administering inhaled APC to mice significantly reduced lipopolysaccharide-induced pulmonary inflammation [62]. Another experimental study tested the preventive effect of inhaled APC against lung injury in mice and found a reduction in lung injury induced by mechanical ventilation in the group that received inhaled APC [63].
Nevertheless, the evidence supporting the use of APC is not strong enough to recommend it for the prevention of ARDS. We need more studies.
Mesenchymal stem cells
Recent studies using experimental models of ALI have demonstrated that the transplantation of mesenchymal stem cells (MSCs) improves the regeneration of lung tissue [64]. The benefits MSCs are derived not only from the incorporation of these cells in the damaged lung, but also from their interaction with damaged lung cells and immunologic modulation. Most of these studies administered MSCs as a pretreatment; one study in rats showed pretreatment with MSCs reduced VILI [65]. However, the use of MSCs is still highly experimental and more studies are necessary before they can be applied as a treatment or prevention strategy.
Other treatments
Aspirin, statins, inhaled corticosteroids, and beta-2 adrenergic agonists have been tested in experimental studies but have yet to show promising results in human patients. More studies are necessary before these drugs can be incorporated into preventive strategies [66]. Although there is still a long way to go in the ARDS prevention field, some new strategies and preliminary studies promise to improve the early identification and early intervention to prevent the progression of the disease (Figure 2).
Figure 2.

Preventive approaches to ARDS.
Conclusions
ARDS is a common and devastating complication after acute illness or injury, and it results in high morbidity, mortality, and healthcare costs. Lung-protective ventilation and appropriate sepsis management seems to be the only strategies proven to improve outcomes in ARDS patients; preventive strategies are a new field of research aiming to avoid the progression of the disease. To date, few preventive strategies have shown clear benefits. The combination of early clinical recognition and predictive scores could help to identify patients at risk and those who might progress to mild, moderate, or severe ARDS. The titration of tidal volume and the duration of mechanical ventilation in patients without ARDS seem to be the best strategy for prevention.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors contributed to the drafting of the manuscript and approved the final version.
Contributor Information
Candelaria de Haro, Email: cdeharo@tauli.cat.
Ignacio Martin-Loeches, Email: drmartinloeches@gmail.com.
Eva Torrents, Email: etorrents@tauli.cat.
Antonio Artigas, Email: aartigas@tauli.cat.
References
- Matthay MA, Zimmerman GA, Esmon C, Bhattacharya J, Coller B, Doerschuk CM, Floros J, Gimbrone MA, Hoffman E, Hubmayr RD, Leppert M, Matalon S, Munford R, Parsons P, Slutsky AS, Tracey KJ, Ward P, Gail DB, Harabin AL. Future research directions in acute lung injury: summary of a National Heart, Lung, and Blood Institute working group. Am J Respir Crit Care Med. 2003;3:1027–1035. doi: 10.1164/rccm.200208-966WS. [DOI] [PubMed] [Google Scholar]
- Charles PE, Tissières P, Barbar SD, Croisier D, Dufour J, Dunn-Siegrist I, Chavanet P, Pugin J. Mild-stretch mechanical ventilation upregulates toll-like receptor 2 and sensitizes the lung to bacterial lipopeptide. Crit Care. 2011;3(4):R181. doi: 10.1186/cc10330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Villar J, Cabrera N, Casula M, Flores C, Valladares F, Muros M, Blanch L, Slutsky AS, Kacmarek RM. Mechanical ventilation modulates Toll-like receptor signaling pathway in a sepsis-induced lung injury model. Intensive Care Med. 2010;3(6):1049–1057. doi: 10.1007/s00134-010-1799-3. [DOI] [PubMed] [Google Scholar]
- Pavord ID, Birring SS, Berry M, Green RH, Brightling CE, Wardlaw AJ. Multiple inflammatory hits and the pathogenesis of severe airway disease. Eur Respir J. 2006;3(5):884–888. doi: 10.1183/09031936.06.00128105. [DOI] [PubMed] [Google Scholar]
- Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med. 1995;3:293–301. doi: 10.1164/ajrccm.151.2.7842182. [DOI] [PubMed] [Google Scholar]
- Fowler AA, Hamman RF, Good JT, Benson KN, Baird M, Eberle DJ, Petty TL, Hyers TM. Adult respiratory distress syndrome: risk with common predispositions. Ann Intern Med. 1983;3:593–597. doi: 10.7326/0003-4819-98-5-593. [DOI] [PubMed] [Google Scholar]
- Gong MN, Thompson BT, Williams P, Pothier L, Boyce PD, Christiani DC. Clinical predictors of and mortality in acute respiratory distress syndrome: potential role of red cell transfusion. Crit Care Med. 2005;3:1191–1198. doi: 10.1097/01.CCM.0000165566.82925.14. [DOI] [PubMed] [Google Scholar]
- Ferguson ND, Frutos-Vivar F, Esteban A, Gordo F, Honrubia T, Peñuelas O, Algora A, García G, Bustos A, Rodríguez I. Clinical risk conditions for acute lung injury in the intensive care unit and hospital ward: a prospective observational study. Crit Care. 2007;3:R96. doi: 10.1186/cc6113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levitt JE, Matthay MA. Clinical review: early treatment of acute lung injury - paradigm shift toward prevention and treatment prior to respiratory failure. Crit Care. 2012;3:223. doi: 10.1186/cc11144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trillo-Alvarez C, Cartin-Ceba R, Kor DJ, Kojicic M, Kashyap R, Thakur S, Thakur L, Herasevich V, Malinchoc M, Gajic O. Acute lung injury prediction score: derivation and validation in a population-based sample. Eur Respir J. 2011;3:604–609. doi: 10.1183/09031936.00036810. [DOI] [PubMed] [Google Scholar]
- Gajic O, Dabbagh O, Park PK, Adesanya A, Chang SY, Hou P, Anderson H, Hoth JJ, Mikkelsen ME, Gentile NT, Gong MN, Talmor D, Bajwa E, Watkins TR, Festic E, Yilmaz M, Iscimen R, Kaufman DA, Esper AM, Sadikot R, Douglas I, Sevransky J, Malinchoc M. Early identification of patients at risk of acute lung injury: evaluation of lung injury prediction score in a multicenter cohort study. Am J Respir Crit Care Med. 2011;3:462–470. doi: 10.1164/rccm.201004-0549OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thakur SJ, Trillo-Alvarez CA, Malinchoc MM, Kashyap R, Thakur L, Ahmed A, Reriani MK, Cartin-Ceba R, Sloan JA, Gajic O. Towards the prevention of acute lung injury: a population based cohort study protocol. BMC Emerg Med. 2010;3:8. doi: 10.1186/1471-227X-10-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herasevich V, Yilmaz M, Khan H, Hubmayr RD, Gajic O. Validation of an electronic surveillance system for acute lung injury. Intensive Care Med. 2009;3:1018–1023. doi: 10.1007/s00134-009-1460-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levitt JE, Bedi H, Calfee CS, Gould MK, Matthay MA. Identification of early acute lung injury at initial evaluation in an acute care setting prior to the onset of respiratory failure. Chest. 2009;3:936–943. doi: 10.1378/chest.08-2346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moriates C, Maisel A. The utility of biomarkers in sorting out the complex patient. Am J Med. 2010;3:393–399. doi: 10.1016/j.amjmed.2009.07.034. [DOI] [PubMed] [Google Scholar]
- Bos LDJ, Fens N, van der Schee MP, Sterk P, Schultz MJ. Fast assessment of ALI/ARDS in the ICU using exhaled breath analysis. Am J Respir Crit Care Med. 2010;3:A2583. [Google Scholar]
- Bos LDJ, Sterk PJ, Schuktz MJ. Exhaled breath analysis in the diagnosis of acute lung injury. Am J Respir Crit Care Med. 2011;3:A1163. [Google Scholar]
- Agrawal A, Matthay MA, Kangelaris KN, Stein J, Chu JC, Imp BM, Cortez A, Abbott J, Liu KD, Calfee CS. Plasma angiopoietin-2 predicts the onset of acute lung injury in critically Ill patients. Am J Respir Crit Care Med. 2013. [Epub ahead of print] [DOI] [PMC free article] [PubMed]
- Ware LB, Koyama T, Billheimer DD, Wu W, Bernard GR, Thompson BT, Brower RG, Standiford TJ, Martin TR, Matthay MA. NHLBI ARDS Clinical Trials Network. Prognostic and pathogenetic value of combining clinical and biochemical indices in patients with acute lung injury. Chest. 2010;3(2):288–296. doi: 10.1378/chest.09-1484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calfee CS, Ware LB, Glidden DV, Eisner MD, Parsons PE, Thompson BT, Matthay MA. National Heart, Blood, and Lung Institute Acute Respiratory Distress Syndrome Network. Use of risk reclassification with multiple biomarkers improves mortality prediction in acute lung injury. Crit Care Med. 2011;3(4):711–717. doi: 10.1097/CCM.0b013e318207ec3c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Copland IB, Kavanagh BP, Engelberts D, McKerlie C, Belik J, Post M. Early changes in lung gene expression due to high tidal volume. Am J Respir Crit Care Med. 2003;3(9):1051–1059. doi: 10.1164/rccm.200208-964OC. Epub 2003 Jun 19. [DOI] [PubMed] [Google Scholar]
- Grigoryev DN, Finigan JH, Hassoun P, Garcia JG. Science review: searching for gene candidates in acute lung injury. Crit Care. 2004;3(6):440–447. doi: 10.1186/cc2901. Epub 2004 Jun 30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin TR. Direct lung injury by bacteria: clarifying the tools of the trade. Crit Care Med. 2004;3(11):2360–2361. doi: 10.1097/01.ccm.0000146135.19642.72. [DOI] [PubMed] [Google Scholar]
- Kojicic M, Li G, Hanson AC, Lee KM, Thakur L, Vedre J, Ahmed A, Baddour LM, Ryu JH, Gajic O. Risk factors for the development of acute lung injury in patients with infectious pneumonia. Crit Care. 2012;3(2):R46. doi: 10.1186/cc11247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tremblay L, Valenza F, Ribeiro SP, Li J, Slutsky AS. Injurious ventilatory strategies increase cytokines and c-fos m-RNA expression in an isolated rat lung model. J Clin Invest. 1997;3:944–952. doi: 10.1172/JCI119259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, Takagaki TY, Carvalho CR. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;3:347–354. doi: 10.1056/NEJM199802053380602. [DOI] [PubMed] [Google Scholar]
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med. 2000;3:1301–1308. doi: 10.1056/NEJM200005043421801. [DOI] [PubMed] [Google Scholar]
- Martin-Loeches I, de Haro C, Dellinger RP, Ferrer R, Phillips GS, Levy MM, Artigas A. Effectiveness of inspiratory pressure-limited approach to mechanical ventilation in septic patients. Eur Respir J. 2012. Apr 20. [Epub ahead of print] [DOI] [PubMed]
- Gajic O, Dara SI, Mendez JL, Adesanya AO, Festic E, Caples SM, Rana R, St Sauver JL, Lymp JF, Afessa B, Hubmayr RD. Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation. Crit Care Med. 2004;3:1817–1824. doi: 10.1097/01.CCM.0000133019.52531.30. [DOI] [PubMed] [Google Scholar]
- Determann RM, Royakkers A, Wolthuis EK, Vlaar AP, Choi G, Paulus F, Hofstra JJ, de Graaff MJ, Korevaar JC, Schultz MJ. Ventilation with lower tidal volumes as compared with conventional tidal volumes for patients without acute lung injury: a preventive randomized controlled trial. Crit Care. 2010;3:R1. doi: 10.1186/cc8230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hemmes SN, Neto AS, Schultz MJ. Intraoperative ventilatory strategies to prevent postoperative pulmonary complications: a meta-analysis. Curr Opin Anaesthesiol. 2013;3(2):126–133. doi: 10.1097/ACO.0b013e32835e1242. [DOI] [PubMed] [Google Scholar]
- Serpa Neto A, Cardoso SO, Manetta JA, Pereira VG, Espósito DC, Pasqualucci Mde O, Damasceno MC, Schultz MJ. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA. 2012;3(16):1651–1659. doi: 10.1001/jama.2012.13730. [DOI] [PubMed] [Google Scholar]
- Schultz MJ, Haitsma JJ, Slutsky AS, Gajic O. What tidal volumes should be used in patients without acute lung injury? Anesthesiology. 2007;3:1226–1231. doi: 10.1097/01.anes.0000267607.25011.e8. [DOI] [PubMed] [Google Scholar]
- Schmidt GB, O'Neill WW, Kotb K, Hwang KK, Bennett EJ, Bombeck CT. Continuous positive airway pressure in the prophylaxis of the adult respiratory distress syndrome. Surg Gynecol Obstet. 1976;3(4):613–618. [PubMed] [Google Scholar]
- Weigelt JA, Mitchell RA, Snyder WH 3rd. Early positive end-expiratory pressure in the adult respiratory distress syndrome. Arch Surg. 1979;3(4):497–501. doi: 10.1001/archsurg.1979.01370280151024. [DOI] [PubMed] [Google Scholar]
- Dreyfuss D, Soler P, Basset G, Saumon G. High inflation pressure pulmonary edema. Respective effects of high airway pressure, high tidal volume, and positive end-expiratory pressure. Am Rev Respir Dis. 1988;3(5):1159–1164. doi: 10.1164/ajrccm/137.5.1159. [DOI] [PubMed] [Google Scholar]
- Ruiz-Bailén M, Fernández-Mondéjar E, Hurtado-Ruiz B, Colmenero-Ruiz M, Rivera-Fernández R, Guerrero-López F, Vázquez-Mata G. Immediate application of positive-end expiratory pressure is more effective than delayed positive-end expiratory pressure to reduce extravascular lung water. Crit Care Med. 1999;3(2):380–384. doi: 10.1097/00003246-199902000-00046. [DOI] [PubMed] [Google Scholar]
- Pepe PE, Hudson LD, Carrico CJ. Early application of positive end-expiratory pressure in patients at risk for the adult respiratory-distress syndrome. N Engl J Med. 1984;3(5):281–286. doi: 10.1056/NEJM198408023110502. [DOI] [PubMed] [Google Scholar]
- Manzano F, Fernández-Mondéjar E, Colmenero M, Poyatos ME, Rivera R, Machado J, Catalán I, Artigas A. Positive-end expiratory pressure reduces incidence of ventilator-associated pneumonia in nonhypoxemic patients. Crit Care Med. 2008;3(8):2225–2231. doi: 10.1097/CCM.0b013e31817b8a92. [DOI] [PubMed] [Google Scholar]
- Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF Jr, Hite RD, Harabin AL. National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;3(24):2564–2575. doi: 10.1056/NEJMoa062200. [DOI] [PubMed] [Google Scholar]
- Simmons RS, Berdine GG, Seidenfeld JJ, Prihoda TJ, Harris GD, Smith JD, Gilbert TJ, Mota E, Johanson WG. Fluid balance and the adult respiratory distress syndrome. Am Rev Respir Dis. 1987;3:924–929. doi: 10.1164/arrd.1987.135.4.924. [DOI] [PubMed] [Google Scholar]
- Sakr Y, Vincent JL, Reinhart K, Groeneveld J, Michalopoulos A, Sprung CL, Artigas A, Ranieri VM. High tidal volume and positive fluid balance are associated with worse outcome in acute lung injury. Chest. 2005;3:3098–3108. doi: 10.1378/chest.128.5.3098. [DOI] [PubMed] [Google Scholar]
- Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AF Jr, Hite RD, Harabin AL. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;3(24):2564–2575. doi: 10.1056/NEJMoa062200. Epub 2006 May 21. [DOI] [PubMed] [Google Scholar]
- Murphy CV, Schramm GE, Doherty JA, Reichley RM, Gajic O, Afessa B, Micek ST, Kollef MH. The importance of fluid management in acute lung injury secondary to septic shock. Chest. 2009;3(1):102–109. doi: 10.1378/chest.08-2706. Epub 2009 Mar 24. [DOI] [PubMed] [Google Scholar]
- Iscimen R, Cartin-Ceba R, Yilmaz M, Khan H, Hubmayr RD, Afessa B, Gajic O. Risk factors for the development of acute lung injury in patients with septic shock: an observational cohort study. Crit Care Med. 2008;3:1518–1522. doi: 10.1097/CCM.0b013e31816fc2c0. [DOI] [PubMed] [Google Scholar]
- Ferrer R, Artigas A, Levy MM, Blanco J, González-Díaz G, Garnacho-Montero J, Ibáñez J, Palencia E, Quintana M, de la Torre-Prados MV. Improvement in process of care and outcome after a multicenter severe sepsis educational program in Spain. JAMA. 2008;3:2294–2303. doi: 10.1001/jama.299.19.2294. [DOI] [PubMed] [Google Scholar]
- Kumar A, Ellis P, Arabi Y, Roberts D, Light B, Parrillo JE, Dodek P, Wood G, Kumar A, Simon D, Peters C, Ahsan M, Chateau D. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest. 2009;3:1237–1248. doi: 10.1378/chest.09-0087. [DOI] [PubMed] [Google Scholar]
- Zilberberg MD, Carter C, Lefebvre P, Raut M, Vekeman F, Duh MS, Shorr AF. Red blood cell transfusions and the risk of acute respiratory distress syndrome among the critically ill: a cohort study. Crit Care. 2007;3:R63. doi: 10.1186/cc5934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan H, Belsher J, Yilmaz M, Afessa B, Winters JL, Moore SB, Hubmayr RD, Gajic O. Fresh-frozen plasma and platelet transfusions are associated with development of acute lung injury in critically ill medical patients. Chest. 2007;3:1308–1314. doi: 10.1378/chest.06-3048. [DOI] [PubMed] [Google Scholar]
- Jia X, Malhotra A, Saeed M, Mark RG, Talmor D. Risk factors for ARDS in patients receiving mechanical ventilation for > 48 h. Chest. 2008;3:853–861. doi: 10.1378/chest.07-1121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toy P, Popovsky MA, Abraham E, Ambruso DR, Holness LG, Kopko PM, McFarland JG, Nathens AB, Silliman CC, Stroncek D. National Heart, Lung and Blood Institute Working Group on TRALI. Transfusion-related acute lung injury: definition and review. Crit Care Med. 2005;3(4):721–726. doi: 10.1097/01.CCM.0000159849.94750.51. [DOI] [PubMed] [Google Scholar]
- Popovsky MA, Moore SB. Diagnostic and pathogenetic considerations in transfusion-related acute lung injury. Transfusion. 1985;3(6):573–577. doi: 10.1046/j.1537-2995.1985.25686071434.x. [DOI] [PubMed] [Google Scholar]
- Silliman CC, Thurman GW, Ambruso DR. Stored blood components contain agents that prime the neutrophil NADPH oxidase through the platelet-activating-factor receptor. Vox Sang. 1992;3(2):133–136. doi: 10.1111/j.1423-0410.1992.tb02500.x. [DOI] [PubMed] [Google Scholar]
- Densmore TL, Goodnough LT, Ali S, Dynis M, Chaplin H. Prevalence of HLA sensitization in female apheresis donors. Transfusion. 1999;3(1):103–106. doi: 10.1046/j.1537-2995.1999.39199116901.x. [DOI] [PubMed] [Google Scholar]
- Gajic O, Yilmaz M, Iscimen R, Kor DJ, Winters JL, Moore SB, Afessa B. Transfusion from male-only versus female donors in critically ill recipients of high plasma volume components. Crit Care Med. 2007;3(7):1645–1648. doi: 10.1097/01.CCM.0000269036.16398.0D. [DOI] [PubMed] [Google Scholar]
- Chapman CE, Stainsby D, Jones H, Love E, Massey E, Win N, Navarrete C, Lucas G, Soni N, Morgan C, Choo L, Cohen H, Williamson LM. Serious Hazards of Transfusion Steering Group. Ten years of hemovigilance reports of transfusion-related acute lung injury in the United Kingdom and the impact of preferential use of male donor plasma. Transfusion. 2009;3(3):440–452. doi: 10.1111/j.1537-2995.2008.01948.x. [DOI] [PubMed] [Google Scholar]
- Wright SE, Snowden CP, Athey SC, Leaver AA, Clarkson JM, Chapman CE, Roberts DR, Wallis JP. Acute lung injury after ruptured abdominal aortic aneurysm repair: the effect of excluding donations from females from the production of fresh frozen plasma. Crit Care Med. 2008;3(6):1796–1802. doi: 10.1097/CCM.0b013e3181743c6e. [DOI] [PubMed] [Google Scholar]
- Looney MR. Acute lung injury after blood product transfusion: are the times changing? Crit Care Med. 2008;3(6):1968–1970. doi: 10.1097/CCM.0b013e318176a8b2. [DOI] [PubMed] [Google Scholar]
- Vlaar AP, Binnekade JM, Schultz MJ, Juffermans NP, Koopman MM. Preventing TRALI: ladies first, what follows? Crit Care Med. 2008;3(12):3283–3284. doi: 10.1097/CCM.0b013e31818f2f37. [DOI] [PubMed] [Google Scholar]
- Yazer MH, Podlosky L, Clarke G, Nahirniak SM. The effect of prestorage WBC reduction on the rates of febrile nonhemolytic transfusion reactions to platelet concentrates and RBC. Transfusion. 2004;3(1):10–15. doi: 10.1046/j.0041-1132.2003.00518.x. [DOI] [PubMed] [Google Scholar]
- Vlaar AP, Schultz MJ, Juffermans NP. Transfusion-related acute lung injury: a change of perspective. Neth J Med. 2009;3(10):320–326. [PubMed] [Google Scholar]
- Slofstra SH, Groot AP, Maris NA, Reitsma PH, Cate HT, Spek CA. Inhalation of activated protein C inhibits endotoxin-induced pulmonary inflammation in mice independent of neutrophil recruitment. Br J Pharmacol. 2006;3(6):740–746. doi: 10.1038/sj.bjp.0706915. Epub 2006 Oct 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maniatis NA, Letsiou E, Orfanos SE, Kardara M, Dimopoulou I, Nakos G, Lekka ME, Roussos C, Armaganidis A, Kotanidou A. Inhaled activated protein C protects mice from ventilator-induced lung injury. Crit Care. 2010;3(2):R70. doi: 10.1186/cc8976. Epub 2010 Apr 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotton DN, Ma BY, Cardoso WV, Sanderson EA, Summer RS, Williams MC, Fine A. Bone marrow-derived cells as progenitors of lung alveolar epithelium. Development. 2001;3(24):5181–5188. doi: 10.1242/dev.128.24.5181. [DOI] [PubMed] [Google Scholar]
- Chimenti L, Luque T, Bonsignore MR, Ramírez J, Navajas D, Farré R. Pre-treatment with mesenchymal stem cells reduces ventilator-induced lung injury. Eur Respir J. 2012;3(4):939–948. doi: 10.1183/09031936.00153211. Epub 2012 Mar 22. [DOI] [PubMed] [Google Scholar]
- Levitt JE, Matthay MA. Clinical review: Early treatment of acute lung injury - paradigm shift toward prevention and treatment prior to respiratory failure. Crit Care. 2012;3(3):223. doi: 10.1186/cc11144. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]