

Abstract
Lipoprotein (a) is a risk factor for adult cardiovascular events, in which the apolipoprotein (a) component is thought to promote atherogenesis and impair fibrinolysis. We investigated whether elevated plasma lipoprotein (a) concentration and small predominant apolipoprotein (a) isoform size (number of kringle-4 domains) are risk factors for childhood arterial ischemic stroke and correlate with plasma fibrinolytic function. Patients who had had an arterial ischemic stroke in childhood (29 days - <21 years at onset; n=43) and healthy controls (n=127) were recruited for plasma sampling and laboratory determinations. Cases were followed for recurrence in a prospective cohort study. The median lipoprotein (a) concentration did not differ between groups [cases: median 18.0 nmol/L (7.5 mg/dL) and observed range 0.9–259 nmol/L (0.38–108.0 mg/dL), controls: 20.4 nmol/L (8.5 mg/dL) and 0.2–282 nmol/L (0.08–117.5 mg/dL); P=0.62]. While odds of incident stroke were not significantly increased, risks of recurrent arterial ischemic stroke were each more than ten-times increased for lipoprotein(a) >90th percentile of race-specific reference values and apolipoprotein (a) <10th percentiles [odds ratio=14.0 (95% confidence interval: 1.0–184), P=0.05 and odds ratio=12.8 (1.61–101), P=0.02]. Statistically significant but weak correlations were observed between euglobulin lysis time and both lipoprotein (a) level (r=0.18, P=0.03) and apolipoprotein (a) size (r= −0.26, P=0.002). In conclusion, elevated lipoprotein (a) and small apolipoprotein (a) potently increase the risk of recurrent arterial ischemic stroke in children, with a mechanism only partially attributable to impaired fibrinolysis. Collaborative studies are warranted to investigate these findings further and, more broadly, to establish key risk factors for incident and recurrent arterial ischemic stroke in children.
Introduction
Lipoprotein (a) [Lp(a)] is a plasma lipoprotein comprising phospholipid, cholesterol, apo B-100, and apolipoprotein (a) [apo(a)]. The apo(a) component of Lp(a) has 80% homology with plasminogen by virtue of shared repetitive kringle-4 domains.1 Lp(a) is believed to be prothrombotic through two main mechanisms: (i) atherogenesis, via a vascular endothelial inflammatory response to oxidized Lp(a) and plaque deposition by foam cells;2,3 and (ii) hypofibrinolysis, via inhibition of plasminogen activation.4 The apo(a) component is thought to play a role in the pathogenesis of cardiovascular events; recently, a meta-analysis of 40 published studies evaluating the relationship between predominant apo(a) isoform size (number of kringle-4 domains) and coronary heart disease or ischemic stroke in adults revealed that patients having a predominant apo(a) isoform of fewer than 22 kringle-4 domains are at an approximately 2-fold increased risk of these conditions.5
Arterial ischemic stroke (AIS) is a rare disease outside of the peri-natal/neonatal period, with an incidence of approximately 5 cases per 100,000 individuals per year in childhood.6–8 At the same time, it is a serious disorder with deficits evident in 70% of children, both acutely9 and in long-term follow-up.10–12 In addition, recurrence is common, with a cumulative probability of recurrent stroke of 6–15% at approximately 1 year.6,13 Numerous causal and contributing factors have been identified in childhood-onset AIS, including thrombophilia (i.e., hypercoagulability), acute infection, congenital heart disease, cardiac catheterization, cerebral/cervical arterial dissection, cerebral angiitis, and other/idiopathic cerebral arteri-opathies.14
Elevated Lp(a) levels have also been implicated as a putative risk factor for childhood-onset AIS. Prospective studies of the risk of ischemic stroke associated with elevated Lp(a) in adults have produced conflicting results, suggesting overall a very mild increase in ischemic stroke risk when Lpa(a) levels were >99th percentile, particularly after adjustment for other common risk factors for stroke.15 In children, a seminal multi-center case-control study in Germany16 demonstrated significantly increased odds of incident idiopathic AIS (i.e., AIS occurring in the absence of known clinical risk factors) in association with Lp(a) >30 mg/dL [odds ratio (OR)=7.2; 95% confident interval (CI)=3.8–13.8]. More recently, in a study in the USA,17 the prevalence of elevated Lp(a) among 59 children with porencephaly or a history of perinatal or childhood onset-AIS was significantly increased compared to that of historical controls who had consisted of healthy German children (20% versus 5.4%); however, concomitant USA-based controls were lacking. Interestingly, in a French study of mother-infant diads of neonatal AIS, elevated maternal Lp(a) was not only implicated in perinatal AIS but also correlated with low birth weight in these infants, leading to a hypothesis that elevated Lp(a) may mediate placental insufficiency.18 With regard to recurrent AIS in childhood, a prospective multicenter cohort study in Germany13 demonstrated that Lp(a) >30 mg/dL was an independent risk factor for recurrent AIS (OR: 2.8; 95% CI: 1.1–7.5).
In consideration of the lack of well-controlled studies of Lp(a) in childhood-onset AIS outside of Germany, and given also that apo(a) size has received little attention in pediatric AIS, we sought to determine the odds of incident and recurrent childhood-onset AIS associated with elevated plasma Lp(a) and small apo(a) isoform size in a pediatric population in the USA. Furthermore, in order to enhance mechanistic understanding of pathophysiology, we investigated the relationship of Lp(a) levels and apo(a) isoform size with overall fibrinolytic capacity in plasma, using two global assays of fibrinolysis.
Design and Methods
Subjects
Children with a history of radiologically-confirmed AIS with symptomatic onset at age 29 days to <21 years (case group, n=43) and healthy children (unmatched, contemporaneous control group, n=127) were consecutively recruited in an Institutional Review Board-approved case-control study at the Children’s Hospital Colorado and the Mountain States Regional Hemophilia and Thrombosis Center at the University of Colorado (Aurora, CO, USA) from 2004 to 2010, with blood sampling for laboratory determinations as described below. Children with AIS were followed in the multidisciplinary Stroke Clinic at the Children’s Hospital Colorado and additionally enrolled from 2006 to 2011 in an Institutional Review Board-approved local prospective cohort study designed to capture and analyze clinically-derived, systematically-assessed data on AIS risk factors, treatments, and long-term outcomes. For patients diagnosed with acute AIS prior to February 28, 2006 (n=21), data were retrospectively collected prior to this date and prospectively ascertained from this date forward. Controls were enrolled from a well-child ambulatory setting as well as a pre-operative environment for outpatient elective surgery, and were systematically screened for exclusion of acute illness, concomitant medication, and personal or family history of early-onset (prior to age 55 years) ischemic stroke, myocardial infarction, or venous thromboembolism.
Diagnostic criteria for acute pediatric AIS consisted of sudden onset of a focal neurological deficit with objective confirmation of a corresponding arterial-distribution ischemia/infarct by computed tomography or magnetic resonance imaging of the brain. Etiological findings obtained through the history, examinations, and diagnostic investigations (vascular imaging of the head and neck, echocardiography, and thrombophilia testing) were classified according to current consensus criteria for childhood-onset AIS.19 Diagnostic criteria for recurrent AIS were identical to those for incident AIS (above); however, events that occurred within 7 days of the initial AIS were not considered as recurrent AIS.
Plasma collection, processing, and storage methods
Blood samples were obtained at rest by peripheral venipuncture into EDTA [for Lp(a) and apo(a) isoform determinations] or sodium citrate (for fibrinolysis assays). Whole blood was processed to plasma by a single centrifugation at 4ºC and 2500 x g for 15 minutes [for Lp(a) and apo(a)] and by double-centrifugation at the same settings (for platelet-poor plasma, used in fibrinolysis assays). Plasma was stored in aliquots of 200–500 μL in polystyrene long-term freezer storage tubes at −70°C.
Lipoprotein (a), apolipoprotein (a) isoform, and global fibrinolytic laboratory assay method
Lp(a) concentration was measured using an enzyme-linked immmunosorbent assay (ELISA) method developed in Dr. Marcovina’s laboratory, based on the detection of a monoclonal antibody recognizing an epitope present in the kringle-4 type 9 domain of apo(a). The assay has been extensively evaluated for its ability to measure Lp(a) levels accurately without being influenced by apo(a) size heterogeneity.20 Lp(a) values are traceable to the World Health Organization/International Federation of Clinical Chemistry and Laboratory Medicine Reference Material SRM-2B and are expressed in nmol/L. Apo(a) isoforms were determined by a high sensitive agarose gel electrophoresis method21 and the isoforms are designated by their respective number of kringle-4 domains. Lp(a) results are expressed as corresponding race-specific percentiles, based upon reference values established in the CARDIA study cohort.21 Apo(a) isoforms are reported as corresponding race-specific percentiles, based upon the isoform distribution obtained in CARDIA.21
Global fibrinolysis assays included the Clot Formation and Lysis (CloFAL) assay and the automated Euglobulin Clot Lysis Assay (ECLA). The CloFAL assay monitored kinetic light absorbance measurements in plasma following the addition of a reagent comprising trace lipidated tissue factor for coagulation activation and tissue plasminogen activator for acceleration of clot lysis, resulting in a clot formation and lysis waveform, as previously described.22–24 A recently-updated fibrinolytic index (FI2) was employed.25 ECLA was performed by an automated spectrophotometric technique as previously described, and the results are expressed as the euglobulin lysis time (ELT).26
Statistical methods
Statistical methods in the descriptive analyses involved calculation of median values with observed ranges. These distributions were compared between groups using the Mann-Whitney U test. Odds ratios were calculated for the association between elevated values and stroke risk, using both the 75th and 90th percentiles of previously-established normal values21 as cutoffs for elevated Lp(a), and the 25th and 10th percentiles as cutoffs for apo(a) isoform size. Ninety-five percent confidence intervals were determined using the Wald method. Correlation testing was performed using Spearman’s method. The value of alpha was set at 0.05 for inferential statistics. All analyses were performed using SAS version 9.1 statistical software (SAS Institute, Cary, NC, USA).
Results
Analyses of risks of incident (case-control) and recurrent (cohort) arterial ischemic strok
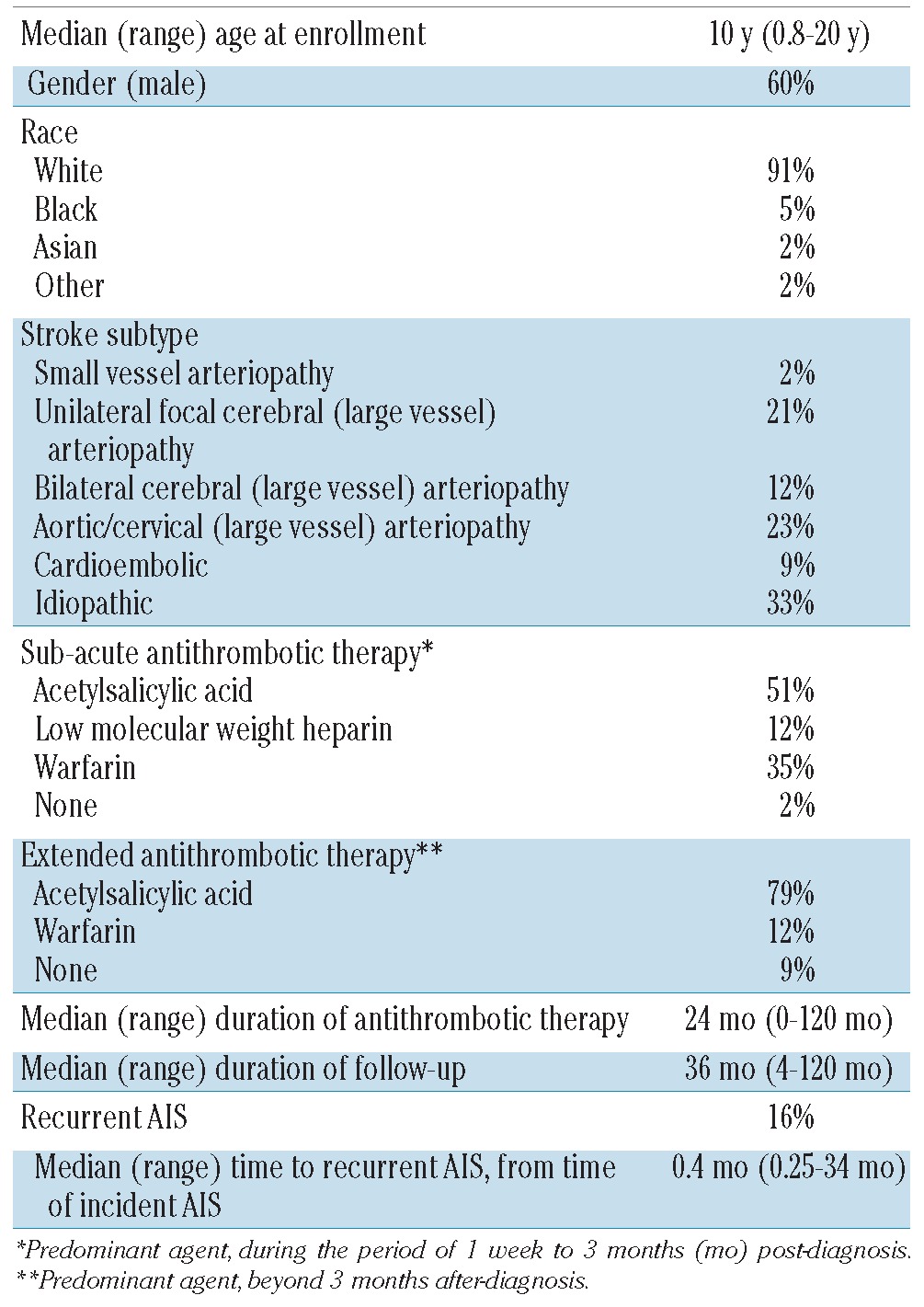
The study population consisted of 43 childhood-onset AIS cases and 127 unmatched, consecutive, contemporaneous, healthy pediatric controls. Stroke subtypes, treatments, and outcomes in the case group are described for the childhood-onset AIS case group in Table 1. The risk of recurrent AIS was 16%, with a median time to recurrence of 4 months after the incident AIS. Antithrombotic treatment histories for cases of incident AIS among patients who developed recurrent AIS were consistent with those of the overall cohort (see Table 1), and comprised the following: sub-acute, acetylsalicylic acid 57% (4/7) and anticoagulation 43% (3/7); extended, acetylsalicylic acid 71% (5/7), anticoagulation 14% (1/7), and none 14% (1/7).
Table 1.
Stroke subtypes, antithrombotic treatments, and outcomes in the childhood-onset AIS case group (n=43).
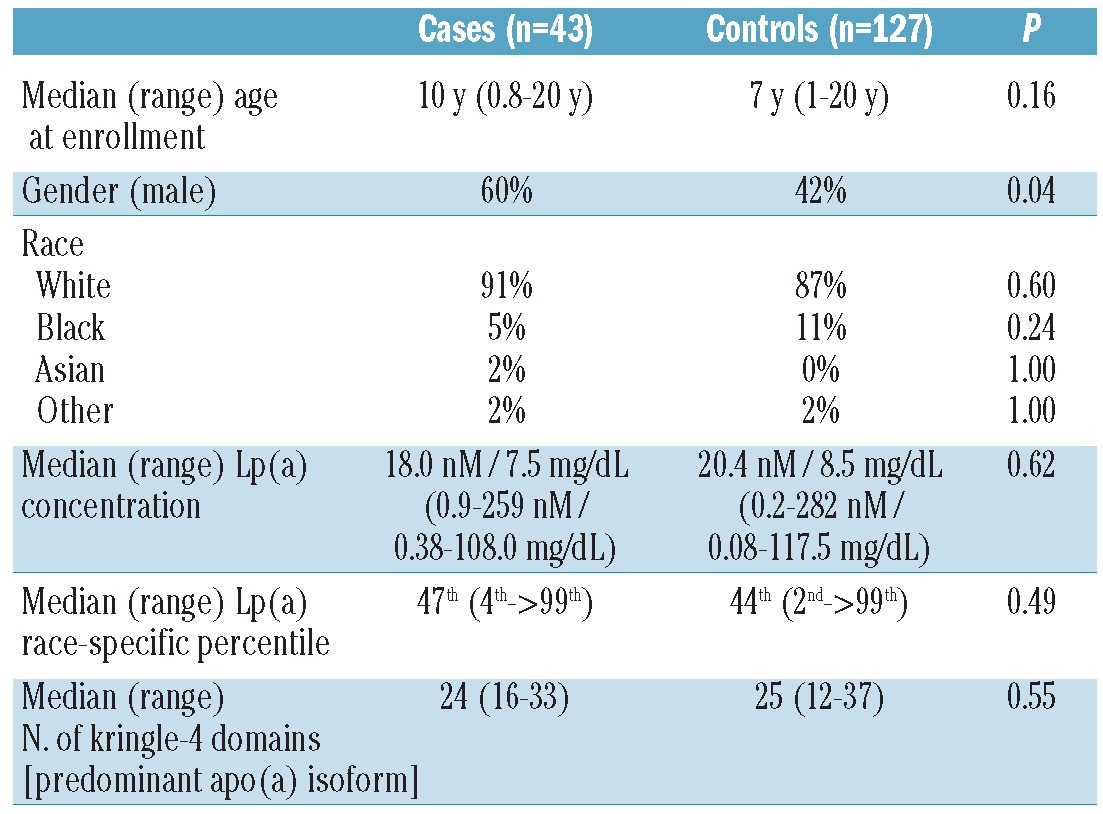
Demographic data and Lp(a) results are summarized in Table 2, by study group. The study groups were similar with respect to demographic characteristics of age at enrollment and race; males were more frequent in the case group (60% versus 42%; P=0.04), consistent with prior publications of a male predilection in pediatric AIS. The median Lp(a) concentration did not differ significantly between cases and controls [median 18.0 nmol/L (7.5 mg/dL) versus 20.4 nmol/L (8.5 mg/dL); P=0.62]. Similarly, with regard to predominant apo(a) isoform size, there was no significant difference in median number of kringle-4 domains between cases and controls [24 domains (16–33 domains) versus 25 domains (12–37 domains); P=0.55].
Table 2.
Demographic data and Lp(a) results, by study group.
The prevalence of elevated Lp(a) (>75th and >90th race-specific percentiles of established reference values) was 16.3% and 7.0%, respectively, among cases, and 15% and 5.5% among controls. The prevalence of small apo(a) isoform size (<25th and <10th race-specific percentiles) was 27.9% and 18.6% among cases, and 25.2% and 14.2% among controls. The odds of incident stroke for elevated Lp(a) levels (>75th and >90th percentiles of previously-established normative values) were 1.50 (95% confidence interval: 0.62–3.63; P=0.36) and 1.29 (0.32–5.21; P=0.49), and those for small apo(a) isoform size (<25th and <10th percentiles) were 1.59 (0.76–3.35; P=0.22) and 0.80 (0.28–2.29; P=0.67). The odds of recurrent AIS for Lp(a) >75th and >90th percentiles were 3.75 (0.66–21.3; P=0.15) and 14.0 (1.0–184; P=0.05), whereas as those for apo(a) isoform <25th and <10th percentiles were 1.50 (0.29–7.81; P=0.68) and 12.8 (1.61–101; P=0.02). Because race-specific percentiles were calculated and reported for both Lp(a) and apo(a), adjustment of the analyses (odds ratios) for race was not pertinent. Additionally, since analyses of incident and recurrent stroke risk employed Lp(a) percentiles referenced to the pediatric normative values established in the CARDIA study,21 and because we found only a weak correlation between age and Lp(a) concentration (r=0.23, P=0.04) and no correlation between age and apo(a) isoform size (r= −0.04, P=0.74), age-adjustment of the odds ratios was not undertaken. Lastly, given that gender was not a significant risk factor for incident or recurrent AIS in univariate logistic regression, odds ratios were not adjusted for gender.
When controls were restricted to those having negative second-degree family histories for early-onset AIS, myocardial infarction, and venous thromboembolism, Lp(a) and apo(a) associated stroke risks were not significantly changed (data not shown). When cases were restricted to idiopathic AIS using CASCADE criteria, odds of incident stroke for Lp(a) >75th and >90th percentiles were 2.53 (0.71–9.04; P=0.22) and 3.43 (95% CI: 0.63–18.7; P=0.17), whereas those for apo(a) isoform <25th and <10th percentiles were 3.46 (1.08–11.1; P=0.047) and 1.82 (0.46–7.24; P=0.25). Odds for recurrent stroke among patients with incident cryptogenic AIS were indeterminate due to low frequency.
Investigations of a mechanistic hypothesis concerning fibrinolysis
To explore mechanisms by which Lp(a) and apo(a) modulate recurrent AIS risk in children, the relationship between these biomarkers and plasma fibrinolytic function was investigated, using two distinct methodologies for overall fibrinolytic capacity: the CloFAL assay and ECLA. These analyses revealed no statistically significant correlation between either Lp(a) levels or apo(a) isoform size and FI2 in the CloFAL assay [r= −0.15 (P=0.11) and r= −0.06 (P=0.52)]. However, there were statistically significant (albeit weak) correlations of Lp(a) levels and predominant apo(a) isoform size (number of kringle-4 repeats) with ELT by ECLA [r=0.18 (P=0.03) and r= −0.26 (P=0.002), respectively]. In addition, as reflected in the scatterplots of Figure 1, ELT was significantly longer (suggesting relative hypofibrinolysis) among children with predominant apo(a) isoforms less than the 25th percentile of normative values, when compared to those greater than or equal to the 25th percentile [median, 279 min (observed range, 120–504 min) versus 187 min (90–482 min), respectively; P=0.006].
Figure 1.
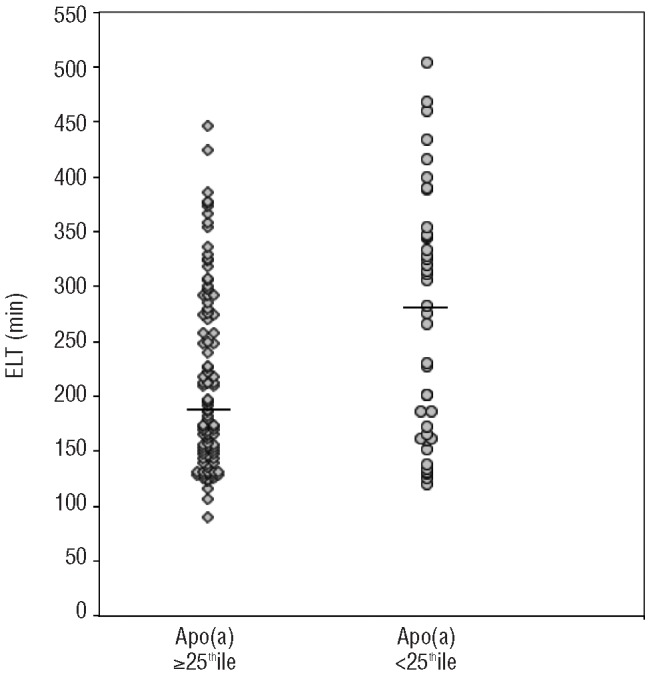
Scatterplot of plasma fibrinolytic function, as measured by euglobulin lysis time (ELT) in the automated euglobulin clot lysis assay, for children with predominant apo(a) isoform size less than versus greater than or equal to, the 25th percentile of normal values i.e., small vs. normal apo(a). ELT was significantly longer (suggesting relative hypofibrinolysis) among children with small apo(a).
Discussion
The present work provides USA data in support of the importance of elevated Lp(a) as a mild prognostic factor for recurrent AIS in childhood, as previously demonstrated in a German multicenter cohort.13 Yet, our study does not substantiate prior German case-control findings of an increase in risk of incident childhood-onset AIS in association with elevated Lp(a),16 nor those of a meta-analysis by Kenet and colleagues (comprising these studies and three others from Germany),27 which identified elevated Lp(a) as a risk factor for incident pediatric AIS (i.e., childhood-onset and/or perinatal/neonatal AIS). In addition, small apo(a) size was not a significant risk factor for incident childhood-onset AIS in the current USA study, despite recent meta-analytic findings from adult studies that small apo(a) size confers a 2-fold increase in the risks of coronary heart disease and ischemic stroke.5 However, small apo(a) was shown in the current work to be a significant risk factor for recurrent childhood-onset AIS, conferring a nearly 13-fold increase in odds. Lastly, in investigations of overall fibrinolytic capacity in plasma, modest correlations were identified between ELT by ECLA and both Lp(a) levels and apo(a) isoform size, and ELT was increased (suggesting relative hyofibrinolysis) among children with apo(a) <25th percentile.
This work is important in its unique demonstration of the odds of incident and recurrent childhood-onset AIS associated with elevated plasma Lp(a) in a USA pediatric population, and its novel investigation of the same with regard to apo(a) isoform size. If substantiated in larger collaborative cohorts, these findings would suggest that Lp(a) measurement is more important for secondary prevention in childhood-onset AIS than for primary prevention, and that determination of apo(a) size does have key implications for clinical management in children who have a history of AIS. The present study also provides unique data on the relationship of Lp(a) levels and apo(a) isoform size with overall fibrinolytic capacity in plasma, as measured by two global assays of fibrinolysis, CloFAL and ECLA. These data suggest a mechanistic basis for the pathogenesis of small apo(a) isoforms—i.e., impairment of fibrinolysis. At the same, the fact that correlations of apo(a) with ELT were statistically significant but not strong may be explained by recent observations that overall plasma fibrinolytic capacity, when measured by the CloFAL assay, is strongly driven by functional fibrinogen levels.25
A few factors may explain the difference between the present findings for Lp(a) in childhood AIS and prior work by Nowak-Göttl and colleagues.16 Foremost among these is the fact that childhood-onset AIS cases in the German case-control study were idiopathic in nature, whereas those in this study included all potential CASCADE subtypes; our secondary analysis restricting the cases group to idiopathic AIS is more comparable to that of Nowak-Göttl’s study, but was limited by a small sample size. Secondly, given that Lp(a) is highly genetically determined, and that both studies utilized non-acute Lp(a) testing to mitigate the acute phase response, it is possible that genetic heterogeneity between the German and USA study populations explains the different findings. It should be noted that the prevalence of elevated Lp(a) (when defined as >75th percentile of race-specific norms in the current study, and as >30 mg/dL in the study by Nowak-Göttl et al.) differed between control groups in the two studies. Lastly, the Lp(a) laboratory methodologies differed between the two studies; the ELISA method was selected for the present study because it has been validated to measure Lp(a) concentration accurately, independently of apo(a) size polymorphism.15
Strengths of the present study include: uniform application of rigorous eligibility criteria to meet the definitions of childhood-onset AIS cases and healthy controls; use of gold-standard Lp(a) assay methodology in a national reference laboratory for the same; analysis of apo(a) size; and evaluation of overall plasma fibrinolytic capacities in two global assays. At the same time, several potential limitations are worthy of note. First, we did not employ time-to-event analyses in evaluating the associations of Lp(a) and apo(a) with recurrent AIS. However, given the left-skew in the time of re-occurrence (i.e. median of 0.4 months with a range of 0.25 months to 34 months), recurrences were generally early in the course of the follow-up, such that the presence/absence of recurrent stroke is more meaningful than the time to re-occurrence per se; hence, the results of a Cox regression analysis would be very unlikely to differ from those reported here using logistic regression. Furthermore, because our a priori choice of logistic regression methodology was based on the accurate assumption that most re-occurrences would be clustered early in the course of follow-up, we decided not to perform additional post-hoc Cox regression analyses. A second potential limitation is the study’s single-center scope and sample size which, although relatively small (n=270, in a 1:2 ratio of childhood-onset AIS cases to unmatched, consecutive, contemporaneous, healthy pediatric controls), is nevertheless the largest pediatric study investigating the relationship between Lp(a) and AIS in a USA population. Still, given the small number of idiopathic AIS cases, we cannot exclude the possibility that elevated Lp(a) is a risk factor for incident cryptogenic childhood-onset AIS, and given the small number of recurrent AIS events, the estimates of recurrence risk associated with Lp(a) and apo(a) should be evaluated in larger follow-up studies. Thirdly, the question of whether Lp(a) is of increased importance for AIS risk in USA children in the setting of additional underlying thrombophilia traits is not addressed by this study. Larger, multicenter studies will be required to definitively address these issues. Notwithstanding these limitations, this study adds to the existing evidence that recurrence risk is increased among patients with elevated Lp(a). Based on our findings, it appears generally that Lp(a) measurement is more important for secondary prevention than for primary prevention of this disease in children, and that determination of apo(a) size has important potential implications for clinical management in children who have a history of AIS, with regard to further risk-stratification. A potential implication of the study is that children with a prior episode of AIS in whom Lp(a) is >90th percentile or apo(a) predominant isoform size is <10th percentile of race-specific reference values could be considered for extended-duration of aspirin therapy (the current mainstay of long-term secondary AIS prevention in most children with incident AIS), particularly if such an approach is supported by safety and efficacy findings from future clinical trials. Collaborative studies are warranted to further investigate these findings, and more broadly to establish key risk factors for incident and recurrent AIS in children.
Acknowledgments
The authors thank the patients and their families for generously participating in this research.
Footnotes
Funding
National Institutes of Health, National Heart Lung and Blood Institute, 1K23HL084055 (NAG) and 1K23HL096895 (TJB), Centers for Disease Control and Prevention UR6/CCU820552 (MJM-J)
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.McLean JW, Tomlinson JE, Kuang W-J, Eaton DL, Chen EY, Fless GM, et al. cDNA sequence of human apolipoprotein(a) is homologous to plasminogen. Nature. 1987; 330:132–7 [DOI] [PubMed] [Google Scholar]
- 2.Keesler GA, Gabel BR, Devlin CM, Koschinsky ML, Tabas I. The binding activity of the macrophage lipoprotein(a)/apolipoprotein(a) receptor is induced by cholesterol via a post-translational mechanism and recognizes distinct kringle domains on apolipoprotein(a). J Biol Chem. 1996; 271:32096–104 [DOI] [PubMed] [Google Scholar]
- 3.Edelstein C, Pfaffinger D, Hinman J, Miller E, Lipkind G, Tsimikas S, et al. Lysine-phos-phatidylcholine adducts in kringle V impart unique immunological and potential pro-inflammatory properties to human apolipoprotein(a). J Biol Chem. 2003;278 (52):52841–7 [DOI] [PubMed] [Google Scholar]
- 4.Koschinsky ML, Marcovina SM. Structure-function relationships in apolipoprotein(a): insights into lipoprotein(a) assembly and pathogenicity. Curr Opin Lipidol. 2004; 15(2):167–74 [DOI] [PubMed] [Google Scholar]
- 5.Erqou S, Thompson A, Di Angelantonio E, Saleheen D, Kaptoge S, Marcovina S, Danesh J. Apolipoprotein(a) isoforms and the risk of vascular disease: systematic review of 40 studies involving 58,000 participants. J Am Coll Cardiol. 2010;55(19):2160–7 [DOI] [PubMed] [Google Scholar]
- 6.Fullerton HJ, Wu YW, Sidney S, Johnston SC. Risk of recurrent childhood arterial ischemic stroke in a population-based cohort: the importance of cerebrovascular imaging. Pediatrics. 2007;119(3):495–501 [DOI] [PubMed] [Google Scholar]
- 7.Schoenberg BS, Mellinger JF, Schoenberg DG. Cerebrovascular disease in infants and children: a study of incidence, clinical features, and survival. Neurology. 1978;28(8): 763–8 [DOI] [PubMed] [Google Scholar]
- 8.Nelson K, Lynch JK. Stroke in newborn infants. Lancet Neurol. 2004;3(3):150–8 [DOI] [PubMed] [Google Scholar]
- 9.Goldenberg NA, Bernard TJ, Fullerton HJ, Gordon A, deVeber GInternational Pediatric Stroke Study Group Antithrombotic treatments, outcomes, and prognostic factors in acute childhood-onset arterial ischaemic stroke: a multicentre, observational, cohort study. Lancet Neurol. 2009;8(12):1120–7 [DOI] [PubMed] [Google Scholar]
- 10.Chabrier S, Husson B, Lasjaunias P, Landrieu P, Tardieu M. Stroke in childhood: outcome and recurrence risk by mechanism in 59 patients. J Child Neurol. 2000;15(5):290–4 [DOI] [PubMed] [Google Scholar]
- 11.Steinlin M, Pfister I, Pavlovic J, Everts R, Boltshauser E, Capone MA, et al. Swiss Societies of Paediatric Neurology and Neonatology The first three years of the Swiss Neuropaediatric Stroke Registry (SNPSR): a population-based study of incidence, symptoms and risk factors. Neuropediatrics. 2005;36(2):90–7 [DOI] [PubMed] [Google Scholar]
- 12.deVeber GA, MacGregor D, Curtis R, Mayank S. Neurologic outcome in survivors of childhood arterial ischemic stroke and sinovenous thrombosis. J Child Neurol. 2000;15(5):316–24 [DOI] [PubMed] [Google Scholar]
- 13.Sträter R, Becker S, von Eckardstein A, Heinecke A, Gutsche S, Junker R, et al. Prospective assessment of risk factors of recurrent stroke during childhood: a 5-year follow-up study. Lancet. 2002;360(9345): 1540–5 [DOI] [PubMed] [Google Scholar]
- 14.Bernard TJ, Goldenberg NA. Pediatric arterial ischemic stroke. Hematol Oncol Clinics North Am. 2010;24(1):167–80 [DOI] [PubMed] [Google Scholar]
- 15.Emerging Risk Factors Collaboration, Erqou S, Kaptoge S, Perry PL, Di Angelantonio E, Thompson A, White IR, et al. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302(4):412–23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nowak-Göttl U, Sträter R, Heinecke A, Junker R, Koch HG, Schuierer G, von Eckardstein A. Lipoprotein (a) and genetic polymorphisms of clotting factor V, pro-thrombin, and methylenetetrahydrofolate reductase are risk factors of spontaneous ischemic stroke in childhood. Blood. 1999; 94(11):3678–82 [PubMed] [Google Scholar]
- 17.Lynch JK, Han CJ, Nee LE, Nelson KB. Prothrombotic factors in children with stroke or porencephaly. Pediatrics. 2005; 116(2):447–53 [DOI] [PubMed] [Google Scholar]
- 18.Renaud C, Bonneau C, Presles E, Laporte S, Depeyre A, Varlet MN, Chabrier SAVCnn Group Lipoprotein (a), birth weight and neonatal stroke. Neonatology. 2010;98(3): 225–8 [DOI] [PubMed] [Google Scholar]
- 19.Bernard TJ, Manco-Johnson MJ, Lo W, MacKay MT, Ganesan V, DeVeber G, et al. Towards a consensus-based classification of childhood arterial ischemic stroke. Stroke. 2012;43(2):371–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Marcovina SM, Albers JJ, Gabel B, Koschinsky ML, Gaur VP. Effect of the number of apolipoprotein(a) kringle 4 domains on immunochemical measurements of lipoprotein(a). Clin Chem. 1995;41(2):246–55 [PubMed] [Google Scholar]
- 21.Marcovina SM, Albers JJ, Wijsman E, Zhang Z, Chapman NH, Kennedy H. Differences in Lp(a) concentrations and apo(a) polymorphs between black and white Americans. J Lipid Res. 1996;37(12):2569–85 [PubMed] [Google Scholar]
- 22.Goldenberg NA, Hathaway WE, Jacobson L, Manco-Johnson MJ. A new global assay of coagulation and fibrinolysis. Thromb Res. 2005;116(4):345–56 [DOI] [PubMed] [Google Scholar]
- 23.Goldenberg NA, Hathaway WE, Jacobson L, McFarland K, Manco-Johnson MJ. Influence of factor VIII on overall coagulability and fibrinolytic potential of haemophilic plasma as measured by global assay: monitoring in haemophilia A. Haemophilia. 2006;12(6): 605–14 [DOI] [PubMed] [Google Scholar]
- 24.Goldenberg NA, Bombardier C, Hathaway WE, McFarland K, Jacobson L, Manco-Johnson MJ. Influence of factor IX on overall plasma coagulability and fibrinolytic potential as measured by global assay: monitoring in haemophilia B. Haemophilia. 2008;14(1): 68–77 [DOI] [PubMed] [Google Scholar]
- 25.Bombardier C, Villalobos-Menuey E, Ruegg K, Hathaway WE, Manco-Johnson MJ, Goldenberg NA. Monitoring hypercoagulability and hypofibrinolysis following acute venous thromboembolism in children: application of the CloFAL assay in a prospective inception cohort study. Thromb Res. 2012; 130(3):343–9 [DOI] [PubMed] [Google Scholar]
- 26.Smith AA, Jacobson LJ, Miller BI, Hathaway WE, Manco-Johnson MJ. A new euglobulin clot lysis assay for global fibrinolysis. Thromb Res. 2003; 112(5–6):329–37 [DOI] [PubMed] [Google Scholar]
- 27.Kenet G, Lütkhoff LK, Albisetti M, Bernard T, Bonduel M, Brandao L, et al. Impact of thrombophilia on risk of arterial ischemic stroke or cerebral sinovenous thrombosis in neonates and children: a systematic review and meta-analysis of observational studies. Circulation. 2010;121(16):1838–47 [DOI] [PubMed] [Google Scholar]